
Real-Life Study of the Benefit of Concomitant Radiotherapy with Cemiplimab in Advanced Cutaneous Squamous Cell Carcinoma (cSCC): A Retrospective Cohort Study

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- -
- Clinically every 2 or 3 weeks before the administration of cemiplimab;
- -
- Radiologically every 3 months with TEP tomodensitometry, cerebro facial MRI or thoraco abdomino pelvic scanner according to tumour localization, using the iRECIST criteria.
Statistical Analysis
3. Results
3.1. Patients
3.2. Efficacy Evaluation during Cemiplimab Treatment
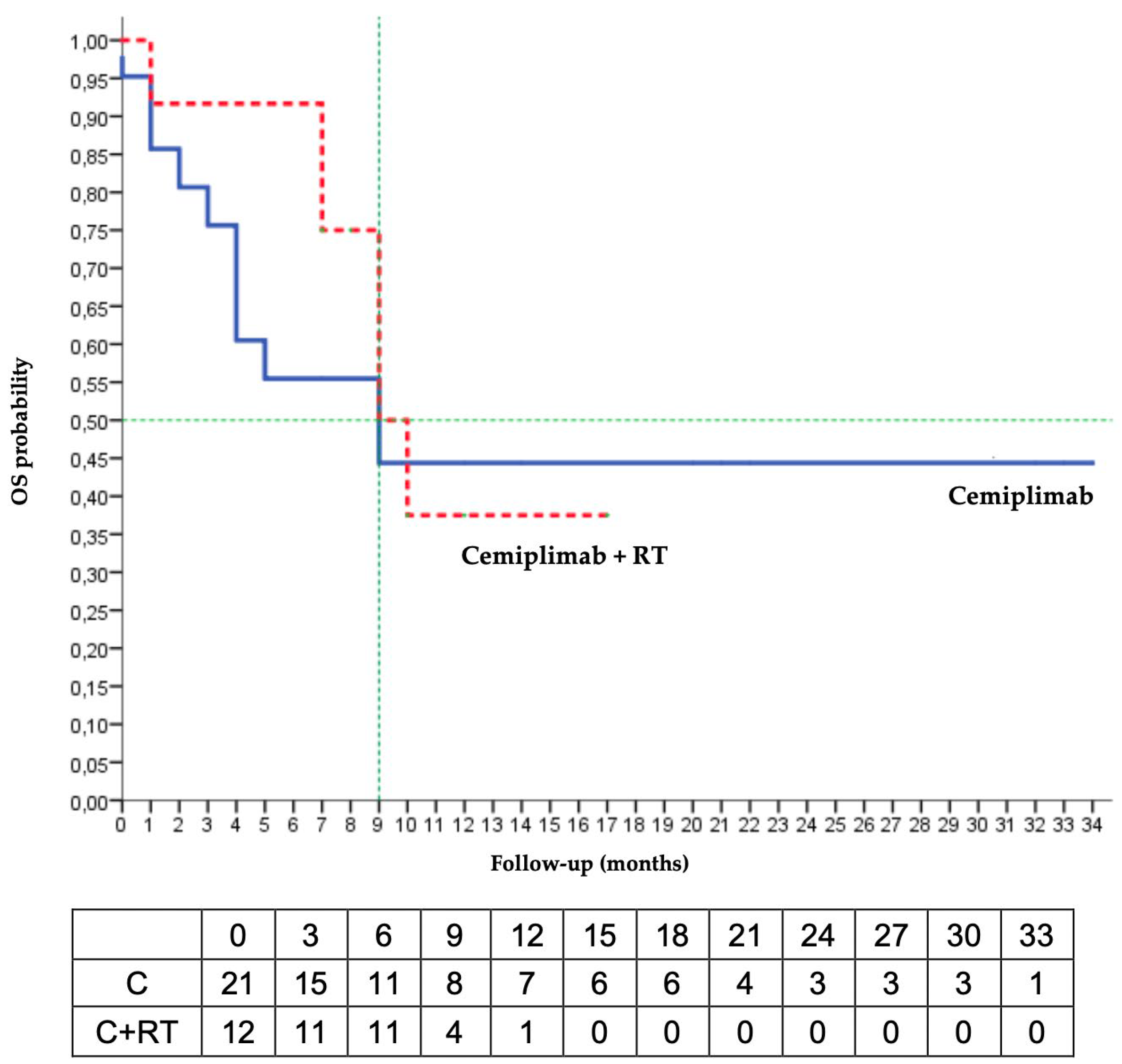
3.3. Analysis after Discontinuation of Cemiplimab
3.4. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stratigos, A.J.; Garbe, C.; Dessinioti, C.; Lebbe, C.; Bataille, V.; Bastholt, L.; Dreno, B.; Fargnoli, M.C.; Forsea, A.M.; Frenard, C.; et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 1. Epidemiology, diagnostics and prevention. Eur. J. Cancer 2020, 128, 60–82. [Google Scholar] [CrossRef] [PubMed]
- Schmults, C.D.; Blitzblau, R.; Aasi, S.Z.; Alam, M.; Andersen, J.S.; Baumann, B.C.; Bordeaux, J.; Chen, P.; Chin, R.; Contreras, C.M.; et al. NCCN Guidelines® Insights: Squamous Cell Skin Cancer, Version 1.2022: Featured Updates to the NCCN Guidelines. J. Natl. Compr. Canc. Netw. 2021, 19, 1382–1394. [Google Scholar] [CrossRef] [PubMed]
- Stratigos, A.J.; Garbe, C.; Dessinioti, C.; Lebbe, C.; Bataille, V.; Bastholt, L.; Dreno, B.; Fargnoli, M.C.; Forsea, A.M.; Frenard, C.; et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 2. Treatment. Eur. J. Cancer 2020, 128, 83–102. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef] [PubMed]
- McGranahan, N.; Furness, A.J.S.; Rosenthal, R.; Ramskov, S.; Lyngaa, R.; Saini, S.K.; Jamal-Hanjani, M.; Wilson, G.A.; Birkbak, N.J.; Hiley, C.T.; et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 2016, 351, 1463–1469. [Google Scholar] [CrossRef]
- Goodman, A.M.; Kato, S.; Bazhenova, L.; Patel, S.P.; Frampton, G.M.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol. Cancer Ther. 2017, 16, 2598–2608. [Google Scholar] [CrossRef]
- Migden, M.R.; Rischin, D.; Schmults, C.D.; Guminski, A.; Hauschild, A.; Lewis, K.D.; Chung, C.H.; Hernandez-Aya, L.F.; Lim, A.M.; Chang, A.L.S.; et al. PD-1 Blockade with Cemiplimab in Advanced Cutaneous Squamous-Cell Carcinoma. N. Engl. J. Med. 2018, 379, 341–351. [Google Scholar] [CrossRef]
- Hughes, B.G.M.; Munoz-Couselo, E.; Mortier, L.; Bratland, Å.; Gutzmer, R.; Roshdy, O.; Mendoza, R.G.; Schachter, J.; Arance, A.; Grange, F.; et al. Pembrolizumab for locally advanced and recurrent/metastatic cutaneous squamous cell carcinoma (KEYNOTE-629 study): An open-label, nonrandomized, multicenter, phase II trial. Ann. Oncol. 2021, 32, 1276–1285. [Google Scholar] [CrossRef]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune Checkpoint Blockade: A Common Denominator Approach to Cancer Therapy. Cancer Cell 2015, 27, 450–461. [Google Scholar] [CrossRef]
- Allen, C.; Her, S.; Jaffray, D.A. Radiotherapy for Cancer: Present and Future. Adv. Drug Deliv. Rev. 2017, 109, 1–2. [Google Scholar] [CrossRef]
- Quéro, L.; Fumagalli, I.; Benadon, B.; Mignot, F.; Guillerm, S.; Labidi, M.; Hennequin, C. Place de la radiothérapie dans le traitement des carcinomes cutanés. Cancer/Radiothérapie 2021, 25, 593–597. [Google Scholar] [CrossRef]
- Demaria, S.; Golden, E.B.; Formenti, S.C. Role of Local Radiation Therapy in Cancer Immunotherapy. JAMA Oncol. 2015, 1, 1325–1332. [Google Scholar] [CrossRef]
- Formenti, S.C.; Demaria, S. Systemic effects of local radiotherapy. Lancet Oncol. 2009, 10, 718–726. [Google Scholar] [CrossRef]
- Demaria, S.; Guha, C.; Schoenfeld, J.; Morris, Z.; Monjazeb, A.; Sikora, A.; Crittenden, M.; Shiao, S.; Khleif, S.; Gupta, S.; et al. Radiation dose and fraction in immunotherapy: One-size regimen does not fit all settings, so how does one choose? J. Immunother. Cancer 2021, 9, e002038. [Google Scholar] [CrossRef]
- Demaria, S.; Ng, B.; Devitt, M.L.; Babb, J.; Kawashima, N.; Liebes, L.; Formenti, S.C. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int. J. Radiat. Oncol. 2004, 58, 862–870. [Google Scholar] [CrossRef]
- Asna, N.; Livoff, A.; Batash, R.; Debbi, R.; Schaffer, P.; Rivkind, T. Radiation Therapy and Immunotherapy—A Potential Combination in Cancer Treatment. Curr. Oncol. 2018, 25, 454–460. [Google Scholar] [CrossRef]
- Ngwa, W.; Irabor, O.C.; Schoenfeld, J.D.; Hesser, J.; Demaria, S.; Formenti, S.C. Using immunotherapy to boost the abscopal effect. Nat. Rev. Cancer 2018, 18, 313–322. [Google Scholar] [CrossRef]
- Chicas-Sett, R.; Morales-Orue, I.; Rodriguez-Abreu, D.; Lara-Jimenez, P. Combining radiotherapy and ipilimumab induces clinically relevant radiation-induced abscopal effects in metastatic melanoma patients: A systematic review. Clin. Transl. Radiat. Oncol. 2018, 9, 5–11. [Google Scholar] [CrossRef]
- Koller, K.M.; Mackley, H.B.; Liu, J.; Wagner, H.; Talamo, G.; Schell, T.; Pameijer, C.; Neves, R.; Anderson, B.; Kokolus, K.; et al. Improved survival and complete response rates in patients with advanced melanoma treated with concurrent ipilimumab and radiotherapy versus ipilimumab alone. Cancer Biol. Ther. 2017, 18, 36–42. [Google Scholar] [CrossRef]
- Theelen, W.S.M.E.; Chen, D.; Verma, V.; Hobbs, B.P.; Peulen, H.M.U.; Aerts, J.G.J.V.; Bahce, I.; Niemeijer, A.L.N.; Chang, J.Y.; de Groot, P.M.; et al. Pembrolizumab with or without radiotherapy for metastatic non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Respir. Med. 2021, 9, 467–475. [Google Scholar] [CrossRef]
- Forner, D.; Horwich, P.; Trites, J.R.; Hollenhorst, H.; Bullock, M.; Lamond, N. The Abscopal Effect in Head-and-Neck Squamous Cell Carcinoma Treated with Radiotherapy and Nivolumab: A Case Report and Literature Review. Curr. Oncol. 2020, 27, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Salzmann, M.; Leiter, U.; Loquai, C.; Zimmer, L.; Ugurel, S.; Gutzmer, R.; Thoms, K.-M.; Enk, A.H.; Hassel, J.C. Programmed cell death protein 1 inhibitors in advanced cutaneous squamous cell carcinoma: Real-world data of a retrospective, multicenter study. Eur. J. Cancer 2020, 138, 125–132. [Google Scholar] [CrossRef]
- Hober, C.; Fredeau, L.; Pham-Ledard, A.; Boubaya, M.; Herms, F.; Celerier, P.; Aubin, F.; Beneton, N.; Dinulescu, M.; Jannic, A.; et al. Cemiplimab for Locally Advanced and Metastatic Cutaneous Squamous-Cell Carcinomas: Real-Life Experience from the French CAREPI Study Group. Cancers 2021, 13, 3547. [Google Scholar] [CrossRef] [PubMed]
- Baggi, A.; Quaglino, P.; Rubatto, M.; Depenni, R.; Guida, M.; Ascierto, P.A.; Trojaniello, C.; Queirolo, P.; Saponara, M.; Peris, K.; et al. Real world data of cemiplimab in locally advanced and metastatic cutaneous squamous cell carcinoma. Eur. J. Cancer Oxf. Engl. 1990 2021, 157, 250–258. [Google Scholar] [CrossRef] [PubMed]
- McBride, S.; Sherman, E.; Tsai, C.J.; Baxi, S.; Aghalar, J.; Eng, J.; Zhi, W.I.; McFarland, D.; Michel, L.S.; Young, R.; et al. Randomized Phase II Trial of Nivolumab With Stereotactic Body Radiotherapy Versus Nivolumab Alone in Metastatic Head and Neck Squamous Cell Carcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 30–37. [Google Scholar] [CrossRef]
- Abuodeh, Y.; Venkat, P.; Kim, S. Systematic review of case reports on the abscopal effect. Curr. Probl. Cancer 2016, 40, 25–37. [Google Scholar] [CrossRef]
- Tachiki, L.M.L.; Silva, K.W.; Hippe, D.S.; Fritzsche, D.; Raczka, A.; Perdue, A.; Majovski, J.; Spallone, A.; Goldstein, D.A.; Nghiem, P.; et al. Extended duration of anti-PD-1 therapy, using reduced frequency dosing, in patients with advanced melanoma and Merkel cell carcinoma. J. Clin. Oncol. 2022, 40, 2588. [Google Scholar]
- Gross, N.D.; Miller, D.M.; Khushalani, N.I.; Divi, V.; Ruiz, E.S.; Lipson, E.J.; Meier, F.; Su, Y.B.; Swiecicki, P.L.; Atlas, J.; et al. Neoadjuvant Cemiplimab for Stage II to IV Cutaneous Squamous-Cell Carcinoma. N. Engl. J. Med. 2022, 387, 1557–1568. [Google Scholar] [CrossRef]
- Leroy, V.; Gerard, E.; Dutriaux, C.; Prey, S.; Gey, A.; Mertens, C.; Beylot-Barry, M.; Pham-Ledard, A. Adverse events need for hospitalization and systemic immunosuppression in very elderly patients (over 80 years) treated with ipilimumab for metastatic melanoma. Cancer Immunol. Immunother. CII 2019, 68, 545–551. [Google Scholar] [CrossRef]
- Barailler, H.; Salomon, G.; Dutriaux, C.; Prey, S.; Gérard, E.; Dousset, L.; Mertens, C.; Beylot-Barry, M.; Meyer, N.; Pham-Ledard, A. Adverse events, need for hospitalization and systemic immunosuppression in very older patients (over 80 years) treated with anti-PD-1 for metastatic melanoma. J. Geriatr. Oncol. 2020, 11, 1340–1343. [Google Scholar] [CrossRef]
- Kugel, C.H.; Douglass, S.M.; Webster, M.R.; Kaur, A.; Liu, Q.; Yin, X.; Weiss, S.A.; Darvishian, F.; Al-Rohil, R.N.; Ndoye, A.; et al. Age Correlates with Response to Anti-PD1, Reflecting Age-Related Differences in Intratumoral Effector and Regulatory T-Cell Populations. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2018, 24, 5347–5356. [Google Scholar] [CrossRef]
- L’Orphelin, J.-M.; Varey, E.; Khammari, A.; Dreno, B.; Dompmartin, A. Severe Late-Onset Grade III–IV Adverse Events under Immunotherapy: A Retrospective Study of 79 Cases. Cancers 2021, 13, 4928. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cemiplimab (n = 21) | Cemiplimab/RT (n = 12) | |
|---|---|---|
| Age (years) | 75.1 ± 11.8 | 77.2 ± 12.5 |
| <65 yo | 2 (9.5) | 3 (25.0) |
| 65–75 yo | 5 (23.8) | 1 (8.3) |
| >75 yo | 14 (66.7) | 8 (66.7) |
| Gender | ||
| Male | 17 (81) | 11 (91.7) |
| Female | 4 (19) | 1 (8.3) |
| ECOG status | ||
| 0 | 2 (9.5) | 1 (8.4) |
| 1 | 8 (38.1) | 7 (58.3) |
| 2 | 10 (47.6) | 4 (33.3) |
| 3 | 1 (4.8) | 0 |
| Previous cSCC | ||
| No | 8 (38.1) | 6 (50) |
| Yes | 13 (61.9) | 6(50) |
| Immunodepression | ||
| No | 16 (76.2) | 8 (66.7) |
| Yes | 5 (23.8) | 4 (33.3) |
| Lymphopenia | ||
| No | 14 (66.7) | 7 (58.3) |
| Yes | 7 (33.3) | 5 (41.7) |
| Staging | ||
| LacSCC | 3 (14.3) | 1 (8.3) |
| mcSCC | 18 (85.7) | 11 (91.7) |
| Locoregional metastasis | 11 (61.1) | 7 (63.6) |
| Distant metastasis | 7 (38.9) | 4 (36.4) |
| Site | ||
| Face | 16 (76.2) | 6 (50) |
| Scalp | 2 (9.5) | 0 |
| Cervical | 0 | 2 (16.7) |
| Trunk | 2 (9.5) | 1 (8.3) |
| Arm or leg | 1 (4.8) | 3 (25) |
| Size (mm) | 35.4 ± 24.2 | 48.1 ± 33.4 |
| Previous lines of therapy | ||
| No | 19 (90.5) | 11 (91.7) |
| Yes | 2 (9.5) | 1 (8.3) |
| Previous radiotherapy | ||
| No | 7 (33.3) | 11 (91.7) |
| Yes | 14 (66.7) | 1 (8.3) |
| Histological features | ||
| Degree of differentiation | ||
| Well | 9 (52.9) | 5 (41.7) |
| Moderate | 6 (35.3) | 4 (33.3) |
| Poor | 2 (11.8) | 3 (25) |
| PNI | ||
| No | 6 (66.7) | 5 (100) |
| Yes | 3 (33.3) | 0 |
| Bone erosion | ||
| No | 10 (66.7) | 8 (88.9) |
| Yes | 5 (33.3) | 1 (11.1) |
| Invasion beyond subcutaneous fat | ||
| No | 6 (50) | 2 (33.3) |
| Yes | 6 (50) | 4 (66.7) |
| Dose of cemiplimab | ||
| 3 mg/kg/2 weeks | 5 (23.8) | 0 |
| 350 mg/3 weeks | 14 (66.7) | 12 (100) |
| Both # | 2 (9.5) | 0 |
| Intent of radiotherapy | ||
| Curative | 8 (66.7) | |
| Palliative | 4 (33.3) | |
| Site of radiotherapy | ||
| Primary tumour | 2 (16.7) | |
| Metastasis | 10 (83.3) | |
| Dose per fractions (Gy) | 4.0 ± 1.7 | |
| Fractions | 16.2 ± 12.6 | |
| Prescribed dose | 45.5 ± 22.6 | |
| BED | 60.5 ± 26.0 |
| BR | Total | Cemiplimab | Cemiplimab + RT | p | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| CR | 10 | 30.3 | 6 | 28.6 | 4 | 33.3 | 0.229 |
| PR | 5 | 15.2 | 4 | 19.1 | 1 | 8.3 | |
| SD | 5 | 15.2 | 1 | 4.8 | 4 | 33.3 | |
| PD | 6 | 18.2 | 4 | 19.0 | 2 | 16.7 | |
| NE | 7 | 21.2 | 6 | 28.6 | 1 | 8.3 | |
| ORR | 15 | 45.5 | 10 | 47.6 | 5 | 41.6 | 1.000 |
| DCR | 14 | 70.0 | 9 | 81.8 | 5 | 55.6 | 0.336 |
| Variable | Palliative Care Decision or Death | Progression | ||
|---|---|---|---|---|
| HR (95% IC) | p-Value | HR (95% IC) | p-Value | |
| Univariate analysis | ||||
| Gender M vs. F | 0.7 (0.2–2.4) | 0.543 | 0.8 (0.2–3.7) | 0.782 |
| Age (years) | 0.98 (0.93–1.01) | 0.140 | 0.96 (0.91–1.00) | 0.051 |
| 65–75 vs. <65 | 0.6 (0.2–2.5) | 0.538 | 0.3 (0.1–1.4) | 0.132 |
| 75 vs. <65 | 0.4 (0.1–1.4) | 0.163 | 0.2 (0.1–0.7 | 0.014 |
| ECOG status ≥ 2 vs. <2 | 2.1 (0.9–4.7) | 0.076 | 1.5 (0.6–3.8) | 0.378 |
| Previous cSCC | 0.8 (0.3–2.2) | 0.733 | 0.5 (0.2–1.7) | 0.291 |
| Immunodepression | 1.0 (0.4–2.9) | 0.969 | 1.3 (0.4–4.2) | 0.713 |
| Lymphopenia < 1 g/L | 0.7 (0.3–2.0) | 0.515 | 1.1 (0.4–3.6) | 0.830 |
| Staging mcSCC-m vs. LacSCC | 1.4 (0.3–5.6) | 0.701 | 2.1 (0.3–16.1) | 0.483 |
| Previous lignes of therapy | 3.8 (1.1–13.4) | 0.041 | 10.5 (1.9–59.1) | 0.008 |
| Degree of differentiation | 0.917 | 0.648 | ||
| Moderate vs. poor | 1.0 (0.2–5.2) | 0.995 | 0.7 (0.2–3.2) | 0.672 |
| Well vs. poor | 1.3 (0.3–6.1) | 0.786 | 0.5 (0.1–2.3) | 0.354 |
| Size of tumour (n = 19) | 1.01 (0.99–1.03) | 0.274 | 1.02 (1.01–1.05) | 0.036 |
| PNI (n = 14) | 1.0 (0.1–8.6) | 0.963 | 0.7 (0.1–6.2) | 0.736 |
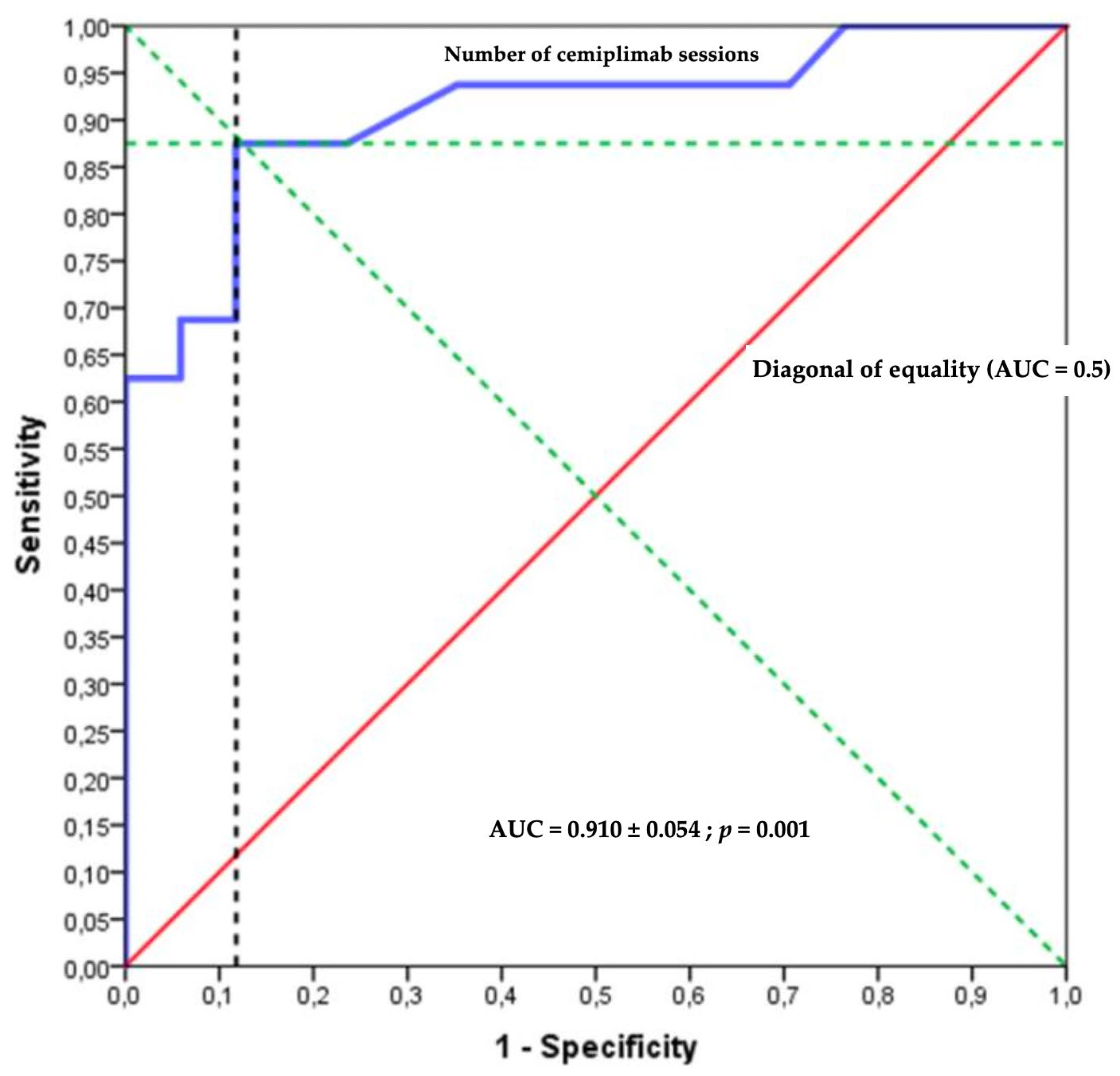
| Number of cemiplimab sessions | 0.8 (0.7–0.9) | 0.001 | 0.8 (0.7–0.9) | 0.005 |
| cemiplimab vs. cemiplimab/RT | 0.8 (0.3–2.2) | 0.666 | 1.5 (0.5–4.5) | 0.517 |
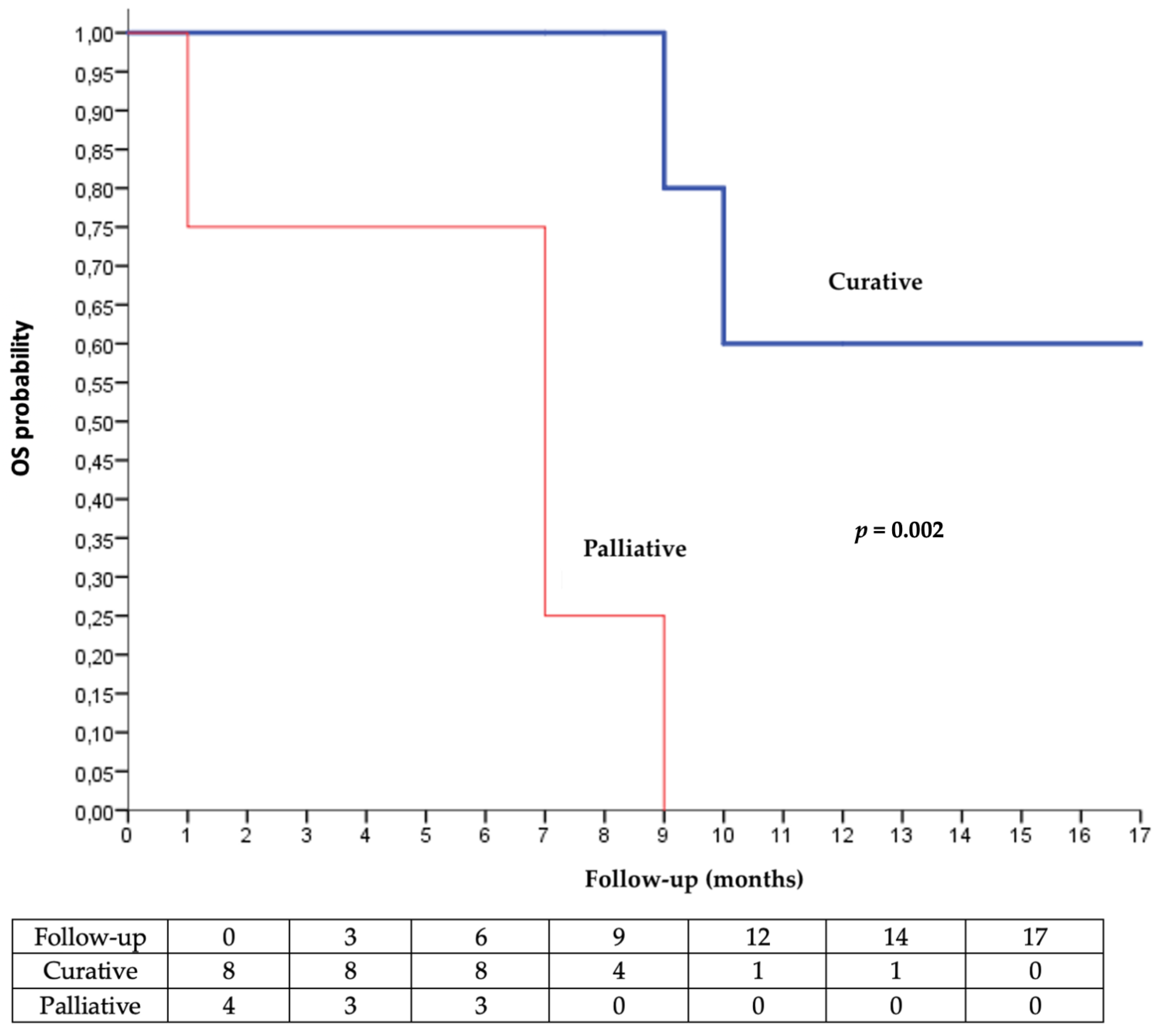
| Intent of radiotherapy: palliative vs. curative | 13.5 (1.5–123.2) | 0.021 | 3.4 (0.7–17.4) | 0.144 |
| Multivariate analysis * | ||||
| Variable significative | Palliative care decision or death | Progression | ||
| HR (95% IC) | p | HR (95% IC) | p | |
| Number of cemiplimab sessions | ||||
| Quantitative | 0.8 (0.7–0.9) | 0.001 | 0.8 (0.7–10.0) | 0.027 |
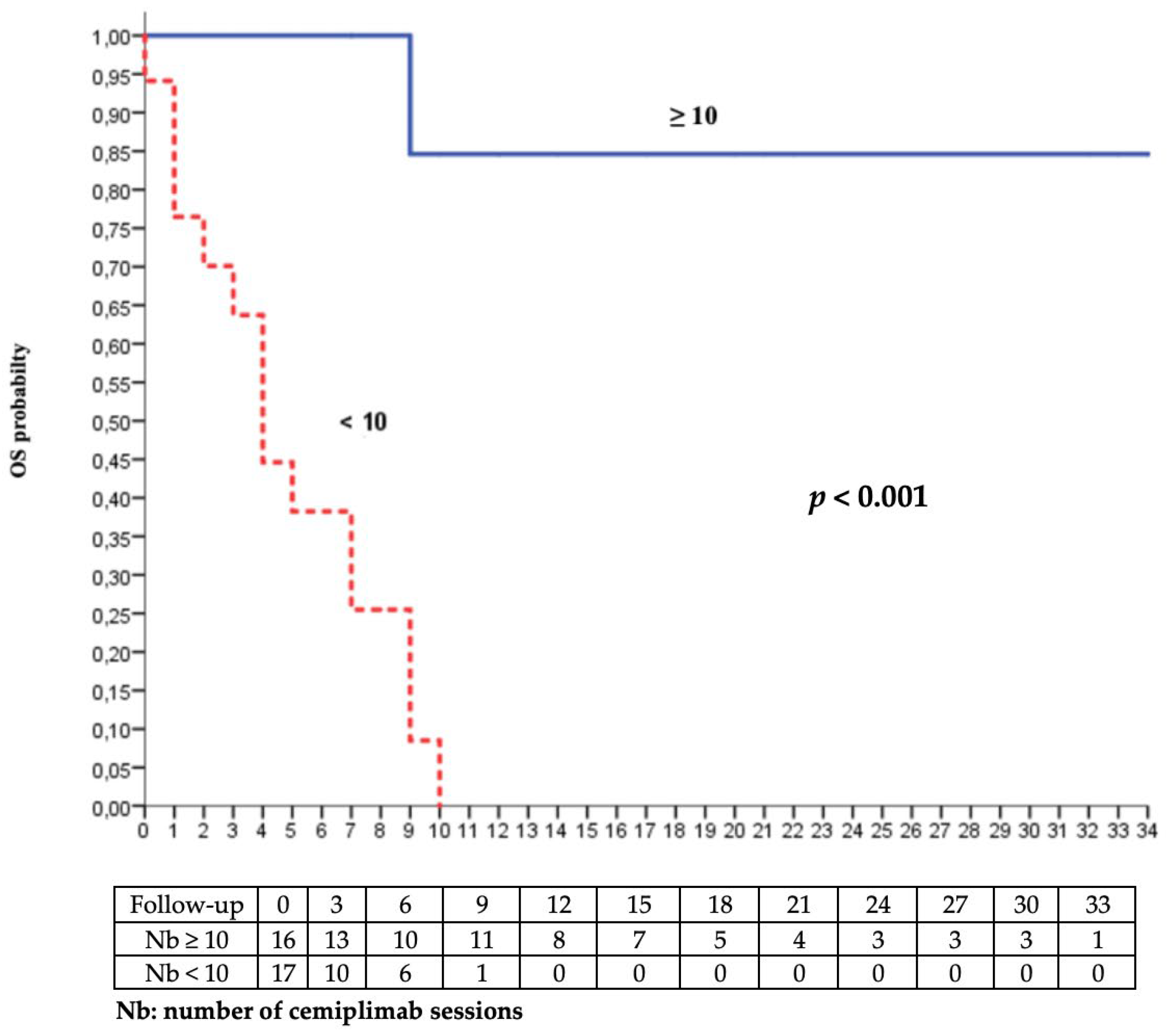
| Qualitative < 10 vs. ≥10 | 19.3 (4.2–88.6) | <0.001 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bailly-Caillé, B.; Kottler, D.; Morello, R.; Lecornu, M.; Kao, W.; Meyer, E.; Dompmartin, A.; L’Orphelin, J.-M. Real-Life Study of the Benefit of Concomitant Radiotherapy with Cemiplimab in Advanced Cutaneous Squamous Cell Carcinoma (cSCC): A Retrospective Cohort Study. Cancers 2023, 15, 495. https://doi.org/10.3390/cancers15020495
Bailly-Caillé B, Kottler D, Morello R, Lecornu M, Kao W, Meyer E, Dompmartin A, L’Orphelin J-M. Real-Life Study of the Benefit of Concomitant Radiotherapy with Cemiplimab in Advanced Cutaneous Squamous Cell Carcinoma (cSCC): A Retrospective Cohort Study. Cancers. 2023; 15(2):495. https://doi.org/10.3390/cancers15020495
Chicago/Turabian StyleBailly-Caillé, Barbara, Diane Kottler, Rémy Morello, Marie Lecornu, William Kao, Emmanuel Meyer, Anne Dompmartin, and Jean-Matthieu L’Orphelin. 2023. "Real-Life Study of the Benefit of Concomitant Radiotherapy with Cemiplimab in Advanced Cutaneous Squamous Cell Carcinoma (cSCC): A Retrospective Cohort Study" Cancers 15, no. 2: 495. https://doi.org/10.3390/cancers15020495
APA StyleBailly-Caillé, B., Kottler, D., Morello, R., Lecornu, M., Kao, W., Meyer, E., Dompmartin, A., & L’Orphelin, J.-M. (2023). Real-Life Study of the Benefit of Concomitant Radiotherapy with Cemiplimab in Advanced Cutaneous Squamous Cell Carcinoma (cSCC): A Retrospective Cohort Study. Cancers, 15(2), 495. https://doi.org/10.3390/cancers15020495