

CD46–ADC Reduces the Engraftment of Multiple Myeloma Patient-Derived Xenografts

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Patient Samples
2.2. Antibody–Drug Conjugate Synthesis
2.3. Flow Cytometry
2.4. Patient Derived Xenografts
2.5. Human Light Chain ELISA
2.6. Statistics
3. Results
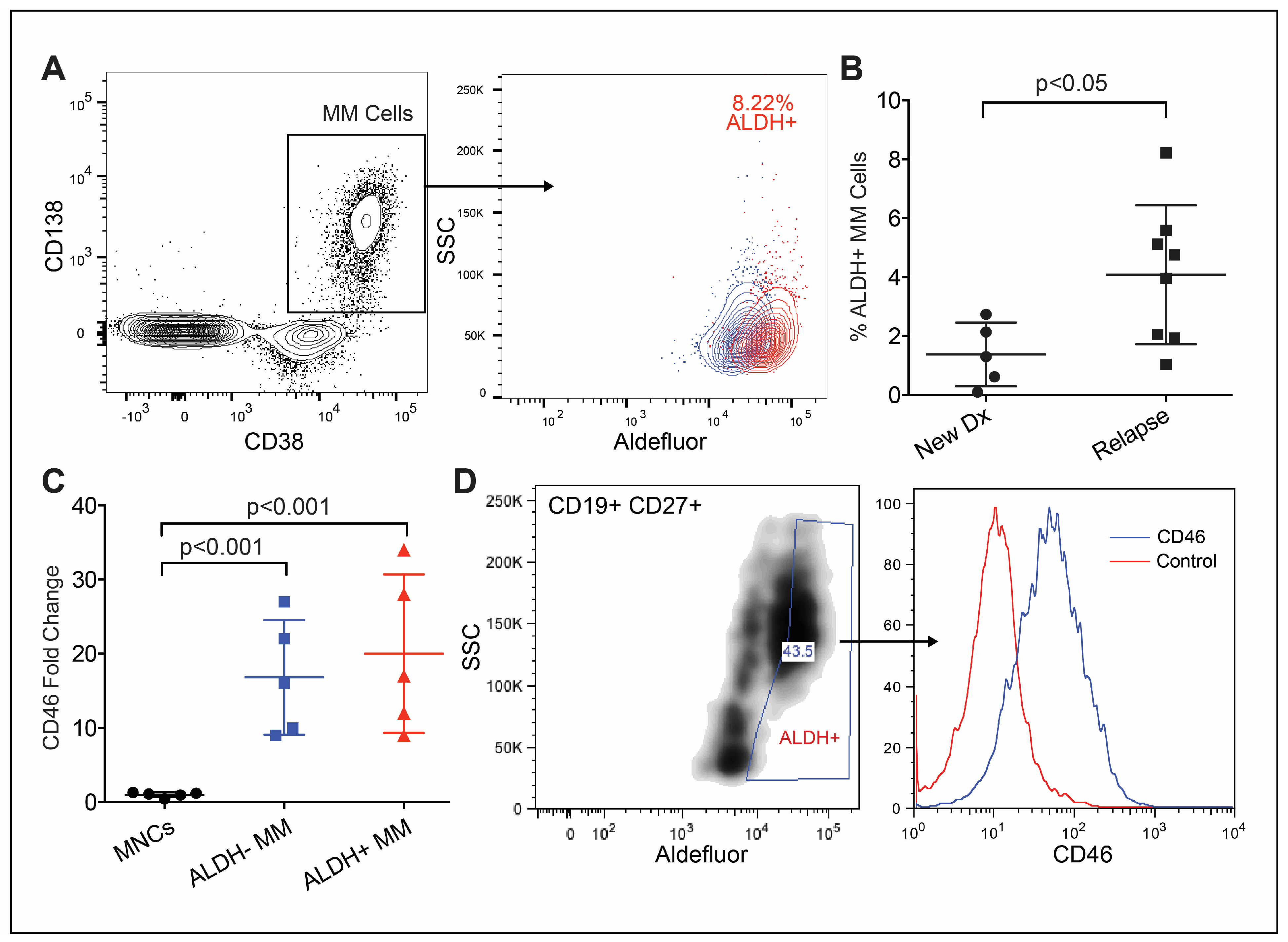
3.1. CD46 Expression on Phenotypically Immature MM Cells
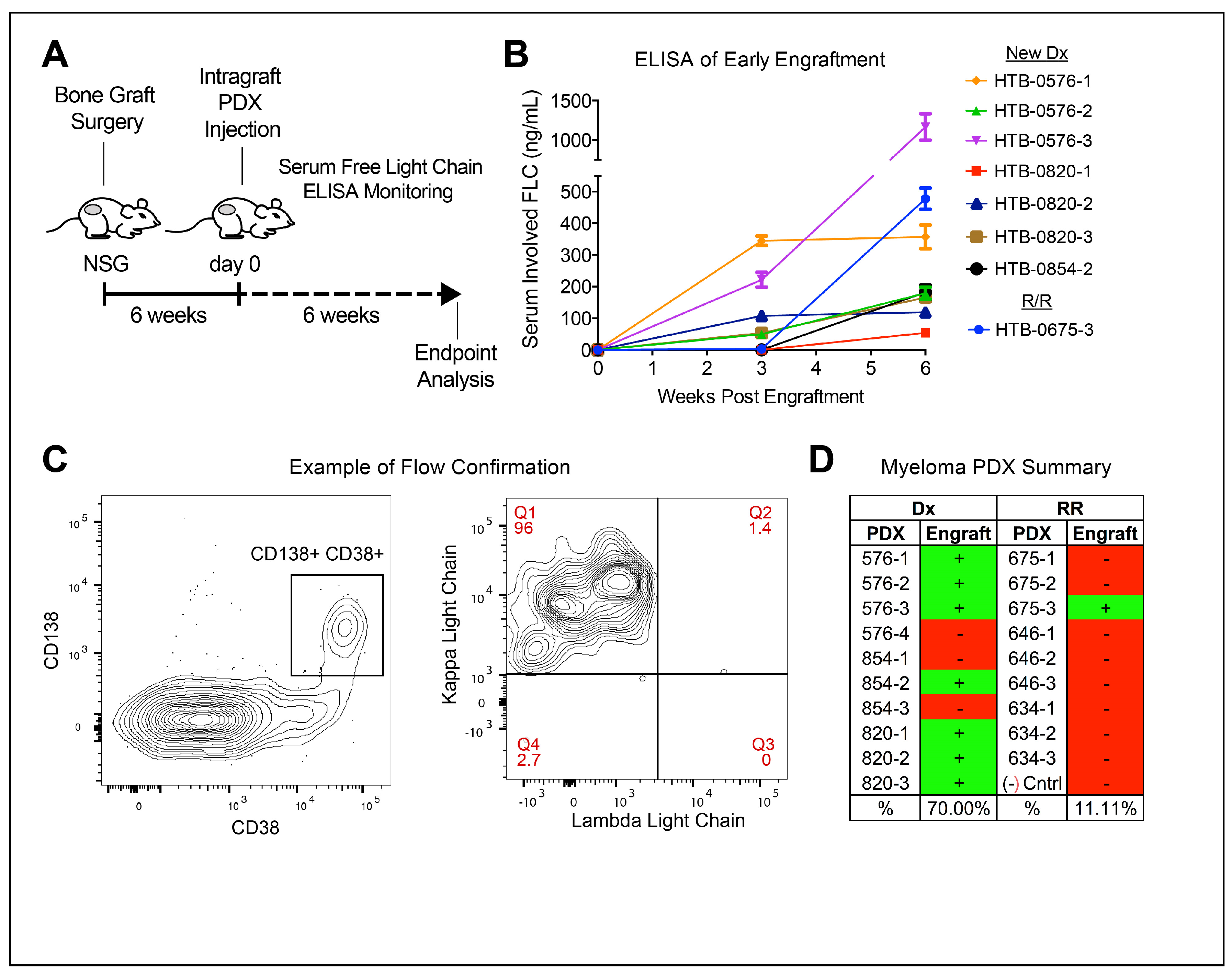
3.2. Treatment-Naïve Myeloma Cells Engraft Better in PDX
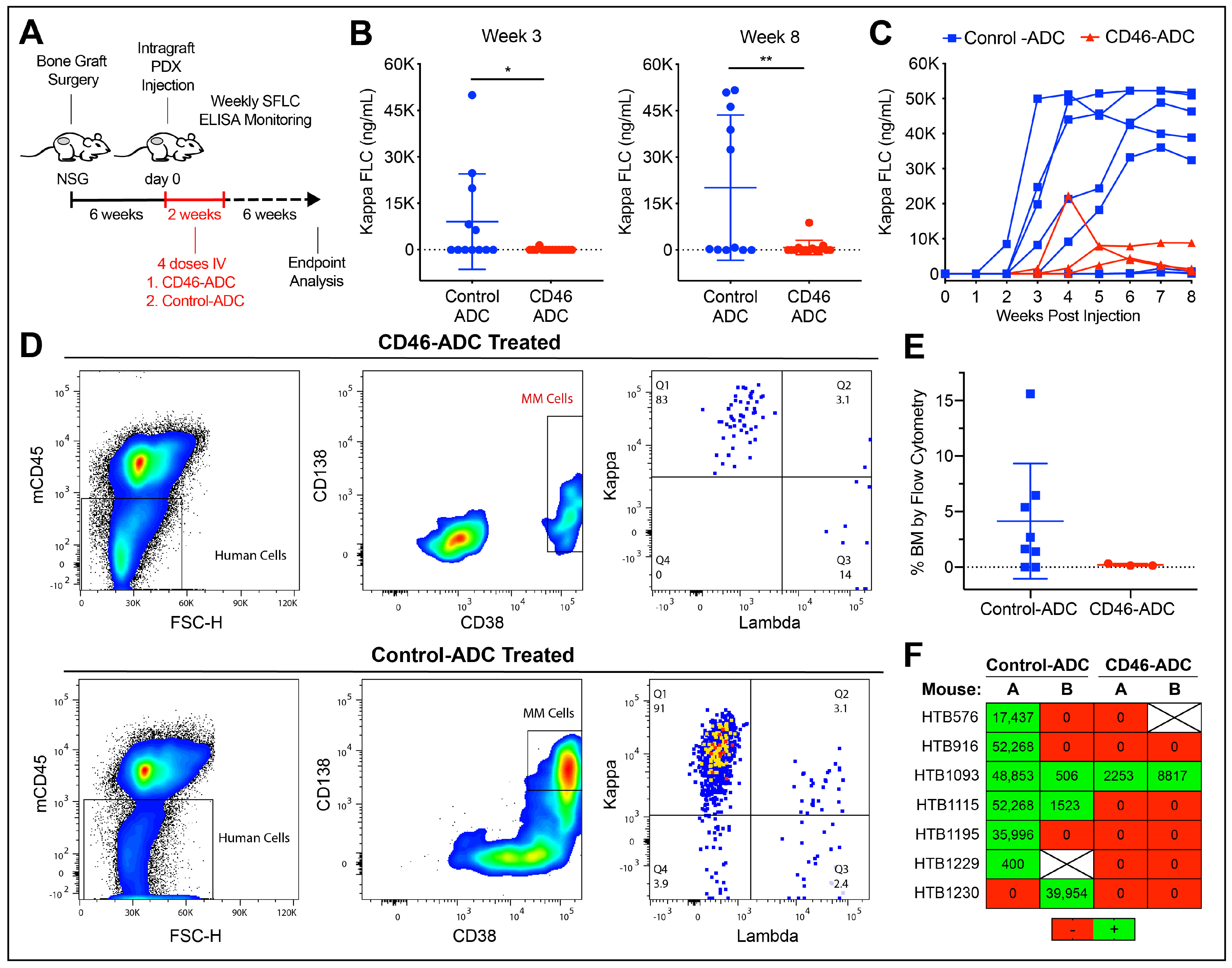
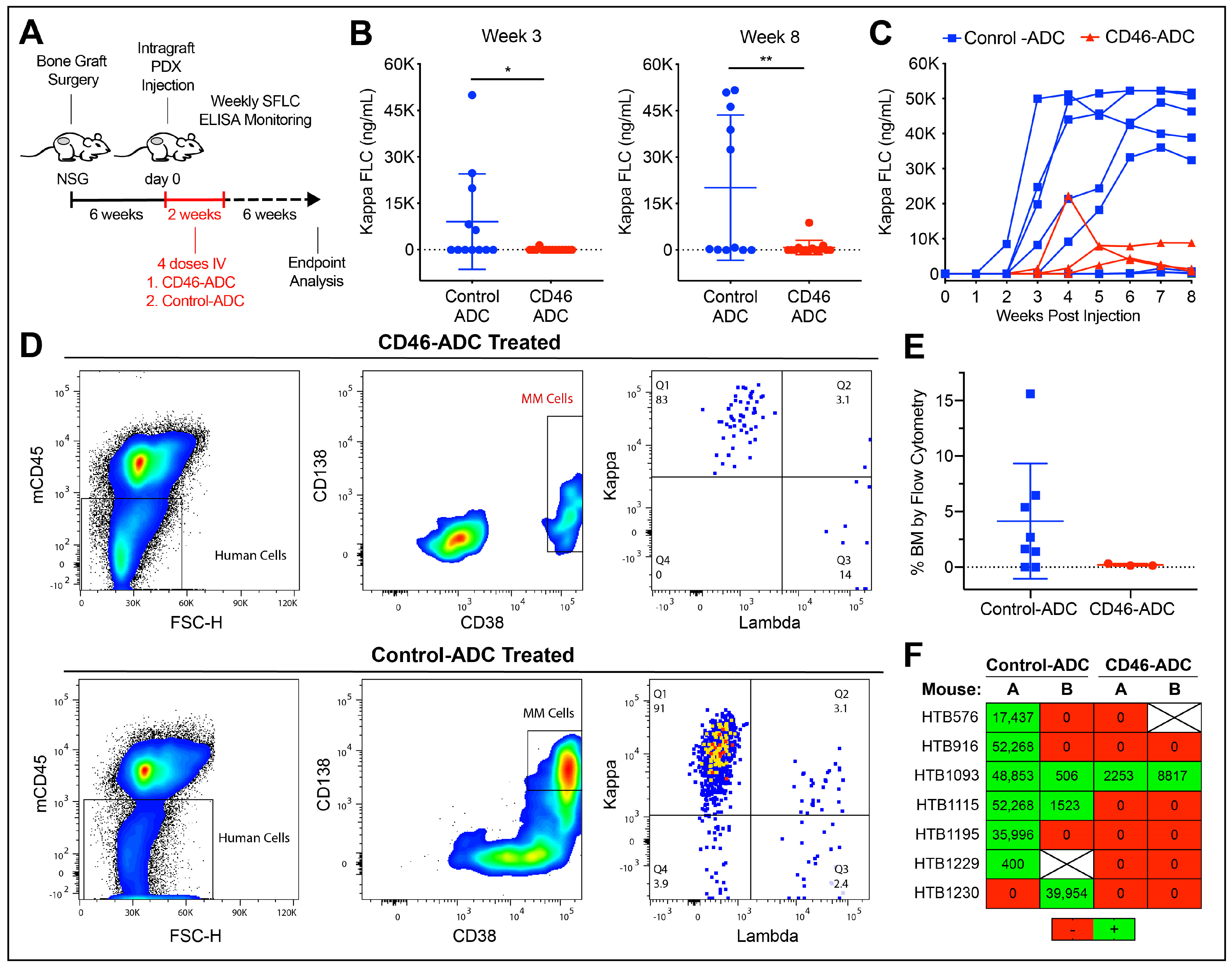
3.3. CD46–ADC Prevents the Engraftment of MM PDX
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- San Miguel, J.F.; Mateos, M.V.; Ocio, E.; Garcia-Sanz, R. Multiple myeloma: Treatment evolution. Hematology 2012, 17 (Suppl. S1), S3–S6. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, P.L.; Holstein, S.A.; Petrucci, M.T.; Richardson, P.G.; Hulin, C.; Tosi, P.; Bringhen, S.; Musto, P.; Anderson, K.C.; Caillot, D.; et al. Lenalidomide Maintenance After Autologous Stem-Cell Transplantation in Newly Diagnosed Multiple Myeloma: A Meta-Analysis. J. Clin. Oncol. 2017, 35, 3279–3289. [Google Scholar] [CrossRef] [PubMed]
- Nijhof, I.S.; Casneuf, T.; van Velzen, J.; van Kessel, B.; Axel, A.E.; Syed, K.; Groen, R.W.; van Duin, M.; Sonneveld, P.; Minnema, M.C.; et al. CD38 expression and complement inhibitors affect response and resistance to daratumumab therapy in myeloma. Blood 2016, 128, 959–970. [Google Scholar] [CrossRef] [PubMed]
- Sherbenou, D.W.; Mark, T.M.; Forsberg, P. Monoclonal Antibodies in Multiple Myeloma: A New Wave of the Future. Clin. Lymphoma Myeloma Leuk. 2017, 17, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Mohan, M.; Becnel, M.R.; Shah, U.A.; Dong, H.; Gundarlapalli, S.; Peterson, T.; Orozco, J.S.; Horowitz, S.; Chhabra, S.; Dhakal, B.; et al. Clinical efficacy of sequencing CD38 targeting monoclonal antibodies in relapsed refractory multiple myeloma: A multi-institutional experience. Am. J. Hematol. 2022, 97, E276–E280. [Google Scholar] [CrossRef] [PubMed]
- Mikhael, J.; Belhadj-Merzoug, K.; Hulin, C.; Vincent, L.; Moreau, P.; Gasparetto, C.; Pour, L.; Spicka, I.; Vij, R.; Zonder, J.; et al. A phase 2 study of isatuximab monotherapy in patients with multiple myeloma who are refractory to daratumumab. Blood Cancer J. 2021, 11, 89. [Google Scholar] [CrossRef]
- Perez de Acha, O.; Reiman, L.; Jayabalan, D.S.; Walker, Z.J.; Bosma, G.N.; Keller, A.L.; Parzych, S.E.; Abbott, D.; Idler, B.M.; Ribadeneyra, D.; et al. CD38 Antibody Re-treatment in Daratumumab-Refractory Multiple Myeloma After Time on Other Therapies. Blood Adv. 2023, 7, 6430–6440. [Google Scholar] [CrossRef]
- Munshi, N.C.; Anderson, L.D., Jr.; Shah, N.; Madduri, D.; Berdeja, J.; Lonial, S.; Raje, N.; Lin, Y.; Siegel, D.; Oriol, A.; et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N. Engl. J. Med. 2021, 384, 705–716. [Google Scholar] [CrossRef]
- Martin, T.; Usmani, S.Z.; Berdeja, J.G.; Agha, M.; Cohen, A.D.; Hari, P.; Avigan, D.; Deol, A.; Htut, M.; Lesokhin, A.; et al. Ciltacabtagene Autoleucel, an Anti-B-cell Maturation Antigen Chimeric Antigen Receptor T-Cell Therapy, for Relapsed/Refractory Multiple Myeloma: CARTITUDE-1 2-Year Follow-Up. J. Clin. Oncol. 2023, 41, 1265–1274. [Google Scholar] [CrossRef]
- Moreau, P.; Garfall, A.L.; van de Donk, N.; Nahi, H.; San-Miguel, J.F.; Oriol, A.; Nooka, A.K.; Martin, T.; Rosinol, L.; Chari, A.; et al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2022, 387, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Lonial, S.; Lee, H.C.; Badros, A.; Trudel, S.; Nooka, A.K.; Chari, A.; Abdallah, A.O.; Callander, N.; Lendvai, N.; Sborov, D.; et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): A two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2020, 21, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Ray, U.; Orlowski, R.Z. Antibody-Drug Conjugates for Multiple Myeloma: Just the Beginning, or the Beginning of the End? Pharmaceuticals 2023, 16, 590. [Google Scholar] [CrossRef] [PubMed]
- Sherbenou, D.W.; Aftab, B.T.; Su, Y.; Behrens, C.R.; Wiita, A.; Logan, A.C.; Acosta-Alvear, D.; Hann, B.C.; Walter, P.; Shuman, M.A.; et al. Antibody-drug conjugate targeting CD46 eliminates multiple myeloma cells. J. Clin. Investig. 2016, 126, 4640–4653. [Google Scholar] [CrossRef] [PubMed]
- Walker, Z.J.; Van Wyngarden, M.J.; Stevens, B.M.; Abbott, D.; Hammes, A.; Langouet-Astrie, C.; Smith, C.A.; Palmer, B.E.; Forsberg, P.A.; Mark, T.M.; et al. Measurement of ex vivo resistance to proteasome inhibitors, IMiDs, and daratumumab during multiple myeloma progression. Blood Adv. 2020, 4, 1628–1639. [Google Scholar] [CrossRef] [PubMed]
- Kyoizumi, S.; Baum, C.M.; Kaneshima, H.; McCune, J.M.; Yee, E.J.; Namikawa, R. Implantation and maintenance of functional human bone marrow in SCID-hu mice. Blood 1992, 79, 1704–1711. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Chen, B.P.; Chen, S.; Pinkus, G.S.; Bronson, R.T.; Dedera, D.A.; Hoshi, Y.; Teoh, G.; Ogata, A.; Treon, S.P.; et al. The development of a model for the homing of multiple myeloma cells to human bone marrow. Blood 1997, 90, 754–765. [Google Scholar] [CrossRef] [PubMed]
- Doronina, S.O.; Mendelsohn, B.A.; Bovee, T.D.; Cerveny, C.G.; Alley, S.C.; Meyer, D.L.; Oflazoglu, E.; Toki, B.E.; Sanderson, R.J.; Zabinski, R.F.; et al. Enhanced activity of monomethylauristatin F through monoclonal antibody delivery: Effects of linker technology on efficacy and toxicity. Bioconjug. Chem. 2006, 17, 114–124. [Google Scholar] [CrossRef]
- Matsui, W.; Huff, C.A.; Wang, Q.; Malehorn, M.T.; Barber, J.; Tanhehco, Y.; Smith, B.D.; Civin, C.I.; Jones, R.J. Characterization of clonogenic multiple myeloma cells. Blood 2004, 103, 2332–2336. [Google Scholar] [CrossRef]
- Matsui, W.; Wang, Q.; Barber, J.P.; Brennan, S.; Smith, B.D.; Borrello, I.; McNiece, I.; Lin, L.; Ambinder, R.F.; Peacock, C.; et al. Clonogenic multiple myeloma progenitors, stem cell properties, and drug resistance. Cancer Res. 2008, 68, 190–197. [Google Scholar] [CrossRef]
- Kim, D.; Park, C.Y.; Medeiros, B.C.; Weissman, I.L. CD19-CD45 low/− CD38 high/CD138+ plasma cells enrich for human tumorigenic myeloma cells. Leukemia 2012, 26, 2530–2537. [Google Scholar] [CrossRef]
- Johnsen, H.E.; Bøgsted, M.; Schmitz, A.; Bødker, J.S.; El-Galaly, T.C.; Johansen, P.; Valent, P.; Zojer, N.; Van Valckenborgh, E.; Vanderkerken, K.; et al. The myeloma stem cell concept, revisited: From phenomenology to operational terms. Haematologica 2016, 101, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, R.; Bergsagel, P.L.; Drach, J.; Shaughnessy, J.; Gutierrez, N.; Stewart, A.K.; Morgan, G.; Van Ness, B.; Chesi, M.; Minvielle, S.; et al. International Myeloma Working Group molecular classification of multiple myeloma: Spotlight review. Leukemia 2009, 23, 2210–2221. [Google Scholar] [CrossRef]
- Hanamura, I.; Stewart, J.P.; Huang, Y.; Zhan, F.; Santra, M.; Sawyer, J.R.; Hollmig, K.; Zangarri, M.; Pineda-Roman, M.; van Rhee, F.; et al. Frequent gain of chromosome band 1q21 in plasma-cell dyscrasias detected by fluorescence in situ hybridization: Incidence increases from MGUS to relapsed myeloma and is related to prognosis and disease progression following tandem stem-cell transplantation. Blood 2006, 108, 1724–1732. [Google Scholar] [CrossRef] [PubMed]
- Pillarisetti, K.; Edavettal, S.; Mendonça, M.; Li, Y.; Tornetta, M.; Babich, A.; Majewski, N.; Husovsky, M.; Reeves, D.; Walsh, E.; et al. A T-cell-redirecting bispecific G-protein-coupled receptor class 5 member D x CD3 antibody to treat multiple myeloma. Blood 2020, 135, 1232–1243. [Google Scholar] [CrossRef] [PubMed]
- Ovacik, A.M.; Li, J.; Lemper, M.; Danilenko, D.; Stagg, N.; Mathieu, M.; Ellerman, D.; Gupta, V.; Kalia, N.; Nguy, T.; et al. Single cell-produced and in vitro-assembled anti-FcRH5/CD3 T-cell dependent bispecific antibodies have similar in vitro and in vivo properties. mAbs 2019, 11, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Sherbenou, D.W.; Su, Y.; Behrens, C.R.; Aftab, B.T.; Perez de Acha, O.; Murnane, M.; Bearrows, S.C.; Hann, B.C.; Wolf, J.L.; Martin, T.G.; et al. Potent Activity of an Anti-ICAM1 Antibody-Drug Conjugate against Multiple Myeloma. Clin. Cancer Res. 2020, 26, 6028–6038. [Google Scholar] [CrossRef] [PubMed]
- Shultz, L.D.; Brehm, M.A.; Garcia-Martinez, J.V.; Greiner, D.L. Humanized mice for immune system investigation: Progress, promise and challenges. Nat. Rev. Immunol. 2012, 12, 786–798. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Strowig, T.; Verma, R.; Koduru, S.; Hafemann, A.; Hopf, S.; Kocoglu, M.H.; Borsotti, C.; Zhang, L.; Branagan, A.; et al. Microenvironment-dependent growth of preneoplastic and malignant plasma cells in humanized mice. Nat. Med. 2016, 22, 1351–1357. [Google Scholar] [CrossRef]
- Wong, S.; Imus, P.; Mark, T.; Kaufman, J.; Imus, A.; Zonder, J.A.; Walker, Z.; Sherbenou, D.; Schroeder, M.; Abbey, J.; et al. P-225: A first-in-human study of FOR46 in patients with triple refractory Multiple Myeloma. Clin. Lymphoma Myeloma Leuk. 2021, 21, S164. [Google Scholar] [CrossRef]
- Su, Y.; Liu, Y.; Behrens, C.R.; Bidlingmaier, S.; Lee, N.K.; Aggarwal, R.; Sherbenou, D.W.; Burlingame, A.L.; Hann, B.C.; Simko, J.P.; et al. Targeting CD46 for both adenocarcinoma and neuroendocrine prostate cancer. JCI Insight 2018, 3, e121497. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| DISEASE STATE | BM MM% | IG | PRIOR TREATMENT | FISH | |
|---|---|---|---|---|---|
| HTB-0576 | New diagnosis | 40–50% | KLC | None | Hyperdiploid, 13q-, uncharacterized IgH translocation, 11q+ |
| HTB-0820 | New diagnosis | 95% | KLC | None | t(8;22), 1q+, 13q-, 11q+ |
| HTB-0854 | New diagnosis | 80% | KLC | None | t(4;14), 1p-, 12- |
| HTB-0675 | Relapse | 90% | LLC | RVD, ASCT, Rm, VDT-PACE, ASCT, Pom, CarPomD, Panda/RD | 1q+, t(11;14) |
| HTB-0634 | Relapse | 50–60% | LLC | VD, ASCT, RD, VD, KD, Ixa/Dex | 11q+ |
| HTB-0646 | Relapse | 80% | LLC | VD, VDPACE, ASCT, KRD, Benda-RD, Elo-RD, Dara | 1q+ 13q- 1p-, t(4;14) |
| HTB-0916 | New diagnosis | 80% | KLC | None | t(11;14) |
| HTB-1093 | New diagnosis | 90% | KLC | None | t(8;14), 1q+, 13- |
| HTB-1115 | New diagnosis | 70% | KLC | None | t(11;14), 1q+, 11q+ |
| HTB-1195 | New diagnosis | 90% | KLC | None | t(8;22), t(14;16), 1q+, +11, +13, +17 |
| HTB-1229 | New diagnosis | 40% | KLC | None | +11q, +17 |
| HTB-1230 | New diagnosis | 75% | KLC | None | Hyperdiploid, 1q+, 13q- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
VanWyngarden, M.J.; Walker, Z.J.; Su, Y.; Perez de Acha, O.; Stevens, B.M.; Forsberg, P.A.; Mark, T.M.; Matsui, W.; Liu, B.; Sherbenou, D.W. CD46–ADC Reduces the Engraftment of Multiple Myeloma Patient-Derived Xenografts. Cancers 2023, 15, 5335. https://doi.org/10.3390/cancers15225335
VanWyngarden MJ, Walker ZJ, Su Y, Perez de Acha O, Stevens BM, Forsberg PA, Mark TM, Matsui W, Liu B, Sherbenou DW. CD46–ADC Reduces the Engraftment of Multiple Myeloma Patient-Derived Xenografts. Cancers. 2023; 15(22):5335. https://doi.org/10.3390/cancers15225335
Chicago/Turabian StyleVanWyngarden, Michael J., Zachary J. Walker, Yang Su, Olivia Perez de Acha, Brett M. Stevens, Peter A. Forsberg, Tomer M. Mark, William Matsui, Bin Liu, and Daniel W. Sherbenou. 2023. "CD46–ADC Reduces the Engraftment of Multiple Myeloma Patient-Derived Xenografts" Cancers 15, no. 22: 5335. https://doi.org/10.3390/cancers15225335
APA StyleVanWyngarden, M. J., Walker, Z. J., Su, Y., Perez de Acha, O., Stevens, B. M., Forsberg, P. A., Mark, T. M., Matsui, W., Liu, B., & Sherbenou, D. W. (2023). CD46–ADC Reduces the Engraftment of Multiple Myeloma Patient-Derived Xenografts. Cancers, 15(22), 5335. https://doi.org/10.3390/cancers15225335