
Demographics, Clinical Characteristics and Survival Outcomes of Primary Urinary Tract Malignant Melanoma Patients: A Population-Based Analysis

 ,
,  , , ,
, , ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Variables and Outcome of Interest
2.3. Statistical Analyses
3. Results
3.1. Patient and Tumor Characteristics in Overall Primary Urinary Tract Malignant Melanoma Patients
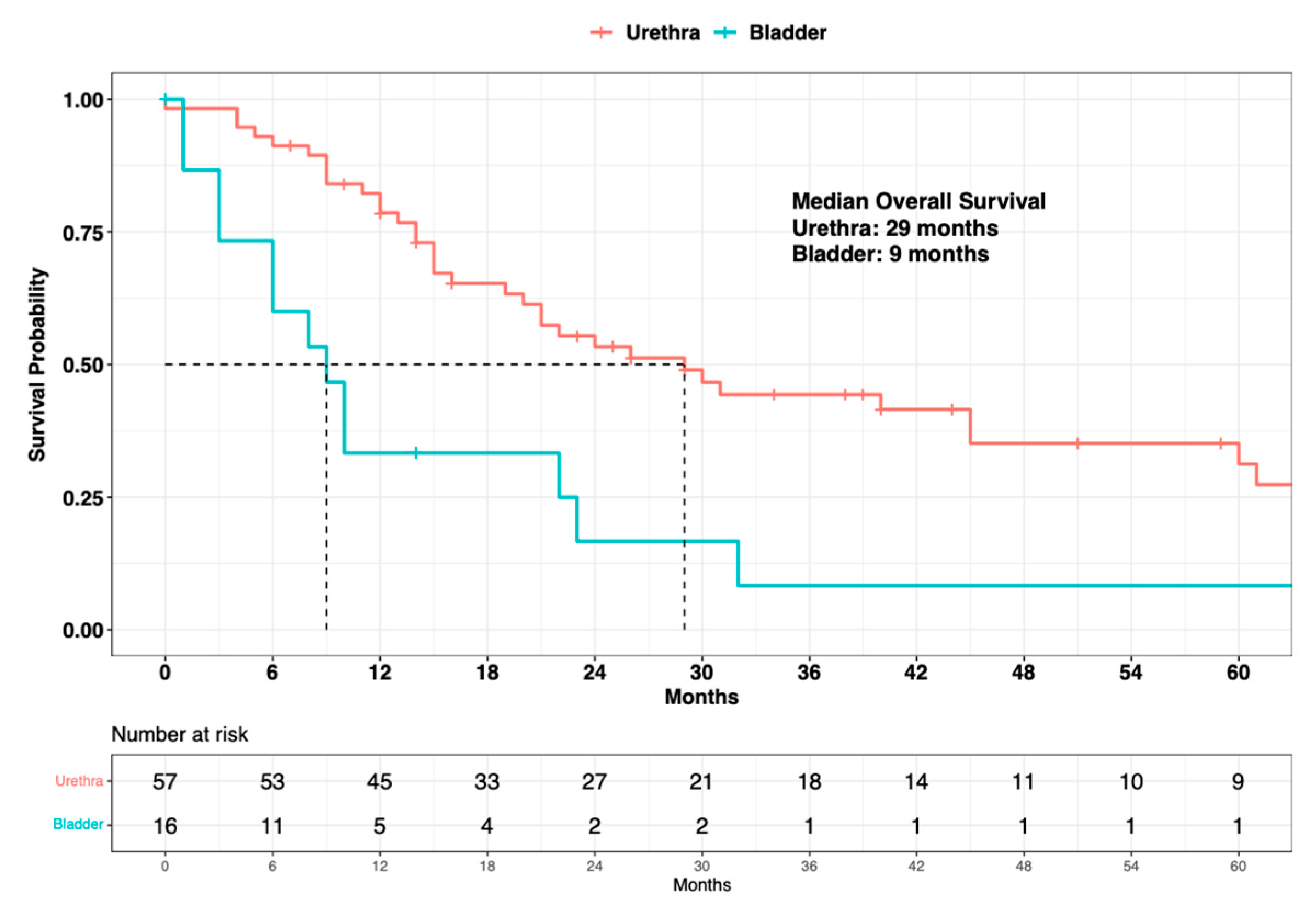
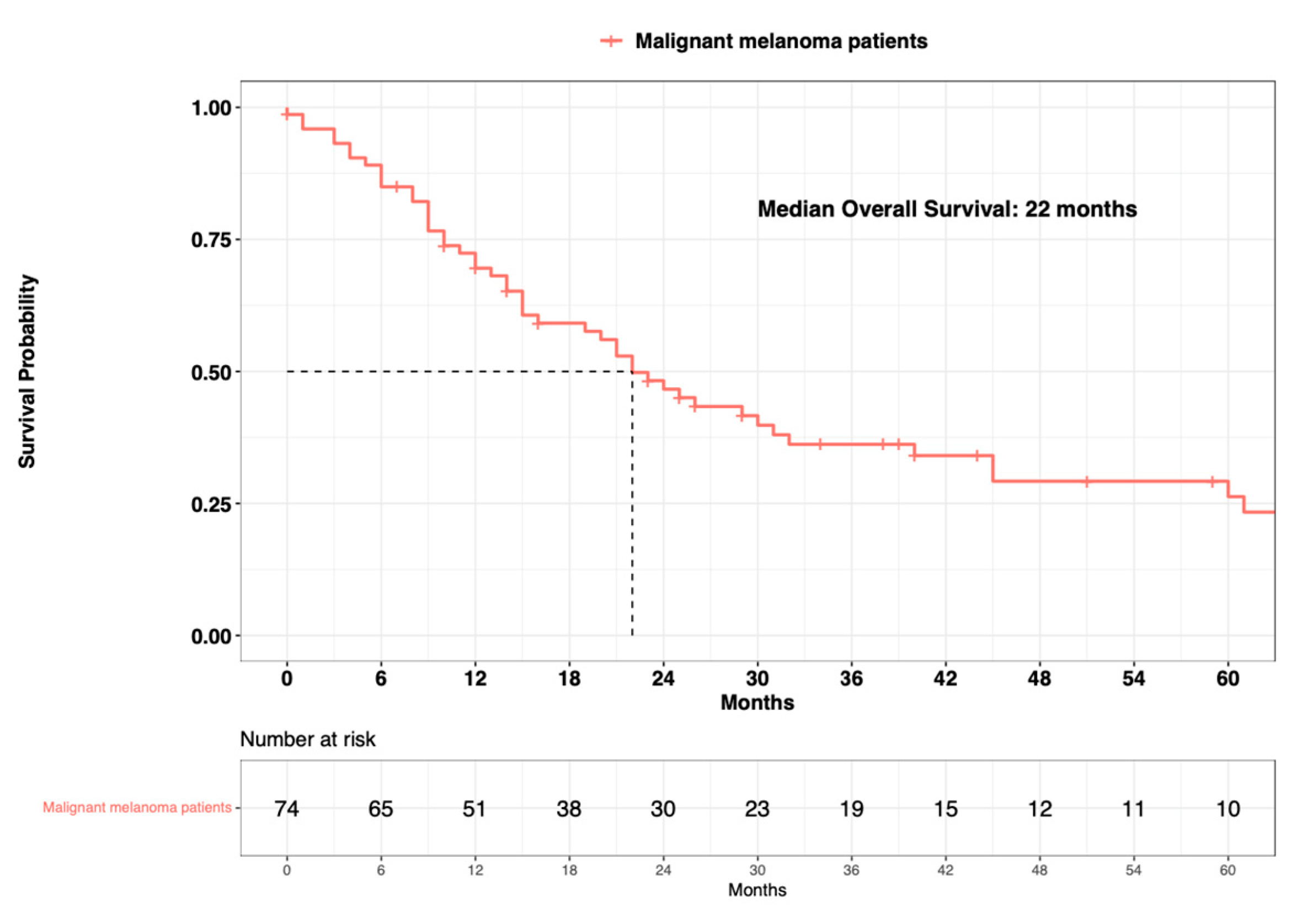
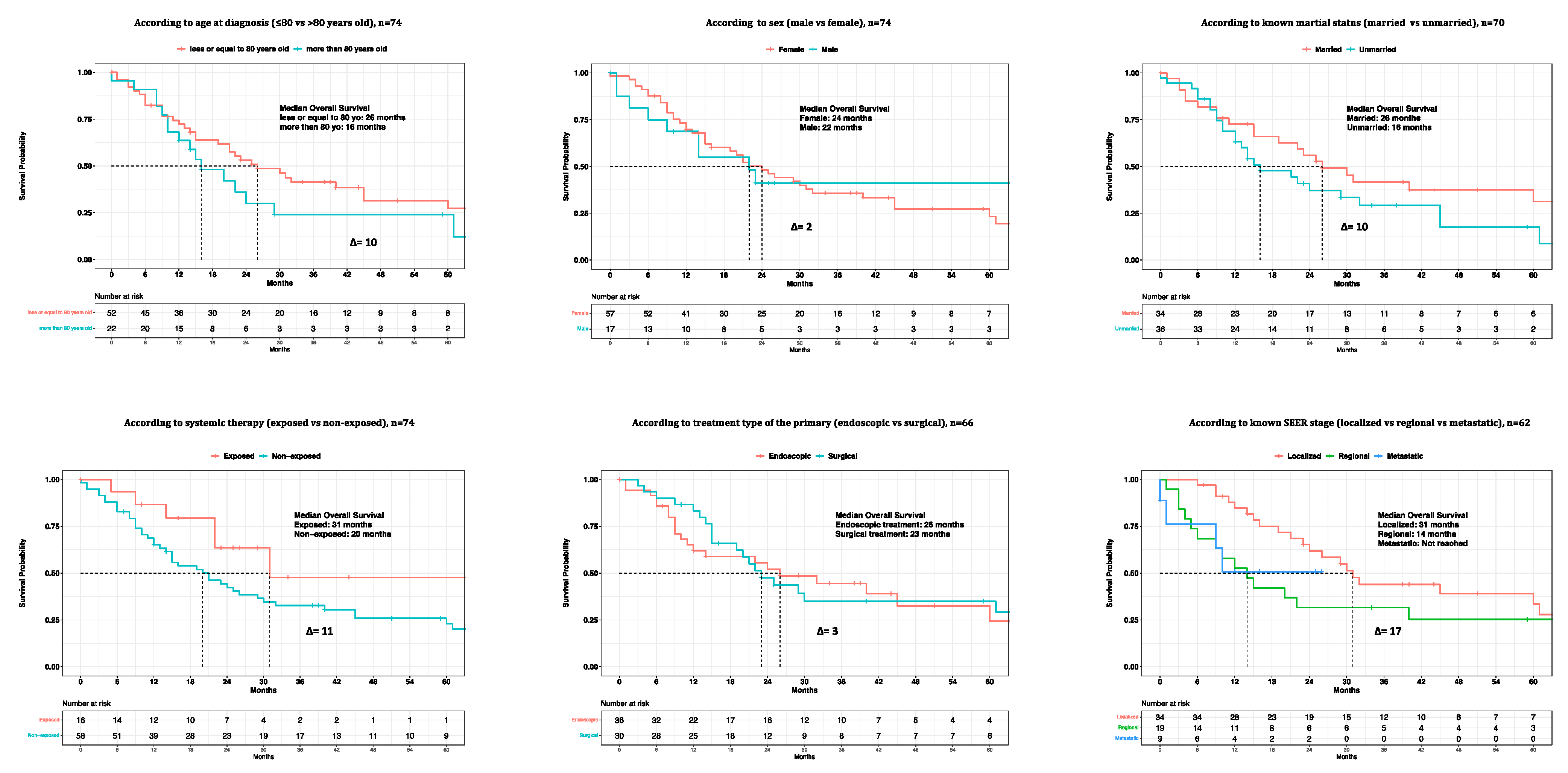
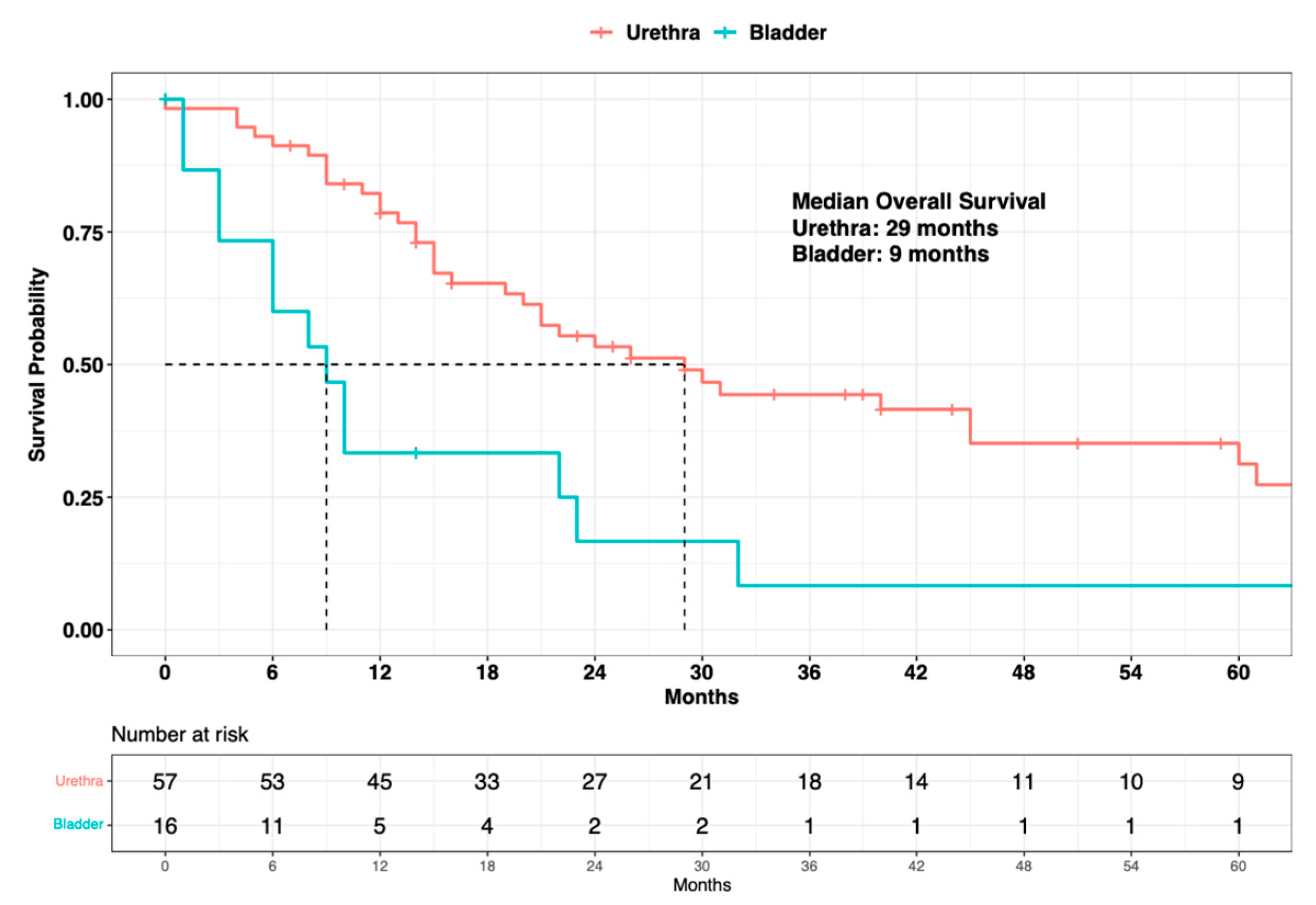
3.2. Survival Analyses in Primary Urinary Tract Malignant Melanoma Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olla, D.; Neumeister, M.W. Mucosal Melanoma. Clin. Plast. Surg. 2021, 48, 707–711. [Google Scholar] [CrossRef]
- Chang, A.E.; Karnell, L.H.; Menck, H.R. The National Cancer Data Base Report on Cutaneous and Noncutaneous Melanoma: A Summary of 84,836 Cases from the Past Decade. Cancer 1998, 83, 1664–1678. [Google Scholar] [CrossRef]
- Patrick, R.J.; Fenske, N.A.; Messina, J.L. Primary Mucosal Melanoma. J. Am. Acad. Dermatol. 2007, 56, 828–834. [Google Scholar] [CrossRef]
- Pooja, H.R.; Scott, J.F.; Vyas, R.; Gerstenblith, M.R. Genitourinary Melanoma. In Noncutaneous Melanoma; Gerstenblith, M.R., Ed.; Codon Publications: Singapore, 2018; pp. 61–81. ISBN 978-0-9944381-5-7. [Google Scholar]
- Tainio, H.M.; Kylmälä, T.M.; Haapasalo, H.K. Primary Malignant Melanoma of the Urinary Bladder Associated with Widespread Metastases. Scand. J. Urol. Nephrol. 1999, 33, 406–407. [Google Scholar] [CrossRef] [PubMed]
- Piura, B. Management of Primary Melanoma of the Female Urogenital Tract. Lancet Oncol. 2008, 9, 973–981. [Google Scholar] [CrossRef] [PubMed]
- DePalo, D.K.; Elleson, K.M.; Carr, M.J.; Spiess, P.E.; Zager, J.S. Genitourinary Melanoma: An Overview for the Clinician. Asian J. Urol. 2022, 9, 407–422. [Google Scholar] [CrossRef]
- Reed, C.A.L. Melano-Sarcoma of the Female Urethra-Urethrectomy—Recovery. Buffalo Med. J. 1896, 36, 344. [Google Scholar]
- Wheelock, M.C. Sarcoma of the Urinary Bladder. J. Urol. 1942, 48, 628–634. [Google Scholar] [CrossRef]
- Su, C.-T.; Prince, C.L. Melanoma of the Bladder. J. Urol. 1962, 87, 365–367. [Google Scholar] [CrossRef]
- Judd, R.L. Melanoma of the Ureter: A Case Report. J. Urol. 1962, 87, 805–807. [Google Scholar] [CrossRef]
- Bhutani, N.; Kajal, P.; Pawar, D. Primary Malignant Melanoma of the Female Urethra: Report of a Rare Neoplasm of the Urinary Tract. Int. J. Surg. Case Rep. 2017, 41, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Sayar, H.; Erdogan, S.; Adamhasan, F.; Gurbuz, E.; İnci, M.F. Malignant Melanoma of the Bladder: A Case Report. Can. Urol. Assoc. J. 2014, 8, 54. [Google Scholar] [CrossRef] [PubMed]
- Laudisio, A.; Giua, R.; Papalia, R.; Taffon, C.; Muto, G.; Antonelli Incalzi, R. An Unusual Cause of Hematuria: Primary Bladder Melanoma in an Older Man. J. Am. Geriatr. Soc. 2016, 64, e122–e123. [Google Scholar] [CrossRef]
- Davuluri, M.; Long, B.; Semple, S.; Villanueva-Siles, E.; Aboumohamed, A. Primary Urethral Melanoma: A Case Report and Literature Review. Urology 2019, 126, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Papeš, D.; Altarac, S.; Arslani, N.; Rajković, Z.; Antabak, A.; Ćaćić, M. Melanoma of the Glans Penis and Urethra. Urology 2014, 83, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Papeš, D.; Altarac, S. Melanoma of the Female Urethra. Med. Oncol. 2013, 30, 329. [Google Scholar] [CrossRef]
- Tacastacas, J.D.; Bray, J.; Cohen, Y.K.; Arbesman, J.; Kim, J.; Koon, H.B.; Honda, K.; Cooper, K.D.; Gerstenblith, M.R. Update on Primary Mucosal Melanoma. J. Am. Acad. Dermatol. 2014, 71, 366–375. [Google Scholar] [CrossRef]
- Pacella, M.; Gallo, F.; Gastaldi, C.; Ambruosi, C.; Carmignani, G. Primary Malignant Melanoma of the Bladder. Int. J. Urol. 2006, 13, 635–637. [Google Scholar] [CrossRef]
- Venyo, A.K.-G. Melanoma of the Urinary Bladder: A Review of the Literature. Surg. Res. Pract. 2014, 2014, 605802. [Google Scholar] [CrossRef]
- Sanchez, A.; Rodríguez, D.; Allard, C.B.; Bechis, S.K.; Sullivan, R.J.; Boeke, C.E.; Kuppermann, D.; Cheng, J.-S.; Barrisford, G.W.; Preston, M.A.; et al. Primary Genitourinary Melanoma: Epidemiology and Disease-Specific Survival in a Large Population-Based Cohort. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 166.e7–166.e14. [Google Scholar] [CrossRef]
- Acikalin, A.; Bagir, E.; Karim, S.; Bisgin, A.; Izol, V.; Erdogan, S. Primary Melanoma of the Urinary Tract; Clinicopathologic and Molecular Review of a Case Series. Pathol.-Res. Pract. 2020, 216, 153095. [Google Scholar] [CrossRef] [PubMed]
- Oliva, E.; Quinn, T.R.; Amin, M.B.; Eble, J.N.; Epstein, J.I.; Srigley, J.R.; Young, R.H. Primary Malignant Melanoma of the Urethra: A Clinicopathologic Analysis of 15 Cases. Am. J. Surg. Pathol. 2000, 24, 785–796. [Google Scholar] [CrossRef] [PubMed]
- Hale, N.E.; Prudnick, C.C.; Deem, S.G. Primary Melanoma of the Urinary Tract. J. Osteopath. Med. 2015, 115, 579. [Google Scholar] [CrossRef]
- Barillaro, F.; Camilli, M.; Dessanti, P.; Gorji, N.; Chiesa, F.; Villa, A.; Pastorino, A.; Aschele, C.; Conti, E. Primary Melanoma of the Bladder: Case Report and Review of the Literature. Arch. Ital. Urol. Androl. 2018, 90, 224–226. [Google Scholar] [CrossRef]
- Anichkov, N.M.; Nikonov, A.A. Primary Malignant Melanomas of the Bladder. J. Urol. 1982, 128, 813–815. [Google Scholar] [CrossRef]
- Goldschmidt, P.; Py, J.M.; Kostakopoulos, A.; Jacqmin, D.; Grosshans, E.; Bollack, C. Primary Malignant Melanomas of the Urinary Bladder. Br. J. Urol. 1988, 61, 359. [Google Scholar] [CrossRef]
- Rapisarda, S.; Bada, M.; Polara, A.; Crocetto, F.; Creta, M.; Chiancone, F.; Occhipinti, M.; Bertoloni, R.; Marciano, A.; Aresu, L.; et al. Conservative Management of Primary Malignant Melanoma of the Bladder: A Case Report. J. Med. Case Rep. 2021, 15, 39. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.E.; Monserrat, J.M.; Gonzalez Martin, G. Melanoma of the ureter. Rev. Argent. Urol. Nefrol. 1969, 38, 58–61. [Google Scholar]
- SEER Cancer Statistics Review, 1975–2018. Available online: https://seer.cancer.gov/csr/1975_2018/index.html (accessed on 14 January 2023).
- Netto, G.J.; Amin, M.B.; Berney, D.M.; Compérat, E.M.; Gill, A.J.; Hartmann, A.; Menon, S.; Raspollini, M.R.; Rubin, M.A.; Srigley, J.R.; et al. The 2022 World Health Organization Classification of Tumors of the Urinary System and Male Genital Organs—Part B: Prostate and Urinary Tract Tumors. Eur. Urol. 2022, 82, 469–482. [Google Scholar] [CrossRef]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 14 January 2023).
- Carbó-Bagué, A.; Rubió-Casadevall, J.; Puigdemont, M.; Sanvisens, A.; Oliveras, G.; Coll, M.; del Olmo, B.; Perez-Bueno, F.; Marcos-Gragera, R. Epidemiology and Molecular Profile of Mucosal Melanoma: A Population-Based Study in Southern Europe. Cancers 2022, 14, 780. [Google Scholar] [CrossRef]
- Bishop, K.D.; Olszewski, A.J. Epidemiology and Survival Outcomes of Ocular and Mucosal Melanomas: A Population-Based Analysis: Survival of Ocular and Mucosal Melanomas. Int. J. Cancer 2014, 134, 2961–2971. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Melanoma: Cutaneous NCCN Evidence Blocks™ Version 2.2023—10 March 2023. Available online: https://www.nccn.org/guidelines/category_1 (accessed on 10 March 2023).
- Rosiello, G.; Palumbo, C.; Knipper, S.; Pecoraro, A.; Dzyuba-Negrean, C.; Luzzago, S.; Tian, Z.; Gallina, A.; Montorsi, F.; Shariat, S.F.; et al. Unmarried Men Have Worse Oncologic Outcomes after Radical Cystectomy for Nonmetastatic Urothelial Bladder Cancer. Urol. Oncol. 2020, 38, 76.e1–76.e9. [Google Scholar] [CrossRef] [PubMed]
- Ruvolo, C.C.; Nocera, L.; Stolzenbach, F.L.; Wenzel, M.; Würnschimmel, C.; Fusco, F.; Palmieri, A.; Tian, Z.; Shariat, S.F.; Saad, F.; et al. Contemporary Analysis of the Effect of Marital Status on Survival in Upper Tract Urothelial Carcinoma Patients Treated with Radical Nephroureterectomy: A Population-Based Study. Urol. Oncol. 2021, 39, 789.e9–789.e17. [Google Scholar] [CrossRef]
- Shariat, S.F.; Godoy, G.; Lotan, Y.; Droller, M.; Karakiewicz, P.I.; Raman, J.D.; Isbarn, H.; Weizer, A.; Remzi, M.; Roscigno, M.; et al. Advanced Patient Age Is Associated with Inferior Cancer-Specific Survival after Radical Nephroureterectomy: Association of Age with Outcomes of Upper Tract Urothelial Carcinoma. BJU Int. 2009, 105, 1672–1677. [Google Scholar] [CrossRef]
- Sorce, G.; Chierigo, F.; Flammia, R.S.; Hoeh, B.; Hohenhorst, L.; Tian, Z.; Goyal, J.A.; Graefen, M.; Terrone, C.; Gallucci, M.; et al. Survival Trends in Chemotherapy Exposed Metastatic Bladder Cancer Patients and Chemotherapy Effect across Different Age, Sex, and Race/Ethnicity. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 380.e19–380.e27. [Google Scholar] [CrossRef] [PubMed]
- Alfaar, A.; Saad, A.; Chlad, P.; Elsherif, O.E.; Elshami, M.; Busch, C.; Rehak, M. Uveal Melanoma and Marital Status: A Relationship That Affects Survival. Int. Ophthalmol. 2022, 42, 3857–3867. [Google Scholar] [CrossRef]
- Cai, W.; Fan, J.; Shen, T.; Yu, J. The Influence of Marital Status on the Survival of Patients with Uveal Melanoma. J. Ophthalmol. 2020, 2020, 7012940. [Google Scholar] [CrossRef] [PubMed]
- Rachidi, S.; Deng, Z.; Sullivan, D.Y.; Lipson, E.J. Shorter Survival and Later Stage at Diagnosis among Unmarried Patients with Cutaneous Melanoma: A US National and Tertiary Care Center Study. J. Am. Acad. Dermatol. 2020, 83, 1012–1020. [Google Scholar] [CrossRef]
- Maas, J.A.; Monreal, A.J.; Diaz, E.L.; Castro, G.; Rodriguez de la Vega, P.; Varella, M. Marital Status and Survival in Patients Diagnosed with Melanoma. Dermatol. Res. Pract. 2020, 2020, 2485401. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall, N = 74 1 |
|---|---|
| Age | 75 (66, 82) |
| Sex | |
| Male | 17 (23%) |
| Female | 57 (77%) |
| Race/ethnicity | |
| Caucasian | 56 (76%) |
| Non-Caucasian | 18 (24%) |
| Marital status | |
| Married | 34 (46%) |
| Unmarried | 36 (49%) |
| Unknown | 4 (5%) |
| Tumor location | |
| Urethra | 57 (77%) |
| Bladder | 16 (22%) |
| Ureter | 1 (1%) |
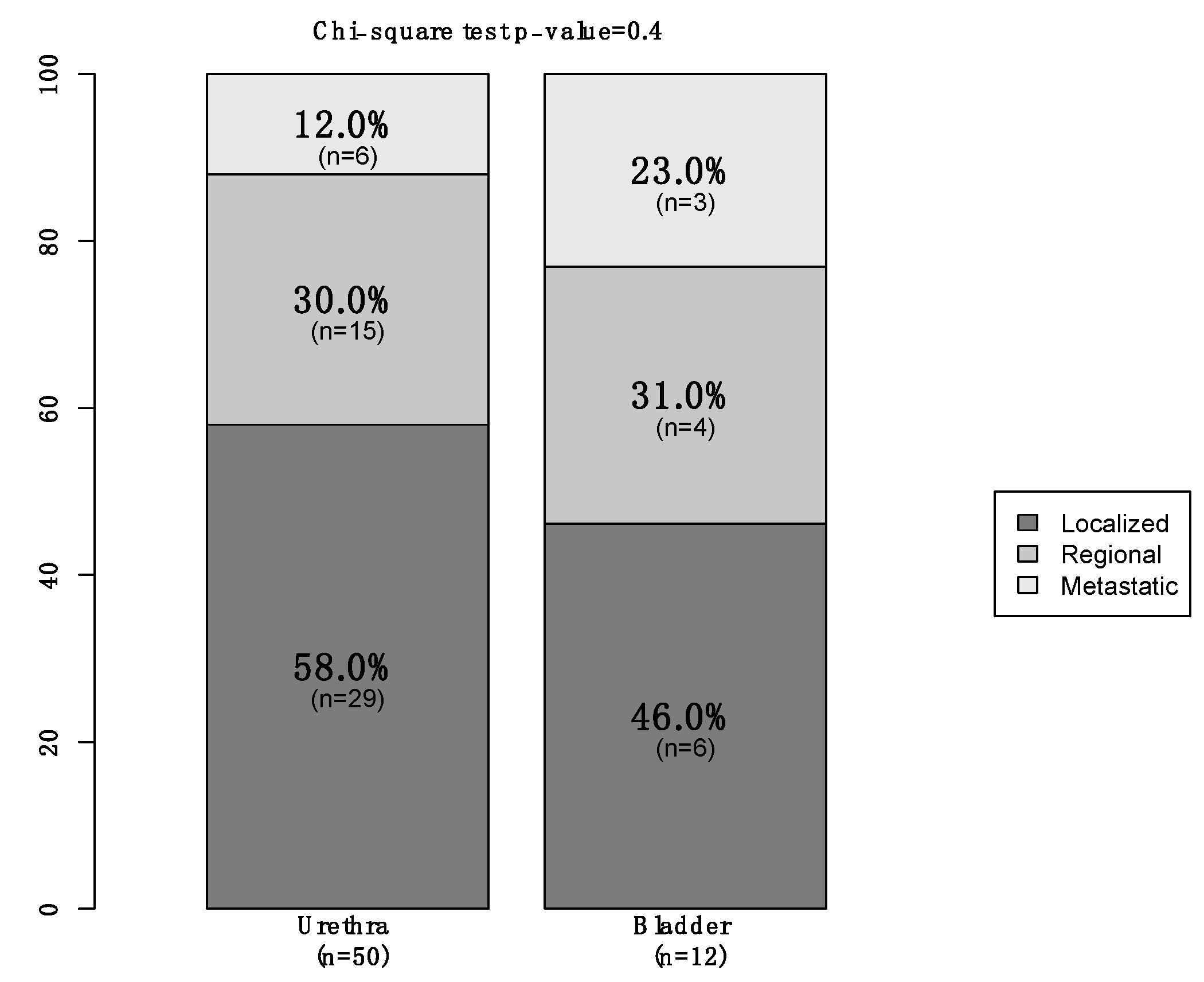
| SEER stage | |
| Localized | 35 (47%) |
| Locally advanced | 19 (26%) |
| Metastatic | 9 (12%) |
| Unknown | 11 (15%) |
| Systemic therapy | |
| Yes | 16 (22%) |
| No | 58 (78%) |
| Surgical treatment of the primary | |
| Performed | 66 (89%) |
| Not performed | 8 (11%) |
| Characteristic | HR 1 | 95% CI 1 | p-Value |
|---|---|---|---|
| Site of origin | |||
| Urethra | — | — | |
| Bladder | 2.90 | 1.55–5.42 | <0.001 |
| Age at diagnosis | |||
| ≤80 years | — | — | |
| >80 years | 1.61 | 0.89–2.91 | 0.1 |
| Sex | |||
| Female | — | — | |
| Male | 1.01 | 0.52–1.99 | 0.9 |
| Marital status | |||
| Married | — | — | |
| Unmarried | 1.41 | 0.79–2.49 | 0.2 |
| Systemic therapy | |||
| Exposed | — | — | |
| Not exposed | 2.27 | 0.96–5.35 | 0.06 |
| SEER stage | |||
| Localized | — | — | |
| Regional | 1.35 | 0.69–2.60 | 0.4 |
| Metastatic | 1.67 | 0.57–4.90 | 0.4 |
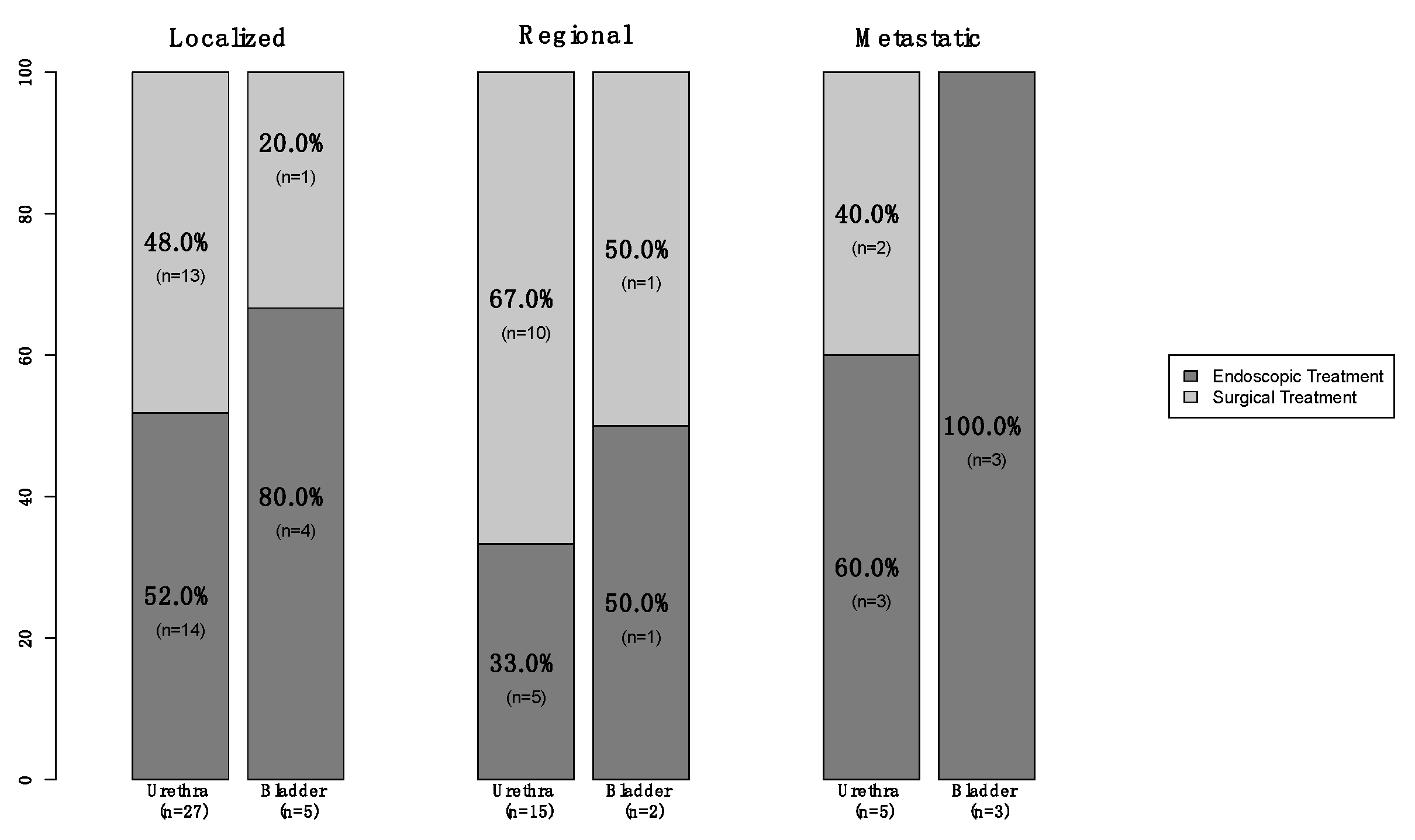
| Treatment of the primary | |||
| Endoscopic | — | — | |
| Surgical | 0.82 | 0.45–1.49 | 0.5 |
| Multivariable | |||
|---|---|---|---|
| HR 1 | 95% CI | p-Value | |
| Site of origin | |||
| Urethra | - | - | Ref |
| Bladder | 3.00 | 1.42–6.34 | 0.004 |
| SEER stage | |||
| Localized | - | - | Ref |
| Regional | 1.84 | 0.92–3.68 | 0.08 |
| Metastatic | 2.77 | 0.85–9.00 | 0.09 |
| Systemic therapy | |||
| Exposed | - | - | Ref |
| Non-exposed | 2.67 | 0.96–7.45 | 0.06 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morra, S.; Incesu, R.-B.; Scheipner, L.; Baudo, A.; Jannello, L.M.I.; de Angelis, M.; Siech, C.; Goyal, J.A.; Tian, Z.; Saad, F.; et al. Demographics, Clinical Characteristics and Survival Outcomes of Primary Urinary Tract Malignant Melanoma Patients: A Population-Based Analysis. Cancers 2023, 15, 4498. https://doi.org/10.3390/cancers15184498
Morra S, Incesu R-B, Scheipner L, Baudo A, Jannello LMI, de Angelis M, Siech C, Goyal JA, Tian Z, Saad F, et al. Demographics, Clinical Characteristics and Survival Outcomes of Primary Urinary Tract Malignant Melanoma Patients: A Population-Based Analysis. Cancers. 2023; 15(18):4498. https://doi.org/10.3390/cancers15184498
Chicago/Turabian StyleMorra, Simone, Reha-Baris Incesu, Lukas Scheipner, Andrea Baudo, Letizia Maria Ippolita Jannello, Mario de Angelis, Carolin Siech, Jordan A. Goyal, Zhe Tian, Fred Saad, and et al. 2023. "Demographics, Clinical Characteristics and Survival Outcomes of Primary Urinary Tract Malignant Melanoma Patients: A Population-Based Analysis" Cancers 15, no. 18: 4498. https://doi.org/10.3390/cancers15184498
APA StyleMorra, S., Incesu, R.-B., Scheipner, L., Baudo, A., Jannello, L. M. I., de Angelis, M., Siech, C., Goyal, J. A., Tian, Z., Saad, F., Califano, G., la Rocca, R., Capece, M., Shariat, S. F., Ahyai, S., Carmignani, L., de Cobelli, O., Musi, G., Tilki, D., ... Karakiewicz, P. I. (2023). Demographics, Clinical Characteristics and Survival Outcomes of Primary Urinary Tract Malignant Melanoma Patients: A Population-Based Analysis. Cancers, 15(18), 4498. https://doi.org/10.3390/cancers15184498