

Feasibility and Activity of Megestrol Acetate in Addition to Etoposide, Doxorubicin, Cisplatin, and Mitotane as First-Line Therapy in Patients with Metastatic/Unresectable Adrenocortical Carcinoma with Low Performance Status

 ,
,  , ,
, ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
2.3.1. Study Power
2.3.2. Collection and Statistical Analysis of Data
3. Results
3.1. Patient Characteristics
3.2. Treatment-Related Toxicities
3.3. Clinical Benefit Rate
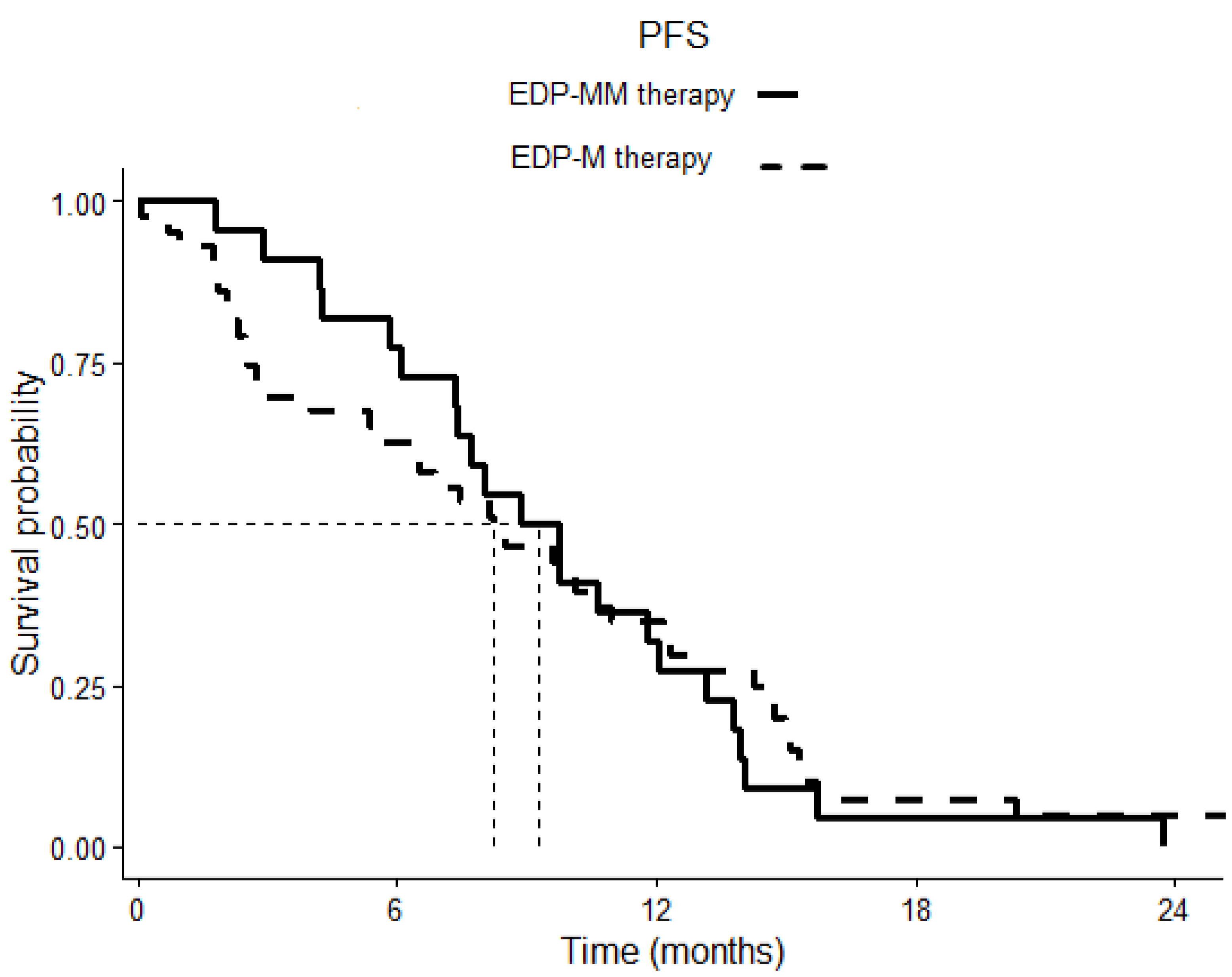
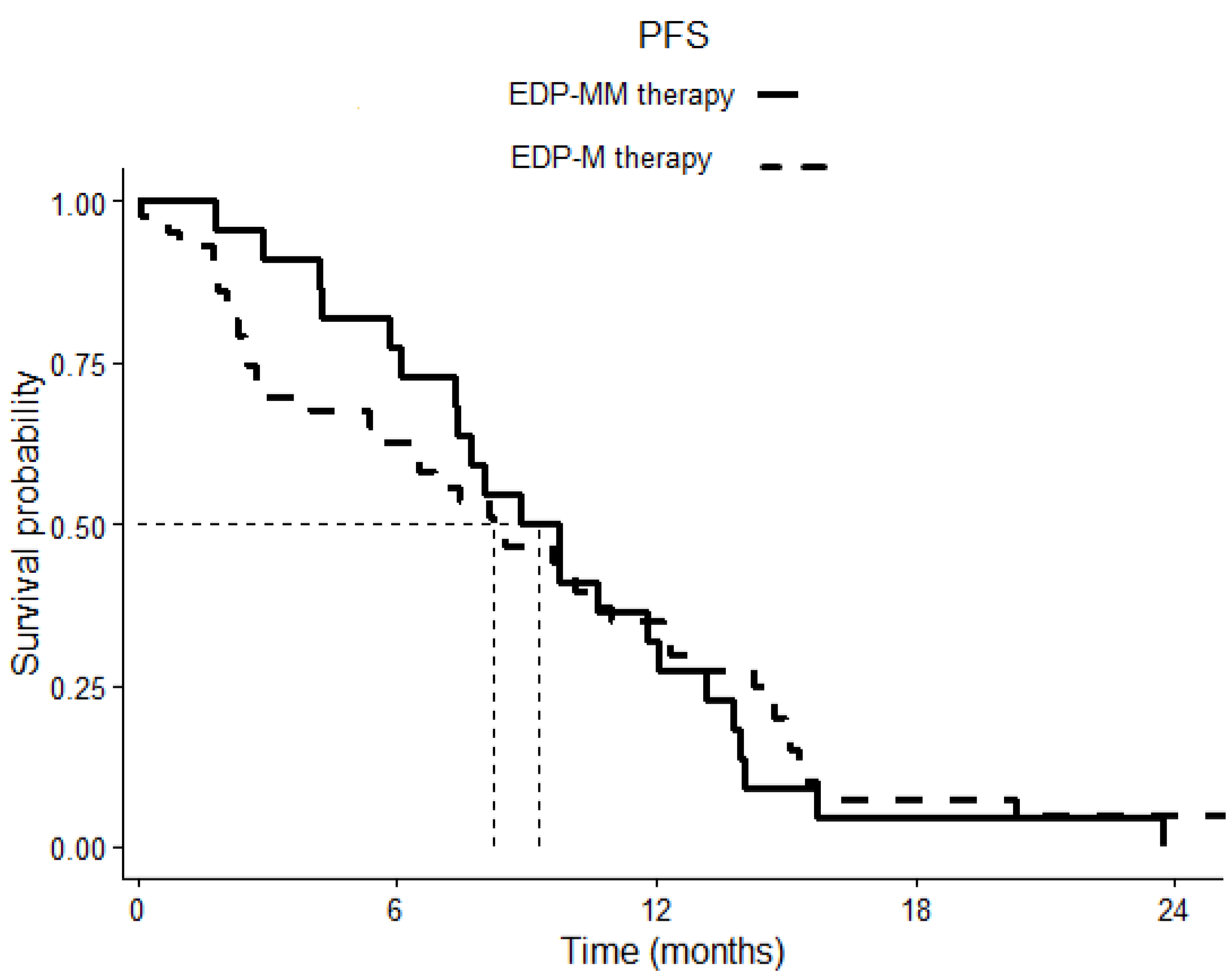
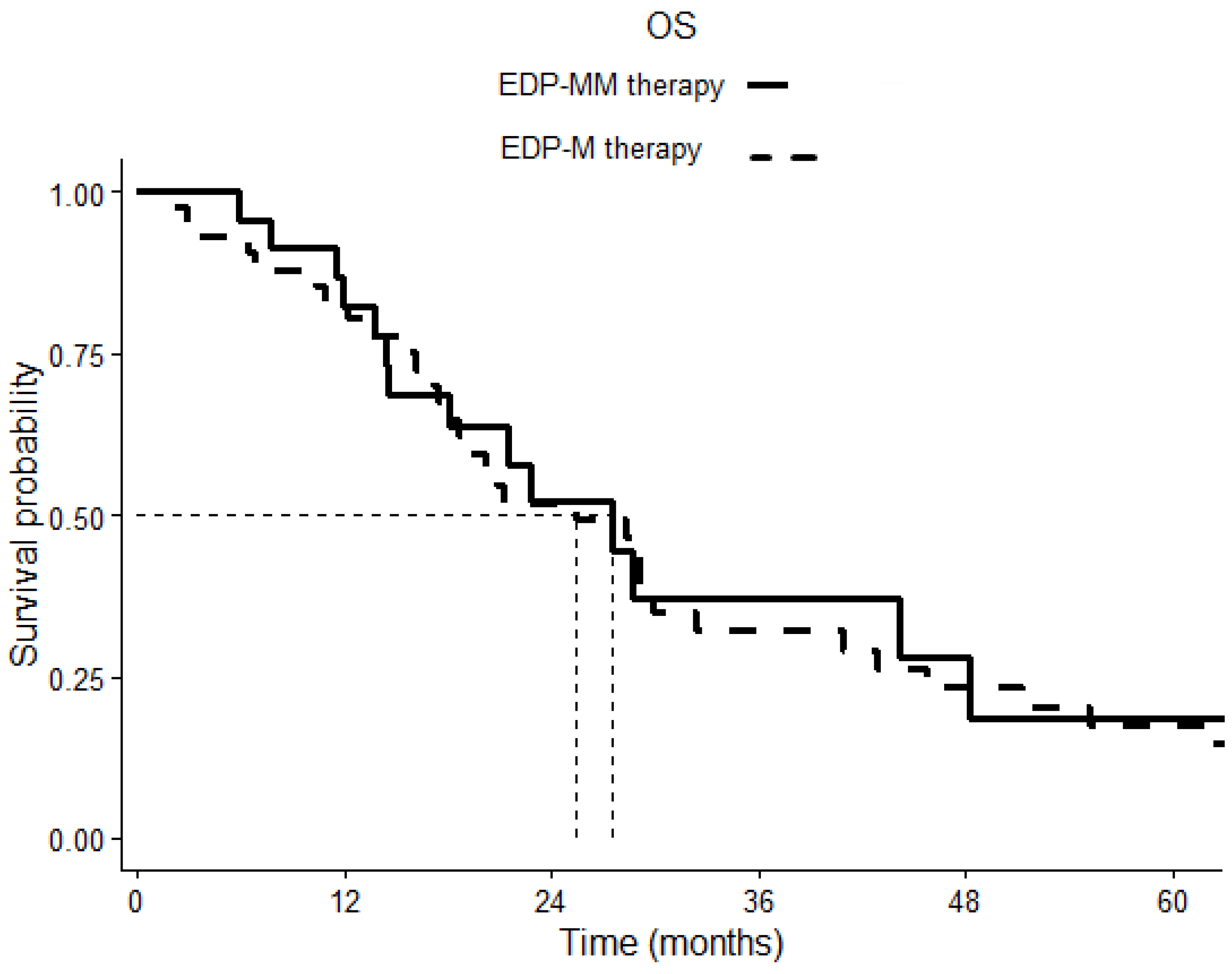
3.4. Efficacy of EDP-M and Megestrol Treatment in Terms of PFS and OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Volante, M.; Buttigliero, C.; Greco, E.; Berruti, A.; Papotti, M. Pathological and Molecular Features of Adrenocortical Carcinoma: An Update. J. Clin. Pathol. 2008, 61, 787–793. [Google Scholar] [CrossRef]
- Fassnacht, M.; Assie, G.; Baudin, E.; Eisenhofer, G.; de la Fouchardiere, C.; Haak, H.R.; de Krijger, R.; Porpiglia, F.; Terzolo, M.; Berruti, A. Adrenocortical Carcinomas and Malignant Phaeochromocytomas: ESMO–EURACAN Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2020, 31, 1476–1490. [Google Scholar] [CrossRef] [PubMed]
- Berruti, A.; Terzolo, M.; Sperone, P.; Pia, A.; Della Casa, S.; Gross, D.J.; Carnaghi, C.; Casali, P.; Porpiglia, F.; Mantero, F.; et al. Etoposide, Doxorubicin and Cisplatin plus Mitotane in the Treatment of Advanced Adrenocortical Carcinoma: A Large Prospective Phase II Trial. Endocr. Relat. Cancer 2005, 12, 657–666. [Google Scholar] [CrossRef]
- Fassnacht, M.; Terzolo, M.; Allolio, B.; Baudin, E.; Haak, H.; Berruti, A.; Welin, S.; Schade-Brittinger, C.; Lacroix, A.; Jarzab, B.; et al. Combination Chemotherapy in Advanced Adrenocortical Carcinoma. N. Engl. J. Med. 2012, 366, 2189–2197. [Google Scholar] [CrossRef] [PubMed]
- Elhassan, Y.S.; Altieri, B.; Berhane, S.; Cosentini, D.; Calabrese, A.; Haissaguerre, M.; Kastelan, D.; Fragoso, M.C.B.V.; Bertherat, J.; Al Ghuzlan, A.; et al. S-GRAS Score for Prognostic Classification of Adrenocortical Carcinoma: An International, Multicenter ENSAT Study. Eur. J. Endocrinol. 2022, 186, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Wortmann, S.; Quinkler, M.; Ritter, C.; Kroiss, M.; Johanssen, S.; Hahner, S.; Allolio, B.; Fassnacht, M. Bevacizumab plus Capecitabine as a Salvage Therapy in Advanced Adrenocortical Carcinoma. Eur. J. Endocrinol. 2010, 162, 349–356. [Google Scholar] [CrossRef]
- Quinkler, M.; Hahner, S.; Wortmann, S.; Johanssen, S.; Adam, P.; Ritte, C.; Strasburger, C.; Allolio, B.; Fassnacht, M. Treatment of Advanced Adrenocortical Carcinoma with Erlotinib plus Gemcitabine. J. Clin. Endocrinol. Metab. 2008, 93, 2057–2062. [Google Scholar] [CrossRef]
- Samnotra, V.; Vassilopoulou-Sellin, R.; Fojo, A.T.; Oh, W.K.; LaRocca, R.V.; Ernstoff, M.S.; Memoli, V.A.; Cole, B.F.; Quinn, D.I.; Simmons, P.A.; et al. A Phase II Trial of Gefitinib Monotherapy in Patients with Unresectable Adrenocortical Carcinoma (ACC). J. Clin. Oncol. 2007, 25, 15527. [Google Scholar] [CrossRef]
- O’Sullivan, C.; Edgerly, M.; Velarde, M.; Wilkerson, J.; Venkatesan, A.M.; Pittaluga, S.; Yang, S.X.; Nguyen, D.; Balasubramaniam, S.; Fojo, T. The VEGF Inhibitor Axitinib Has Limited Effectiveness as a Therapy for Adrenocortical Cancer. J. Clin. Endocrinol. Metab. 2014, 99, 1291–1297. [Google Scholar] [CrossRef]
- Kroiss, M.; Deutschbein, T.; Schlötelburg, W.; Ronchi, C.L.; Hescot, S.; Körbl, D.; Megerle, F.; Beuschlein, F.; Neu, B.; Quinkler, M.; et al. Treatment of Refractory Adrenocortical Carcinoma with Thalidomide: Analysis of 27 Patients from the European Network for the Study of Adrenal Tumours Registry. Exp. Clin. Endocrinol. Diabetes 2019, 127, 578–584. [Google Scholar] [CrossRef]
- Galsky, M.D.; Dritselis, A.; Kirkpatrick, P.; Oh, W.K. Cabazitaxel. Nat. Rev. Drug Discov. 2010, 9, 677–678. [Google Scholar] [CrossRef] [PubMed]
- Naing, A.; Meric-Bernstam, F.; Stephen, B.; Karp, D.D.; Hajjar, J.; Rodon Ahnert, J.; Piha-Paul, S.A.; Colen, R.R.; Jimenez, C.; Raghav, K.P.; et al. Phase 2 Study of Pembrolizumab in Patients with Advanced Rare Cancers. J. Immunother. Cancer 2020, 8, e000347. [Google Scholar] [CrossRef] [PubMed]
- Raj, N.; Zheng, Y.; Kelly, V.; Katz, S.S.; Chou, J.; Do, R.K.G.; Capanu, M.; Zamarin, D.; Saltz, L.B.; Ariyan, C.E.; et al. PD-1 Blockade in Advanced Adrenocortical Carcinoma. J. Clin. Oncol. 2020, 38, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Klein, O.; Senko, C.; Carlino, M.S.; Markman, B.; Jackett, L.; Gao, B.; Lum, C.; Kee, D.; Behren, A.; Palmer, J.; et al. Combination Immunotherapy with Ipilimumab and Nivolumab in Patients with Advanced Adrenocortical Carcinoma: A Subgroup Analysis of CA209-538. Oncoimmunology 2021, 10, 1908771. [Google Scholar] [CrossRef]
- Carneiro, B.A.; Konda, B.; Costa, R.B.; Costa, R.L.B.; Sagar, V.; Gursel, D.B.; Kirschner, L.S.; Chae, Y.K.; Abdulkadir, S.A.; Rademaker, A.; et al. Nivolumab in Metastatic Adrenocortical Carcinoma: Results of a Phase 2 Trial. J. Clin. Endocrinol. Metab. 2019, 104, 6193–6200. [Google Scholar] [CrossRef]
- Habra, M.A.; Stephen, B.; Campbell, M.; Hess, K.; Tapia, C.; Xu, M.; Rodon Ahnert, J.; Jimenez, C.; Lee, J.E.; Perrier, N.D.; et al. Phase II Clinical Trial of Pembrolizumab Efficacy and Safety in Advanced Adrenocortical Carcinoma. J. Immunother. Cancer 2019, 7, 253. [Google Scholar] [CrossRef]
- Araujo-Castro, M.; Pascual-Corrales, E.; Molina-Cerrillo, J.; Alonso-Gordoa, T. Immunotherapy in Adrenocortical Carcinoma: Predictors of Response, Efficacy, Safety, and Mechanisms of Resistance. Biomedicines 2021, 9, 304. [Google Scholar] [CrossRef]
- Fedotcheva, T.A. Clinical Use of Progestins and Their Mechanisms of Action: Present and Future (Review). Sovrem. Tehnol. V Med. 2021, 13, 93. [Google Scholar] [CrossRef]
- Fiorentini, C.; Fragni, M.; Perego, P.; Vezzoli, S.; Bonini, S.A.; Tortoreto, M.; Galli, D.; Claps, M.; Tiberio, G.A.; Terzolo, M.; et al. Antisecretive and Antitumor Activity of Abiraterone Acetate in Human Adrenocortical Cancer: A Preclinical Study. J. Clin. Endocrinol. Metab. 2016, 101, 4594–4602. [Google Scholar] [CrossRef]
- Fragni, M.; Fiorentini, C.; Rossini, E.; Fisogni, S.; Vezzoli, S.; Bonini, S.A.; Dalmiglio, C.; Grisanti, S.; Tiberio, G.A.M.; Claps, M.; et al. In Vitro Antitumor Activity of Progesterone in Human Adrenocortical Carcinoma. Endocrine 2019, 63, 592–601. [Google Scholar] [CrossRef]
- Garg, D.; Ng, S.S.M.; Baig, K.M.; Driggers, P.; Segars, J. Progesterone-Mediated Non-Classical Signaling. Trends Endocrinol. Metab. 2017, 28, 656–668. [Google Scholar] [CrossRef] [PubMed]
- Abate, A.; Rossini, E.; Tamburello, M.; Laganà, M.; Cosentini, D.; Grisanti, S.; Fiorentini, C.; Tiberio, G.A.M.; Scatolini, M.; Grosso, E.; et al. Ribociclib Cytotoxicity Alone or Combined With Progesterone and/or Mitotane in in Vitro Adrenocortical Carcinoma Cells. Endocrinology 2022, 163, bqab248. [Google Scholar] [CrossRef] [PubMed]
- Rossini, E.; Tamburello, M.; Abate, A.; Beretta, S.; Fragni, M.; Cominelli, M.; Cosentini, D.; Hantel, C.; Bono, F.; Grisanti, S.; et al. Cytotoxic Effect of Progesterone, Tamoxifen and Their Combination in Experimental Cell Models of Human Adrenocortical Cancer. Front. Endocrinol. 2021, 12, 669426. [Google Scholar] [CrossRef]
- Tamburello, M.; Abate, A.; Rossini, E.; Basnet, R.M.; Zizioli, D.; Cosentini, D.; Hantel, C.; Laganà, M.; Tiberio, G.A.M.; Grisanti, S.; et al. Preclinical Evidence of Progesterone as a New Pharmacological Strategy in Human Adrenocortical Carcinoma Cell Lines. Int. J. Mol. Sci. 2023, 24, 6829. [Google Scholar] [CrossRef] [PubMed]
- Oaknin, A.; Bosse, T.J.; Creutzberg, C.L.; Giornelli, G.; Harter, P.; Joly, F.; Lorusso, D.; Marth, C.; Makker, V.; Mirza, M.R.; et al. Endometrial Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2022, 33, 860–877. [Google Scholar] [CrossRef] [PubMed]
- Gennari, A.; André, F.; Barrios, C.H.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the Diagnosis, Staging and Treatment of Patients with Metastatic Breast Cancer. Ann. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef]
- Arends, J.; Strasser, F.; Gonella, S.; Solheim, T.S.; Madeddu, C.; Ravasco, P.; Buonaccorso, L.; de van der Schueren, M.A.E.; Baldwin, C.; Chasen, M.; et al. Cancer Cachexia in Adult Patients: ESMO Clinical Practice Guidelines☆. ESMO Open 2021, 6, 100092. [Google Scholar] [CrossRef]
- Mantovani, G.; Macciò, A.; Esu, S.; Lai, P.; Santona, M.C.; Massa, E.; Dessi, D.; Melis, G.B.; Del Giacco, G.S. Medroxyprogesterone Acetate Reduces the in Vitro Production of Cytokines and Serotonin Involved in Anorexia/Cachexia and Emesis by Peripheral Blood Mononuclear Cells of Cancer Patients. Eur. J. Cancer 1997, 33, 602–607. [Google Scholar] [CrossRef]
- Ruiz Garcia, V.; López-Briz, E.; Carbonell Sanchis, R.; Gonzalvez Perales, J.L.; Bort-Martí, S. Megestrol Acetate for Treatment of Anorexia-Cachexia Syndrome. Cochrane Database Syst. Rev. 2013, 3, CD004310. [Google Scholar] [CrossRef]
- Turla, A.; Laganà, M.; Grisanti, S.; Abate, A.; Ferrari, V.D.; Cremaschi, V.; Sigala, S.; Consoli, F.; Cosentini, D.; Berruti, A. Supportive Therapies in Patients with Advanced Adrenocortical Carcinoma Submitted to Standard EDP-M Regimen. Endocrine 2022, 77, 438–443. [Google Scholar] [CrossRef]
- Luthy, I.A.; Begin, D.J.; Labrie, F. Androgenic Activity of Synthetic Progestins and Spironolactone in Androgen-Sensitive Mouse Mammary Carcinoma (Shionogi) Cells in Culture. J. Steroid. Biochem. 1988, 31, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Teulings, F.A.; van Gilse, H.A.; Henkelman, M.S.; Portengen, H.; Alexieva-Figusch, J. Estrogen, Androgen, Glucocorticoid, and Progesterone Receptors in Progestin-Induced Regression of Human Breast Cancer. Cancer Res. 1980, 40, 2557–2561. [Google Scholar] [PubMed]
- Sung, J.-H.; An, H.-S.; Jeong, J.-H.; Shin, S.; Song, S.Y. Megestrol Acetate Increases the Proliferation, Migration, and Adipogenic Differentiation of Adipose-Derived Stem Cells via Glucocorticoid Receptor. Stem Cells Transl. Med. 2015, 4, 789–799. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Patient Characteristics | EDP-MM1 Patients | EDP-M2 Patients | p |
|---|---|---|---|
| Total patients | 24 | 48 | - |
| Gender | 0.028 | ||
| Male | 3 (12.5%) | 18 (37.5%) | |
| Female | 21 (87.5%) | 30 (62.5%) | |
| Missing | 0 | 0 | |
| Age at diagnosis | 0.892 | ||
| Median | 46.48 | 46 | |
| Range | 19–67 | 16–72 | |
| Missing | 0 | 0 | |
| Clinical presentation | 0.601 | ||
| Mass symptoms | 13 (54.2%) | 25 (52.1%) | |
| Hormonal symptoms | 6 (25%) | 14 (29.2%) | |
| Mass/hormonal symptoms | 4 (16.6%) | 4 (8.3%) | |
| Incidentaloma | 1 (4.2%) | 5 (10.4%) | |
| Missing | 0 | 0 | |
| Secreting tumor * | 0.012 | ||
| Yes | 18 (94.7%) | 27 (62.8%) | |
| No | 1 (5.3%) | 16 (37.2%) | |
| Missing | 5 | 2 | |
| ENSAT stage at diagnosis * | 0.267 | ||
| 1–2 | 5 (20.8%) | 13 (27.7%) | |
| 3 | 5 (20.8%) | 16 (34.0%) | |
| 4 | 14 (58.4%) | 18 (38.3%) | |
| Missing | 0 | 1 | |
| GRAS at diagnosis * | 0.408 | ||
| Favorable | 0 | 2 (4.4%) | |
| Unfavorable | 4 (22.2%) | 15 (33.3%) | |
| Pejorative | 14 (77.8%) | 28 (62.3%) | |
| Missing | 6 | 3 | |
| Surgery | 0.850 | ||
| Yes | 18 (75%) | 35 (72.9%) | |
| No | 6 (25%) | 13 (27.1%) | |
| Missing | 0 | 0 | |
| Radical surgery | 0.096 | ||
| R0 | 10 (55.5%) | 26 (74.3%) | |
| R1-R2 | 8 (44.4%) | 9 (25.7%) | |
| Missing | 0 | 0 | |
| Mitotane in an adjuvant setting | 0.085 | ||
| Yes | 4 (22.2%) | 15 (42.9%) | |
| No | 14 (77.8%) | 20 (57.1%) | |
| Missing | 0 | 0 |
| Toxicity Related to EDP-M2 Treatment | EDP-MM1 Patients | EDP-M2 Patients | p ** | ||||
|---|---|---|---|---|---|---|---|
| Treatment-related toxicities * | |||||||
| Yes | 23 (95.8%) | 38 (97.4%) | |||||
| No | 1 (4.2%) | 1 (2.6%) | 0.725 | ||||
| Unavailable | 0 | 9 | |||||
| Any grade | G1–2 | G3–4 | Any grade | G1–2 | G3–4 | ||
| Nausea | 17 (70.9%) | 16 (66.7%) | 1 (4.2%) | 14 (35.9%) | 12 (30.8%) | 2 (5.1%) | 0.010 |
| Vomiting | 8 (33.3%) | 8 (33.3%) | 0 | 18 (46.2%) | 16 (41.1%) | 2 (5.1%) | 0.315 |
| Diarrhea | 0 | 0 | 0 | 1 (2.6%) | 1 (2.6%) | 0 | 0.421 |
| Asthenia | 20 (83.3%) | 17 (70.8%) | 3 (12.5%) | 23 (59%) | 20 (51.3%) | 3 (7.7%) | 0.044 |
| Constipation | 4 (16.7%) | 4 (16.7%) | 0 | 3 (7.7%) | 2 (5.1%) | 1 (2.6%) | 0.271 |
| Hematological | 12 (50%) | 10 (41.7%) | 2 (8.3%) | 13 (33.3%) | 11 (28.2%) | 2 (5.1%) | 0.189 |
| Neutropenia | 4 (16.6%) | 2 (8.3%) | 2 (8.3%) | 3 (7.7%) | 2 (5.1%) | 1 (2.6%) | 0.271 |
| Thrombocytopenia | 5 (20.8%) | 3 (12.5%) | 2 (8.3%) | 2 (5.1%) | 1 (2.5%) | 1 (2.5%) | 0.095 |
| Anemia | 12 (50%) | 10 (41.7%) | 2 (8.3%) | 11 (28.2%) | 9 (20.5%) | 3 (7.7%) | 0.108 |
| Other toxicities | 0 | 0 | 0 | 14 (35.9%) | 14 (35.9%) | 0 | 0.001 |
| Response to Systemic Treatment | EDP-MM1 Patients | EDP-M2 Patients | p |
|---|---|---|---|
| CR + PR + SD * CR PR SD | 18 (75%) 0 12 (50%) 6 (25%) | 29 (60.4%) 1 (2.1%) 19 (39.6%) 9 (18.7%) | 0.224 |
| PD ** | 6 (25%) | 19 (39.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turla, A.; Laganà, M.; Abate, A.; Cremaschi, V.; Zamparini, M.; Chittò, M.; Consoli, F.; Alberti, A.; Ambrosini, R.; Tamburello, M.; et al. Feasibility and Activity of Megestrol Acetate in Addition to Etoposide, Doxorubicin, Cisplatin, and Mitotane as First-Line Therapy in Patients with Metastatic/Unresectable Adrenocortical Carcinoma with Low Performance Status. Cancers 2023, 15, 4491. https://doi.org/10.3390/cancers15184491
Turla A, Laganà M, Abate A, Cremaschi V, Zamparini M, Chittò M, Consoli F, Alberti A, Ambrosini R, Tamburello M, et al. Feasibility and Activity of Megestrol Acetate in Addition to Etoposide, Doxorubicin, Cisplatin, and Mitotane as First-Line Therapy in Patients with Metastatic/Unresectable Adrenocortical Carcinoma with Low Performance Status. Cancers. 2023; 15(18):4491. https://doi.org/10.3390/cancers15184491
Chicago/Turabian StyleTurla, Antonella, Marta Laganà, Andrea Abate, Valentina Cremaschi, Manuel Zamparini, Matteo Chittò, Francesca Consoli, Andrea Alberti, Roberta Ambrosini, Mariangela Tamburello, and et al. 2023. "Feasibility and Activity of Megestrol Acetate in Addition to Etoposide, Doxorubicin, Cisplatin, and Mitotane as First-Line Therapy in Patients with Metastatic/Unresectable Adrenocortical Carcinoma with Low Performance Status" Cancers 15, no. 18: 4491. https://doi.org/10.3390/cancers15184491
APA StyleTurla, A., Laganà, M., Abate, A., Cremaschi, V., Zamparini, M., Chittò, M., Consoli, F., Alberti, A., Ambrosini, R., Tamburello, M., Grisanti, S., Tiberio, G. A. M., Sigala, S., Cosentini, D., & Berruti, A. (2023). Feasibility and Activity of Megestrol Acetate in Addition to Etoposide, Doxorubicin, Cisplatin, and Mitotane as First-Line Therapy in Patients with Metastatic/Unresectable Adrenocortical Carcinoma with Low Performance Status. Cancers, 15(18), 4491. https://doi.org/10.3390/cancers15184491