

Role of HIPEC after Complete Cytoreductive Surgery (CRS) in Peritoneal Recurrence of Platinum-Sensitive Recurrent Ovarian Cancer (OC): The Aim for Standardization at Two Reference Centers for CRS
 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Cytoreductive Surgery
2.3. HIPEC
2.4. Statistical Analysis
3. Results
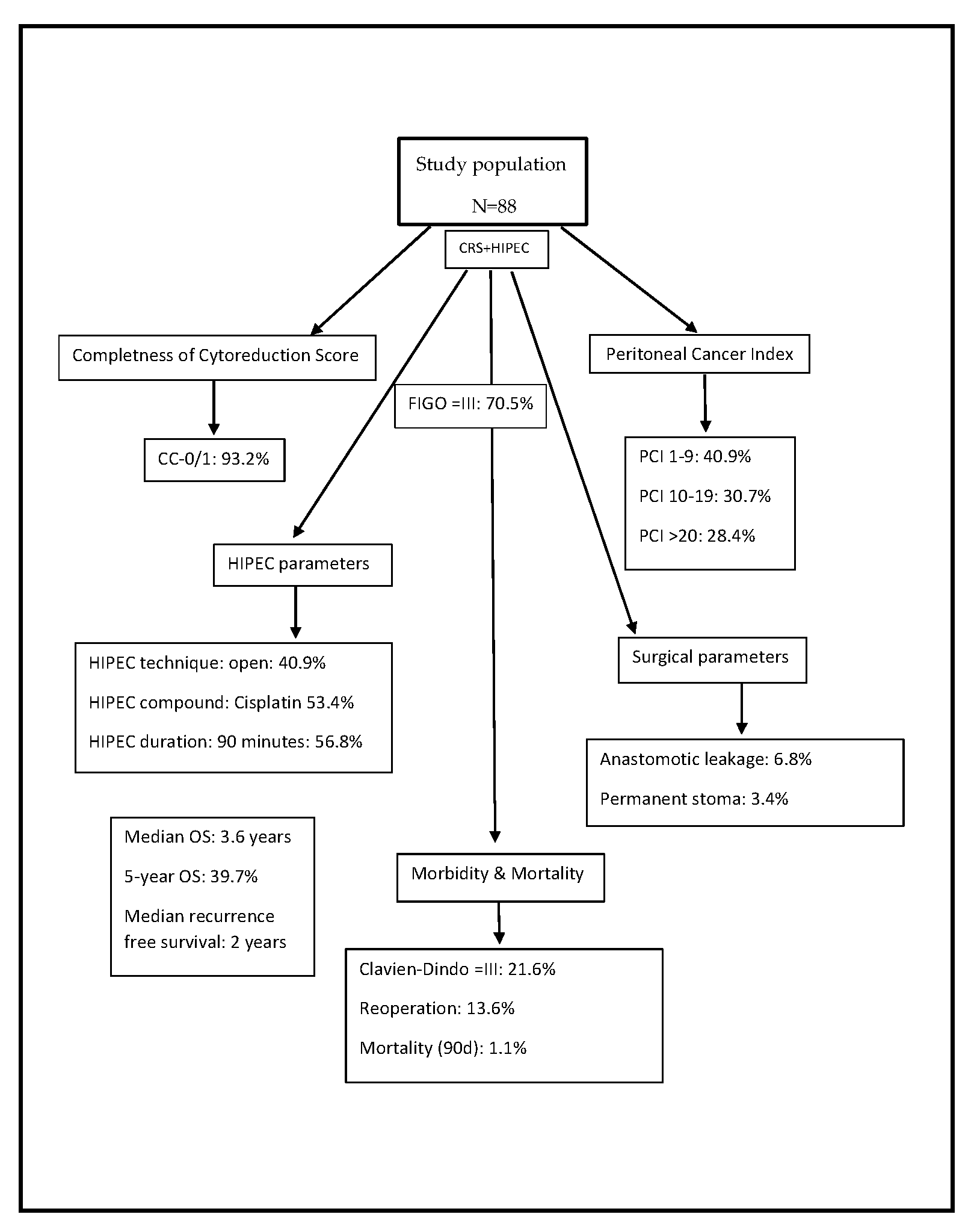
3.1. Characteristics of Patients, Tumor, Therapy, and Short-Term Outcome
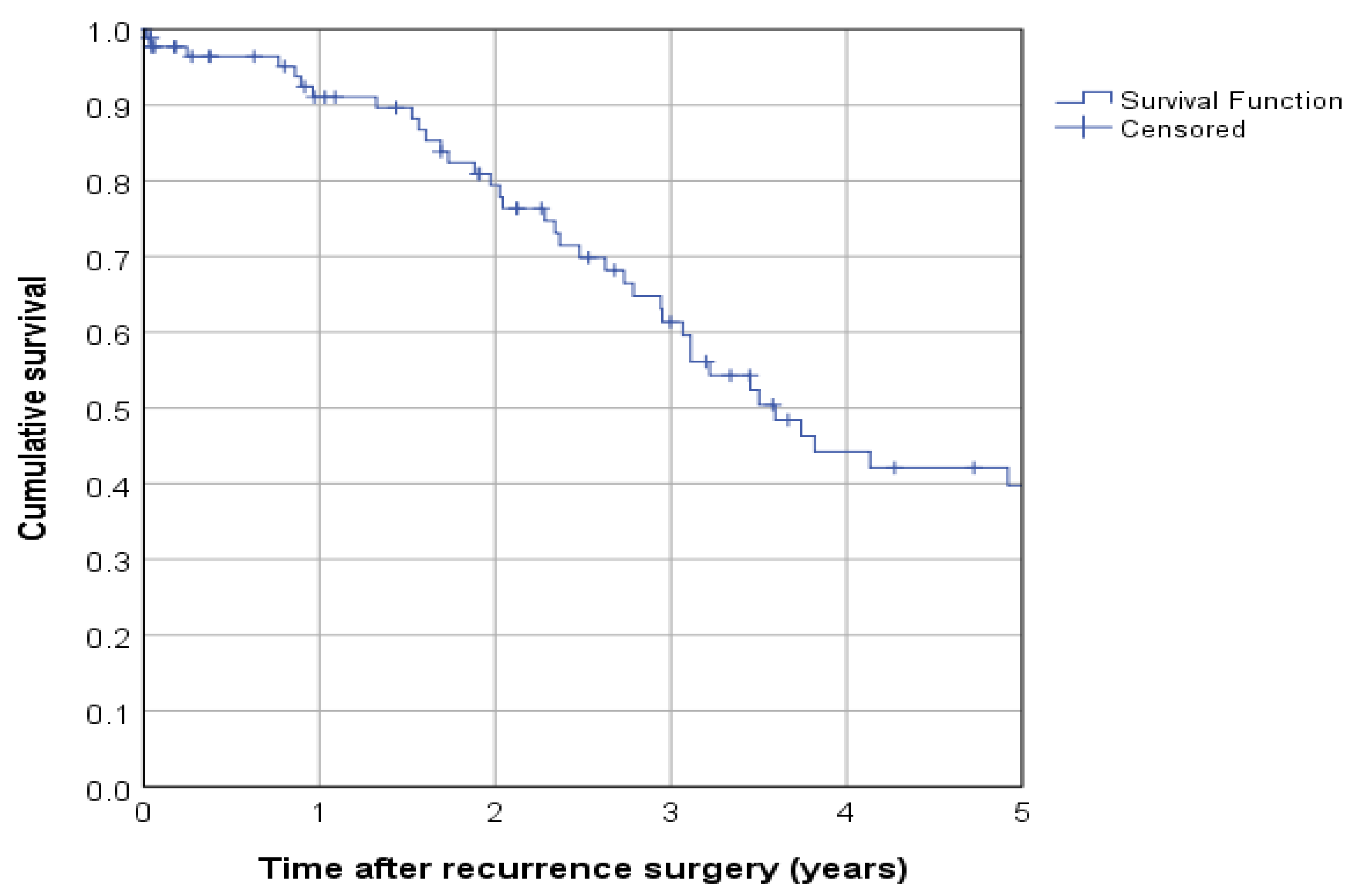
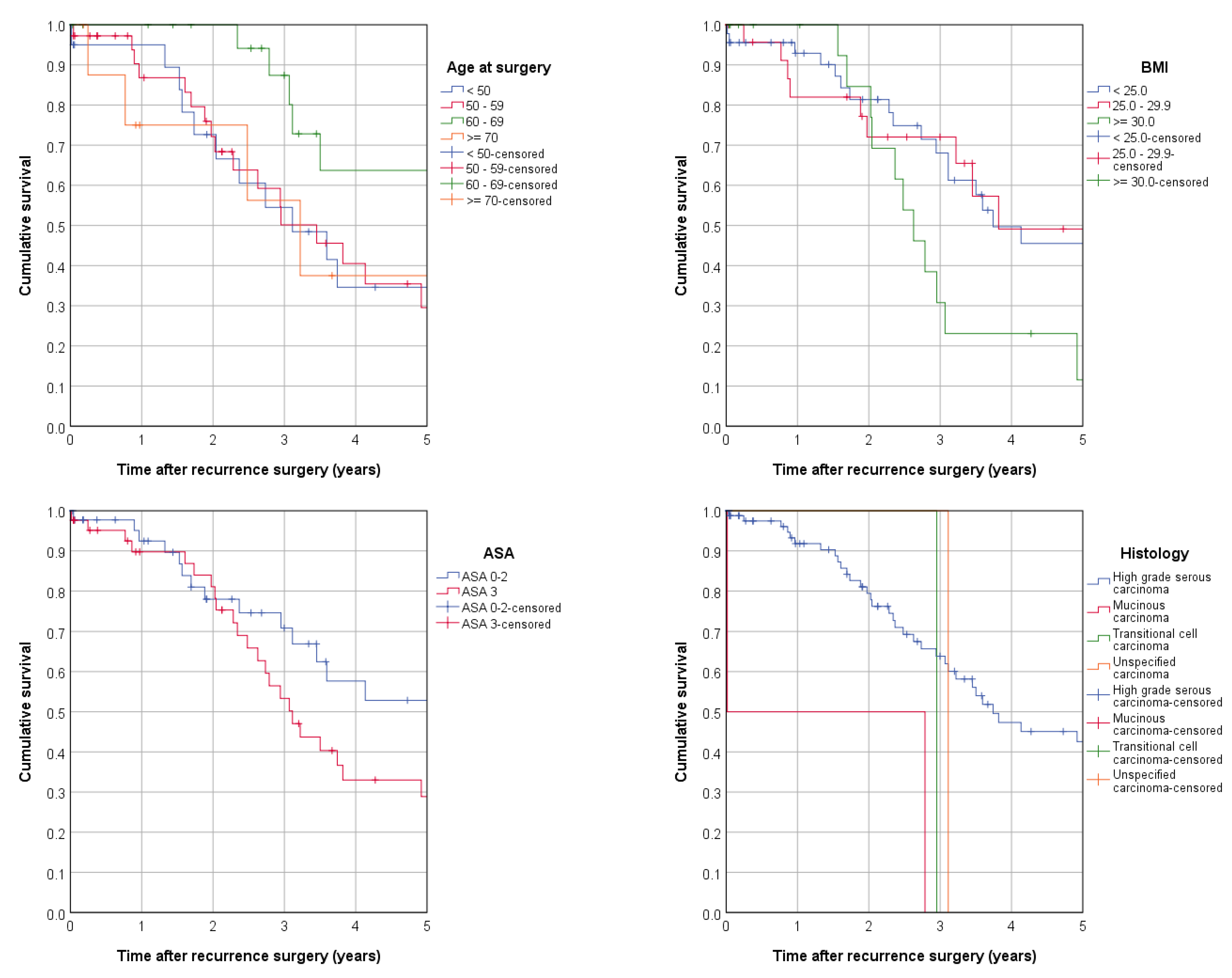
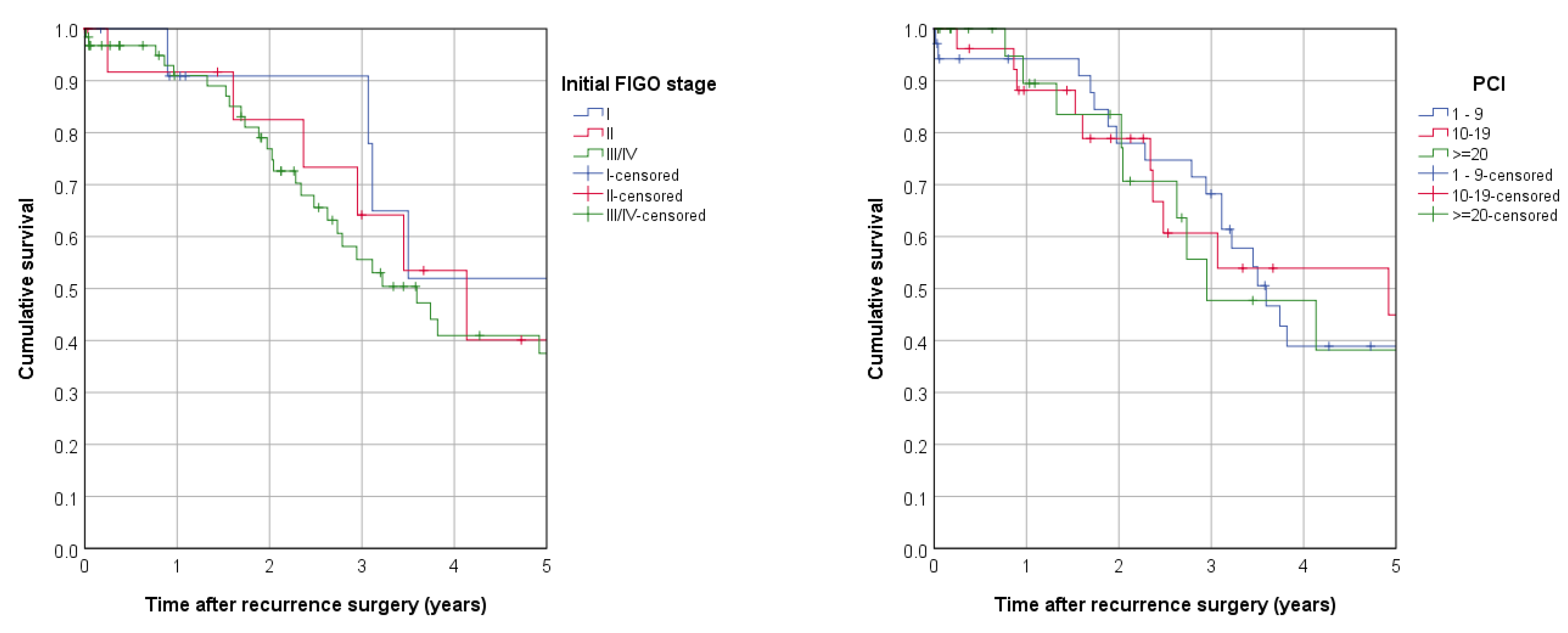
3.2. Long-Term Outcome
4. Discussion
4.1. Role of Surgery in Recurrent Epithelial Ovarian Cancer without HIPEC
4.2. HIPEC for Epithelial Ovarian Cancer
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harter, P.; Sehouli, J.; Vergote, I.; Ferron, G.; Reuss, A.; Meier, W.; Greggi, S.; Mosgaard, B.J.; Selle, F.; Guyon, F.; et al. Randomized trial of cytoreductive surgery for relapsed ovarian cancer. N. Engl. J. Med. 2021, 385, 2123–2131. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Hahmann, M.; Lueck, H.J.; Poelcher, M.; Wimberger, P.; Ortmann, O.; Canzler, U.; Richter, B.; Wagner, U.; Hasenburg, A.; et al. Surgery for recurrent ovarian cancer: Role of peritoneal carcinomatosis: Exploratory analysis of the desktop i trial about risk factors, surgical implications, and prognostic value of peritoneal carcinomatosis. Ann. Surg. Oncol. 2009, 16, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Sehouli, J.; Reuss, A.; Hasenburg, A.; Scambia, G.; Cibula, D.; Mahner, S.; Vergote, I.; Reinthaller, A.; Burges, A.; et al. Prospective validation study of a predictive score for operability of recurrent ovarian cancer: The multicenter intergroup study desktop ii. A project of the ago kommission ovar, ago study group, noggo, ago-austria, and mito. Int. J. Gynecol. Cancer 2011, 21, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Spiliotis, J.; Prodromidou, A. Narrative review of hyperthermic intraperitoneal chemotherapy (hipec) in patients with advanced ovarian cancer: A critical reappraisal of the current evidence. J. Gastrointest. Oncol. 2021, 12, S182–S188. [Google Scholar] [CrossRef] [PubMed]
- Coccolini, F.; Fugazzola, P.; Montori, G.; Ansaloni, L.; Chiarugi, M. Intraperitoneal chemotherapy for ovarian cancer with peritoneal metastases, systematic review of the literature and focused personal experience. J. Gastrointest. Oncol. 2021, 12, S144–S181. [Google Scholar] [CrossRef]
- Deutsche Krebsgesellschaft, D.K.; AWMF. S3-Leitlinie Diagnostik, Therapie und Nachsorge Maligner Ovarialtumoren Langversion 4.0, Awmf Registrierungsnummer: 032/035ol 2020. Available online: https://www.leitlinienprogramm-onkologie.de/fileadmin/user_upload/Downloads/Leitlinien/Ovarialkarzinom/Version_4/LL_Ovarialkarzinom_Kurzversion_4.0.pdf (accessed on 11 October 2022).
- Harter, P.; du Bois, A.; Hahmann, M.; Hasenburg, A.; Burges, A.; Loibl, S.; Gropp, M.; Huober, J.; Fink, D.; Schroder, W.; et al. Surgery in recurrent ovarian cancer: The arbeitsgemeinschaft gynaekologische onkologie (ago) desktop ovar trial. Ann. Surg. Oncol. 2006, 13, 1702–1710. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Current methodologies for clinical assessment of patients with peritoneal carcinomatosis. J. Exp. Clin. Cancer Res. 1996, 15, 49–58. [Google Scholar]
- Sugarbaker, P.H. Peritonectomy procedures. Ann. Surg. 1995, 221, 29–42. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Peritonectomy procedures. Cancer Treat. Res. 2007, 134, 247–264. [Google Scholar]
- Van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.; Hermans, R.H.; De Hingh, I.H.; Van Der Velden, J.; Arts, H.J.; Massuger, L.F.; et al. Hyperthermic intraperitoneal chemotherapy in ovarian cancer. N. Engl. J. Med. 2018, 378, 230–340. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The strengthening the reporting of observational studies in epidemiology (strobe) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Al Rawahi, T.; Lopes, A.D.; Bristow, R.E.; Bryant, A.; Elattar, A.; Chattopadhyay, S.; Galaal, K. Surgical cytoreduction for recurrent epithelial ovarian cancer. Cochrane Database Syst. Rev. 2013, 2016, CD008765. [Google Scholar] [CrossRef]
- Gockley, A.; Melamed, A.; Cronin, A.; Bookman, M.A.; Burger, R.A.; Cristae, M.C.; Griggs, J.J.; Mantia-Smaldone, G.; Matulonis, U.A.; Meyer, L.A.; et al. Outcomes of secondary cytoreductive surgery for patients with platinum-sensitive recurrent ovarian cancer. Am. J. Obstet. Gynecol. 2019, 221, 625.e1–625.e14. [Google Scholar] [CrossRef]
- Tian, W.J.; Chi, D.S.; Sehouli, J.; Trope, C.G.; Jiang, R.; Ayhan, A.; Cormio, G.; Xing, Y.; Breitbach, G.P.; Braicu, E.I.; et al. A risk model for secondary cytoreductive surgery in recurrent ovarian cancer: An evidence-based proposal for patient selection. Ann. Surg. Oncol. 2012, 19, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Acs, M.; Dadras, A.; Blaj, S.; Leebmann, H.; Piso, P. Selection criteria for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy with special emphasis on laparoscopy as an efficient tool. In Vivo 2022, 36, 1367–1374. [Google Scholar] [CrossRef]
- Yurttas, C.; Uberruck, L.; Nadiradze, G.; Konigsrainer, A.; Horvath, P. Limitations of laparoscopy to assess the peritoneal cancer index and eligibility for cytoreductive surgery with hipec in peritoneal metastasis. Langenbecks Arch. Surg. 2022, 407, 1667–1675. [Google Scholar] [CrossRef]
- Coleman, R.L.; Spirtos, N.M.; Enserro, D.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Kim, J.W.; Park, S.Y.; Kim, B.G.; Nam, J.H.; et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N. Engl. J. Med. 2019, 381, 1929–1939. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Zhu, J.; Feng, Y.; Tu, D.; Zhang, Y.; Zhang, P.; Jia, H.; Huang, X.; Cai, Y.; Yin, S.; et al. Secondary cytoreduction followed by chemotherapy versus chemotherapy alone in platinum-sensitive relapsed ovarian cancer (soc-1): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Bristow, R.E.; Puri, I.; Chi, D.S. Cytoreductive surgery for recurrent ovarian cancer: A meta-analysis. Gynecol. Oncol. 2009, 112, 265–274. [Google Scholar] [CrossRef]
- Bickell, N.A.; Egorova, N.; Prasad-Hayes, M.; Franco, R.; Howell, E.A.; Wisnivesky, J.; Deb, P. Secondary surgery versus chemotherapy for recurrent ovarian cancer. Am. J. Clin. Oncol. 2018, 41, 458–464. [Google Scholar] [CrossRef]
- Sugarbaker, P.H.; Chang, D. Results of treatment of 385 patients with peritoneal surface spread of appendiceal malignancy. Ann. Surg. Oncol. 1999, 6, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Segura-Sampedro, J.J.; Morales-Soriano, R.; Arjona-Sanchez, A.; Cascales-Campos, P. Secondary surgical cytoreduction needs to be assessed taking into account surgical technique, completeness of cytoreduction, and extent of disease. World J. Surg. Oncol. 2020, 18, 92. [Google Scholar] [CrossRef] [PubMed]
- Zivanovic, O.; Aldini, A.; Carlson, J.W.; Chi, D.S. Advanced cytoreductive surgery: American perspective. Gynecol. Oncol. 2009, 114, S3–S9. [Google Scholar] [CrossRef]
- Elzarkaa, A.A.; Shaalan, W.; Elemam, D.; Mansour, H.; Melis, M.; Malik, E.; Soliman, A.A. Peritoneal cancer index as a predictor of survival in advanced stage serous epithelial ovarian cancer: A prospective study. J. Gynecol. Oncol. 2018, 29, e47. [Google Scholar] [CrossRef] [PubMed]
- van de Vaart, P.J.; van der Vange, N.; Zoetmulder, F.A.; van Goethem, A.R.; van Tellingen, O.; ten Bokkel Huinink, W.W.; Beijnen, J.H.; Bartelink, H.; Begg, A.C. Intraperitoneal cisplatin with regional hyperthermia in advanced ovarian cancer: Pharmacokinetics and cisplatin-DNA adduct formation in patients and ovarian cancer cell lines. Eur. J. Cancer 1998, 34, 148–154. [Google Scholar] [CrossRef]
- Spiliotis, J.; Halkia, E.; Lianos, E.; Kalantzi, N.; Grivas, A.; Efstathiou, E.; Giassas, S. Cytoreductive surgery and hipec in recurrent epithelial ovarian cancer: A prospective randomized phase iii study. Ann. Surg. Oncol. 2015, 22, 1570–1575. [Google Scholar] [CrossRef]
- Batista, T.P. Comment on: Surgery and hipec in recurrent epithelial ovarian cancer: A prospective randomized phase iii study. Ann. Surg. Oncol. 2017, 24, 630. [Google Scholar] [CrossRef]
- Kim, S.I.; Cho, J.; Lee, E.J.; Park, S.; Park, S.J.; Seol, A.; Lee, N.; Yim, G.W.; Lee, M.; Lim, W.; et al. Selection of patients with ovarian cancer who may show survival benefit from hyperthermic intraperitoneal chemotherapy: A systematic review and meta-analysis. Medicine 2019, 98, e18355. [Google Scholar] [CrossRef]
- Zivanovic, O.; Chi, D.S.; Zhou, Q.; Iasonos, A.; Konner, J.A.; Makker, V.; Grisham, R.N.; Brown, A.K.; Nerenstone, S.; Diaz, J.P.; et al. Secondary cytoreduction and carboplatin hyperthermic intraperitoneal chemotherapy for platinum-sensitive recurrent ovarian cancer: An msk team ovary phase ii study. J. Clin. Oncol. 2021, 39, 2594–2604. [Google Scholar] [CrossRef]
- Bakrin, N.; Cotte, E.; Golfier, F.; Gilly, F.N.; Freyer, G.; Helm, W.; Glehen, O.; Bereder, J.M. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (hipec) for persistent and recurrent advanced ovarian carcinoma: A multicenter, prospective study of 246 patients. Ann. Surg. Oncol. 2012, 19, 4052–4058. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; Harter, P.; Chiva, L. Hyperthermic intraperitoneal chemotherapy does not improve survival in advanced ovarian cancer. Cancer 2019, 125 (Suppl. S24), 4594–4597. [Google Scholar] [CrossRef] [PubMed]
- Fotopoulou, C.; Sehouli, J.; Mahner, S.; Harter, P.; Van Nieuwenhuysen, E.; Gonzalez-Martin, A.; Vergote, I.; Chiva, L.; Du Bois, A. Hipec: Hope or hype in the fight against advanced ovarian cancer? Ann. Oncol. 2018, 29, 1610–1613. [Google Scholar] [CrossRef]
- Piso, P.; Nedelcut, S.D.; Rau, B.; Konigsrainer, A.; Glockzin, G.; Strohlein, M.A.; Horbelt, R.; Pelz, J. Morbidity and mortality following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: Data from the dgav studoq registry with 2149 consecutive patients. Ann. Surg. Oncol. 2019, 26, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Bartels, H.C.; Rogers, A.C.; Postle, J.; Shields, C.; Mulsow, J.; Conneely, J.; Brennan, D.J. Morbidity and mortality in women with advanced ovarian cancer who underwent primary cytoreductive surgery compared to cytoreductive surgery for recurrent disease: A meta-analysis. Pleura Peritoneum 2019, 4, 20190014. [Google Scholar] [CrossRef]
- Kurreck, A.; Gronau, F.; Alberto Vilchez, M.E.; Abels, W.; Enghard, P.; Brandl, A.; Francis, R.; Fohre, B.; Lojewski, C.; Pratschke, J.; et al. Sodium thiosulfate reduces acute kidney injury in patients undergoing cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy with cisplatin: A single-center observational study. Ann. Surg. Oncol. 2021, 29, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Glennon, K.; Mulligan, K.; Carpenter, K.; Mooney, R.; Mulsow, J.; McCormack, O.; Boyd, W.; Walsh, T.; McVey, R.; Thompson, C.; et al. The addition of sodium thiosulphate to hyperthermic intraperitoneal chemotherapy with cisplatin in ovarian cancer. Gynecol. Oncol. Rep. 2021, 37, 100796. [Google Scholar] [CrossRef] [PubMed]
- Hubner, M.; Kusamura, S.; Villeneuve, L.; Al-Niaimi, A.; Alyami, M.; Balonov, K.; Bell, J.; Bristow, R.; Guiral, D.C.; Fagotti, A.; et al. Guidelines for perioperative care in cytoreductive surgery (crs) with or without hyperthermic intraperitoneal chemotherapy (hipec): Enhanced recovery after surgery (eras(r)) society recommendations—Part i: Preoperative and intraoperative management. Eur. J. Surg. Oncol. 2020, 46, 2292–2310. [Google Scholar] [CrossRef] [PubMed]
- Hubner, M.; Kusamura, S.; Villeneuve, L.; Al-Niaimi, A.; Alyami, M.; Balonov, K.; Bell, J.; Bristow, R.; Guiral, D.C.; Fagotti, A.; et al. Guidelines for perioperative care in cytoreductive surgery (crs) with or without hyperthermic intraperitoneal chemotherapy (hipec): Enhanced recovery after surgery (eras(r)) society recommendations—Part ii: Postoperative management and special considerations. Eur. J. Surg. Oncol. 2020, 46, 2311–2323. [Google Scholar]
- Acs, M.; Halmy, L.; Isgandarova, S.; Blaj, S.; Gerken, M.; Hormann, B.; Piso, P. Hyperthermic intraperitoneal chemotherapy with cisplatin and doxorubicin for 90 minutes versus 60 minutes after cytoreductive surgery (crs). Does the 30-minute difference matter? A comparative study in a high volume centre. Anticancer Res. 2022, 42, 1019–1029. [Google Scholar] [CrossRef]
- Acs, M.; Herold, Z.; Szasz, A.M.; Mayr, M.; Häusler, S.; Piso, P. Prolonged exposition with hyperthermic intraperitoneal chemotherapy (hipec) may provide survival benefit after cytoreductive surgery (crs) in advanced primary epithelial ovarian, fallopian tube, and primary peritoneal cancer. Cancers 2022, 14, 3301. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CRS/HIPEC | |||
|---|---|---|---|
| n | % | ||
| Age at surgery | <50 | 21 | 23.9% |
| 50–59 | 36 | 40.9% | |
| 60–69 | 22 | 25.0% | |
| ≥70 | 9 | 10.2% | |
| Age | Mean/range | 57.4 | 28.3–77.2 |
| Median/IQR | 55.8 | 50.3–66.2 | |
| Time to first recurrence (years) | Mean/95%-CI | 3.4 | 2.7–4.0 |
| Median/95%-CI | 2.3 | 2.0–2.6 | |
| BMI | <25.0 | 45 | 51.1% |
| 25.0–29.9 | 25 | 28.4% | |
| ≥30.0 | 18 | 20.5% | |
| BMI | Mean/range | 25.9 | 16.3–41.8 |
| Median/IQR | 24.9 | 22.6–28.4 | |
| ASA | ASA 0–2 | 46 | 52.3% |
| ASA 3 | 42 | 47.7% | |
| ASA | Mean/range | 2 | 0–3 |
| Median/IQR | 2 | 2–3 | |
| Histology | High-grade serous carcinoma | 84 | 95.5% |
| Mucinous carcinoma | 2 | 2.3% | |
| Transitional cell carcinoma | 1 | 1.1% | |
| Unspecified carcinoma | 1 | 1.1% | |
| Initial FIGO stage | I | 12 | 13.6% |
| II | 14 | 15.9% | |
| IIIA IIIB IIIC | 2 18 41 | 2.3% 20.5% 46.6% | |
| IV | 1 | 1.1% | |
| PCI | 1–9 | 36 | 40.9% |
| 10–19 | 27 | 30.7% | |
| ≥20 | 25 | 28.4% | |
| PCI | Mean/range | 14.0 | 3.0–39.0 |
| Median/IQR | 12.0 | 7.0–20.5 | |
| Total | 88 | 100.0% | |
| CRS/HIPEC | |||
|---|---|---|---|
| n | % | ||
| CCR score | CCR-0 | 65 | 73.9% |
| CCR-1 | 17 | 19.3% | |
| CCR-2/3 | 6 | 6.8% | |
| Length of surgery (min, without HIPEC) | Mean/Range | 439 | 113–885 |
| Median/IQR | 404 | 310–565 | |
| HIPEC technique | Open | 36 | 40.9% |
| Closed | 33 | 37.5% | |
| Open-closed | 19 | 21.6% | |
| HIPEC duration | HIPEC 60 min | 38 | 43.2% |
| HIPEC 90 min | 50 | 56.8% | |
| HIPEC substances | Cisplatin | 47 | 53.4% |
| Cisplatin + Doxorubicin | 35 | 39.8% | |
| Gemcitabine | 3 | 3.4% | |
| Mitomycin C | 3 | 3.4% | |
| Parietal peritonectomy | Yes | 77 | 87.5% |
| Peritonectomy pelvis | Yes | 59 | 67.0% |
| Peritonectomy omental bursa | Yes | 16 | 18.2% |
| Peritonectomy right upper quadrant | Yes | 48 | 54.5% |
| Peritonectomy left upper quadrant | Yes | 33 | 37.9% |
| Thoracic drainage | Yes | 9 | 10.2% |
| Diaphragm resection | Yes | 20 | 22.7% |
| Hepatic capsule resection | Yes | 10 | 11.4% |
| Appendectomy | Yes | 7 | 8.0% |
| Colon resection | Yes | 36 | 40.9% |
| Small bowel resection | Yes | 25 | 28.4% |
| Low anterior rectum resection | Yes | 29 | 33.0% |
| Splenectomy | Yes | 29 | 33.0% |
| Pancreatectomy (tail) | Yes | 4 | 4.5% |
| Cholecystectomy | Yes | 27 | 30.7% |
| Greater omentectomy | Yes | 33 | 37.5% |
| Lesser omentectomy | Yes | 13 | 14.8% |
| Liver resection | Yes | 11 | 12.5% |
| Stomach resection | Yes | 6 | 6.8% |
| Hysterectomy | Yes | 2 | 2.3% |
| Adnexectomy | Yes | 1 | 1.1% |
| Resection other organs | Yes | 10 | 11.4% |
| Anastomosis small bowel–small bowel | Yes | 13 | 14.8% |
| Anastomosis stomach–small bowel | Yes | 1 | 1.1% |
| Anastomosis small bowel–colon | Yes | 26 | 29.5% |
| Anastomosis colon–colon | Yes | 5 | 5.7% |
| Anastomosis colon–rectum | Yes | 29 | 33.0% |
| Anastomosis small bowel–rectum | Yes | 4 | 4.5% |
| Colostomy | Yes | 2 | 2.3% |
| Ileostomy | Yes | 7 | 8.0% |
| Permanent colostomy | Yes | 1 | 1.1% |
| Permanent ileostomy | Yes | 2 | 2.3% |
| Total | 88 | 100.0% | |
| CRS/HIPEC | |||
|---|---|---|---|
| n | % | ||
| Length of hospital stay | Mean/range | 20.4 | 8–93 |
| Median/IQR | 15.0 | 13–21 | |
| Length of ICU stay | Mean/range | 3.8 | 1–15 |
| Median/IQR | 3.0 | 2–4 | |
| Erythrocyte concentrates | Yes | 19 | 21.6% |
| Fresh frozen plasma | Yes | 36 | 40.9% |
| Human albumin | Yes | 3 | 3.4% |
| Chest drain | Yes | 6 | 6.8% |
| Pleural puncture | Yes | 5 | 5.7% |
| Complication grade (Clavien–Dindo) | 0 | 44 | 50.0% |
| II | 25 | 28.4% | |
| III | 16 | 18.2% | |
| IV | 2 | 2.3% | |
| V | 1 | 1.1% | |
| Complication grade (Clavien–Dindo) | Mean/Range | 1 | 0–5 |
| Median/IQR | 1 | 0–2 | |
| Anastomotic insufficiency | Yes | 6 | 6.8% |
| Pneumonia | Yes | 4 | 4.5% |
| Pulmonary embolism | Yes | 13 | 14.8% |
| Pleural effusion | Yes | 9 | 10.2% |
| Urinary tract infection | Yes | 6 | 6.8% |
| Renal insufficiency | Yes | 1 | 1.1% |
| Pancreatitis | Yes | 2 | 2.3% |
| Pancreatic fistula | Yes | 2 | 2.3% |
| Deep vein thrombosis | Yes | 4 | 4.5% |
| Surgical site infection | Yes | 9 | 10.2% |
| Mortality (90 d) | Yes | 1 | 1.1% |
| Reoperation | Yes | 12 | 13.6% |
| Total | 88 | 100.0% | |
| Variable | Category | Univariable Regression | Multivariable Regression | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR * | Lower 95%-CI | Upper 95%-CI | p | HR * | Lower 95%-CI | Upper 95%-CI | p | ||
| CCR score | CCR-0 | 1.000 | 1.000 | ||||||
| CCR-1/2/3 | 1.289 | 0.631 | 2.633 | 0.486 | 0.718 | 0.238 | 2.166 | 0.557 | |
| HIPEC duration | HIPEC 60 min | 1.000 | 1.000 | ||||||
| HIPEC 90 min | 0.541 | 0.300 | 0.978 | 0.042 | 3.048 | 0.569 | 16.343 | 0.193 | |
| HIPEC substances & | Cisplatin | 1.000 | 0.032 | 0.114 | |||||
| Cisplatin + doxorubicin | 2.269 | 1.230 | 4.186 | 0.009 | 5.788 | 1.068 | 31.380 | 0.042 $ | |
| Gemcitab./mytomycin | 1.687 | 0.493 | 5.774 | 0.405 | 4.385 | 0.411 | 46.806 | 0.221 | |
| Age at surgery | <50 | 1.000 | 0.098 | 1.000 | 0.081 | ||||
| 50–59 | 1.154 | 0.565 | 2.356 | 0.694 | 1.272 | 0.523 | 3.096 | 0.596 | |
| 60–69 | 0.444 | 0.180 | 1.094 | 0.078 | 0.332 | 0.122 | 0.901 | 0.030 $ | |
| ≥70 | 1.497 | 0.523 | 4.284 | 0.452 | 1.137 | 0.318 | 4.068 | 0.844 | |
| BMI | <25.0 | 1.000 | 0.095 | 1.000 | 0.421 | ||||
| 25.0–29.9 | 1.076 | 0.530 | 2.187 | 0.839 | 1.250 | 0.519 | 3.011 | 0.619 | |
| ≥30.0 | 2.155 | 1.049 | 4.428 | 0.037 | 1.876 | 0.734 | 4.793 | 0.189 | |
| ASA | ASA 0–2 | 1.000 | 1.000 | ||||||
| ASA 3 | 1.945 | 1.048 | 3.610 | 0.035 | 1.251 | 0.545 | 2.871 | 0.597 | |
| Histology | High-grade serous Ca | 1.000 | 1.000 | ||||||
| Others | 2.959 | 1.025 | 8.540 | 0.045 | 2.555 | 0.558 | 11.714 | 0.227 | |
| Initial FIGO stage | I | 1.000 | 0.409 | 1.000 | 0.796 | ||||
| II | 1.624 | 0.523 | 5.038 | 0.401 | 0.698 | 0.166 | 2.937 | 0.624 | |
| III/IV | 1.783 | 0.689 | 4.610 | 0.233 | 1.019 | 0.302 | 3.443 | 0.975 | |
| PCI | 0–9 | 1.000 | 0.528 | 1.000 | 0.382 | ||||
| 10–19 | 0.689 | 0.328 | 1.451 | 0.327 | 1.087 | 0.407 | 2.905 | 0.868 | |
| ≥20 | 1.092 | 0.531 | 2.244 | 0.812 | 1.951 | 0.697 | 5.461 | 0.203 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acs, M.; Gerken, M.; Schmitt, V.; Piso, P.; Königsrainer, A.; Baransi, S.; Yurttas, C.; Häusler, S.; Horvath, P. Role of HIPEC after Complete Cytoreductive Surgery (CRS) in Peritoneal Recurrence of Platinum-Sensitive Recurrent Ovarian Cancer (OC): The Aim for Standardization at Two Reference Centers for CRS. Cancers 2023, 15, 405. https://doi.org/10.3390/cancers15020405
Acs M, Gerken M, Schmitt V, Piso P, Königsrainer A, Baransi S, Yurttas C, Häusler S, Horvath P. Role of HIPEC after Complete Cytoreductive Surgery (CRS) in Peritoneal Recurrence of Platinum-Sensitive Recurrent Ovarian Cancer (OC): The Aim for Standardization at Two Reference Centers for CRS. Cancers. 2023; 15(2):405. https://doi.org/10.3390/cancers15020405
Chicago/Turabian StyleAcs, Miklos, Michael Gerken, Vanessa Schmitt, Pompiliu Piso, Alfred Königsrainer, Saher Baransi, Can Yurttas, Sebastian Häusler, and Philipp Horvath. 2023. "Role of HIPEC after Complete Cytoreductive Surgery (CRS) in Peritoneal Recurrence of Platinum-Sensitive Recurrent Ovarian Cancer (OC): The Aim for Standardization at Two Reference Centers for CRS" Cancers 15, no. 2: 405. https://doi.org/10.3390/cancers15020405
APA StyleAcs, M., Gerken, M., Schmitt, V., Piso, P., Königsrainer, A., Baransi, S., Yurttas, C., Häusler, S., & Horvath, P. (2023). Role of HIPEC after Complete Cytoreductive Surgery (CRS) in Peritoneal Recurrence of Platinum-Sensitive Recurrent Ovarian Cancer (OC): The Aim for Standardization at Two Reference Centers for CRS. Cancers, 15(2), 405. https://doi.org/10.3390/cancers15020405