
Midline Gliomas: A Retrospective Study from a Cancer Center in the Middle East
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Setting, and Participants
2.2. Pathology and Immunohistochemistry
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Included Participants
3.2. Univariate Analysis
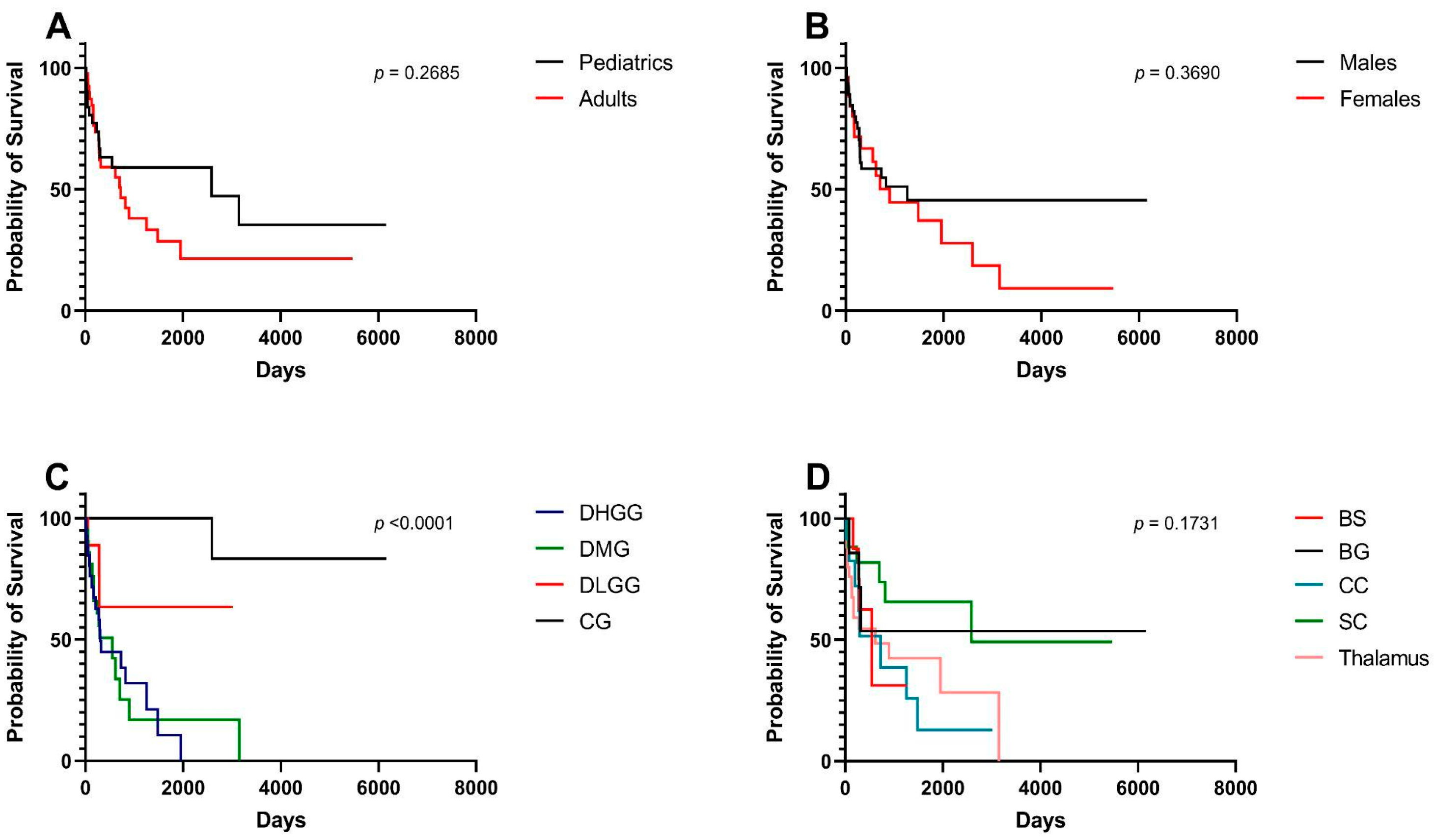
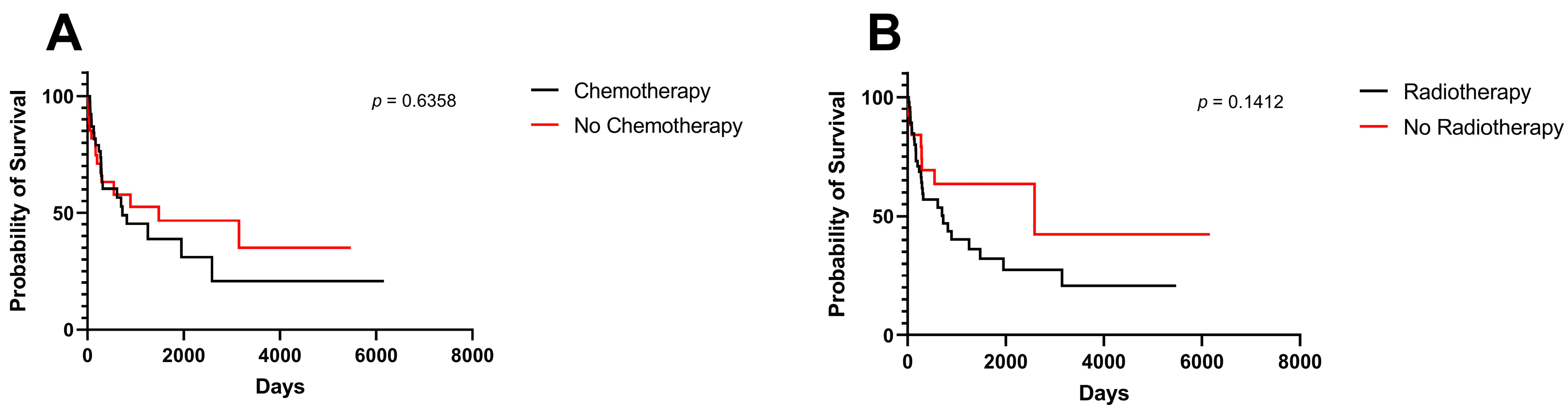
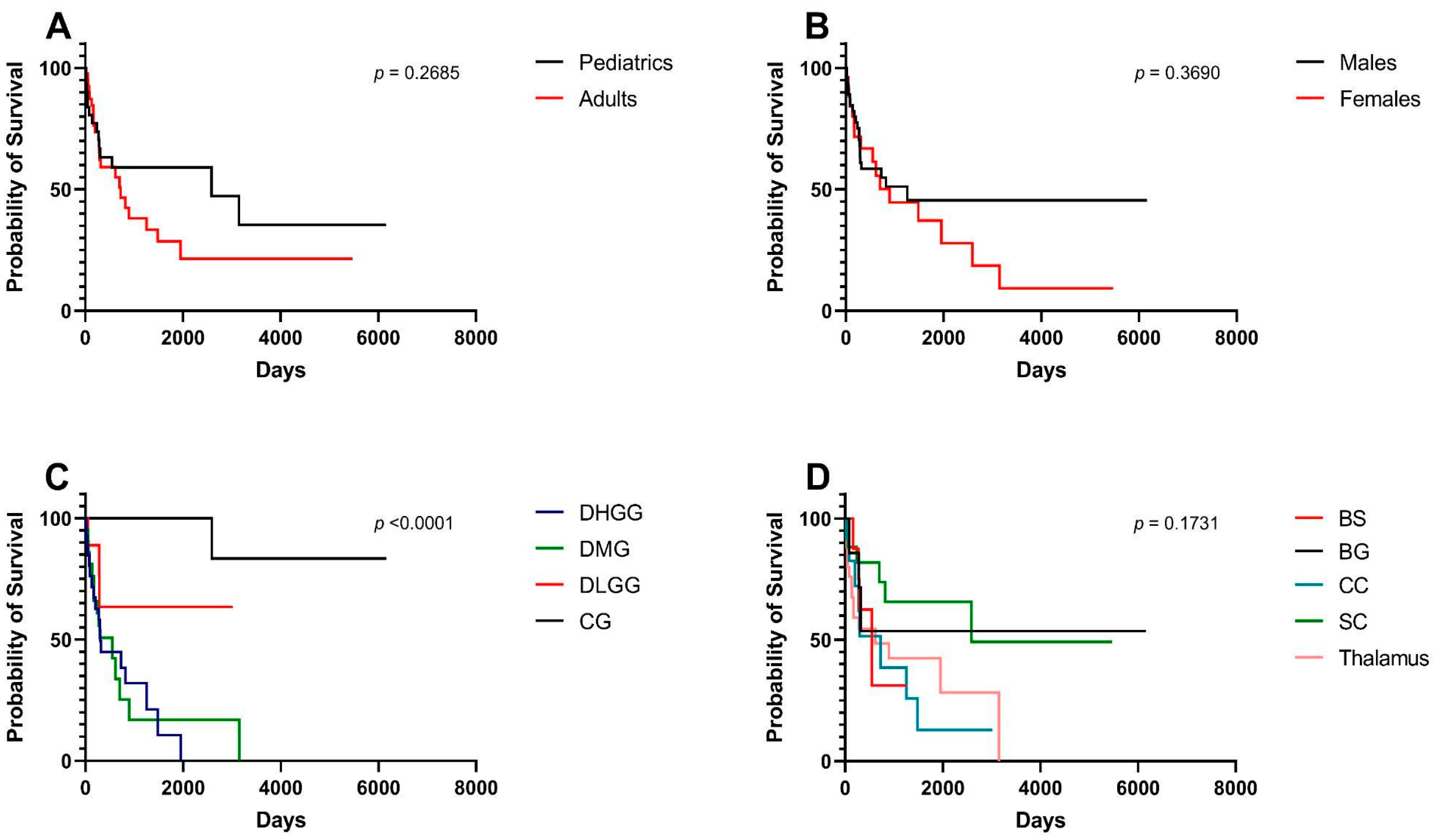
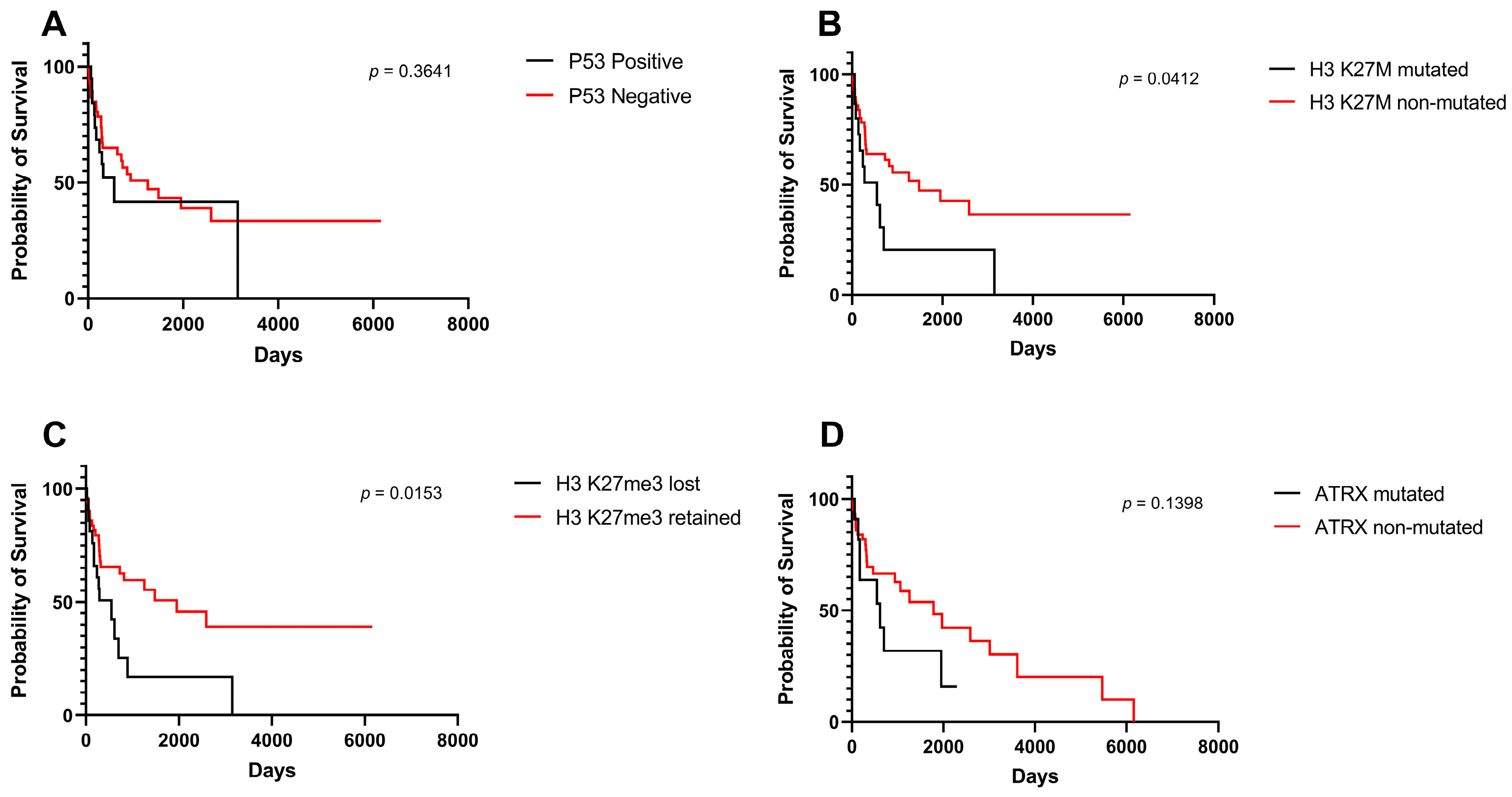
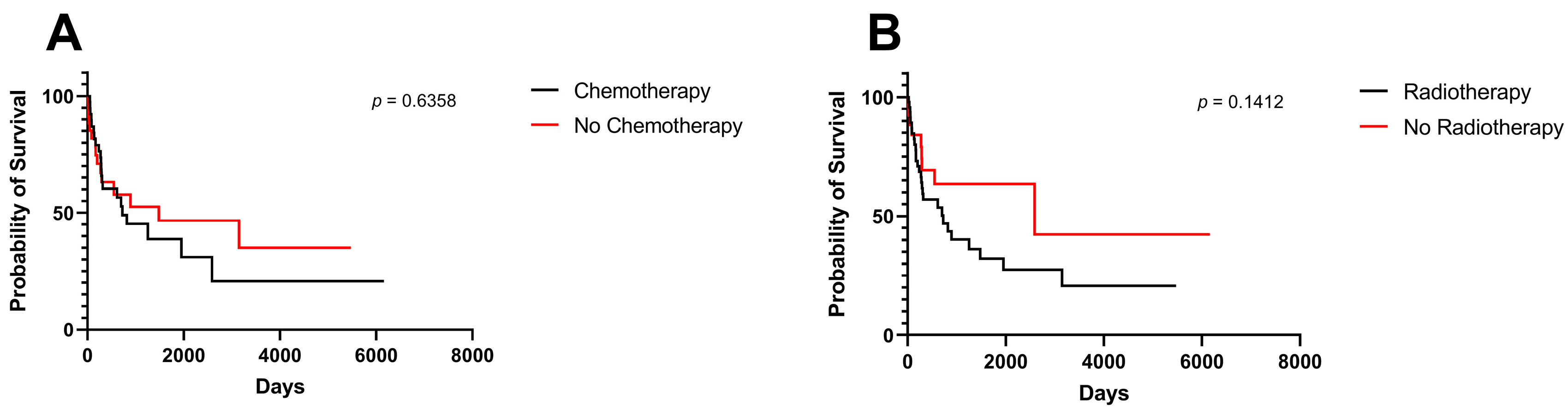
3.3. Survival Analysis
3.4. Multivariate Survival Analysis
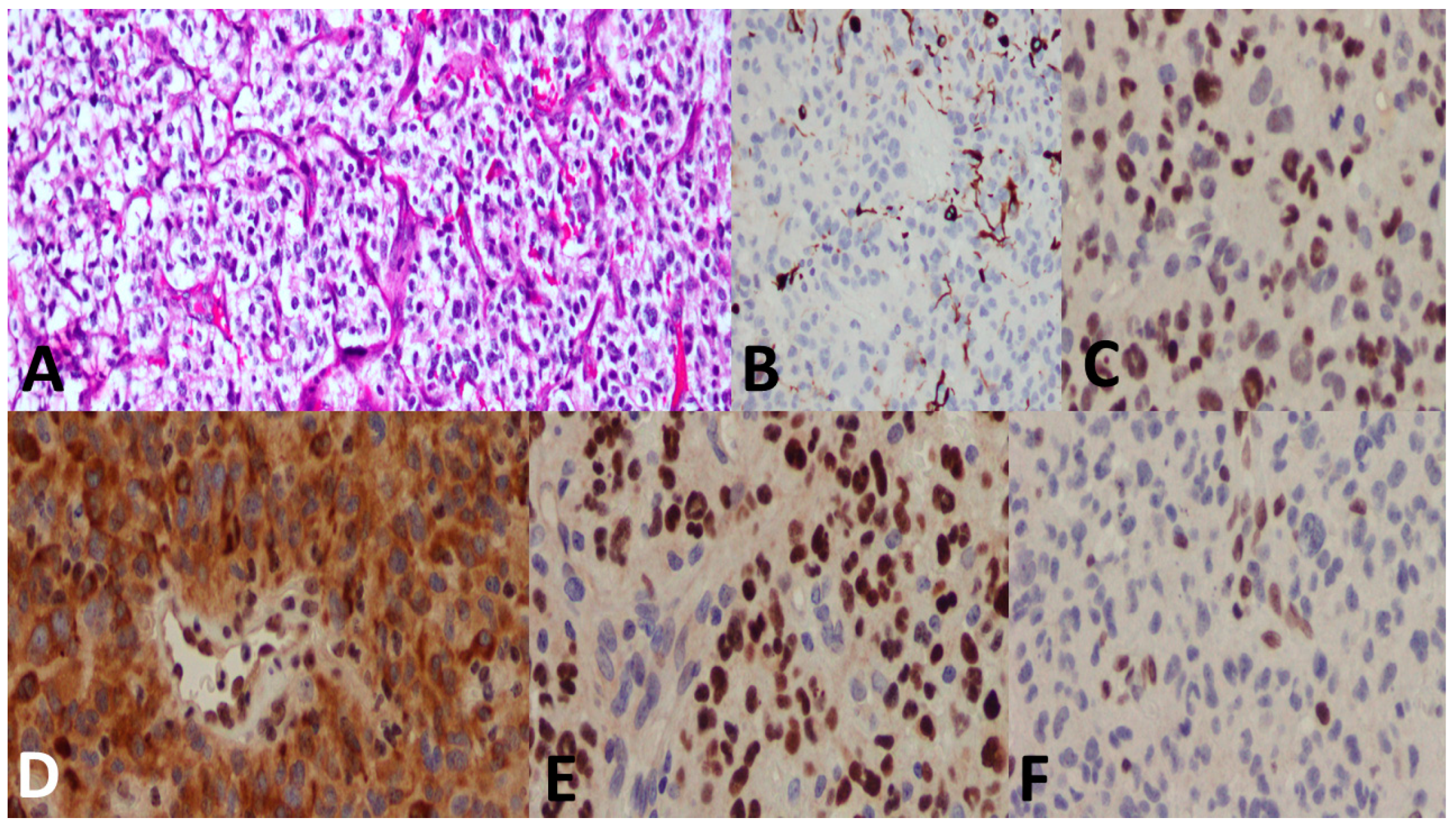
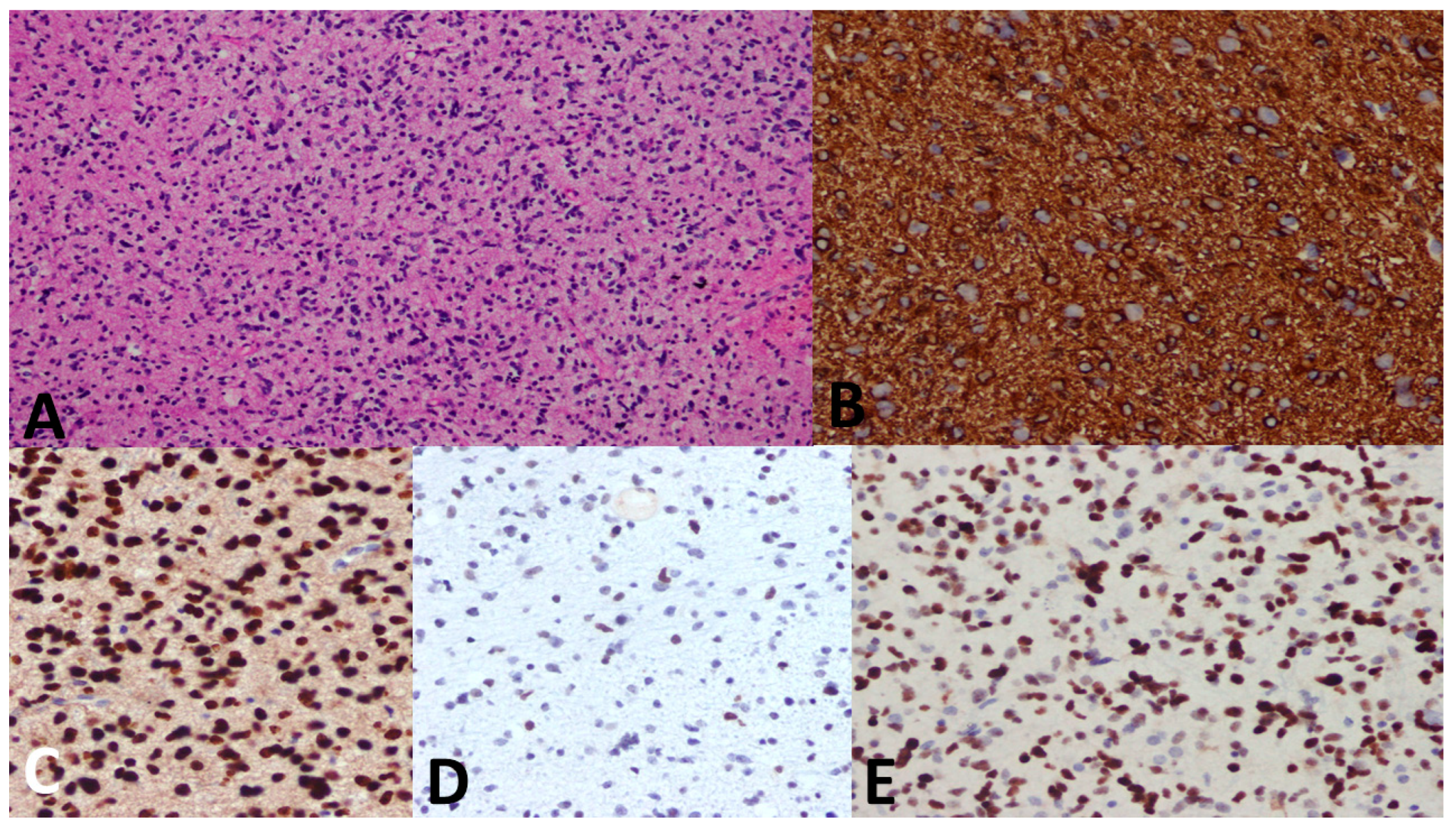
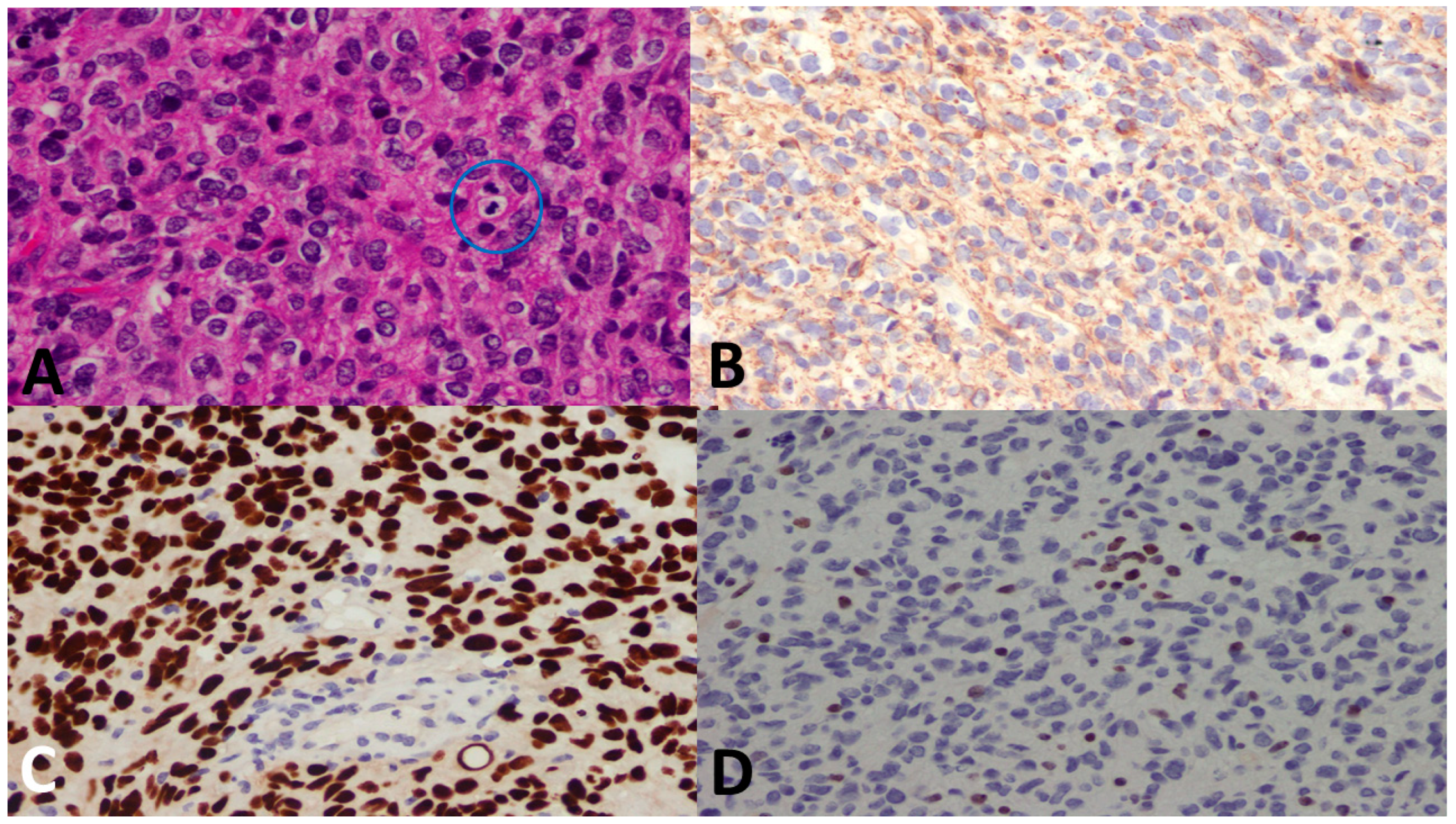
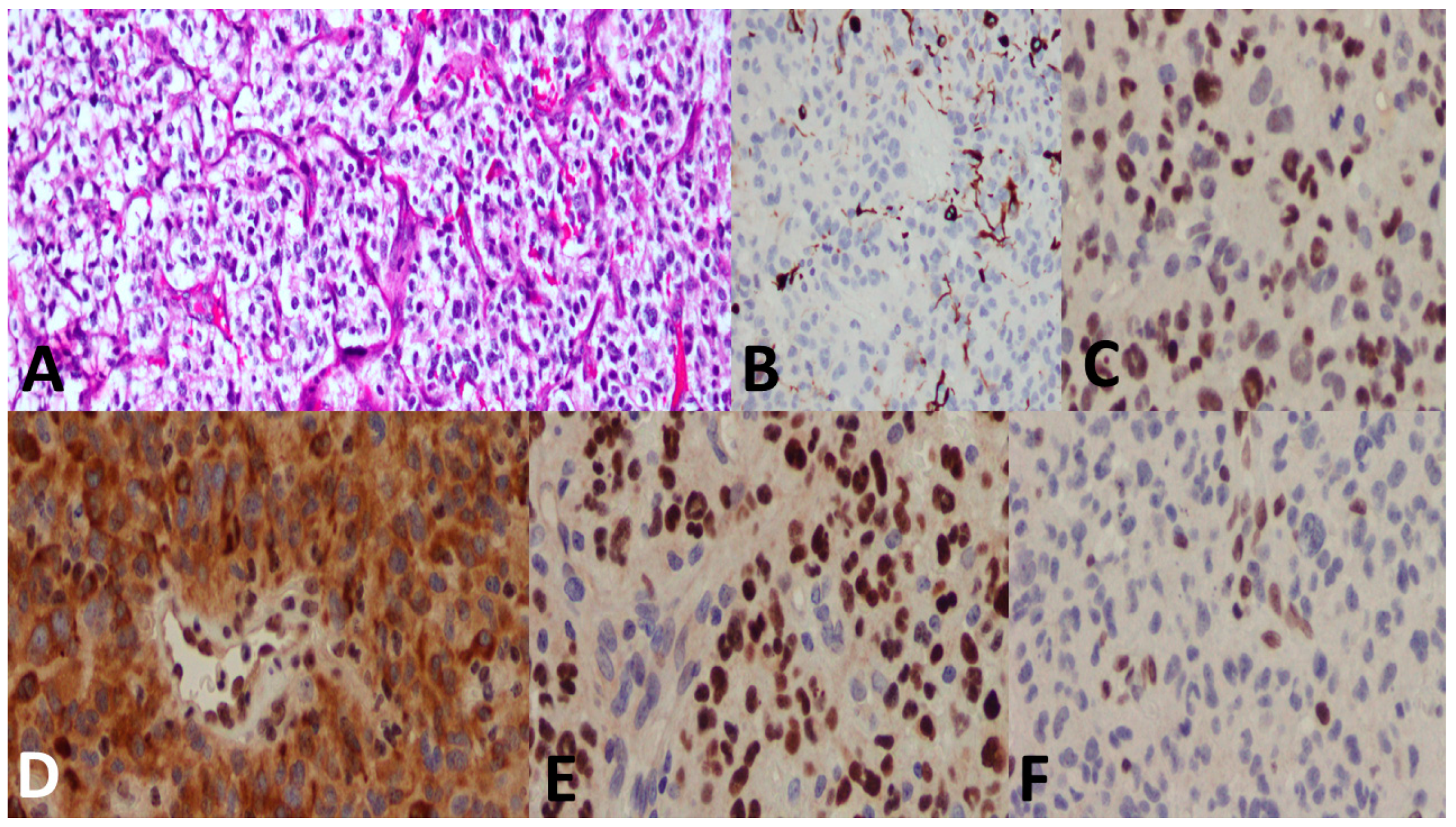
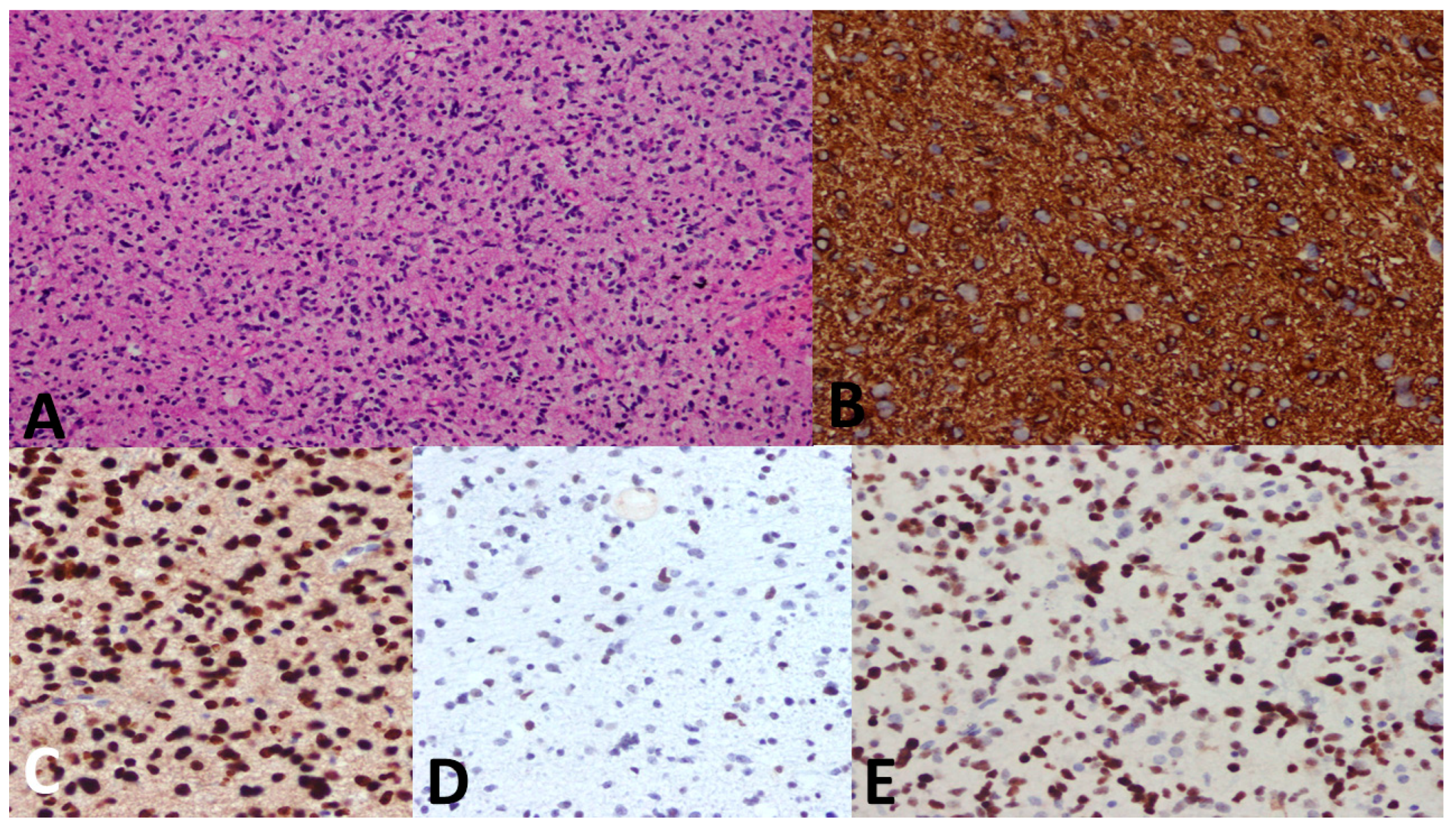
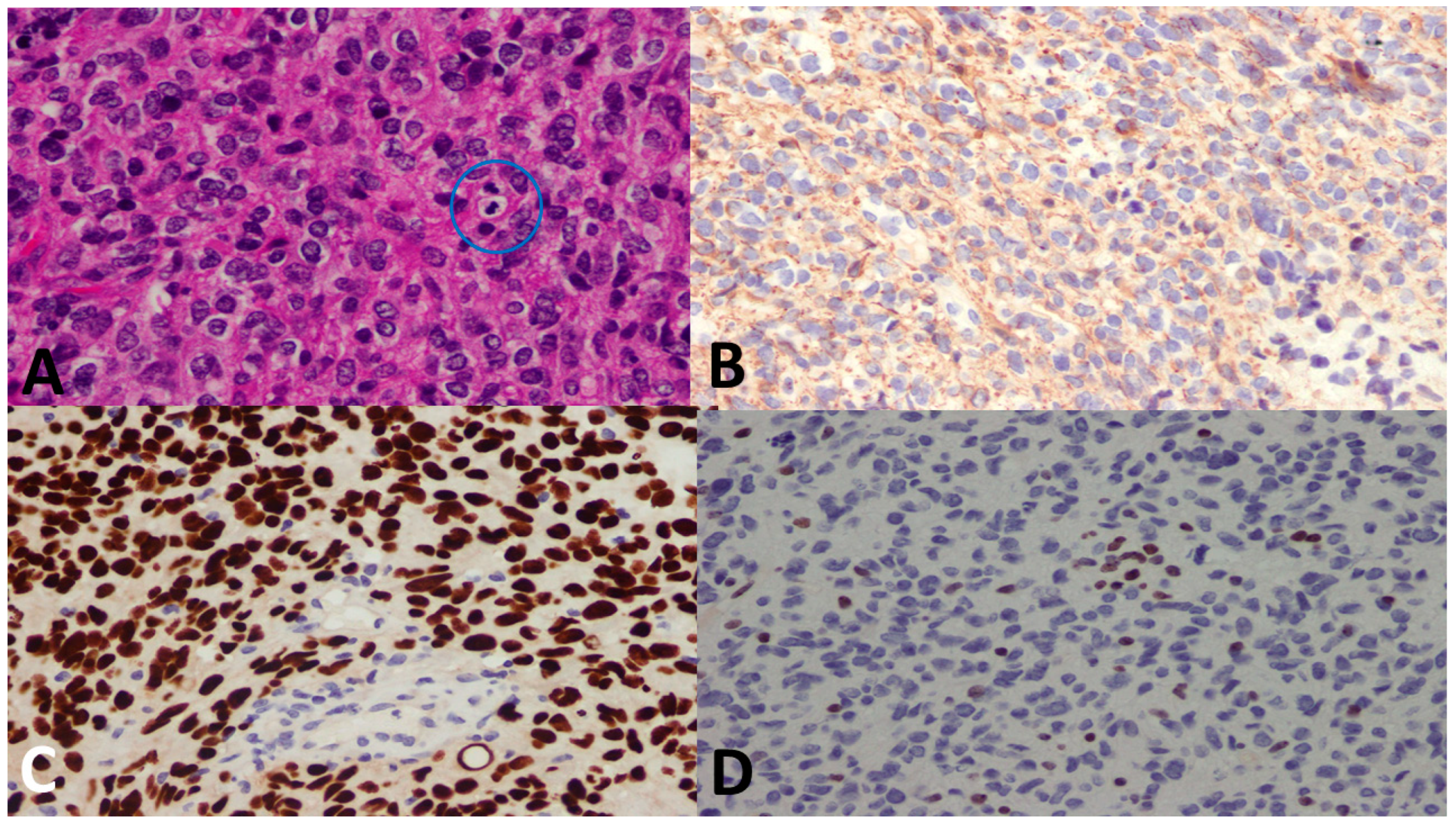
3.5. Pathological Examples of DMG in Various Locations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santisukwongchote, S.; Teerapakpinyo, C.; Chankate, P.; Techavichit, P.; Boongird, A.; Sathornsumetee, S.; Thammachantha, S.; Cheunsuchon, P.; Tanboon, J.; Thorner, P.S.; et al. Simplified approach for pathological diagnosis of diffuse gliomas in adult patients. Pathol. Res. Pract. 2021, 223, 153483. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef]
- Louis, D.N.; Giannini, C.; Capper, D.; Paulus, W.; Figarella-Branger, D.; Lopes, M.B.; Batchelor, T.T.; Cairncross, J.G.; van den Bent, M.; Wick, W.; et al. cIMPACT-NOW update 2: Diagnostic clarifications for diffuse midline glioma, H3 K27M-mutant and diffuse astrocytoma/anaplastic astrocytoma, IDH-mutant. Acta Neuropathol. 2018, 135, 639–642. [Google Scholar] [CrossRef]
- Buczkowicz, P.; Hoeman, C.; Rakopoulos, P.; Pajovic, S.; Letourneau, L.; Dzamba, M.; Morrison, A.; Lewis, P.; Bouffet, E.; Bartels, U.; et al. Genomic analysis of diffuse intrinsic pontine gliomas identifies three molecular subgroups and recurrent activating ACVR1 mutations. Nat. Genet. 2014, 46, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Kazarian, E.; Marks, A.; Cui, J.; Darbinyan, A.; Tong, E.; Mueller, S.; Cha, S.; Aboian, M.S. Topographic correlates of driver mutations and endogenous gene expression in pediatric diffuse midline gliomas and hemispheric high-grade gliomas. Sci. Rep. 2021, 11, 14377. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.A.; Wood, M.D.; Tihan, T.; Bollen, A.W.; Gupta, N.; Phillips, J.J.; Perry, A. Diffuse Midline Gliomas with Histone H3-K27M Mutation: A Series of 47 Cases Assessing the Spectrum of Morphologic Variation and Associated Genetic Alterations. Brain Pathol. 2016, 26, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Venneti, S.; Garimella, M.T.; Sullivan, L.M.; Martinez, D.; Huse, J.T.; Heguy, A.; Santi, M.; Thompson, C.B.; Judkins, A.R. Evaluation of histone 3 lysine 27 trimethylation (H3K27me3) and enhancer of Zest 2 (EZH2) in pediatric glial and glioneuronal tumors shows decreased H3K27me3 in H3F3A K27M mutant glioblastomas. Brain Pathol. 2013, 23, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Di Ruscio, V.; Del Baldo, G.; Fabozzi, F.; Vinci, M.; Cacchione, A.; de Billy, E.; Megaro, G.; Carai, A.; Mastronuzzi, A. Pediatric Diffuse Midline Gliomas: An Unfinished Puzzle. Diagnostics 2022, 12, 2064. [Google Scholar] [CrossRef]
- Argersinger, D.P.; Rivas, S.R.; Shah, A.H.; Jackson, S.; Heiss, J.D. New Developments in the Pathogenesis, Therapeutic Targeting, and Treatment of H3K27M-Mutant Diffuse Midline Glioma. Cancers 2021, 13, 5280. [Google Scholar] [CrossRef]
- López-Pérez, C.A.; Franco-Mojica, X.; Villanueva-Gaona, R.; Díaz-Alba, A.; Rodríguez-Florido, M.A.; Navarro, V.G. Adult diffuse midline gliomas H3 K27-altered: Review of a redefined entity. J. Neurooncol. 2022, 158, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Price, G.; Bouras, A.; Hambardzumyan, D.; Hadjipanayis, C.G. Current knowledge on the immune microenvironment and emerging immunotherapies in diffuse midline glioma. eBioMedicine 2021, 69, 103453. [Google Scholar] [CrossRef] [PubMed]
- Valério, E.; Alves de Castro, J.V.; Carraro, D.M.; Torrezan, G.T.; Kulikowski, L.D.; Costa, F.D. Beyond Midline: Diffuse Hemispheric Glioma, H3 K27M-Mutant with Aggressive Behavior. J. Neuropathol. Exp. Neurol. 2022, 81, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Santosh, V.; Nicholas, G.G. Diffuse Intrinsic Pontine Glioma. In Brain Tumors; Amit, A., Luis Rafael, M.-S., Eds.; IntechOpen: Rijeka, Croatia, 2018; Chapter 2. [Google Scholar]
- Vitanza, N.A.; Biery, M.C.; Myers, C.; Ferguson, E.; Zheng, Y.; Girard, E.J.; Przystal, J.M.; Park, G.; Noll, A.; Pakiam, F.; et al. Optimal therapeutic targeting by HDAC inhibition in biopsy-derived treatment-naïve diffuse midline glioma models. Neuro-oncology 2021, 23, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Pratt, D.; Natarajan, S.K.; Banda, A.; Giannini, C.; Vats, P.; Koschmann, C.; Mody, R.; Chinnaiyan, A.; Venneti, S. Circumscribed/non-diffuse histology confers a better prognosis in H3K27M-mutant gliomas. Acta Neuropathol. 2018, 135, 299–301. [Google Scholar] [CrossRef]
- Zhao, B.; Sun, K.; Zhang, Z.; Xu, T.; Zhao, L.; Liu, C.; Xiao, Y. A rare presentation of primary lateral ventricle H3 K27-altered diffuse midline glioma in a 14-year-old girl: A case description. Quant. Imaging Med. Surg. 2022, 12, 5288–5295. [Google Scholar] [CrossRef]
- Abdel-Razeq, H.; Attiga, F.; Mansour, A. Cancer care in Jordan. Hematol. Oncol. Stem Cell Ther. 2015, 8, 64–70. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011–2015. Neuro-Oncology 2018, 20, iv1–iv86. [Google Scholar] [CrossRef]
- Hoffman, L.M.; Veldhuijzen van Zanten, S.E.M.; Colditz, N.; Baugh, J.; Chaney, B.; Hoffmann, M.; Lane, A.; Fuller, C.; Miles, L.; Hawkins, C.; et al. Clinical, Radiologic, Pathologic, and Molecular Characteristics of Long-Term Survivors of Diffuse Intrinsic Pontine Glioma (DIPG): A Collaborative Report From the International and European Society for Pediatric Oncology DIPG Registries. J. Clin. Oncol. 2018, 36, 1963–1972. [Google Scholar] [CrossRef]
- Picca, A.; Berzero, G.; Bielle, F.; Touat, M.; Savatovsky, J.; Polivka, M.; Trisolini, E.; Meunier, S.; Schmitt, Y.; Idbaih, A.; et al. FGFR1 actionable mutations, molecular specificities, and outcome of adult midline gliomas. Neurology 2018, 90, e2086–e2094. [Google Scholar] [CrossRef]
- Dono, A.; Takayasu, T.; Ballester, L.Y.; Esquenazi, Y. Adult diffuse midline gliomas: Clinical, radiological, and genetic characteristics. J. Clin. Neurosci. 2020, 82, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schreck, K.C.; Ranjan, S.; Skorupan, N.; Bettegowda, C.; Eberhart, C.G.; Ames, H.M.; Holdhoff, M. Incidence and clinicopathologic features of H3 K27M mutations in adults with radiographically-determined midline gliomas. J. Neuro-Oncol. 2019, 143, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Cooney, T.; Lane, A.; Bartels, U.; Bouffet, E.; Goldman, S.; Leary, S.E.S.; Foreman, N.K.; Packer, R.J.; Broniscer, A.; Minturn, J.E.; et al. Contemporary survival endpoints: An International Diffuse Intrinsic Pontine Glioma Registry study. Neuro Oncol. 2017, 19, 1279–1280. [Google Scholar] [CrossRef] [PubMed]
- Johung, T.B.; Monje, M. Diffuse Intrinsic Pontine Glioma: New Pathophysiological Insights and Emerging Therapeutic Targets. Curr. Neuropharmacol. 2017, 15, 88–97. [Google Scholar] [CrossRef]
- Castel, D.; Philippe, C.; Kergrohen, T.; Sill, M.; Merlevede, J.; Barret, E.; Puget, S.; Sainte-Rose, C.; Kramm, C.M.; Jones, C.; et al. Transcriptomic and epigenetic profiling of ‘diffuse midline gliomas, H3 K27M-mutant’ discriminate two subgroups based on the type of histone H3 mutated and not supratentorial or infratentorial location. Acta Neuropathol. Commun. 2018, 6, 117. [Google Scholar] [CrossRef]
- Zheng, L.; Gong, J.; Yu, T.; Zou, Y.; Zhang, M.; Nie, L.; Chen, X.; Yue, Q.; Liu, Y.; Mao, Q.; et al. Diffuse Midline Gliomas with Histone H3 K27M Mutation in Adults and Children: A Retrospective Series of 164 Cases. Am. J. Surg. Pathol. 2022, 46, 863–871. [Google Scholar] [CrossRef]
- Chia, N.; Wong, A.; Teo, K.; Tan, A.P.; Vellayappan, B.A.; Yeo, T.T.; Oh, S.Y.; Tan, C.L. H3K27M-mutant, hemispheric diffuse glioma in an adult patient with prolonged survival. Neurooncol. Adv. 2021, 3, vdab135. [Google Scholar] [CrossRef]
- Wang, Y.; Feng, L.L.; Ji, P.G.; Liu, J.H.; Guo, S.C.; Zhai, Y.L.; Sankey, E.W.; Wang, Y.; Xue, Y.R.; Wang, N.; et al. Clinical Features and Molecular Markers on Diffuse Midline Gliomas with H3K27M Mutations: A 43 Cases Retrospective Cohort Study. Front. Oncol. 2020, 10, 602553. [Google Scholar] [CrossRef]
- Nguyen, A.T.; Colin, C.; Nanni-Metellus, I.; Padovani, L.; Maurage, C.A.; Varlet, P.; Miquel, C.; Uro-Coste, E.; Godfraind, C.; Lechapt-Zalcman, E.; et al. Evidence for BRAF V600E and H3F3A K27M double mutations in paediatric glial and glioneuronal tumours. Neuropathol. Appl. Neurobiol. 2015, 41, 403–408. [Google Scholar] [CrossRef]
- Orillac, C.; Thomas, C.; Dastagirzada, Y.; Hidalgo, E.T.; Golfinos, J.G.; Zagzag, D.; Wisoff, J.H.; Karajannis, M.A.; Snuderl, M. Pilocytic astrocytoma and glioneuronal tumor with histone H3 K27M mutation. Acta Neuropathol. Commun. 2016, 4, 84. [Google Scholar] [CrossRef]
- Hochart, A.; Escande, F.; Rocourt, N.; Grill, J.; Koubi-Pick, V.; Beaujot, J.; Meignan, S.; Vinchon, M.; Maurage, C.A.; Leblond, P. Long survival in a child with a mutated K27M-H3.3 pilocytic astrocytoma. Ann. Clin. Transl. Neurol. 2015, 2, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Kleinschmidt-DeMasters, B.K.; Mulcahy Levy, J.M. H3 K27M-mutant gliomas in adults vs. children share similar histological features and adverse prognosis. Clin. Neuropathol. 2018, 37, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, H.; Tan, J.; Lai, M.; Chen, W.; Liu, M.; Zhou, Z.; Deng, D.; Cheng, B.; Fan, C. The Biological Behavior of High-Grade Glioma in H3K27M Mutant Circumscribed Midline Gliomas; Research Square: Durham, NC, USA, 2022. [Google Scholar]
- Long, W.; Yi, Y.; Chen, S.; Cao, Q.; Zhao, W.; Liu, Q. Potential New Therapies for Pediatric Diffuse Intrinsic Pontine Glioma. Front. Pharmacol. 2017, 8, 495. [Google Scholar] [CrossRef] [PubMed]
- Cohen, K.J.; Broniscer, A.; Glod, J. Pediatric glial tumors. Curr. Treat. Opt. Oncol. 2001, 2, 529–536. [Google Scholar] [CrossRef]
- Vanan, M.I.; Underhill, D.A.; Eisenstat, D.D. Targeting Epigenetic Pathways in the Treatment of Pediatric Diffuse (High Grade) Gliomas. Neurotherapeutics 2017, 14, 274–283. [Google Scholar] [CrossRef]
- Mohammad, F.; Weissmann, S.; Leblanc, B.; Pandey, D.P.; Højfeldt, J.W.; Comet, I.; Zheng, C.; Johansen, J.V.; Rapin, N.; Porse, B.T.; et al. EZH2 is a potential therapeutic target for H3K27M-mutant pediatric gliomas. Nat. Med. 2017, 23, 483–492. [Google Scholar] [CrossRef]
- Bernstock, J.D.; Hoffman, S.E.; Kappel, A.D.; Valdes, P.A.; Essayed, W.; Klinger, N.V.; Kang, K.D.; Totsch, S.K.; Olsen, H.E.; Schlappi, C.W.; et al. Immunotherapy approaches for the treatment of diffuse midline gliomas. Oncoimmunology 2022, 11, 2124058. [Google Scholar] [CrossRef]
- Noon, A.; Galban, S. Therapeutic avenues for targeting treatment challenges of diffuse midline gliomas. Neoplasia 2023, 40, 100899. [Google Scholar] [CrossRef]
- Prabhu, V.V.; Morrow, S.; Rahman Kawakibi, A.; Zhou, L.; Ralff, M.; Ray, J.; Jhaveri, A.; Ferrarini, I.; Lee, Y.; Parker, C.; et al. ONC201 and imipridones: Anti-cancer compounds with clinical efficacy. Neoplasia 2020, 22, 725–744. [Google Scholar] [CrossRef]
- El-Soussi, S.; Hanna, R.; Semaan, H.; Khater, A.R.; Abdallah, J.; Abou-Kheir, W.; Abou-Antoun, T. A Novel Therapeutic Mechanism of Imipridones ONC201/ONC206 in MYCN-Amplified Neuroblastoma Cells via Differential Expression of Tumorigenic Proteins. Front. Pediatr. 2021, 9, 693145. [Google Scholar] [CrossRef]
- Mueller, T.; Laternser, S.; Guerreiro Stücklin, A.S.; Gerber, N.U.; Mourabit, S.; Rizo, M.; Rushing, E.J.; Kottke, R.; Grotzer, M.; Krayenbühl, N.; et al. Real-time drug testing of paediatric diffuse midline glioma to support clinical decision making: The Zurich DIPG/DMG centre experience. Eur. J. Cancer 2023, 178, 171–179. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 104) n, % | Thalamic (n = 31) n, % | Brainstem (n = 13) n, % | Spinal Cord (n = 23) n, % | Basal Ganglia (n = 10) n, % | Corpus Callosum (n = 22) n, % | Other (n = 5) n, % | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Median age in years (IQR) | 23 (10–48) | 18 (3–69) | 9 (2–63) | 8 (1–48) | 48 (6–60) | 53 (20–74) | 18 (15–56) | 0.698 |
| Age Group | 0.001 | |||||||
| Adults | 56 (58.33%) | 15 (48.38%) | 5 (38.46%) | 9 (39.13%) | 7 (78%) | 17 (100%) | 3 (60%) | |
| Pediatrics | 40 (41.67%) | 14 (51.62%) | 8 (61.54%) | 14 (60.87%) | 2 (22%) | 0 (0%) | 2 (40%) | |
| Gender | 0.405 | |||||||
| Male | 64 (61.54%) | 17 (54.84%) | 7 (53.85%) | 12 (52.17%) | 8 (80%) | 16 (72.73%) | 4 (75%) | |
| Female | 40 (38.46%) | 14 (45.16%) | 6 (46.15%) | 11 (47.83%) | 2 (20%) | 6 (27.27%) | 1 (25%) | |
| Diagnostic Entity | 0.000 | |||||||
| Circumscribed glioma | 21 (20.19%) | 4 (12.9%) | 5 (38.46%) | 10 (43.48%) | 2 (20%) | 0 (0%) | 0 (0%) | |
| Diffuse midline glioma | 30 (28.85%) | 17 (54.84%) | 5 (38.46%) | 8 (34.78%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Diffuse high-grade glioma | 43 (41.35%) | 8 (25.81%) | 2 (15.39%) | 3 (13.04%) | 4 (40%) | 21 (95.45%) | 5 (100%) | |
| Diffuse low-grade glioma | 10 (9.61%) | 2 (6.45%) | 1 (7.69%) | 2 (8.7%) | 4 (40%) | 1 (4.55%) | 0 (0%) | |
| Immunohistochemistry | ||||||||
| GFAP | 74 (71.15%) | 27 (87.1%) | 13 (100%) | 20 (86.96%) | 8 (80%) | 2 (9.1%) | 4 (80%) | 0.000 |
| IDH1 (p.R132H) | 2 (1.92%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (20%) | 0 (0%) | 0 (0%) | 0.002 |
| p53 | 26 (25%) | 11 (35.48%) | 4 (30.77%) | 4 (17.39%) | 5 (50%) | 1 (4.55%) | 1 (20%) | 0.050 |
| ATRX | 12 (11.54%) | 9 (29.03%) | 1 (7.69%) | 2 (8.7%) | 0 (0%) | 0 (0%) | 0 (0%) | 0.013 |
| H3 K27M | 21 (20.19%) | 11 (35.48%) | 4 (30.77%) | 6 (26.09%) | 0 (0%) | 0 (0%) | 0 (0%) | 0.009 |
| H3 K27me3 | 30 (28.85%) | 17 (54.84%) | 5 (38.46%) | 8 (34.78%) | 0 (0%) | 0 (0%) | 0 (0%) | 0.000 |
| Intervention | ||||||||
| Chemotherapy | 44 (42.31%) | 11 (35.48%) | 3 (23.08%) | 13 (56.52%) | 8 (80%) | 6 (27.27%) | 3 (60%) | 0.024 |
| Radiotherapy | 54 (51.92%) | 14 (45.16%) | 2 (15.39%) | 12 (52.17%) | 8 (80%) | 15 (68.18%) | 3 (60%) | 0.022 |
| Outcome | 0.208 | |||||||
| Alive | 26 (25%) | 7 (22.58%) | 3 (23.08%) | 10 (43.48%) | 3 (30%) | 1 (4.55%) | 2 (40%) | |
| Dead | 45 (43.27%) | 16 (51.61%) | 4 (30.77%) | 8 (34.78%) | 5 (50%) | 10 (45.45%) | 2 (40%) | |
| Lost to Follow-up | 33 (31.73%) | 7 (25.81%) | 6 (46.15%) | 5 (21.74%) | 2 (20%) | 11 (50%) | 1 (20%) |
| Total (n = 104) n, % | Diffuse Midline Glioma (n = 30) n, % | Diffuse High-Grade Glioma (n = 43) n, % | Diffuse Low-Grade Glioma (n = 10) n, % | Circumscribed Glioma (n = 21) n, % | p-Value | |
|---|---|---|---|---|---|---|
| Median age in years (IQR) | 23 (10–48) | 19.5 (3–67) | 46 (2–74) | 45.5 (2–59) | 8 (1–48) | 0.202 |
| Age group | 0.001 | |||||
| Adult | 56 (58.33%) | 17 (56.67%) | 29 (80.55%) | 5 (55.56%) | 5 (23.81%) | |
| Pediatric | 40 (41.67%) | 13 (43.33%) | 7 (19.45%) | 4 (44.44%) | 16 (76.19%) | |
| Gender | 0.269 | |||||
| Male | 64 (61.54%) | 15 (50%) | 29 (67.44%) | 8 (80%) | 12 (57.14%) | |
| Female | 40 (38.46%) | 15 (50%) | 14 (32.56%) | 2 (20%) | 9 (42.86%) | |
| Location | 0.000 | |||||
| Thalamic | 31 (29.8%) | 17 (56.67%) | 8 (18.6%) | 2 (20%) | 4 (19.05%) | |
| Brainstem | 13 (12.5%) | 5 (16.66%) | 2 (4.65%) | 1 (10%) | 5 (23.81%) | |
| Spinal Cord | 23 (22.1%) | 8 (26.67%) | 3 (6.98%) | 2 (20%) | 10 (47.62%) | |
| Basal Ganglia | 10 (9.6%) | 0 (0%) | 4 (9.4%) | 4 (40%) | 2 (9.52%) | |
| Corpus Callosum | 22 (21.2%) | 0 (0%) | 21 (48.83%) | 1 (10%) | 0 (0%) | |
| Other | 5 (4.8%) | 0 (0%) | 5 (11.63%) | 0 (0%) | 0 (0%) | |
| Immunohistochemistry | ||||||
| GFAP | 74 (71.15%) | 28 (93.33%) | 21 (48.84%) | 6 (60%) | 19 (90.48%) | 0.000 |
| IDH1 | 2 (1.92%) | 0 (0%) | 0 (0%) | 2 (20%) | 0 (0%) | 0.000 |
| p53 | 26 (25%) | 15 (50%) | 10 (23.26%) | 1 (10%) | 0 (0%) | 0.000 |
| ATRX | 12 (11.54%) | 10 (33.33%) | 2 (4.65%) | 0 (0%) | 0 (0%) | 0.000 |
| H3 K27M | 21 (20.19%) | 21 (70%) | 0 (0%) | 0 (0%) | 0 (0%) | 0.000 |
| H3 K27me3 | 30 (28.85%) | 30 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 0.000 |
| Intervention | ||||||
| Chemotherapy | 44 (42.31%) | 11 (36.67%) | 20 (46.51%) | 5 (50%) | 8 (38.1%) | 0.778 |
| Radiotherapy | 54 (51.92%) | 15 (50%) | 29 (67.44%) | 6 (60%) | 4 (19.05%) | 0.004 |
| Outcome | 0.001 | |||||
| Alive | 26 (25%) | 6 (20%) | 7 (16.28%) | 4 (40%) | 9 (42.86%) | |
| Dead | 45 (43.27%) | 18 (60%) | 23 (53.49%) | 3 (30%) | 1 (4.76%) | |
| Lost to Follow-up | 33 (31.73%) | 6 (20%) | 13 (30.23%) | 3 (30%) | 11 (52.38%) |
| HR | p-Value | 95% CI | |
|---|---|---|---|
| Age | 1.010 | 0.546 | 0.982–1.034 |
| Gender | |||
| Female | 1.000 | - | - |
| Male | 0.673 | 0.339 | 0.299–1.514 |
| Location | |||
| Brainstem | 1.000 | - | - |
| Thalamus | 1.210 | 0.777 | 0.330–4.407 |
| Spinal Cord | 1.470 | 0.621 | 0.318–6.793 |
| Corpus Callosum | 1.630 | 0.561 | 0.315–8.391 |
| Basal Ganglia | 2.870 | 0.276 | 0.429–19.218 |
| Other | 1.270 | 0.839 | 0.123–13.141 |
| Group | |||
| Diffuse high-grade glioma | 1.000 | - | - |
| Diffuse midline glioma | 0.890 | 0.817 | 0.320–2.451 |
| Diffuse low-grade glioma | 0.310 | 0.103 | 0.075–1.265 |
| Circumscribed glioma | 0.013 | 0.000 | 0.001–0.142 |
| Intervention | |||
| Chemotherapy * | 1.430 | 0.436 | 0.582–3.509 |
| Radiotherapy * | 0.300 | 0.048 | 0.090–0.987 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Sharie, S.; Abu Laban, D.; Nazzal, J.; Iqneibi, S.; Ghnaimat, S.; Al-Ani, A.; Al-Hussaini, M. Midline Gliomas: A Retrospective Study from a Cancer Center in the Middle East. Cancers 2023, 15, 4545. https://doi.org/10.3390/cancers15184545
Al Sharie S, Abu Laban D, Nazzal J, Iqneibi S, Ghnaimat S, Al-Ani A, Al-Hussaini M. Midline Gliomas: A Retrospective Study from a Cancer Center in the Middle East. Cancers. 2023; 15(18):4545. https://doi.org/10.3390/cancers15184545
Chicago/Turabian StyleAl Sharie, Sarah, Dima Abu Laban, Jamil Nazzal, Shahad Iqneibi, Sura Ghnaimat, Abdallah Al-Ani, and Maysa Al-Hussaini. 2023. "Midline Gliomas: A Retrospective Study from a Cancer Center in the Middle East" Cancers 15, no. 18: 4545. https://doi.org/10.3390/cancers15184545
APA StyleAl Sharie, S., Abu Laban, D., Nazzal, J., Iqneibi, S., Ghnaimat, S., Al-Ani, A., & Al-Hussaini, M. (2023). Midline Gliomas: A Retrospective Study from a Cancer Center in the Middle East. Cancers, 15(18), 4545. https://doi.org/10.3390/cancers15184545