
Influence of MRI Follow-Up on Treatment Decisions during Standard Concomitant and Adjuvant Chemotherapy in Patients with Glioblastoma: Is Less More?
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Extraction
2.2. MRI Acquisition
2.3. Statistical Analysis
3. Results
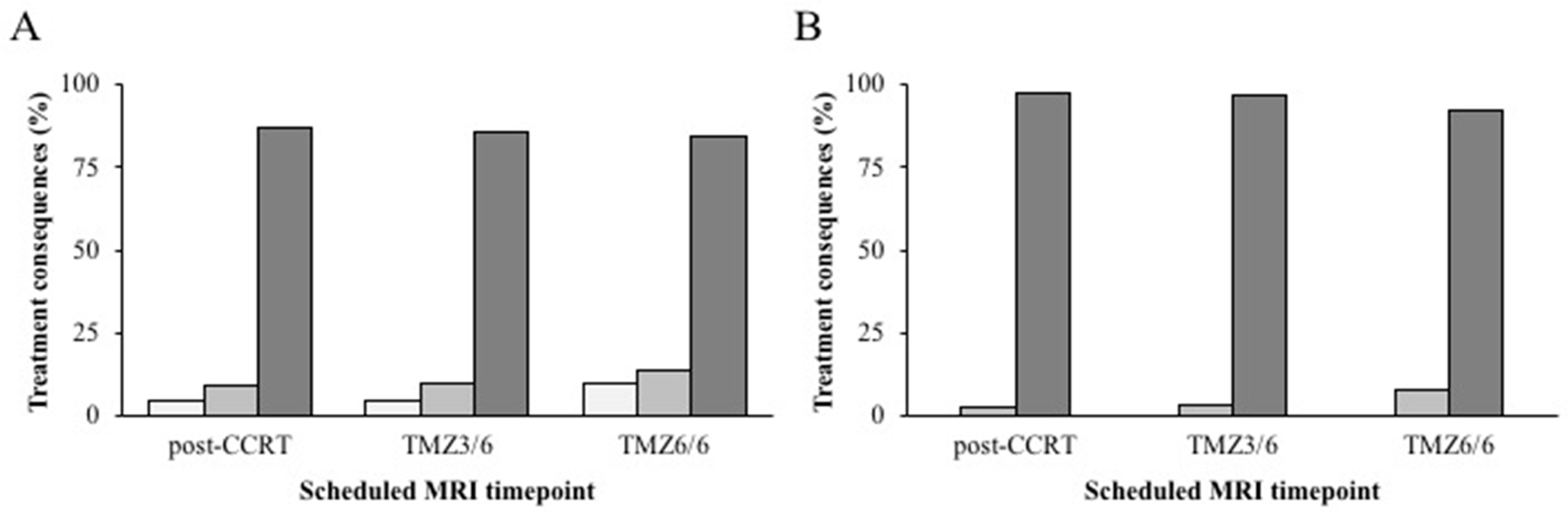
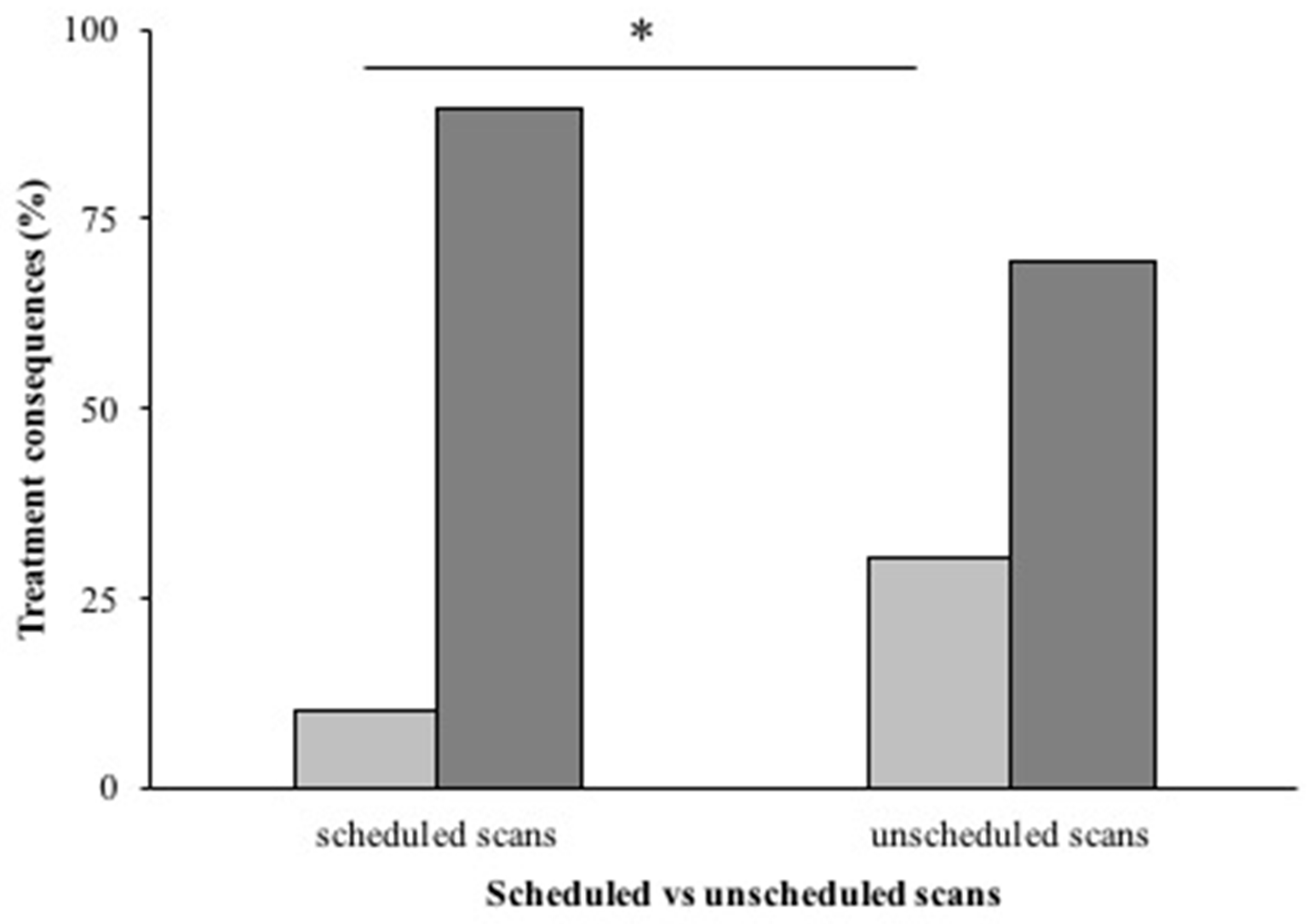
3.1. Treatment Consequences
3.2. Diagnostic Uncertainty on MRI
3.3. Perfusion Weighted Imaging
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.Y.; Lee, J.; Lee, J.H.; Lee, S.T.; Won, J.K.; Kim, J.W.; Kim, Y.H.; Kim, T.M.; Choi, S.H.; Park, S.H.; et al. Radiological assessment schedule for high-grade glioma patients during the surveillance period using parametric modeling. Neuro-Oncology 2021, 23, 837–847. [Google Scholar] [CrossRef]
- Lundy, P.; Domino, J.; Ryken, T.; Fouke, S.; McCracken, D.J.; Ormond, D.R.; Olsom, J.J. The role of imaging for the management of newly diagnosed glioblastoma in adults: A systematic review and evidence-based clinical practice guideline update. J. Neuro-Oncol. 2020, 150, 95–120. [Google Scholar] [CrossRef]
- Monroe, C.L.; Travers, S.; Woldu, H.G.; Litofsky, N.S. Does Surveillance-Detected Disease Progression Yield Superior Patient Outcomes in High-Grade Glioma? World Neurosurg. 2020, 135, e410–e417. [Google Scholar] [CrossRef]
- Brandsma, D.; Stalpers, L.; Taal, W.; Sminia, P.; van den Bent, M.J. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol. 2008, 9, 453–461. [Google Scholar] [CrossRef]
- Van Dijken, B.R.J.; van Laar, P.J.; Holtman, G.A.; van der Hoorn, A. Diagnostic accuracy of magnetic resonance imaging techniques for treatment response evaluation in patients with high-grade glioma, a systematic review and meta-analysis. Eur. Radiol. 2017, 27, 4129–4144. [Google Scholar] [CrossRef]
- Ellingson, B.M.; Chung, C.; Pope, W.B.; Boxerman, J.L.; Kaufmann, T.J. Pseudoprogression, radionecrosis, inflammation or true tumor progression? challenges associated with glioblastoma response assessment in an evolving therapeutic landscape. J. Neuro-Oncol. 2017, 134, 495–504. [Google Scholar] [CrossRef]
- Le Fèvre, C.; Constans, J.M.; Chambrelant, I.; Antoni, D.; Bund, C.; Lery-Freschini, B.; Schott, R.; Cebula, H.; Noël, G. Pseudoprogression versus true progression in glioblastoma patients: A multiapproach literature review. Part 2—Radiological features and metric markers. Crit. Rev. Oncol. Hematol. 2021, 159, 103230. [Google Scholar] [CrossRef]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; DeGroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.; Lawrie, T.A.; Kernohan, A.; Jenksinson, M.D. Interval brain imaging for adults with cerebral glioma. Cochrane Database Syst. Rev. 2019, 2019, CD013137. [Google Scholar] [CrossRef] [PubMed]
- Stensjøen, A.L.; Solheim, O.; Kvistad, K.A.; Håberg, A.K.; Salvesen, Ø.; Berntsen, E.M. Growth dynamics of untreated glioblastomas in vivo. Neuro-Oncology 2015, 17, 1402–1411. [Google Scholar] [CrossRef]
- Booth, T.C.; Luis, A.; Brazil, L.; Thompson, G.; Daniel, R.A.; Shuaib, H.; Ashkan, K.; Pandey, A. Glioblastoma post-operative imaging in neuro-oncology: Current UK practice (GIN CUP study). Eur. Radiol. 2020, 31, 2933–2943. [Google Scholar] [CrossRef]
- Gillespie, C.S.; Bligh, E.R.; Poon, M.T.C.; Solomou, G.; Islim, A.I.; Mustafa, M.A.; Rominiyi, O.; Williams, S.T.; Kalra, N.; Neurology and Neurosurgery Interest Group (NANSIG); et al. Imaging timing after glioblastoma surgery (INTERVAL-GB): Protocol for a UK and Ireland, multicentre retrospective cohort study. BMJ Open 2022, 12, e063043. [Google Scholar] [CrossRef]
- Mrowczynski, O.D.; Zammar, S.; Bourcier, A.J. Utility of Early Postoperative Magnetic Resonance Imaging After Glioblastoma Resection: Implications on Patient Survival. World Neurosurg. 2018, 120, e1171–e1174. [Google Scholar] [CrossRef] [PubMed]
- Sanai, N.; Polley, M.Y.; McDermottt, M.W.; Parsa, A.T.; Berger, M.S. An extent of resection threshold for newly diagnosed glioblastomas. J. Neurosurg. 2011, 115, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro-Oncology 2014, 16, 113–122. [Google Scholar] [CrossRef]
- Brown, T.J.; Brennan, M.C.; Li, M.; Church, E.W.; Brandmeir, N.J.; Rakszawski, K.L.; Patel, A.S.; Rizk, E.B.; Suki, D.; Sawaya, S.; et al. Association of the Extent of Resection with Survival in Glioblastoma: A Systematic Review and Meta-analysis. JAMA Oncol. 2016, 2, 1460–1469. [Google Scholar] [CrossRef]
- Prust, M.J.; Jafari-Khouzani, K.; Kalpathy-Cramer, J.; Polaskova, P.; Batchelor, T.T.; Gerstner, E.R.; Dietrich, J. Standard chemoradiation for glioblastoma results in progressive brain volume loss. Neurology 2015, 85, 683–691. [Google Scholar] [CrossRef]
- Petr, J.; Hofheinz, F.; Mutsaerts, H.J.M.M.; Asllani, I.; van Osch, M.J.P.; Seidlitz, A.; Krukowski, P.; Gommlich, A.; Beuthien-Baumann, B.; Jentsch, C.; et al. Photon vs. proton radiochemotherapy: Effects on brain tissue volume and perfusion. Radiother. Oncol. 2018, 128, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.W.; Westerlaan, H.E.; Holtman, G.A.; Aden, K.M.; van Laar, P.J.; van der Hoorn, A. Incidence of Tumour Progression and Pseudoprogression in High-Grade Gliomas: A Systematic Review and Meta-Analysis. Clin. Neuroradiol. 2018, 28, 401–411. [Google Scholar] [CrossRef]
- Thompson, C.A.; Charlson, M.E.; Schenkein, E. Surveillance CT scans are a source of anxiety and fear of recurrence in long-term lymphoma survivors. Ann. Oncol. 2010, 21, 2262–2266. [Google Scholar] [CrossRef]
- Goebel, S.; Mehdorn, H.M. Fear of disease progression in adult ambulatory patients with brain cancer: Prevalence and clinical correlates. Support. Care Cancer 2019, 27, 3521–3529. [Google Scholar] [CrossRef]
- Loughan, A.R.; Lanoye, A.; Aslanzadeh, F.J.; Villanueva, A.A.L.; Boutte, R.; Husain, M.; Braun, S. Fear of Cancer Recurrence and Death Anxiety: Unaddressed Concerns for Adult Neuro-oncology Patients. J. Clin. Psychol. Med. Settings 2021, 28, 16–30. [Google Scholar] [CrossRef]
- Bauml, J.M.; Troxel, A.; Epperson, C.N.; Cohen, R.B.; Schmitz, K.; Stricker, C.; Shulman, L.N.; Bradbury, A.; Mao, J.J.; Langer, C.J. Scan-Associated Distress in Lung Cancer: Quantifying the Impact of “Scanxiety”. Lung Cancer 2016, 100, 110–113. [Google Scholar] [CrossRef]
- Derry-Vick, H.M.; Heathcote, L.C.; Glesby, N.; Stribling, J.; Luebke, M.; Epstein, A.S.; Prigerson, H.G. Scanxiety among Adults with Cancer: A Scoping Review to Guide Research and Interventions. Cancers 2023, 15, 1381. [Google Scholar] [CrossRef]
- Booth, T.C.; Thompson, G.; Bulbeck, H.; Boele, F.; Buckley, C.; Cardoso, J.; Dos Santos Canas, L.; Jenkinson, D.; Ashkan, K.; Kreindler, J.; et al. A Position Statement on the Utility of Interval Imaging in Standard of Care Brain Tumour Management: Defining the Evidence Gap and Opportunities for Future Research. Front. Oncol. 2021, 11, 620070. [Google Scholar] [CrossRef] [PubMed]
- Leonetti, A.; Puglisi, G.; Rossi, M.; Viganò, L.; Conti Nibali, M.; Gay, L.; Sciortino, T.; Howells, H.; Fornia, L.; Riva, M.; et al. Factors Influencing Mood Disorders and Health Related Quality of Life in Adults With Glioma: A Longitudinal Study. Front. Oncol. 2021, 11, 662039. [Google Scholar] [CrossRef] [PubMed]
- Tyldesley-Marshall, N.; Greenfield, S.; Neilson, S.; English, M.; Adamski, J.; Peet, A. Qualitative study: Patients’ and parents’ views on brain tumour MRIs. Arch. Dis. Child. 2020, 105, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Van Dijken, B.R.J.; van Laar, P.J.; Smits, M.; Dankbaar, J.W.; Enting, R.H.; van der Hoorn, A. Perfusion MRI in treatment evaluation of glioblastomas: Clinical relevance of current and future techniques. J. Magn. Reson. Imaging 2019, 49, 11–22. [Google Scholar] [CrossRef]
- Martucci, M.; Russo, R.; Giordano, C.; Schiarelli, C.; D’Apolito, G.; Tuzza, L.; Lisi, F.; Ferrara, G.; Schimperna, F.; Vassalli, S.; et al. Advanced Magnetic Resonance Imaging in the Evaluation of Treated Glioblastoma: A Pictorial Essay. Cancers 2023, 15, 3790. [Google Scholar] [CrossRef]
- Thust, S.C.; Heiland, S.; Falini, A.; Jäger, H.R.; Waldman, A.D.; Sundgren, P.C.; Godi, C.; Katsaros, V.K.; Ramos, A.; Bargallo, N.; et al. Glioma imaging in Europe: A survey of 220 centres and recommendations for best clinical practice. Eur. Radiol. 2018, 28, 3306–3317. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Number | % | |
|---|---|---|---|
| Number of patients | 261 | ||
| Median age at diagnosis | 59 years | ||
| Median overall survival | 15 months | ||
| Sex | Men | 164 | 62.8 |
| Women | 97 | 37.2 | |
| IDH mutation | IDH-1 | 10 | 3.8 |
| Wild type | 84 | 32.2 | |
| Unknown | 167 | 64.0 | |
| MGMT status | Methylated | 13 | 5.0 |
| Unmethylated | 8 | 3.1 | |
| Unknown | 240 | 92.0 | |
| Extent of resection | Gross-total | 79 | 30.3 |
| Sub-total | 120 | 46.0 | |
| Biopsy | 39 | 14.9 | |
| Unknown | 23 | 8.8 | |
| Completion of Stupp protocol | Yes | 151 | 57.9 |
| No | 110 | 42.1 |
| Timepoint | Field Strength | Total | ||
|---|---|---|---|---|
| 1.5T | 3.0T | N | ||
| Post-OP | N (%) | 159 (84.6) | 29 (15.4) | 188 |
| Post-CCRT | N (%) | 256 (99.2) | 2 (0.8) | 258 |
| TMZ3/6 | N (%) | 188 (98.2) | 2 (1.1) | 190 |
| TMZ6/6 | N (%) | 154 (100) | 0 (0) | 154 |
| Total | N (%) | 757 (95.8) | 33 (4.2) | 790 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Dijken, B.R.J.; Doff, A.R.; Enting, R.H.; van Laar, P.J.; Jeltema, H.-R.; Dierckx, R.A.J.O.; van der Hoorn, A. Influence of MRI Follow-Up on Treatment Decisions during Standard Concomitant and Adjuvant Chemotherapy in Patients with Glioblastoma: Is Less More? Cancers 2023, 15, 4973. https://doi.org/10.3390/cancers15204973
van Dijken BRJ, Doff AR, Enting RH, van Laar PJ, Jeltema H-R, Dierckx RAJO, van der Hoorn A. Influence of MRI Follow-Up on Treatment Decisions during Standard Concomitant and Adjuvant Chemotherapy in Patients with Glioblastoma: Is Less More? Cancers. 2023; 15(20):4973. https://doi.org/10.3390/cancers15204973
Chicago/Turabian Stylevan Dijken, Bart R. J., Annerieke R. Doff, Roelien H. Enting, Peter Jan van Laar, Hanne-Rinck Jeltema, Rudi A. J. O. Dierckx, and Anouk van der Hoorn. 2023. "Influence of MRI Follow-Up on Treatment Decisions during Standard Concomitant and Adjuvant Chemotherapy in Patients with Glioblastoma: Is Less More?" Cancers 15, no. 20: 4973. https://doi.org/10.3390/cancers15204973
APA Stylevan Dijken, B. R. J., Doff, A. R., Enting, R. H., van Laar, P. J., Jeltema, H.-R., Dierckx, R. A. J. O., & van der Hoorn, A. (2023). Influence of MRI Follow-Up on Treatment Decisions during Standard Concomitant and Adjuvant Chemotherapy in Patients with Glioblastoma: Is Less More? Cancers, 15(20), 4973. https://doi.org/10.3390/cancers15204973