
Oncological Outcomes, Long-Term Toxicities, Quality of Life and Sexual Health after Pencil-Beam Scanning Proton Therapy in Patients with Low-Grade Glioma

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
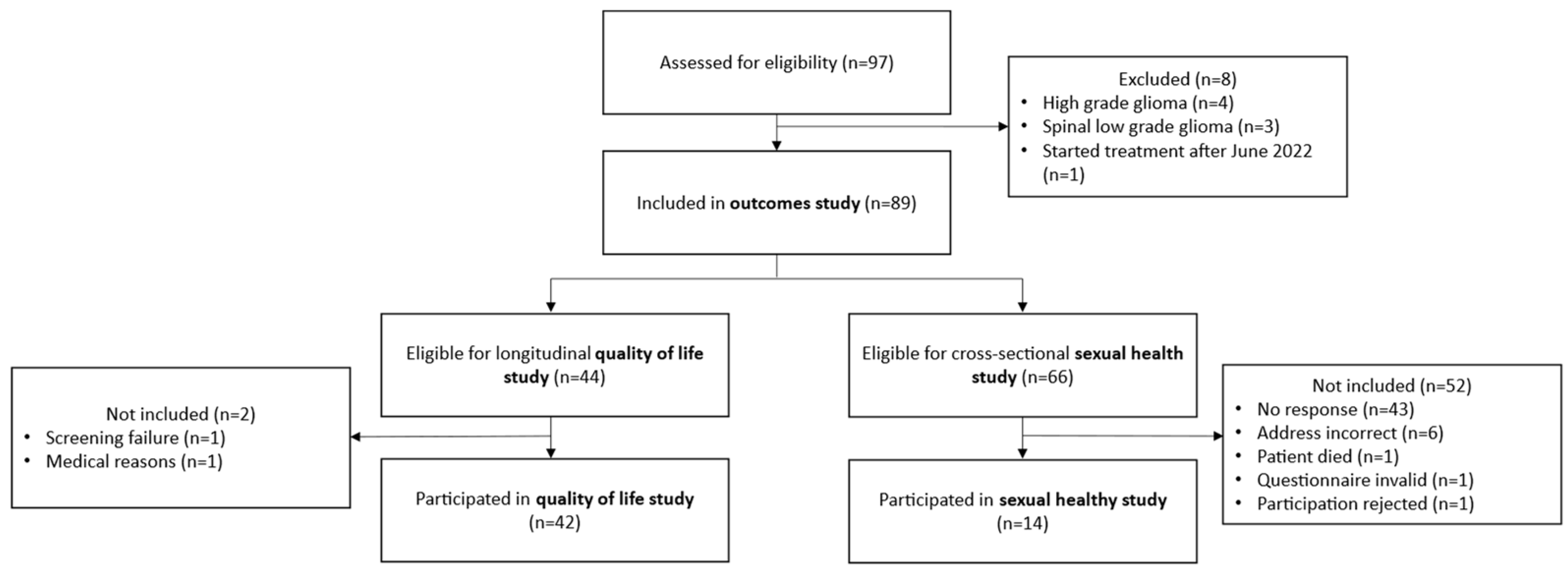
2.1. Patients
2.2. Study Design
2.3. Treatment and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
3.2. Oncological Outcomes and Patterns of Failure
3.3. Toxicity
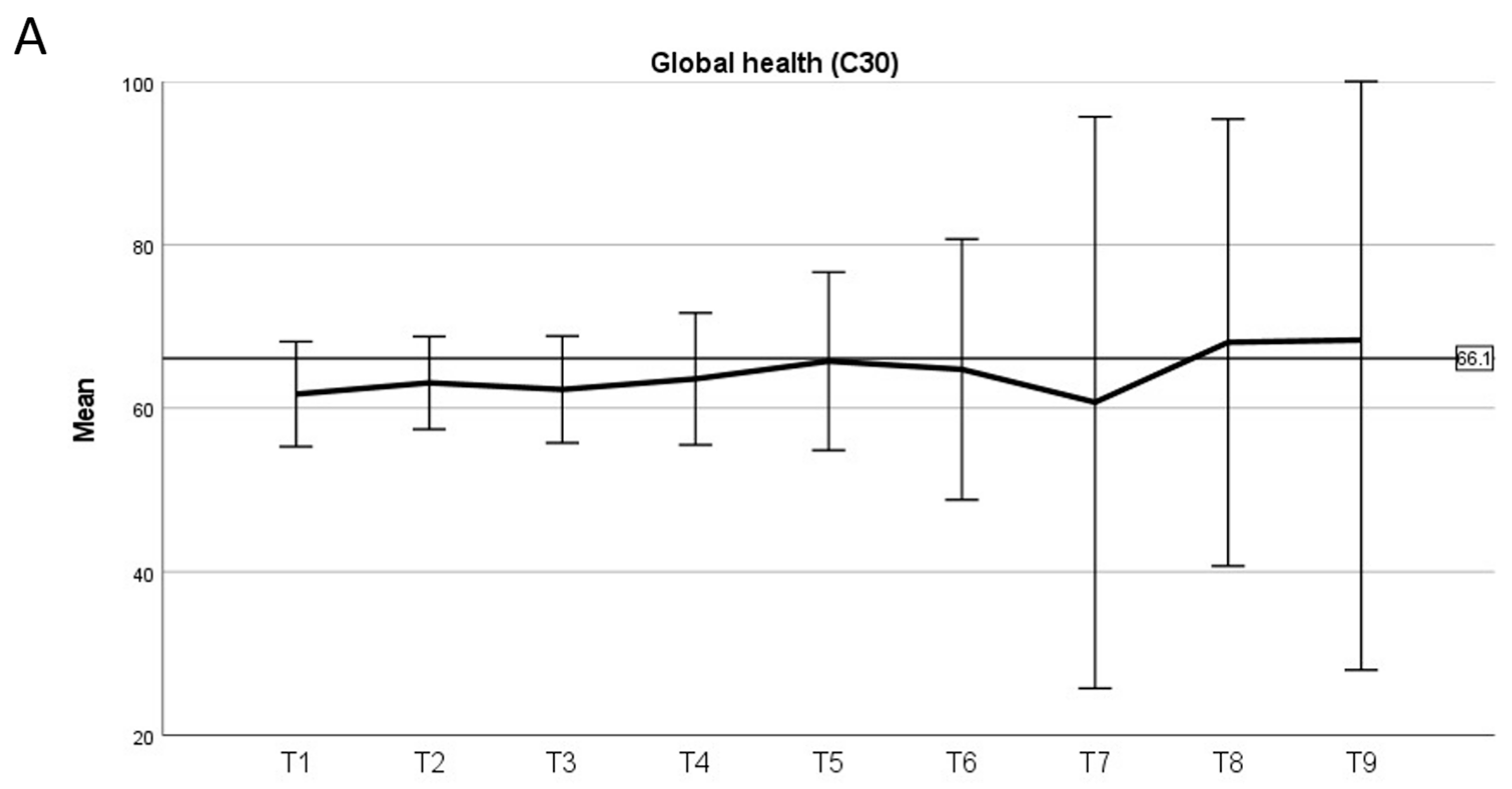
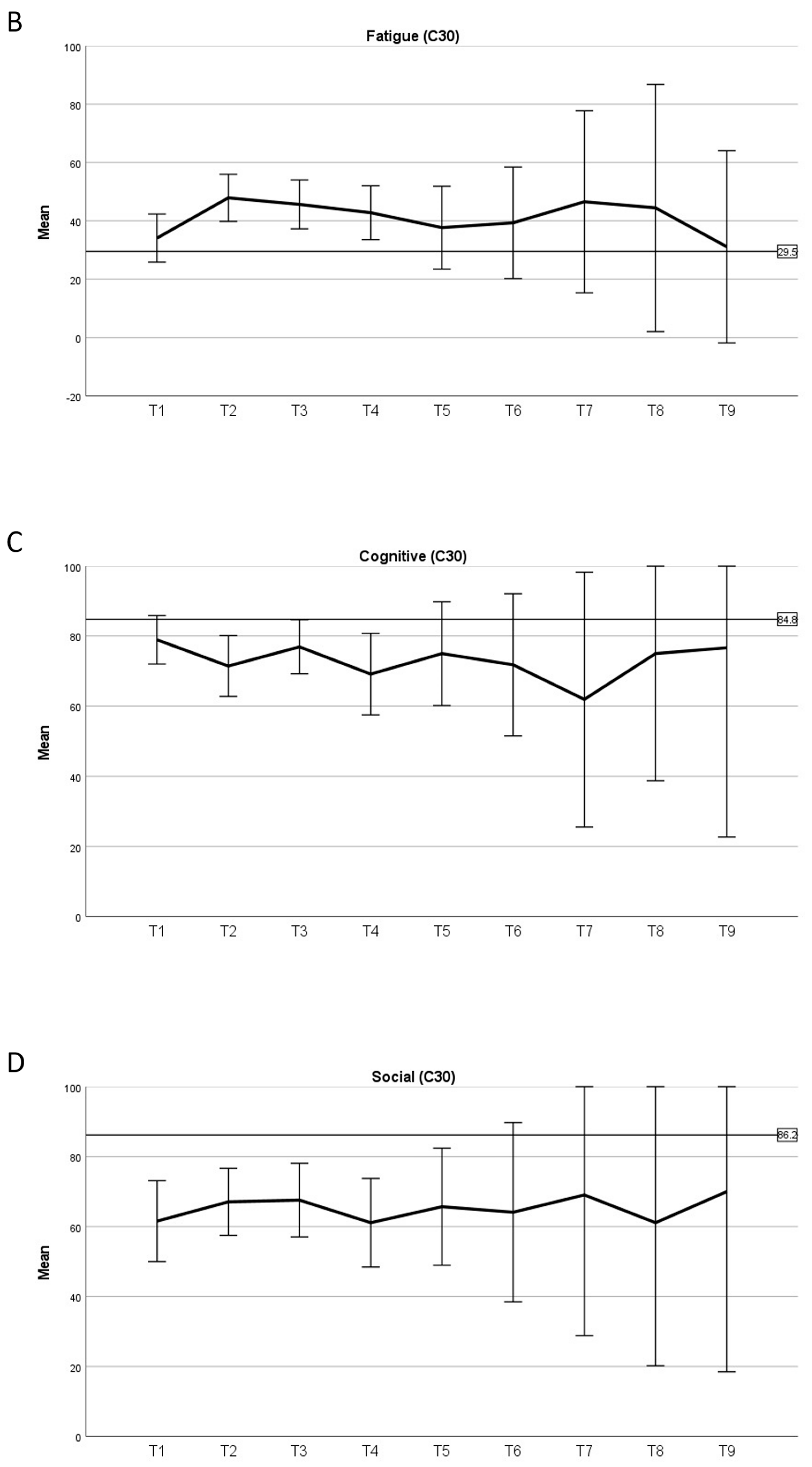
3.4. Quality of Life
3.5. Sexual Health
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kleihues, P.; Louis, D.N.; Scheithauer, B.W.; Rorke, L.B.; Reifenberger, G.; Burger, P.C.; Cavenee, W.K. The WHO Classification of Tumors of the Nervous System. J. Neuropathol. Exp. Neurol. 2002, 61, 215–225, discussion 226–229. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Cioffi, G.; Gittleman, H.; Patil, N.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012–2016. Neuro Oncol. 2019, 21, v1–v100. [Google Scholar] [CrossRef]
- Brown, T.J.; Bota, D.A.; Bent, M.J.v.D.; Brown, P.D.; Maher, E.; Aregawi, D.; Liau, L.M.; Buckner, J.C.; Weller, M.; Berger, M.S.; et al. Management of low-grade glioma: A systematic review and meta-analysis. Neuro Oncol. Pract. 2019, 6, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Mellinghoff, I.K.; Bent, M.J.v.D.; Blumenthal, D.T.; Touat, M.; Peters, K.B.; Clarke, J.; Mendez, J.; Yust-Katz, S.; Welsh, L.; Mason, W.P.; et al. Vorasidenib in IDH1- or IDH2-Mutant Low-Grade Glioma. N. Engl. J. Med. 2023, 389, 589–601. [Google Scholar] [CrossRef]
- Shaw, E.G.; Wang, M.; Coons, S.W.; Brachman, D.G.; Buckner, J.C.; Stelzer, K.J.; Barger, G.R.; Brown, P.D.; Gilbert, M.R.; Mehta, M.P. Randomized trial of radiation therapy plus procarbazine, lomustine, and vincristine chemotherapy for supratentorial adult low-grade glioma: Initial results of RTOG 9802. J. Clin. Oncol. 2012, 30, 3065–3070. [Google Scholar] [CrossRef] [PubMed]
- van den Bent, M.J.; Afra, D.; de Witte, O.; Ben Hassel, M.; Schraub, S.; Hoang-Xuan, K.; Malmström, P.-O.; Collette, L.; Piérart, M.; Mirimanoff, R.; et al. Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: The EORTC 22845 randomised trial. Lancet 2005, 366, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Karim, A.B.; Maat, B.; Hatlevoll, R.; Menten, J.; Rutten, E.H.; Thomas, D.G.; Mascarenhas, F.; Horiot, J.C.; Parvinen, L.M.; van Reijn, M.; et al. A randomized trial on dose-response in radiation therapy of low-grade cerebral glioma: European Organization for Research and Treatment of Cancer (EORTC) study 22844. Int. J. Radiat. Oncol. 1996, 36, 549–556. [Google Scholar] [CrossRef]
- Buckner, J.C.; Shaw, E.G.; Pugh, S.L.; Chakravarti, A.; Gilbert, M.R.; Barger, G.R.; Coons, S.; Ricci, P.; Bullard, D.; Brown, P.D.; et al. Radiation plus Procarbazine, CCNU, and Vincristine in Low-Grade Glioma. N. Engl. J. Med. 2016, 374, 1344–1355. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.C.; Lim, P.S.; Tran, S.; Walser, M.; Bolsi, A.; Kliebsch, U.; Beer, J.; Bachtiary, B.; Lomax, T.; Pica, A. Proton therapy for brain tumours in the area of evidence-based medicine. Br. J. Radiol. 2020, 93, 20190237. [Google Scholar] [CrossRef]
- McAleer, M.F.; Brown, P.D. Neurocognitive Function Following Therapy for Low-Grade Gliomas. Semin. Radiat. Oncol. 2015, 25, 210–218. [Google Scholar] [CrossRef]
- Greenberger, B.A.; Pulsifer, M.B.; Ebb, D.H.; MacDonald, S.M.; Jones, R.M.; Butler, W.E.; Huang, M.S.; Marcus, K.J.; Oberg, J.A.; Tarbell, N.J.; et al. Clinical outcomes and late endocrine, neurocognitive, and visual profiles of proton radiation for pediatric low-grade gliomas. Int. J. Radiat. Oncol. 2014, 89, 1060–1068. [Google Scholar] [CrossRef]
- Klein, M.; Drijver, A.J.; Bent, M.J.v.D.; Bromberg, J.C.; Hoang-Xuan, K.; Taphoorn, M.J.B.; Reijneveld, J.C.; Ben Hassel, M.; Vauleon, E.; Eekers, D.B.P.; et al. Memory in low-grade glioma patients treated with radiotherapy or temozolomide: A correlative analysis of EORTC study 22033–26033. Neuro Oncol. 2021, 23, 803–811. [Google Scholar] [CrossRef] [PubMed]
- van der Weide, H.L.; Kramer, M.C.; Scandurra, D.; Eekers, D.B.; Klaver, Y.L.; Wiggenraad, R.G.; Romero, A.M.; Coremans, I.E.; Boersma, L.; van Vulpen, M.; et al. Proton therapy for selected low grade glioma patients in the Netherlands. Radiother. Oncol. 2021, 154, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Shih, H.A.; Sherman, J.C.; Nachtigall, L.B.; Colvin, M.K.; Fullerton, B.C.; Daartz, J.; Winrich, B.K.; Batchelor, T.T.; Thornton, L.T.; Mancuso, S.M.; et al. Proton therapy for low-grade gliomas: Results from a prospective trial. Cancer 2015, 121, 1712–1719. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, T.S.; Dirven, L.; Arons, D.; Bates, A.; Chang, S.M.; Coens, C.; Espinasse, C.; Gilbert, M.R.; Jenkinson, D.; Kluetz, P.; et al. Glioma patient-reported outcome assessment in clinical care and research: A Response Assessment in Neuro-Oncology collaborative report. Lancet Oncol. 2020, 21, e97–e103. [Google Scholar] [CrossRef]
- Dirven, L.; Vos, M.E.; Walbert, T.; Armstrong, T.S.; Arons, D.; Bent, M.J.v.D.; Blakeley, J.; Brown, P.D.; Bulbeck, H.; Chang, S.M.; et al. Systematic review on the use of patient-reported outcome measures in brain tumor studies: Part of the Response Assessment in Neuro-Oncology Patient-Reported. Neuro Oncol. 2021, 8, 417–425. Available online: https://academic.oup.com/nop/article-abstract/8/4/417/6134357 (accessed on 17 October 2023). [CrossRef]
- Lombard, A.; Duffau, H. Sexual Dysfunction of Patients with Diffuse Low-Grade Glioma: A Qualitative Review of a Neglected Concern. Cancers 2022, 14, 3025. [Google Scholar] [CrossRef]
- Greimel, E.; Nagele, E.; Lanceley, A.; Oberguggenberger, A.S.; Nordin, A.; Kuljanic, K.; Arraras, J.I.; Wei-Chu, C.; Jensen, P.T.; Tomaszewski, K.A.; et al. Psychometric validation of the European Organisation for Research and Treatment of Cancer–Quality of Life Questionnaire Sexual Health (EORTC QLQ-SH22). Eur. J. Cancer 2021, 154, 235–245. [Google Scholar] [CrossRef]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Groenvold, M.; Klee, M.C.; Sprangers, M.A.; Aaronson, N.K. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J. Clin. Epidemiol. 1997, 50, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Taphoorn, M.J.; Claassens, L.; Aaronson, N.K.; Coens, C.; Mauer, M.; Osoba, D.; Stupp, R.; Mirimanoff, R.O.; Bent, M.J.v.D.; Bottomley, A. An international validation study of the EORTC brain cancer module (EORTC QLQ-BN20) for assessing health-related quality of life and symptoms in brain cancer patients. Eur. J. Cancer 2010, 46, 1033–1040. [Google Scholar] [CrossRef] [PubMed]
- Frey, K.; Unholtz, D.; Bauer, J.; Debus, J.; Min, C.H.; Bortfeld, T.; Paganetti, H.; Parodi, K. Automation and uncertainty analysis of a method for in-vivo range verification in particle therapy. Phys. Med. Biol. 2014, 59, 5903–5919. [Google Scholar] [CrossRef]
- Nolte, S.; Liegl, G.; Petersen, M.; Aaronson, N.; Costantini, A.; Fayers, P.; Groenvold, M.; Holzner, B.; Johnson, C.; Kemmler, G.; et al. General population normative data for the EORTC QLQ-C30 health-related quality of life questionnaire based on 15,386 persons across 13 European countries, Canada and the Unites States. Eur. J. Cancer 2019, 107, 153–163. [Google Scholar] [CrossRef]
- Baumert, B.G.; Hegi, M.E.; Bent, M.J.v.D.; von Deimling, A.; Gorlia, T.; Hoang-Xuan, K.; Brandes, A.A.; Kantor, G.; Taphoorn, M.J.B.; Ben Hassel, M.; et al. Temozolomide chemotherapy versus radiotherapy in high-risk low-grade glioma (EORTC 22033-26033): A randomised, open-label, phase 3 intergroup study. Lancet Oncol. 2016, 17, 1521–1532. [Google Scholar] [CrossRef]
- Fisher, B.J.; Pugh, S.L.; Macdonald, D.R.; Chakravatri, A.; Lesser, G.J.; Fox, S.; Rogers, C.L.; Werner-Wasik, M.; Doyle, T.; Bahary, J.P.; et al. Phase 2 Study of a Temozolomide-Based Chemora-diation Therapy Regimen for High-Risk, Low-Grade Gliomas: Long-Term Results of Radiation Therapy Oncology Group 0424. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 720–725. [Google Scholar] [CrossRef]
- McDuff, S.G.R.; Dietrich, J.; Atkins, K.M.; Oh, K.S.; Loeffler, J.S.; Shih, H.A. Radiation and chemotherapy for high-risk lower grade gliomas: Choosing between temozolomide and PCV. Cancer Med. 2020, 9, 3–11. [Google Scholar] [CrossRef]
- Indelicato, D.J.; Rotondo, R.L.; Uezono, H.; Sandler, E.S.; Aldana, P.R.; Ranalli, N.J.; Beier, A.D.; Morris, C.G.; Bradley, J.A. Outcomes Following Proton Therapy for Pe-diatric Low-Grade Glioma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 149–156. [Google Scholar] [CrossRef]
- Kamran, S.C.; Dworkin, M.; Niemierko, A.; Bussiere, M.; Oh, K.S.; Loeffler, J.S.; Shih, H.A. Patterns of Failure among Patients with Low-grade Glioma Treated with Proton Radiation Therapy. Pract. Radiat. Oncol. 2019, 9, e356–e361. [Google Scholar] [CrossRef]
- A Lawrie, T.; Gillespie, D.; Dowswell, T.; Evans, J.; Erridge, S.; Vale, L.; Kernohan, A.; Grant, R. Long-term neurocognitive and other side effects of radiotherapy, with or without chemotherapy, for glioma. Cochrane Database Syst. Rev. 2019, 8, CD013047. [Google Scholar] [CrossRef] [PubMed]
- Harrabi, S.B.; Bougatf, N.; Mohr, A.; Haberer, T.; Herfarth, K.; Combs, S.E.; Debus, J.; Adeberg, S. Dosimetric advantages of proton therapy over con-ventional radiotherapy with photons in young patients and adults with low-grade glioma. Strahlenther. Onkol. 2016, 192, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, S.; Yeap, B.Y.; Sherman, J.C.; Nachtigall, L.B.; Colvin, M.K.; Dworkin, M.; Fullerton, B.C.; Daartz, J.; Royce, T.J.; Oh, K.S.; et al. Long-term outcomes and late adverse effects of a prospective study on proton radiotherapy for patients with low-grade glioma. Radiother. Oncol. 2019, 137, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Sherman, J.C.; Colvin, M.K.; Mancuso, S.M.; Batchelor, T.T.; Oh, K.S.; Loeffler, J.S.; Yeap, B.Y.; Shih, H.A. Neurocognitive effects of proton radiation therapy in adults with low-grade glioma. J. Neuro Oncol. 2016, 126, 157–164. [Google Scholar] [CrossRef]
- Surbeck, W.; Herbet, G.; Duffau, H. Sexuality after surgery for diffuse low-grade glioma. Neuro Oncol. 2015, 17, 574–579. [Google Scholar] [CrossRef]
- Finocchiaro, C.Y.; Petruzzi, A.; Fedeli, G.; Vistalli, M.G.; Innocenti, A.; Silvani, A.; Lamperti, E. Hidden reality: Sexual sphere in brain tumor patients. Psychol. Health Med. 2017, 22, 370–380. [Google Scholar] [CrossRef]
- Boccia, M.L.; Anyanda, E.I.; Fonkem, E. A Preliminary Report on Quality of Life and Sexual Function in Brain Tumor Patients. J. Sex. Med. 2021, 18, 737–742. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (N = 89) |
|---|---|
| Age | |
| Median (IQR) in years | 25.4 (12.3–38.1) |
| Sex | |
| female | 49 (55.1%) |
| male | 40 (44.9%) |
| Subtype | |
| Oligodendroglioma | 21 (23.6%) |
| Astrocytoma | 27 (30.3%) |
| Oligoastrocytoma | 2 (2.2%) |
| Pilocytic | 21 (23.6%) |
| Pilomyxoid | 6 (6.7%) |
| Other/unknown | 12 (13.5%) |
| WHO grade | |
| 2 | 58 (65.2%) |
| 1 | 17 (19.1%) |
| Unknown or radiographically diagnosed | 14 (15.7%) |
| Location | |
| Frontotemporal | 31 (34.8%) |
| Visual/thalamic | 43 (48.3%) |
| Other | 15 (16.9%) |
| Laterality | |
| Right | 27 (30.3%) |
| Left | 25 (28.1%) |
| Central | 37 (41.6%) |
| IDH status | |
| Wild type | 4 (4.5%) |
| Mutated | 47 (52.8%) |
| Unknown | 38 (42.7%) |
| 1p19q status | |
| Wild type | 18 (20.2%) |
| Co-deleted | 17 (19.1%) |
| Unknown | 54 (60.7%) |
| Neurofibromatosis type 1 | |
| No | 85 (95.5%) |
| Yes | 4 (4.5%) |
| Pathology confirmation | |
| Radiological | 10 (11.2%) |
| Biopsy | 18 (20.2%) |
| Surgery | 61 (68.5%) |
| Tumor type | |
| Primary | 46 (51.7%) |
| Recurrence/progression | 43 (48.3%) |
| Treatment indication | |
| Primary, definitive | 18 (20.2%) |
| Primary, postoperative | 28 (31.5%) |
| Recurrence/progression, definitive | 33 (37.1%) |
| Recurrence/progression, postoperative | 10 (11.2%) |
| Radiotherapy dose | |
| Median (interquartile range; range) in Gy (RBE) | 54 (52.2–54; 46–64) |
| Previous chemotherapy | |
| No | 65 (73.0%) |
| Yes | 24 (27.0%) |
| Concomitant chemotherapy | |
| No | 85 (95.5%) |
| Yes | 4 (4.5%) |
| Adjuvant chemotherapy | |
| No | 61 (68.5%) |
| Yes | 28 (31.5%) |
| Current Study | Reference | |||||
|---|---|---|---|---|---|---|
| Total | Mean | Standard Deviation | Total | Mean | Standard Deviation | |
| Sexual satisfaction | 14 | 44.86 | 22.77 | 152 | 42.80 | 26.39 |
| Sexual pain | 12 | 6.57 | 13.79 | 151 | 19.98 | 27.50 |
| Importance of sexual activity | 14 | 36.11 | 33.21 | 153 | 45.53 | 32.84 |
| Decreased libido | 14 | 41.67 | 35.18 | 153 | 46.84 | 36.56 |
| Worry incontinence | 14 | 13.89 | 26.43 | 154 | 17.97 | 29.80 |
| Fatigue | 14 | 36.11 | 33.21 | 151 | 37.97 | 35.70 |
| Treatment effect on sexuality | 13 | 30.56 | 33.21 | 152 | 51.32 | 39.47 |
| Communication with professionals | 14 | 91.67 | 20.72 | 151 | 17.44 | 29.02 |
| Insecurity with partner | 13 | 25.00 | 28.87 | 144 | 29.63 | 35.06 |
| Confidence erection | 5 | 25.00 | 31.92 | 55 | 39.39 | 37.46 |
| Body image (male) | 5 | 16.67 | 19.24 | 56 | 39.88 | 35.63 |
| Vaginal dryness | 9 | 37.50 | 37.53 | 88 | 46.21 | 39.93 |
| Body image female | 9 | 25.00 | 29.55 | 96 | 34.03 | 37.14 |
| First Author, Year | Design | Patients | Main Inclusion Criteria | Median Follow-Up (Years) | Outcomes | Toxicity |
|---|---|---|---|---|---|---|
| Shih, 2015 [16] | Prospective single-arm | 20 | LGG WHO grade 2 ≥19 years of age No baseline cognitive deficits to compromise neurocognitive assessment No prior cranial irradiation | 5.1 | PFS at 3 years 85%, at 5 years 40% | No changes in QoL, cognitive function Baseline neurocognitive impairment in 8 patients New endocrine dysfunction in 6 patients |
| Greenberger, 2014 [13] | Retrospective database | 32 | LGG WHO 1 and 2 Location in brain or spinal cord ≤21 years of age | 7.6 | PFS at 6 years 89.7%, at 8-year 82.8% OS at 8 years 100% | No significant declines in neurocognition Subgroup analysis indicated significant neurocognitive decline for young children (<7 years) and those with higher dose to the left temporal lobe/hippocampus |
| Indelicato, 2019 [29] | Prospective single-arm | 174 | LGG WHO 1 and 2 Location in brain or spinal cord ≤21 years of age | 4.4 | 5-year actuarial local control 85% 5-year actuarial PFS 84% 5-year actuarial OS 92% | 4% of patients with serious toxicities, including brainstem necrosis requiring corticosteroids, symptomatic vasculopathy, radiation retinopathy, epilepsy, and death from radiation-induced high-grade glioma Central hormone deficiency in 39 patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willmann, J.; Leiser, D.; Weber, D.C. Oncological Outcomes, Long-Term Toxicities, Quality of Life and Sexual Health after Pencil-Beam Scanning Proton Therapy in Patients with Low-Grade Glioma. Cancers 2023, 15, 5287. https://doi.org/10.3390/cancers15215287
Willmann J, Leiser D, Weber DC. Oncological Outcomes, Long-Term Toxicities, Quality of Life and Sexual Health after Pencil-Beam Scanning Proton Therapy in Patients with Low-Grade Glioma. Cancers. 2023; 15(21):5287. https://doi.org/10.3390/cancers15215287
Chicago/Turabian StyleWillmann, Jonas, Dominic Leiser, and Damien Charles Weber. 2023. "Oncological Outcomes, Long-Term Toxicities, Quality of Life and Sexual Health after Pencil-Beam Scanning Proton Therapy in Patients with Low-Grade Glioma" Cancers 15, no. 21: 5287. https://doi.org/10.3390/cancers15215287
APA StyleWillmann, J., Leiser, D., & Weber, D. C. (2023). Oncological Outcomes, Long-Term Toxicities, Quality of Life and Sexual Health after Pencil-Beam Scanning Proton Therapy in Patients with Low-Grade Glioma. Cancers, 15(21), 5287. https://doi.org/10.3390/cancers15215287