Patient Characteristics Associated with Growth of Patient-Derived Tumor Implants in Mice (Patient-Derived Xenografts)

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Background
1.1. Background Findings Associated with Engraftment Success Rate
1.1.1. Tumor Stage
1.1.2. Sample Origin: Metastases
1.1.3. Tumor Type and Subtype
2. Methods
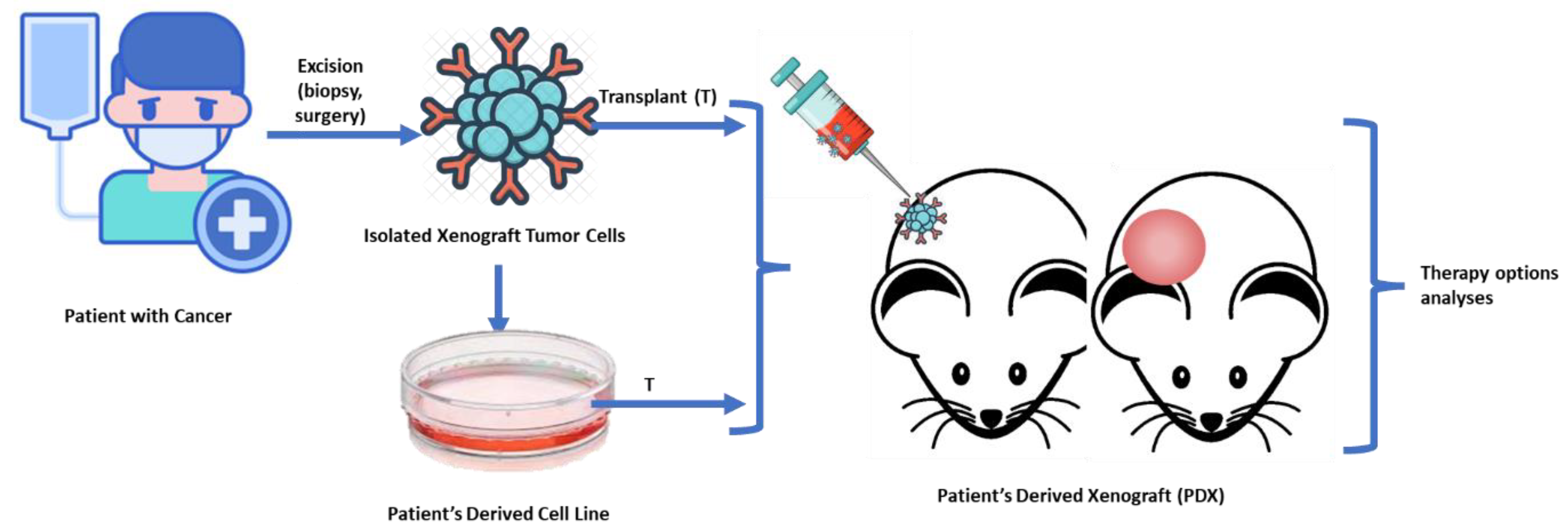
2.1. PDX Generation
- (1)
- PX0: Time elapsed between the moment of patient’s tumor implant in mice, and achievement of tumor growth (reaching a volume of 150 mm3). Because we mean to evaluate potential patient and tumor characteristics on the final success, retrieving those models that achieve a minimum initial growth was required.
- (2)
- PX1: or First Passage: time elapsed between the moment the patient’s tumor implant in mice achieves 150 mm3 and the moment the tumor is retrieved from the model and implanted on a second mouse.
- (3)
- PX2: or Second Passage: time elapsed between the moment of implant in the second mouse, and the moment of implant in the third mouse.
- (4)
- PX3: or Third Passage (coincides with the definition of final engraftment success).
2.2. Statistical Analysis
2.2.1. Assessment of Success or Failure of Engraftment
2.2.2. Comparison of Tumor Growth Rates at Each Step
2.2.3. Associations of Variables with Tumor Growth Rate in Each Passage
- If the coefficient is positive, the correlation is positive; therefore, the higher the variable, the higher the tumor growth rate should be.
- If the coefficient is negative, the correlation is negative; therefore, the higher the variable, the lower the tumor growth rate should be.
3. Results
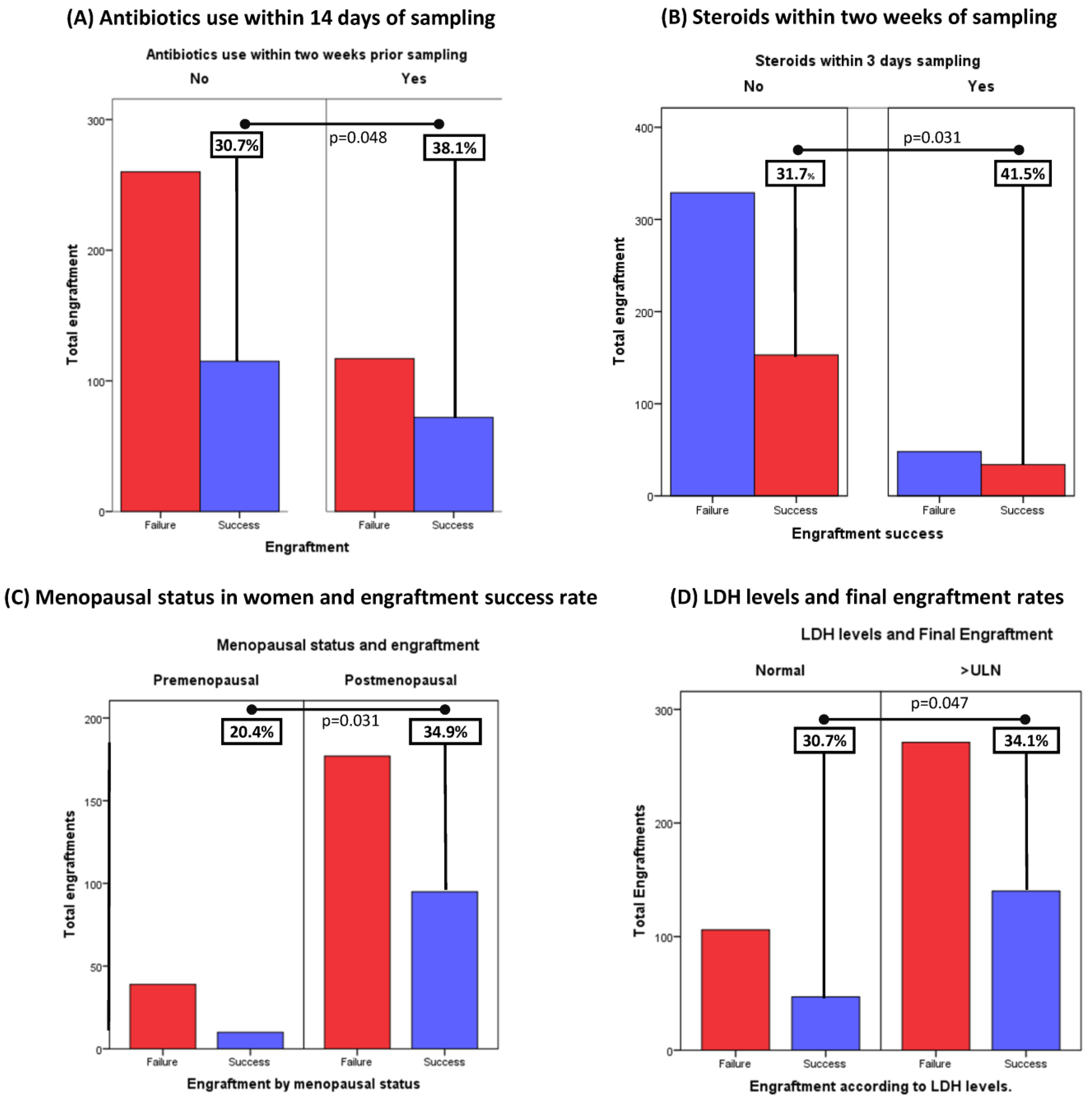
3.1. Baseline Clinical Characteristics Significantly Correlate with Engraftment Success
3.2. Tumor Growth Rate Increases throughout Passages, and Can Predict Final Success in Engraftment of Pdx Models
ROC Curves for Tumor Growth Rates in the Second Passage
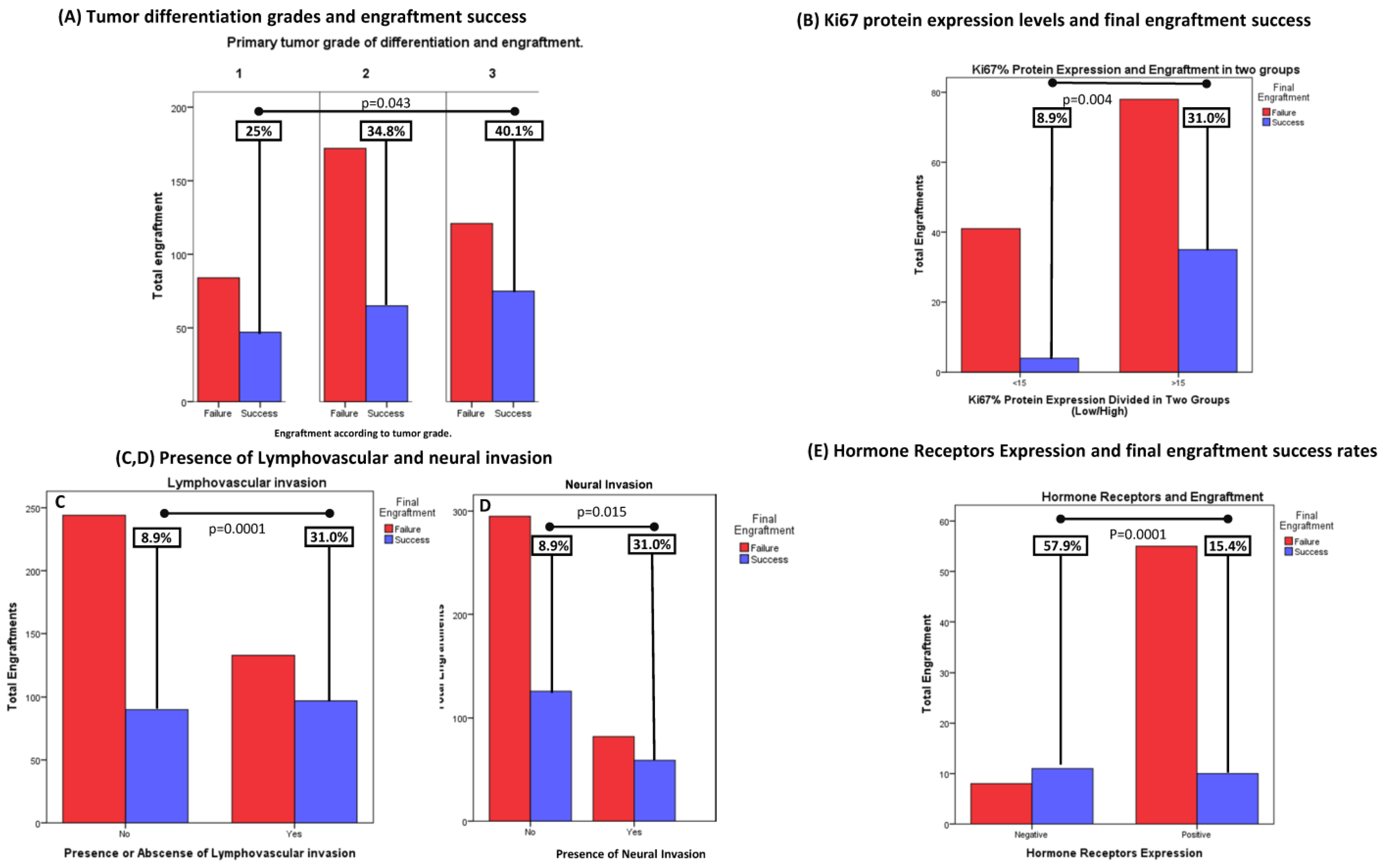
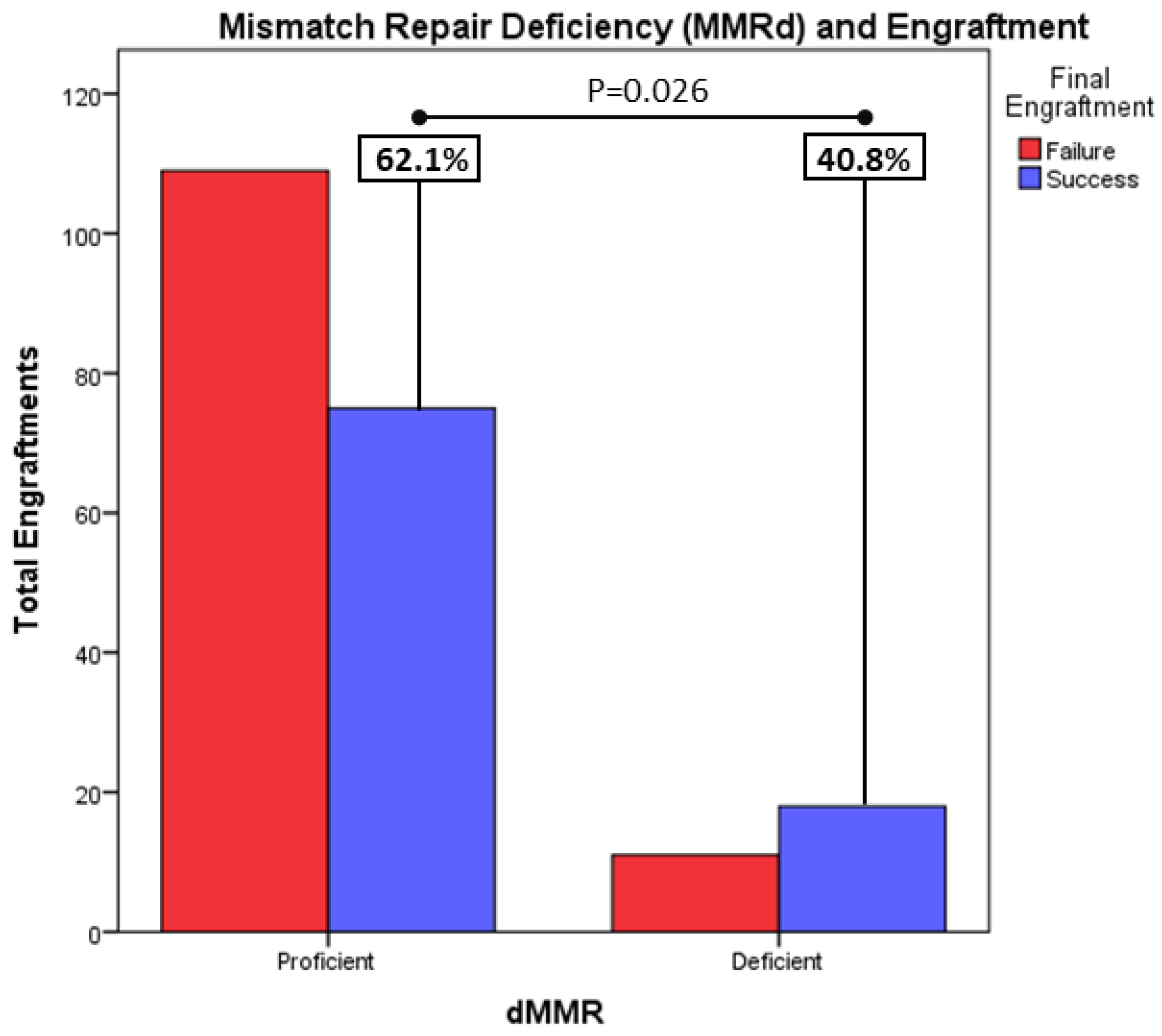
3.3. Baseline Clinical and Histological Variables Can Also Help Predict Engraftment Success
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BRAF | v-raf murine sarcoma viral oncogene homologue B1 gene |
| BRCA | Breast Cancer Gene |
| EGFR | Epidermal Growth Factor Receptor gene |
| ER | Estrogen Receptors |
| Exp | Exponential |
| FJD | Fundación Jiménez Díaz |
| HER2 | Epidermal Growth Factor Receptor 2 |
| HR | Hormone Receptors |
| IHC | Immunohistochemistry |
| IQR | Interquartile Range |
| K-RAS | Kirsten rat sarcoma viral oncogene homolog gene |
| LDH | Lactate Dehydrogenase |
| MLH1 | MutL Homolog 1 gene |
| MLH2 | MutL Homolog 2 gene |
| MMRd | Mismatch Repair Deficiency |
| MMRp | Mismatch Repair Proficiency |
| MSH6 | MutS Homolog 6 gene |
| MSI | Microsatellite Instability |
| mTGR | Median Tumor Growth Rate |
| NGS | Next-Generation Sequencing |
| N-RAS | Neuroblastoma RAS gene |
| PDXs/PDTXs | Patient-Derived Xenografts |
| PMS2 | Postmeiotic Segregation Increased 2 gene |
| PR | Progesterone Receptors |
| PX1 | Passage 1 |
| PX2 | Passage 2 |
| PX3 | Passage 3 |
| ROC | Receiver Operating Characteristic Curve |
| RPMI | Roswell Park Memorial Institute |
| START | South Texas Accelerated Research Therapeutics |
| TGR/TG | Tumor Growth Rate |
| TTG | Time to Tumor Growth |
| ULN | Upper Limit of Normality |
| V0 | Baseline Tumor Volume |
| Vt | Tumor Volume at X time. |
| WT | Wild-Type |
References
- Hidalgo, M.; Amant, F.; Biankin, A.V.; Budinská, E.; Byrne, A.T.; Caldas, C.; Clarke, R.B.; de Jong, S.; Jonkers, J.; Mælandsmo, G.M.; et al. Patient-Derived Xenograft Models: An Emerging Platform for Translational Cancer Research. Cancer Discov. 2014, 4, 998–1013. [Google Scholar] [CrossRef] [PubMed]
- Izumchenko, E.; Meir, J.; Bedi, A.; Wysocki, P.T.; Hoque, M.O.; Sidransky, D. Patient-derived xenografts as tools in pharmaceutical development. Clin. Pharmacol. Ther. 2016, 99, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Koga, Y.; Ochiai, A. Systematic Review of Patient-Derived Xenograft Models for Preclinical Studies of Anti-Cancer Drugs in Solid Tumors. Cells 2019, 8, 418. [Google Scholar] [CrossRef]
- Yada, E.; Wada, S.; Yoshida, S.; Sasada, T. Use of patient-derived xenograft mouse models in cancer research and treatment. In Future Science OA; Future Medicine Ltd.: London, UK, 2018; Volume 4. [Google Scholar]
- Xu, C.; Li, X.; Liu, P.; Li, M.; Luo, F. Patient-derived xenograft mouse models: A high fidelity tool for individualized medicine (review). In Oncology Letters; Spandidos Publications: London, UK, 2019; pp. 3–10. [Google Scholar]
- Toolan, H.W. Successful subcutaneous growth and transplantation of human tumors in X-irradiated laboratory animals. Proc. Soc. Exp. Biol. Med. 1951, 77, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Angevin, E.; Glukhova, L.; Pavon, C.; Chassevent, A.; Terrier-Lacombe, M.J.; Goguel, A.F.; Bougaran, J.; Ardouin, P.; Court, B.H.; Perrin, J.L.; et al. Human renal cell carcinoma xenografts in SCID mice: Tumorigenicity correlates with a poor clinical prognosis. Lab Investig. 1999, 79, 879–888. [Google Scholar]
- Loukopoulos, P.; Kanetaka, K.; Takamura, M.; Shibata, T.; Sakamoto, M.; Hirohashi, S. Orthotopic transplantation models of pancreatic adenocarcinoma derived from cell lines and primary tumors and displaying varying metastatic activity. Pancreas 2004, 29, 193203. [Google Scholar] [CrossRef]
- Shultz, L.D.; Schweitzer, P.A.; Christianson, S.W.; Gott, B.; Schweitzer, I.B.; Tennent, B.; McKenna, S.; Mobraaten, L.; Rajan, T.V.; Greiner, D.L.; et al. Multiple defects in innate and adaptive immunologic function in NOD/LtSz-scid mice. J. Immunol. 1995, 154, 180–191. [Google Scholar] [CrossRef]
- Shultz, L.D.; Brehm, M.A.; Garcia-Martinez, J.V.; Greiner, D.L. Humanized mice for immune system investigation: Progress, promise and challenges. Nat. Rev. Immunol. 2012, 12, 786–798. [Google Scholar] [CrossRef]
- Press, J.Z.; Kenyon, J.A.; Xue, H.; Miller, M.A.; De Luca, A.; Miller, D.M.; Huntsman, D.G.; Gilks, C.B.; McAlpine, J.N.; Wang, Y.Z.; et al. Xenografts of primary human gynecological tumors grown under the renal capsule of NOD/SCID mice show genetic stability during serial transplantation and respond to cytotoxic chemotherapy. Gynecol. Oncol. 2008, 110, 256–264. [Google Scholar] [CrossRef]
- Cutz, J.C.; Guan, J.; Bayani, J.; Yoshimoto, M.; Xue, H.; Sutcliffe, M.; English, J.; Flint, J.; LeRiche, J.; Yee, J.; et al. Establishment in Severe Combined Immunodeficiency Mice of Subrenal Capsule Xenografts and Transplantable Tumor Lines from a Variety of Primary Human Lung Cancers: Potential Models for Studying Tumor Progression–Related Changes. Clin. Cancer Res. 2006, 12, 4043–4054. [Google Scholar] [CrossRef]
- Boyd, M.R. The NCI in vitro anticancer drug discovery screen: Concept, implementation, and operation 1985–1995. In Anticancer Drug Development Guide: Preclinical Screening, Clinical Trials, and Approval; Humana Press: Totowa, NJ, USA, 1997. [Google Scholar]
- Alley, M.C.; Scudiero, D.A.; Monks, A.; Hursey, M.L.; Czerwinski, M.J.; Fine, D.L.; Abbott, B.J.; Mayo, J.G.; Shoemaker, R.H.; Boyd, M.R. Feasibility of drug screening with panels of human tumor cell lines using a microculture tetrazolium assay. Cancer Res. 1988, 48, 589–601. [Google Scholar] [PubMed]
- Chen, C.; Lin, W.; Huang, Y.; Chen, X.; Wang, H.; Teng, L. The Essential Factors of Establishing Patient-derived Tumor Model. J. Cancer 2021, 12, 28–37. [Google Scholar] [CrossRef]
- Ben-David, U.; Ha, G.; Tseng, Y.Y.; Greenwald, N.F.; Oh, C.; Shih, J.; McFarland, J.M.; Wong, B.; Boehm, J.S.; Beroukhim, R.; et al. Patient-derived xenografts undergo mouse-specific tumor evolution. Nat. Genet. 2017, 49, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Karamboulas, C.; Meens, J.; Ailles, L. Establishment and Use of Patient-Derived Xenograft Models for Drug Testing in Head and Neck Squamous Cell Carcinoma. STAR Protoc. 2020, 1, 100024. [Google Scholar] [CrossRef] [PubMed]
- Echeverria, G.V.; Cai, S.; Tu, Y.; Shao, J.; Powell, E.; Redwood, A.B.; Jiang, Y.; McCoy, A.; Rinkenbaugh, A.L.; Lau, R.; et al. Predictors of success in establishing orthotopic patient-derived xenograft models of triple negative breast cancer. NPJ Breast Cancer 2023, 9, 2. [Google Scholar] [CrossRef]
- Dong, X.; Guan, J.; English, J.C.; Flint, J.; Yee, J.; Evans, K.; Murray, K.; MacAulay, C.; Ng, R.T.; Gout, P.W.; et al. Patient-derived first generation xenografts of non-small cell lung cancers: Promising tools for predicting drug responses for personalized chemotherapy. Clin. Cancer Res. 2010, 16, 1442–1451. [Google Scholar] [CrossRef]
- Klinghammer, K.; Otto, R.; Raguse, J.D.; Albers, A.E.; Tinhofer, I.; Fichtner, I.; Leser, U.; Keilholz, U.; Hoffmann, J. Basal subtype is predictive for response to cetuximab treatment in patient-derived xenografts of squamous cell head and neck cancer. Int. J. Cancer 2017, 141, 1215–1221. [Google Scholar] [CrossRef]
- Na, D.; Chae, J.; Cho, S.Y.; Kang, W.; Lee, A.; Min, S.; Choi, J.; Lee, W.; Shin, D.; Min, A.; et al. Predictive biomarkers for 5-fluorouracil and oxaliplatin-based chemotherapy in gastric cancers via profiling of patient-derived xenografts. Nat. Commun. 2021, 12, 4840. [Google Scholar] [CrossRef]
- Garrido-Laguna, I.; Uson, M.; Rajeshkumar, N.V.; Tan, A.C.; De Oliveira, E.; Karikari, C.; Villaroel, M.C.; Salomon, A.; Taylor, G.; Sharma, R.; et al. Tumor engraftment in nude mice and enrichment in stroma-related gene pathways predict poor survival and resistance to gemcitabine in patients with pancreatic cancer. Clin. Cancer Res. 2011, 17, 5793–5800. [Google Scholar] [CrossRef]
- McAuliffe, P.F.; Evans, K.W.; Akcakanat, A.; Chen, K.; Zheng, X.; Zhao, H.; Eterovic, A.K.; Sandai, T.; Holder, A.M.; Sharma, C.; et al. Ability to generate patient-derived Breast cancer xenografts is enhanced in chemoresistant disease and predicts poor patient outcomes. PLoS ONE 2015, 10, e0136851. [Google Scholar] [CrossRef]
- Aparicio, S.; Hidalgo, M.; Kung, A.L. Examining the utility of patient-derived xenograft mouse models. Nat. Rev. Cancer 2015, 15, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, R.M. Patient-derived orthotopic xenografts: Better mimic of metastasis than subcutaneous xenografts. Nat. Rev. Cancer 2015, 15, 451–452. [Google Scholar] [CrossRef] [PubMed]
- Merino, D.; Weber, T.S.; Serrano, A.; Vaillant, F.; Liu, K.; Pal, B.; Chen, Y.; Asselin-Labat, M.L.; Shumacher, T.N.; Cameron, D.; et al. Barcoding reveals complex clonal behavior in patient-derived xenografts of metastatic triple negative breast cancer. Nat. Commun. 2019, 10, 766. [Google Scholar] [CrossRef] [PubMed]
- Baschnagel, A.M.; Kaushik, S.; Durmaz, A.; Goldstein, S.; Ong, I.M.; Abel, L.; Clar, P.A.; Gurel, Z.; Leal, T.; Buehler, D.; et al. Development and characterization of patient-derived xenografts from non-small cell lung cancer brain metastases. Sci. Rep. 2021, 11, 2520. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, R.; Wang, L.; Correa, A.M.; Pataer, A.; Xu, Y.; Zhang, X.; Ren, C.; Xu, Y.; Wu, S.; et al. Tumor characteristics associated with engraftment of patient-derived non-small cell lung cancer xenografts in immunocompromised mice. Cancer 2019, 125, 3738–3748. [Google Scholar] [CrossRef]
- Magnotti, E.; Marasco, W.A. The latest animal models of ovarian cancer for novel drug discovery. Expert Opin. Drug Discov. 2018, 13, 249–257. [Google Scholar] [CrossRef]
- Lai, Y.; Wei, X.; Lin, S.; Qin, L.; Cheng, L.; Li, P. Current status and perspectives of patient-derived xenograft models in cancer research. J. Hematol. Oncol. 2017, 10, 1–14. [Google Scholar] [CrossRef]
- Oh, B.Y.; Lee, W.Y.; Jung, S.; Hong, H.K.; Nam, D.H.; Park, Y.A.; Huh, J.W.; Yun, S.H.; Kim, H.C.; Chung, H.K.; et al. Correlation between tumor engraftment in patient-derived xenograft models and clinical outcomes in colorectal cancer patients. Oncotarget 2015, 6, 16059–16068. [Google Scholar] [CrossRef]
- Jung, J.; Seol, H.S.; Chang, S. The generation and application of patient-derived xenograft model for cancer research. Cancer Res. Treat. 2018, 50, 1–10. [Google Scholar] [CrossRef]
- Jung, J.; Lee, C.H.; Seol, H.S.; Choi, Y.S.; Kim, E.; Lee, E.J.; Rhee, J.K.; Singh, S.R.; Jun, E.S.; Han, B.; et al. Generation and molecular characterization of pancreatic cancer patient-derived xenografts reveals their heterologous nature. Oncotarget 2016, 7, 62533–62546. [Google Scholar] [CrossRef]
- Weroha, S.J.; Becker, M.A.; Enderica-Gonzalez, S.; Harrington, S.C.; Oberg, A.L.; Maurer, M.J.; Perkins, S.E.; AlHilli, M.; Butler, K.A.; McKinstry, S.; et al. Tumor grafts as In Vivo Surrogates for Women with Ovarian Cancer. Clin. Cancer Res. 2014, 20, 1288–1297. [Google Scholar] [CrossRef] [PubMed]
- Byrne, A.T.; Alférez, D.G.; Amant, F.; Annibali, D.; Arribas, J.; Biankin, A.V.; Bruna, A.; Budinská, E.; Caldas, C.; Chang, D.K.; et al. Interrogating open issues in cancer precision medicine with patient-derived xenografts. Nat. Rev. Cancer 2017, 17, 254–268. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, M.C.; Bergquist, J.R.; Leiting, J.L.; Ivanics, T.; Yang, L.; Smoot, R.L.; Nagorney, D.M.; Truty, M.J. Patient-Derived Xenografts Can Be Reliably Generated from Patient Clinical Biopsy Specimens. J. Gastrointest. Surg. 2019, 23, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Rosfjord, E.; Lucas, J.; Li, G.; Gerber, H.P. Advances in patient-derived tumor xenografts: From target identification to predicting clinical response rates in oncology. Biochem. Pharmacol. 2014, 91, 135–143. [Google Scholar] [CrossRef]
- Kim, M.P.; Evans, D.B.; Wang, H.; Abbruzzese, J.L.; Fleming, J.B.; Gallick, G.E. Generation of orthotopic and heterotopic human pancreatic cancer xenografts in immunodeficient mice. Nat. Protoc. 2009, 4, 1670–1680. [Google Scholar] [CrossRef]
- Oshi, M.; Okano, M.; Maiti, A.; Rashid, O.M.; Saito, K.; Kono, K.; Matsuyama, R.; Endo, I.; Takabe, K. Novel Breast Cancer Brain Metastasis Patient-Derived Orthotopic Xenograft Model for Preclinical Studies. Cancers 2020, 12, 444. [Google Scholar] [CrossRef]
- Puig, I.; Chicote, I.; Tenbaum, S.P.; Arqués, O.; Herance, J.R.; Gispert, J.D.; Jimenez, J.; Landolfi, S.; Caci, K.; Allende, H.; et al. A Personalized Preclinical Model to Evaluate the Metastatic Potential of Patient-Derived Colon Cancer Initiating Cells. Clin. Cancer Res. 2013, 19, 6787–6801. [Google Scholar] [CrossRef]
- Goetz, M.P.; Kalari, K.R.; Suman, V.J.; Moyer, A.M.; Yu, J.; Visscher, D.W.; Dockter, T.; Vedell, P.; Sinnwell, J.; Tang, X.; et al. Tumor Sequencing and Patient-Derived Xenografts in the Neoadjuvant Treatment of Breast Cancer. J. Natl. Cancer Inst. 2017, 109, djw306. [Google Scholar] [CrossRef]
- Ilie, M.; Nunes, M.; Blot, L.; Hofman, V.; Long-Mira, E.; Butori, C.; Selva, E.; Merino-Trigo, A.; Vénissanc, N.; Mouroux, J.; et al. Setting up a wide panel of patient-derived tumor xenografts of non-small cell lung cancer by improving the preanalytical steps. Cancer Med. 2015, 4, 201–211. [Google Scholar] [CrossRef]
- Liu, L.; Wu, M.; Huang, A.; Gao, C.; Yang, Y.; Liu, H.; Jiang, H.; Yu, L.; Huang, Y.; Wang, H. Establishment of a high-fidelity patient-derived xenograft model for cervical cancer enables the evaluation of patient’s response to conventional and novel therapies. J. Transl. Med. 2023, 21, 611. [Google Scholar] [CrossRef]
- Fiebig, H.H.; Neumann, H.A.; Henß, H.; Koch, H.; Kaiser, D.; Arnold, H. Development of Three Human Small Cell Lung Cancer Models in Nude Mice. Recent Results Cancer Res. 1985, 97, 77–86. [Google Scholar] [PubMed]
- Kerstetter-Fogle, A.E.; Harris, P.L.R.; Brady-Kalnay, S.M.; Sloan, A.E. Generation of Glioblastoma Patient-Derived Intracranial Xenografts for Preclinical Studies. Int. J. Mol. Sci. 2020, 21, 5113. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jo, D.H.; Kim, J.H.; Cho, C.S.; Han, J.E.; Kim, Y.; Park, H.; Yoo, S.H.; Yu, Y.S.; Moon, H.E.; et al. Development of a patient-derived xenograft model of glioblastoma via intravitreal injection in mice. Exp. Mol. Med. 2019, 51, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Ruan, Z.; Tang, J.; Liu, M.; Hu, C.; Fan, P.; Dai, X. Generation, evolution, interfering factors, applications, and challenges of patient-derived xenograft models in immunodeficient mice. Cancer Cell Int. 2023, 23, 120. [Google Scholar] [CrossRef] [PubMed]
- Pretlow, T.G.; Delmoro, C.M.; Dilley, G.G.; Spadafora, C.G.; Pretlow, T.P. Transplantation of Human Prostatic Carcinoma into Nude Mice in Matrigel. Cancer Res. 1991, 51, 3814–3817. [Google Scholar]
- Nool, A.; De Pauw-Gillet2, M.C.; Purnell’, G.; Nusgens3, B.; Lapiere3, C.M.; Foidart’, J.M. Enhancement of tumorigenicity of human breast adenocarcinoma cells in nude mice by matrigel and fibroblasts. Br. J. Cancer 1993, 68, 909–915. [Google Scholar] [CrossRef]
- Wulaningsih, W.; Holmberg, L.; Garmo, H.; Malmstrom, H.; Lambe, M.; Hammar, N.; Walldius, G.; Jungner, I.; Ng, T.; Hemelrijck, M.V. Serum lactate dehydrogenase and survival following cancer diagnosis. Br. J. Cancer 2015, 113, 1389–1396. [Google Scholar] [CrossRef]
- Liu, R.; Cao, J.; Gao, X.; Zhang, J.; Wang, L.; Wang, B.; Guo, L.; Hu, X.; Wang, Z. Overall survival of cancer patients with serum lactate dehydrogenase greater than 1000 IU/L. Tumor Biol. 2016, 37, 14083–14088. [Google Scholar] [CrossRef]
- Feng, W.; Wang, Y.; Zhu, X. Baseline serum lactate dehydrogenase level predicts survival benefit in patients with metastatic colorectal cancer receiving bevacizumab as first-line chemotherapy: A systematic review and meta-analysis of 7 studies and 1219 patients. Ann. Transl. Med. 2019, 7, 133. [Google Scholar] [CrossRef]
- Martin, B.; Paesmans, M.; Mascaux, C.; Berghmans, T.; Lothaire, P.; Meert, A.P.; Latiffe, J.J.; Sculier, J.P. Ki-67 expression and patients survival in lung cancer: Systematic review of the literature with meta-analysis. Br. J. Cancer 2004, 91, 2018–2025. [Google Scholar] [CrossRef]
- Luo, Z.W.; Zhu, M.G.; Zhang, Z.Q.; Ye, F.J.; Huang, W.H.; Luo, X.Z. Increased expression of Ki-67 is a poor prognostic marker for colorectal cancer patients: A meta analysis. BMC Cancer 2019, 19, 123. [Google Scholar] [CrossRef] [PubMed]
- Moro, M.; Bertolini, G.; Caserini, R.; Borzi, C.; Boeri, M.; Fabbri, A.; Leone, G.; Gasparini, P.; Galeone, C.; Pelosi, C.; et al. Establishment of patient derived xenografts as functional testing of lung cancer aggressiveness. Sci. Rep. 2017, 7, 6689. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.F.; Palakurthi, S.; Zeng, Q.; Zhou, S.; Ivanova, E.; Huang, E.; Zervantonakis, I.K.; Selfors, L.M.; Shen, Y.; Pritchard, C.C.; et al. Establishment of patient-derived tumor xenograft models of epithelial ovarian cancer for pre-clinical evaluation of novel therapeutics. Clin. Cancer Res. 2017, 23, 1263–1273. [Google Scholar] [CrossRef] [PubMed]
- Wick, A.D.; Stein, A.P.; McCulloch, T.M.; Hartig, G.; Ong, I.M.; Sampene, E.; Prabakaran, P.J.; Liu, C.; Kimple, R.J. Defining the boundaries and expanding the utility of head and neck cancer patient derived xenografts. Oral Oncol. 2017, 64, 65–72. [Google Scholar]
- Zhong, Y.M.; Tong, F.; Shen, J. Lympho-vascular invasion impacts the prognosis in breast-conserving surgery: A systematic review and meta-analysis. BMC Cancer 2022, 22, 102. [Google Scholar] [CrossRef] [PubMed]
- Christianson, S.W.; Greiner, D.L.; Schweitzer, I.B.; Gott, B.; Beamer, G.L.; Schweitzer, P.A.; Hesselton, R.M.; Shultz, L.D. Role of Natural Killer Cells on Engraftment of Human Lymphoid Cells and on Metastasis of Human T-Lymphoblastoid Leukemia Cells in C57BL/6J-scidMice and in C57BL/6J-scid bgMice. Cell. Immunol. 1996, 171, 186–199. [Google Scholar] [CrossRef]
- Houvenaeghel, G.; Cohen, M.; Classe, J.M.; Reyal, F.; Mazouni, C.; Chopin, N.; Martínez, A.; Daraï, E.; Coutant, C.; Colombo, P.E.; et al. Lymphovascular invasion has a significant prognostic impact in patients with early breast cancer, results from a large, national, multicenter, retrospective cohort study. ESMO Open 2021, 6, 100316. [Google Scholar] [CrossRef]
- Yu, J.; Qin, B.; Moyer, A.M.; Sinnwell, J.P.; Thompson, K.J.; Copland, J.A.; Marlow, L.; Miller, J.L.; Ying, P.; Gao, B.; et al. Establishing and characterizing patient-derived xenografts using pre-chemotherapy percutaneous biopsy and post-chemotherapy surgical samples from a prospective neoadjuvant breast cancer study. Breast Cancer Res. 2017, 19, 130. [Google Scholar] [CrossRef]
- Sereti, E.; Karagianellou, T.; Kotsoni, I.; Magouliotis, D.; Kamposioras, K.; Ulukaya, E.; Sakellaridis, N.; Zacharouslis, D.; Dimas, K. Patient Derived Xenografts (PDX) for personalized treatment of pancreatic cancer: Emerging allies in the war on a devastating cancer? J. Proteom. 2018, 188, 107–118. [Google Scholar] [CrossRef]
- Derose, Y.S.; Wang, G.; Lin, Y.C.; Bernard, P.S.; Buys, S.S.; Ebbert, M.T.W.; Factor, R.; Matsen, C.; Milash, B.A.; Nelson, E.; et al. Tumor grafts derived from women with breast cancer authentically reflect tumor pathology, growth, metastasis and disease outcomes. Nat. Med. 2013, 17, 1514–1520. [Google Scholar] [CrossRef]
- Zhang, X.; Claerhout, S.; Pratt, A.; Dobrolecki, L.E.; Petrovic, I.; Lai, Q.; Landis, M.D.; Wiechmann, L.; Schiff, R.; Giuliano, M.; et al. A Renewable Tissue Resource of Phenotypically Stable, Biologically and Ethnically Diverse, Patient-derived Human Breast Cancer Xenograft (PDX) Models. Cancer Res. 2013, 73, 4885–4897. [Google Scholar] [CrossRef] [PubMed]
- Fiche, M.; Scabia, V.; Aouad, P.; Battista, L.; Treboux, A.; Stravodimou, A.; Zaman, K.; Dormoy, V.; Ayyanan, A.; Sflomos, G.; et al. Intraductal patient-derived xenografts of estrogen receptor α-positive breast cancer recapitulate the histopathological spectrum and metastatic potential of human lesions. J. Pathol. 2019, 247, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Reyal, F.; Guyader, C.; Decraene, C.; Lucchesi, C.; Auger, N.; Assayag, F.; De Platter, L.; Gentien, D.; Poupon, M.F.; Cottu, P.; et al. Molecular profiling of patient-derived breast cancer xenografts. Breast Cancer Res. 2012, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Park, M.K.; Lee, C.H.; Lee, H. Mouse models of breast cancer in preclinical research. Lab. Anim. Res. 2018, 34, 160. [Google Scholar] [CrossRef] [PubMed]
- Murayama, T.; Gotoh, N. Patient-Derived Xenograft Models of Breast Cancer and Their Application. Cells 2019, 8, 621. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Foster, B.A.; Young, J.; Takabe, K. Current Update of Patient-Derived Xenograft Model for Translational Breast Cancer Research. J. Mammary Gland. Biol. Neoplasia 2017, 22, 131–139. [Google Scholar]
- Morton, C.L.; Houghton, P.J. Establishment of human tumor xenografts in immunodeficient mice. Nat. Protoc. 2007, 2, 247–250. [Google Scholar] [CrossRef]
- Luber, B.S.; Goldberg, R.M.; Wilt, C.; Fader, A.N.; Kemberling, H.; Rucki, A.A.; Laheru, D.; Donehower, R.; Zaheer, A.; Fisher, G.A.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar]
- Kim, S.T.; Klempner, S.J.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Kang, W.K.; Kim, K.M.; Lee, J. Correlating programmed death ligand 1 (PD-L 1) expression, mismatch repair deficiency, and outcomes across tumor types: Implications for immunotherapy. Oncotarget 2017, 8, 77415–77423. [Google Scholar] [CrossRef]
- Okada, S.; Vaeteewoottacharn, K.; Kariya, R. Application of Highly Immunocompromised Mice for the Establishment of Patient-Derived Xenograft (PDX) Models. Cells 2019, 8, 889. [Google Scholar] [CrossRef]
- Gitto, S.B.; Kim, H.; Rafail, S.; Omran, D.K.; Medvedev, S.; Kinose, Y.; Rodríguez-García, A.; Flowers, A.J.; Xu, H.; Schwartz, L.E.; et al. An autologous humanized patient-derived-xenograft platform to evaluate immunotherapy in ovarian cancer. Gynecol. Oncol. 2020, 156, 222–232. [Google Scholar] [CrossRef]
- Pearson, A.T.; Finkel, K.A.; Warner, K.A.; Nör, F.; Tice, D.; Martins, M.D.; Jackson, T.L.; Nör, J.E. Patient-derived xenograft (PDX) tumors increase growth rate with time. Oncotarget 2016, 7, 7993–8005. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Patient Characteristics | n (%) | |
|---|---|---|
| Clinical Characteristics | ||
| Sex | Male | 242 (42.9) |
| Female | 322 (57.1) | |
| Menopausal status | Premenopausal | 49 (8.7) |
| Postmenopausal | 273 (48.2) | |
| Diabetes Mellitus | Diabetic | 89 (15.8%) |
| Non Diabetic | 475 (84.2) | |
| Smoking habit | Non smoker | 300 |
| Smoker | 264 | |
| Chemotherapy < 21 days 1 | Yes | 23 (4%) |
| No | 541 (96%) | |
| Primary Tumor Baseline Characteristics | ||
| Tumor grade | High grade (grade 3) | 196 (34.8%) |
| Middle grade (grade 2) | 237 (42%) | |
| Low grade (grade 1) | 131 (23.2%) | |
| Ki67% | <15 | 45 (8%) |
| 15–30 | 22 (3.9%) | |
| >30 | 91 (16.1%) | |
| Total | 158 (28%) | |
| MMRd 2 | Proficient | 184 (32.6%) |
| Deficient | 29 (5.1%) | |
| Total | 213 (37.8%) | |
| HER2 expression | HER 2 Amplified | 7 (1.2%) |
| HER 2 Negative | 81 (14.4%) | |
| Total: | 88 (15,6%) | |
| Hormone Receptor Expression | Positive | 62 (11.5%) |
| Negative | 19 (3.4%) | |
| Total | 84 (14.9%) | |
| BRCAm 3 | BRCA mutant | 17 (3%) |
| BRCA wild-type | 61 (10.8%) | |
| Total | 78 (13.8) | |
| Sampling characteristics | ||
| Sample source 4 | Primary | 405 (71.8%) |
| Metastatic | 159 (28.2) | |
| Implanted Tumors and Final Growth: Total Numbers | |
|---|---|
| Tumor Type: | Implanted/Grow n |
| CNS | 38/17 |
| Bladder | 15/6 |
| Breast | 56/11 |
| Luminal Subtype | 44/5 |
| HER2 Enriched | 4/0 |
| TNBC | 8/6 |
| Cervix | 12/6 |
| CRC | 128/74 |
| Endometrial | 28/6 |
| Gastric/Gastroesophageal Junction | 11/3 |
| Kidney | 49/9 |
| NSCLC | 86/20 |
| SCLC | 5/3 |
| Ovarian | 62/19 |
| Pancreas | 8/2 |
| Liver | 7/0 |
| Head and neck | 9/3 |
| Biliary tract | 5/2 |
| Other solid tumors | 48/6 |
| Passage | Group | Median (P25%, P75%) | Comparison with PX3 | Comparison between PX1 and PX2 |
|---|---|---|---|---|
| First Passage (PX1) | PX1 | 14.6 (−68.2, 274) | <0.001 | 0.761 |
| PX2 | 64.7 (−1.70, 256) | 0.002 | ||
| PX1 + PX2 | 48.3 (−54.8, 270) | <0.001 | ||
| PX3 | 317 (125, 546) | |||
| Second Passage (PX2) | PX2 | 4079 (1538, 8765) | <0.001 | |
| PX3 | 12,514 (6544, 23,214) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández Guerrero, T.; Baños, N.; del Puerto Nevado, L.; Mahillo-Fernandez, I.; Doger De-Speville, B.; Calvo, E.; Wick, M.; García-Foncillas, J.; Moreno, V. Patient Characteristics Associated with Growth of Patient-Derived Tumor Implants in Mice (Patient-Derived Xenografts). Cancers 2023, 15, 5402. https://doi.org/10.3390/cancers15225402
Hernández Guerrero T, Baños N, del Puerto Nevado L, Mahillo-Fernandez I, Doger De-Speville B, Calvo E, Wick M, García-Foncillas J, Moreno V. Patient Characteristics Associated with Growth of Patient-Derived Tumor Implants in Mice (Patient-Derived Xenografts). Cancers. 2023; 15(22):5402. https://doi.org/10.3390/cancers15225402
Chicago/Turabian StyleHernández Guerrero, Tatiana, Natalia Baños, Laura del Puerto Nevado, Ignacio Mahillo-Fernandez, Bernard Doger De-Speville, Emiliano Calvo, Michael Wick, Jesús García-Foncillas, and Victor Moreno. 2023. "Patient Characteristics Associated with Growth of Patient-Derived Tumor Implants in Mice (Patient-Derived Xenografts)" Cancers 15, no. 22: 5402. https://doi.org/10.3390/cancers15225402
APA StyleHernández Guerrero, T., Baños, N., del Puerto Nevado, L., Mahillo-Fernandez, I., Doger De-Speville, B., Calvo, E., Wick, M., García-Foncillas, J., & Moreno, V. (2023). Patient Characteristics Associated with Growth of Patient-Derived Tumor Implants in Mice (Patient-Derived Xenografts). Cancers, 15(22), 5402. https://doi.org/10.3390/cancers15225402