

A Phase I Trial of Sirolimus with “7&3” Induction Chemotherapy in Patients with Newly Diagnosed Acute Myeloid Leukemia

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Trial Eligibility
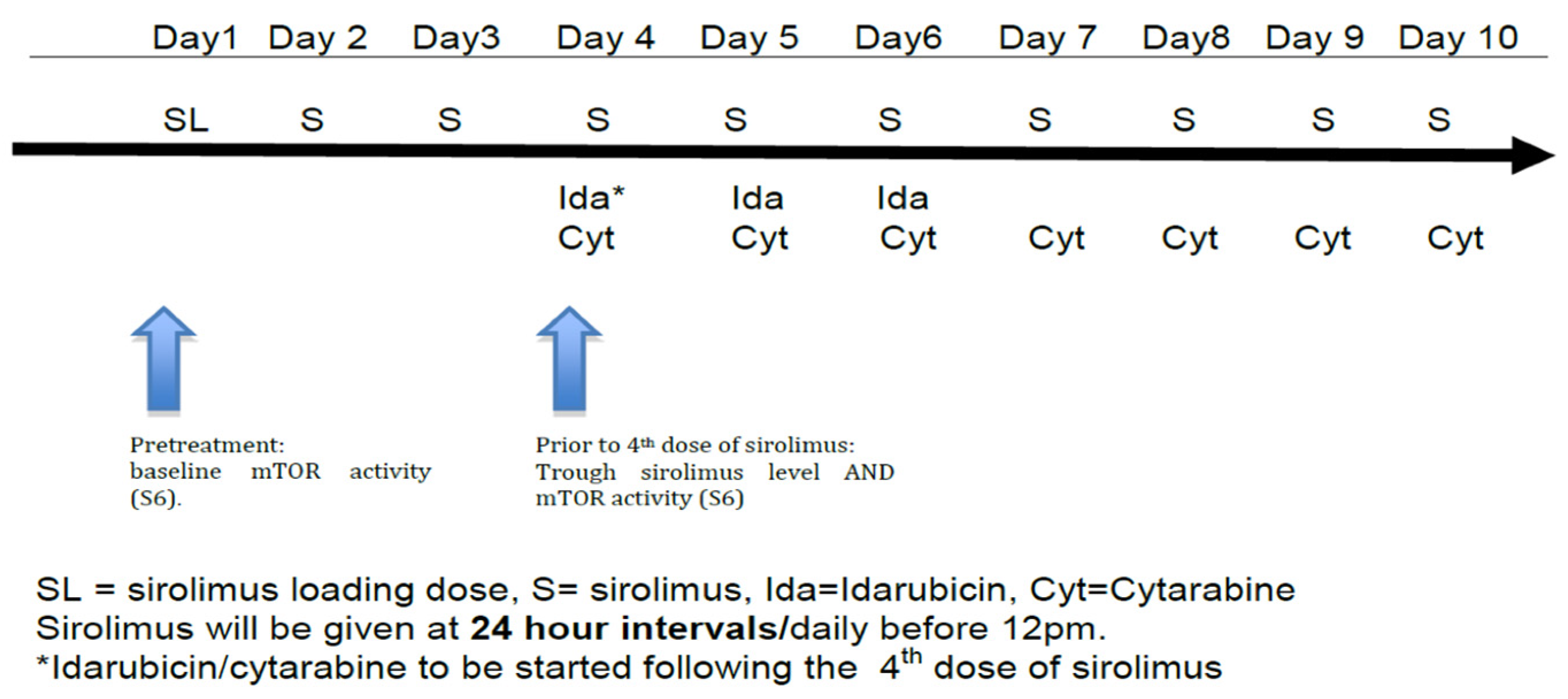
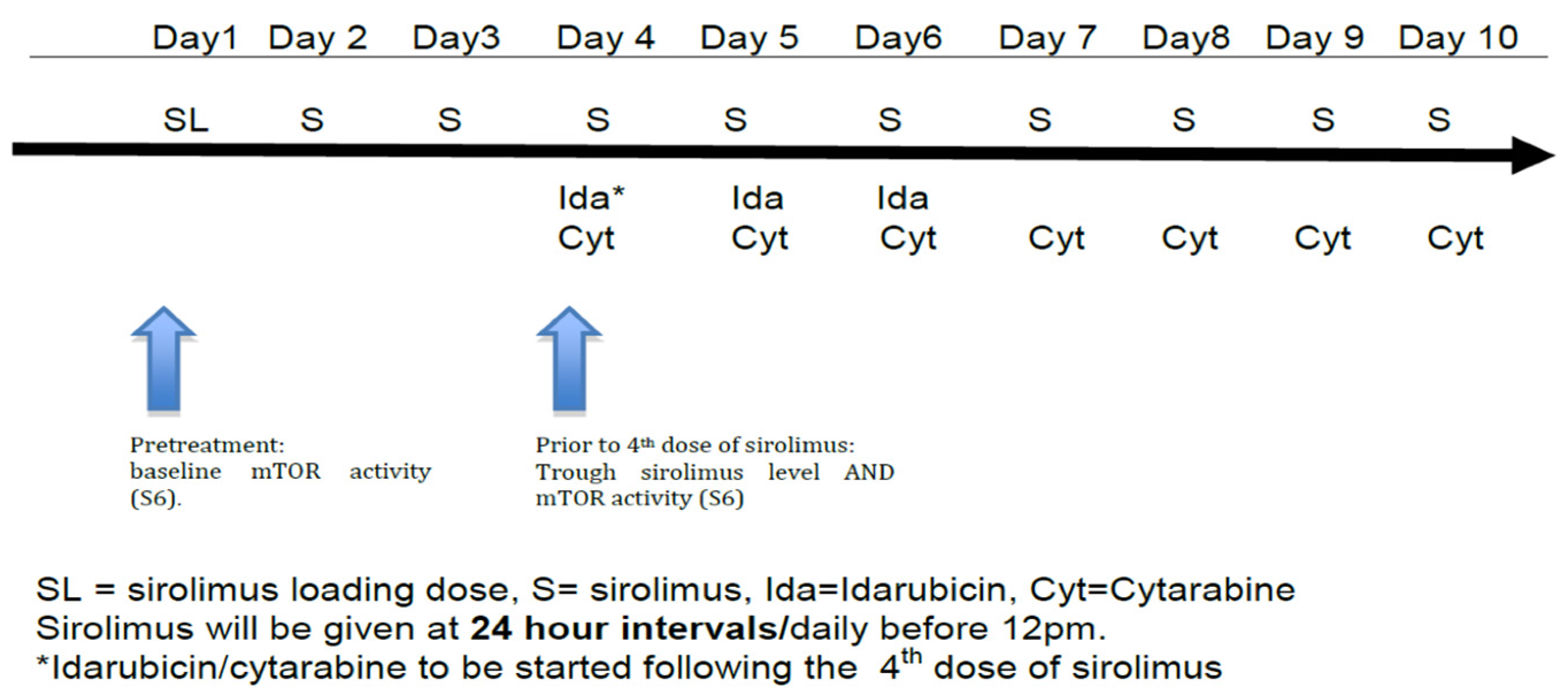
2.2. Treatment Plan
2.3. Clinical Response and Toxicities
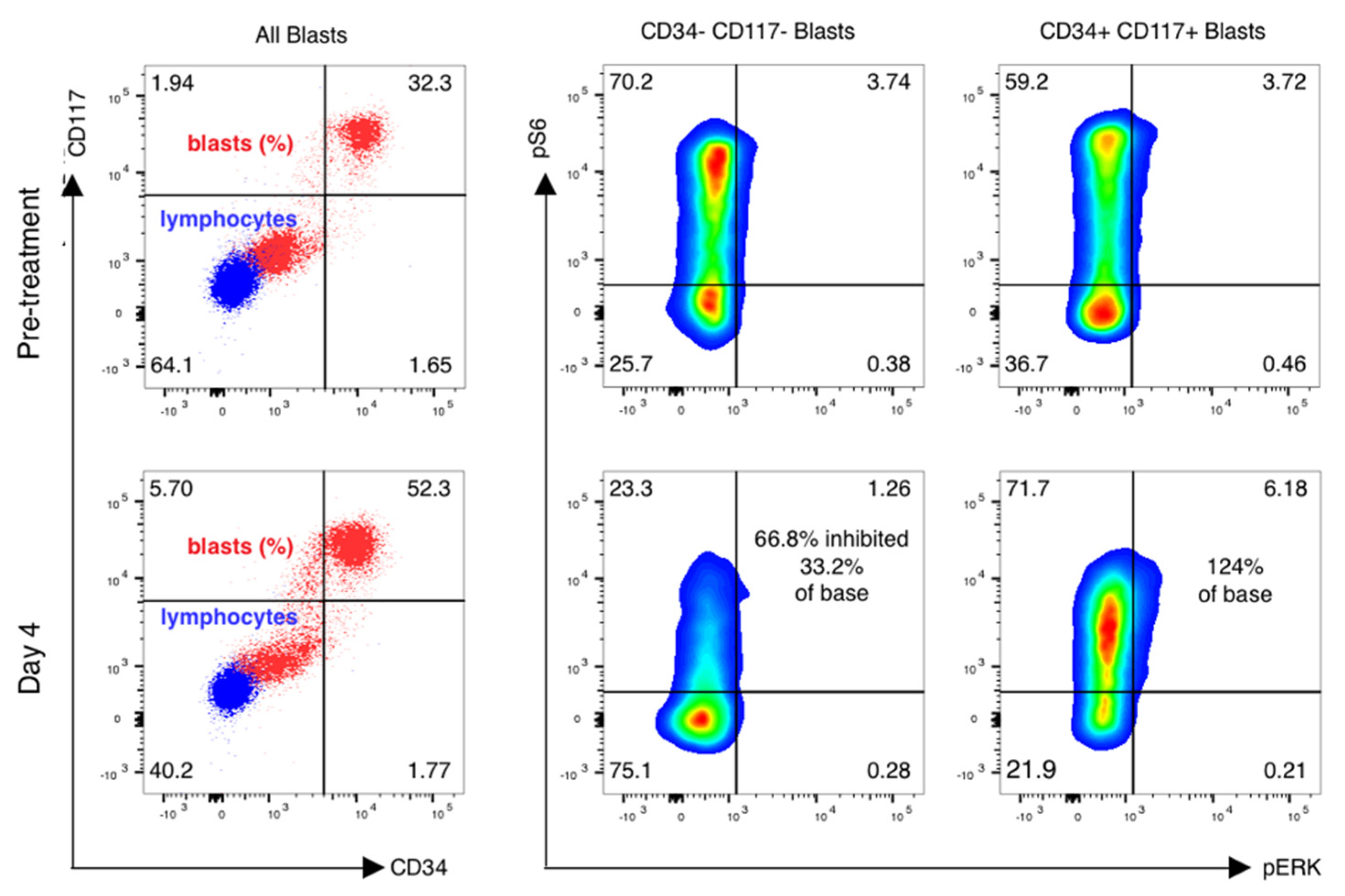
2.4. Therapeutic Drug Monitoring and Pharmacodynamics
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raj, R.V.; Abedin, S.M.; Atallah, E. Incorporating newer agents in the treatment of acute myeloid leukemia. Leuk. Res. 2018, 74, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.M.; Mandrekar, S.J.; Sanford, B.L.; Laumann, K.; Geyer, S.; Bloomfield, C.D.; Thiede, C.; Prior, T.W.; Döhner, K.; Marcucci, G.; et al. Midostaurin plus chemotherapy for acute myeloid leukemia with a FLT3 mutation. N. Engl. J. Med. 2017, 377, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Büchner, T.; Schlenk, R.F.; Schaich, M.; Döhner, K.; Krahl, R.; Krauter, J.; Heil, G.; Krug, U.; Sauerland, M.C.; Heinecke, A.; et al. Acute myeloid leukemia (AML): Different treatment strategies versus a common standard Arm—Combined prospective analysis by the German AML intergroup. J. Clin. Oncol. 2012, 30, 3604–3610. [Google Scholar] [CrossRef]
- Zeidner, J.F.; Foster, M.C.; Blackford, A.L.; Litzow, M.R.; Morris, L.E.; Strickland, S.A.; Lancet, J.E.; Bose, P.; Levy, M.Y.; Tibes, R.; et al. Randomized multicenter phase II study of flavopiridol (alvocidib), cytarabine, and mitoxantrone (FLAM) versus cytarabine/daunorubicin (7+3) in newly diagnosed acute myeloid leukemia. Haematologica 2015, 100, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.; Short, N.J.; Ravandi, F.; Huang, X.; Xiao, L.; Garcia-Manero, G.; Plunkett, W.; Gandhi, V.; Sasaki, K.; Pemmaraju, N.; et al. A randomized phase 2 study of idarubicin and cytarabine with clofarabine or fludarabine in patients with newly diagnosed acute myeloid leukemia. Cancer 2017, 123, 4430–4439. [Google Scholar] [CrossRef] [PubMed]
- Wullschleger, S.; Loewith, R.; Hall, M.N. TOR signaling in growth and metabolism. Cell 2006, 124, 471–484. [Google Scholar] [CrossRef] [PubMed]
- DiNardo, C.D.; Ravandi, F.; Agresta, S.; Konopleva, M.; Takahashi, K.; Kadia, T.; Routbort, M.; Patel, K.P.; Brandt, M.; Pierce, S.; et al. Characteristics, clinical outcome, and prognostic significance of IDH mutations in AML. Am. J. Hematol. 2015, 90, 732–736. [Google Scholar] [CrossRef]
- Edinger, A.L.; Thompson, C.B.; Raff, M. Akt maintains cell size and survival by increasing mTOR-dependent nutrient uptake. Mol. Biol. Cell 2002, 13, 2276–2288. [Google Scholar] [CrossRef]
- Zhao, S.; Konopleva, M.; Cabreira-Hansen, M.; Xie, Z.; Hu, W.; Milella, M.; Estrov, Z.; Mills, G.B.; Andreeff, M. Inhibition of phosphatidylinositol 3-kinase dephosphorylates BAD and promotes apoptosis in myeloid leukemias. Leukemia 2003, 18, 267. [Google Scholar] [CrossRef]
- Bardet, V.; Tamburini, J.; Ifrah, N.; Dreyfus, F.; Mayeux, P.; Bouscary, D.; Lacombe, C. Single cell analysis of phosphoinositide 3-kinase/akt and ERK activation in acute myeloid leukemia by flow cytometry. Haematologica 2006, 91, 757–764. [Google Scholar]
- Thompson, J.E.; Thompson, C.B. Putting the rap on akt. J. Clin. Oncol. 2004, 22, 4217–4226. [Google Scholar] [CrossRef] [PubMed]
- Ley, T.J. Genomic and Epigenomic Landscapes of Adult De Novo Acute Myeloid Leukemia. N. Engl. J. Med. 2013, 368, 2059–2074. [Google Scholar] [PubMed]
- Laplante, M.; Sabatini, D. mTOR signaling in growth control and disease. Cell 2012, 149, 274–293. [Google Scholar] [CrossRef]
- Klawitter, J.; Nashan, B.; Christians, U. Everolimus and sirolimus in transplantation-related but different. Expert Opin. Drug Saf. 2015, 14, 1055–1070. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Thompson, J.E.; Carroll, M. mTOR regulates cell survival after etoposide treatment in primary AML cells. Blood 2005, 106, 4261–4268. [Google Scholar] [CrossRef]
- Perl, A.E.; Kasner, M.T.; Tsai, D.E.; Vogl, D.T.; Loren, A.W.; Schuster, S.J.; Porter, D.L.; Stadtmauer, E.A.; Goldstein, S.C.; Frey, N.V.; et al. A phase I study of the mammalian target of rapamycin inhibitor sirolimus and MEC chemotherapy in relapsed and refractory acute myelogenous leukemia. Clin. Cancer Res. 2009, 15, 6732–6739. [Google Scholar] [CrossRef]
- Perl, A.E.; Kasner, M.T.; Shank, D.; Luger, S.M.; Carroll, M. Single-cell pharmacodynamic monitoring of S6 ribosomal protein phosphorylation in AML blasts during a clinical trial combining the mTOR inhibitor sirolimus and intensive chemotherapy. Clin. Cancer Res. 2012, 18, 1716–1725. [Google Scholar] [CrossRef]
- Teachey, D.T.; Obzut, D.A.; Cooperman, J.; Fang, J.; Carroll, M.; Choi, J.K.; Houghton, P.J.; Brown, V.I.; Grupp, S.A. The mTOR inhibitor CCI-779 induces apoptosis and inhibits growth in preclinical models of primary adult human ALL. Blood 2006, 107, 1149–1155. [Google Scholar] [CrossRef]
- Park, S.; Chapuis, N.; Saint Marcoux, F.; Recher, C.; Prebet, T.; Chevallier, P.; Cahn, J.Y.; Leguay, T.; Bories, P.; Witz, F.; et al. A phase Ib GOELAMS study of the mTOR inhibitor RAD001 in association with chemotherapy for AML patients in first relapse. Leukemia 2013, 27, 1479–1486. [Google Scholar] [CrossRef]
- Daver, N.; Boumber, Y.; Kantarjian, H.; Ravandi, F.; Cortes, J.; Rytting, M.E.; Kawedia, J.D.; Basnett, J.; Culotta, K.S.; Zeng, Z.; et al. A Phase I/II Study of the mTOR Inhibitor Everolimus in Combination with HyperCVAD Chemotherapy in Patients with Relapsed/Refractory Acute Lymphoblastic Leukemia. Clin. Cancer Res. 2015, 21, 2704–2714. [Google Scholar] [CrossRef]
- Amadori, S.; Stasi, R.; Martelli, A.M.; Venditti, A.; Meloni, G.; Pane, F.; Martinelli, G.; Lunghi, M.; Pagano, L.; Cilloni, D.; et al. Temsirolimus, an mTOR inhibitor, in combination with lower-dose clofarabine as salvage therapy for older patients with acute myeloid leukaemia: Results of a phase II GIMEMA study (AML-1107). Br. J. Haematol. 2012, 156, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Oki, T.; Mercier, F.; Kato, H.; Jung, Y.; McDonald, T.O.; Spencer, J.A.; Mazzola, M.C.; van Gastel, N.; Lin, C.P.; Michor, F.; et al. Imaging dynamic mTORC1 pathway activity in vivo reveals marked shifts that support time-specific inhibitor therapy in AML. Nat. Commun. 2021, 12, 245. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the eastern cooperative oncology group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, S.; Tan, Y.; Chen, J. The effects of idarubicin versus other anthracyclines for induction therapy of patients with newly diagnosed leukaemia. Cochrane Database Syst. Rev. 2015, CD010432. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Bennett, J.M.; Kopecky, K.J.; Büchner, T.; Willman, C.L.; Estey, E.H.; Schiffer, C.A.; Doehner, H.; Tallman, M.S.; Lister, T.A.; et al. Revised recommendations of the international working group for diagnosis, standardization of response criteria, treatment outcomes, and reporting standards for therapeutic trials in acute myeloid leukemia. J. Clin. Oncol. 2003, 21, 4642–4649. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef]
- Ohtake, S.; Miyawaki, S.; Fujita, H.; Kiyoi, H.; Shinagawa, K.; Usui, N.; Okumura, H.; Miyamura, K.; Nakaseko, C.; Miyazaki, Y.; et al. Randomized study of induction therapy comparing standard-dose idarubicin with high-dose daunorubicin in adult patients with previously untreated acute myeloid leukemia: The JALSG AML201 study. Blood 2011, 117, 2358–2365. [Google Scholar] [CrossRef]
- Kasner, M.T.; Mick, R.; Jeschke, G.R.; Carabasi, M.; Filicko-O’Hara, J.; Flomenberg, N.; Frey, N.V.; Hexner, E.O.; Luger, S.M.; Loren, A.W.; et al. Sirolimus enhances remission induction in patients with high risk acute myeloid leukemia and mTORC1 target inhibition. Investig. New Drugs 2018, 36, 657–666. [Google Scholar] [CrossRef]
- Zeng, Z.; Shi, Y.X.; Tsao, T.; Qiu, Y.; Kornblau, S.M.; Baggerly, K.A.; Liu, W.; Jessen, K.; Liu, Y.; Kantarjian, H.; et al. Targeting of mTORC1/2 by the mTOR kinase inhibitor PP242 induces apoptosis in AML cells under conditions mimicking the bone marrow microenvironment. Blood 2012, 120, 2679–2689. [Google Scholar] [CrossRef]
- Peterson, T.R.; Laplante, M.; Thoreen, C.C.; Sancak, Y.; Kang, S.A.; Kuehl, W.M.; Gray, N.S.; Sabatini, D.M. DEPTOR is an mTOR inhibitor frequently overexpressed in multiple myeloma cells and required for their survival. Cell 2009, 137, 873–886. [Google Scholar] [CrossRef]
- Pignochino, Y.; Dell’Aglio, C.; Basiricò, M.; Capozzi, F.; Soster, M.; Marchiò, S.; Bruno, S.; Gammaitoni, L.; Sangiolo, D.; Torchiaro, E.; et al. The combination of sorafenib and everolimus abrogates mTORC1 and mTORC2 upregulation in osteosarcoma preclinical models. Clin. Cancer Res. 2013, 19, 2117–2131. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Harkavy, B.; Shen, N.; Grohar, P.; Helman, L.J. Rapamycin induces feedback activation of Akt signaling through an IGF-1R-dependent mechanism. Oncogene 2007, 26, 1932–1940. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, E.; Meng, C.; Case, A.E.; Tiv, H.L.; Gokhale, P.C.; Buhrlage, S.J.; Yang, J.; Liu, X.; Wang, J.; Gray, N.; et al. Effects of the multi-kinase inhibitor midostaurin in combination with chemotherapy in models of acute myeloid leukaemia. J. Cell. Mol. Med. 2020, 24, 2968–2980. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AML | =55 |
| Age—median | 26 (21–75%) |
| Gender | |
| Male | 34 (62%) |
| Female | 21 (38%) |
| Disease status at diagnosis | |
| De novo | 50 (91%) |
| sAML/tAML | 5 (9%) |
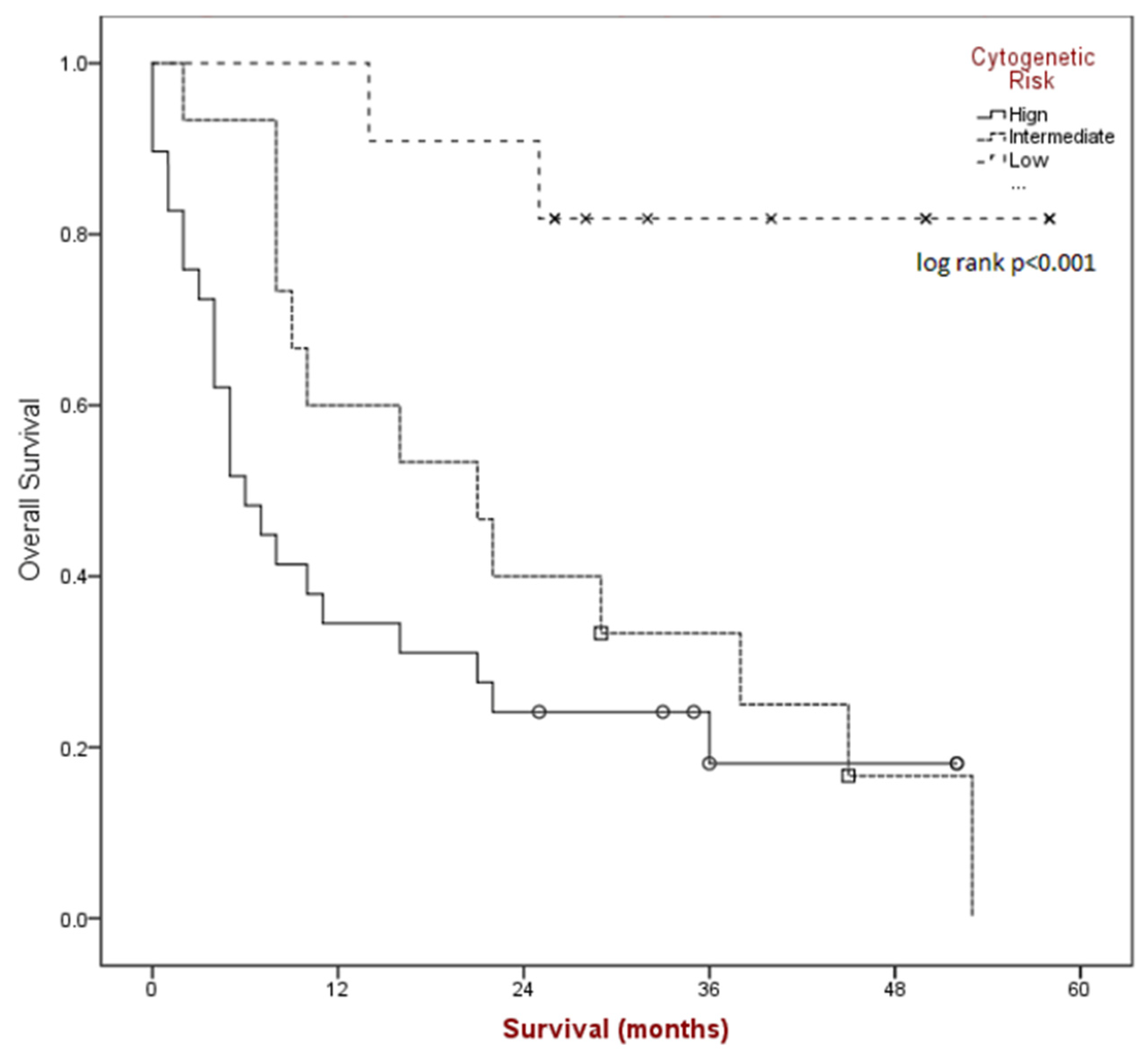
| Risk Classification | |
| Favorable | 11 (20%) |
| Intermediate | 15 (27%) |
| Poor | 29 (53%) |
| All Grades | Grade 3/4 | |||
|---|---|---|---|---|
| N | % | N | % | |
| Diarrhea | 32 | 58.2 | 0 | 0 |
| Febrile Neutropenia | 28 | 50.9 | 21 | 38.2 |
| Nausea | 28 | 50.9 | 0 | 0 |
| Anorexia | 24 | 43.6 | 1 | 1.8 |
| Mucositis | 17 | 30.9 | 1 | 1.8 |
| Rash | 16 | 29.1 | 1 | 1.8 |
| Vomiting | 16 | 29.1 | 0 | 0 |
| Hyperglycemia | 15 | 27.3 | 0 | 0 |
| Hyperbilirubinemia | 13 | 23.6 | 3 | 5.5 |
| Hypokalemia | 13 | 23.6 | 2 | 3.6 |
| Elevated ALT | 12 | 21.8 | 1 | 1.8 |
| Fatigue | 12 | 21.8 | 0 | 0 |
| Coagulopathy | 11 | 20 | 0 | 0 |
| Hypophosphatemia | 10 | 18.2 | 6 | 10.9 |
| Acute Kidney Injury | 9 | 16.4 | 1 | 1.8 |
| Constipation | 9 | 16.4 | 1 | 1.8 |
| Hypertension | 9 | 16.4 | 5 | 9.1 |
| Epistaxis | 8 | 14.5 | 0 | 0 |
| Elevated Alkaline Phosphatase | 7 | 12.7 | 0 | 0 |
| Hypocalcemia | 7 | 12.7 | 1 | 1.8 |
| Hyponatremia | 7 | 12.7 | 1 | 1.8 |
| Pneumonia | 7 | 12.7 | 6 | 10.9 |
| Abdominal pain | 6 | 10.9 | 1 | 1.8 |
| Elevated AST | 6 | 10.9 | 1 | 1.8 |
| Hematuria | 6 | 10.9 | 0 | 0 |
| Sore throat | 6 | 10.9 | 0 | 0 |
| High Risk (n = 29) | Intermediate Risk (n = 15) | Favorable Risk (n = 11) | Total (n = 55) | |
|---|---|---|---|---|
| CR/CRp | 13 | 11 | 11 | 35 (64%) |
| PR | 0 | 2 | 0 | 1 (2%) |
| Non-Response | 14 | 2 | 0 | 17 (30%) |
| Death in Aplasia | 2 | 0 | 0 | 2 (4%) |
| Phospho-Flow Data by Risk Category | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| High Risk | Intermediate Risk | Favorable Risk | All-Comers | ||||||
| n total | 29 | 15 | 11 | 55 | |||||
| n evaluable | 25 | 86% | 7 | 47% | 9 | 82% | 41 | 75% | of total |
| n active | 25 | 100% | 7 | 100% | 9 | 100% | 41 | 100% | of evaluable |
| n inhibited | 17 | 68% | 2 | 29% | 8 | 89% | 27 | 66% | of evaluable |
| CR[p], n | 13 | 45% | 11 | 73% | 11 | 100% | 35 | 64% | of total |
| CR, evaluable | 10 | 77% | 5 | 45% | 9 | 82% | 24 | 69% | of subset total |
| CR, inhibited | 5 | 50% | 2 | 40% | 8 | 89% | 15 | 63% | of evaluable |
| PR, n | 1 | 3% | 1 | 7% | 0 | 2 | 4% | of total | |
| PR, evaluable | 1 | 100% | 0 | 0% | 1 | 50% | of subset total | ||
| PR, inhibited | 0 | 0% | 0 | 0% | of evaluable | ||||
| NR, n | 13 | 45% | 3 | 20% | 0 | 16 | 29% | of total | |
| NR, evaluable | 12 | 92% | 2 | 67% | 14 | 88% | of subset total | ||
| NR, inhibited | 11 | 92% | 0 | 0% | 11 | 79% | of evaluable | ||
| died in aplasia | 2 | 7% | 0 | 0 | 2 | 4% | of total | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmisiano, N.; Jeschke, G.; Wilde, L.; Alpdogan, O.; Carabasi, M.; Filicko-O’Hara, J.; Grosso, D.; Klumpp, T.; Martinez, U.; Wagner, J.; et al. A Phase I Trial of Sirolimus with “7&3” Induction Chemotherapy in Patients with Newly Diagnosed Acute Myeloid Leukemia. Cancers 2023, 15, 5129. https://doi.org/10.3390/cancers15215129
Palmisiano N, Jeschke G, Wilde L, Alpdogan O, Carabasi M, Filicko-O’Hara J, Grosso D, Klumpp T, Martinez U, Wagner J, et al. A Phase I Trial of Sirolimus with “7&3” Induction Chemotherapy in Patients with Newly Diagnosed Acute Myeloid Leukemia. Cancers. 2023; 15(21):5129. https://doi.org/10.3390/cancers15215129
Chicago/Turabian StylePalmisiano, Neil, Grace Jeschke, Lindsay Wilde, Onder Alpdogan, Matthew Carabasi, Joanne Filicko-O’Hara, Dolores Grosso, Thomas Klumpp, Ubaldo Martinez, John Wagner, and et al. 2023. "A Phase I Trial of Sirolimus with “7&3” Induction Chemotherapy in Patients with Newly Diagnosed Acute Myeloid Leukemia" Cancers 15, no. 21: 5129. https://doi.org/10.3390/cancers15215129
APA StylePalmisiano, N., Jeschke, G., Wilde, L., Alpdogan, O., Carabasi, M., Filicko-O’Hara, J., Grosso, D., Klumpp, T., Martinez, U., Wagner, J., Carroll, M. P., Perl, A., & Kasner, M. (2023). A Phase I Trial of Sirolimus with “7&3” Induction Chemotherapy in Patients with Newly Diagnosed Acute Myeloid Leukemia. Cancers, 15(21), 5129. https://doi.org/10.3390/cancers15215129