
Orbital Exenteration for Craniofacial Lesions: A Systematic Review and Meta-Analysis of Patient Characteristics and Survival Outcomes
 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Data Synthesis and Quality Assessment
2.5. Statistical Analysis
3. Results
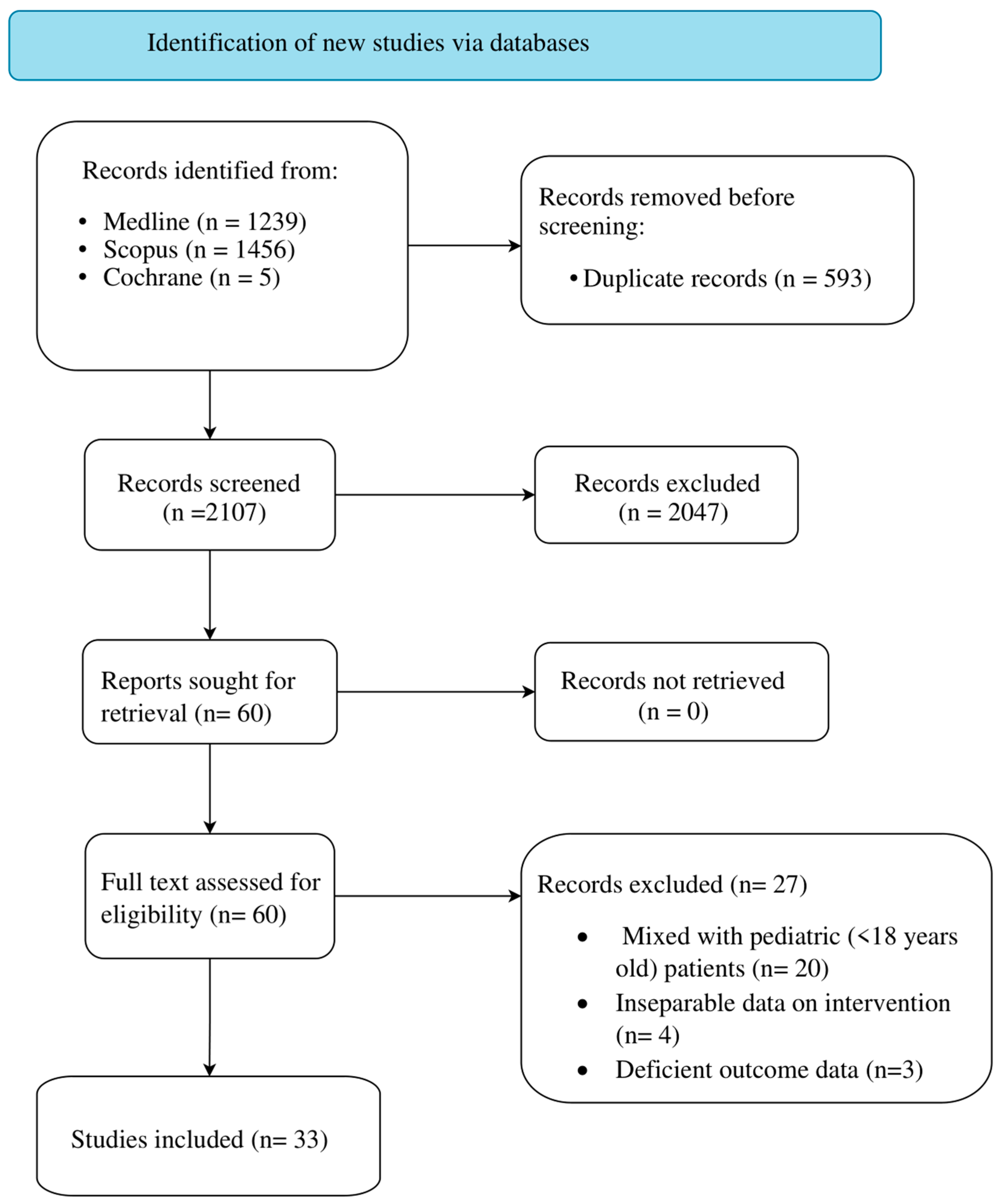
3.1. Study Selection
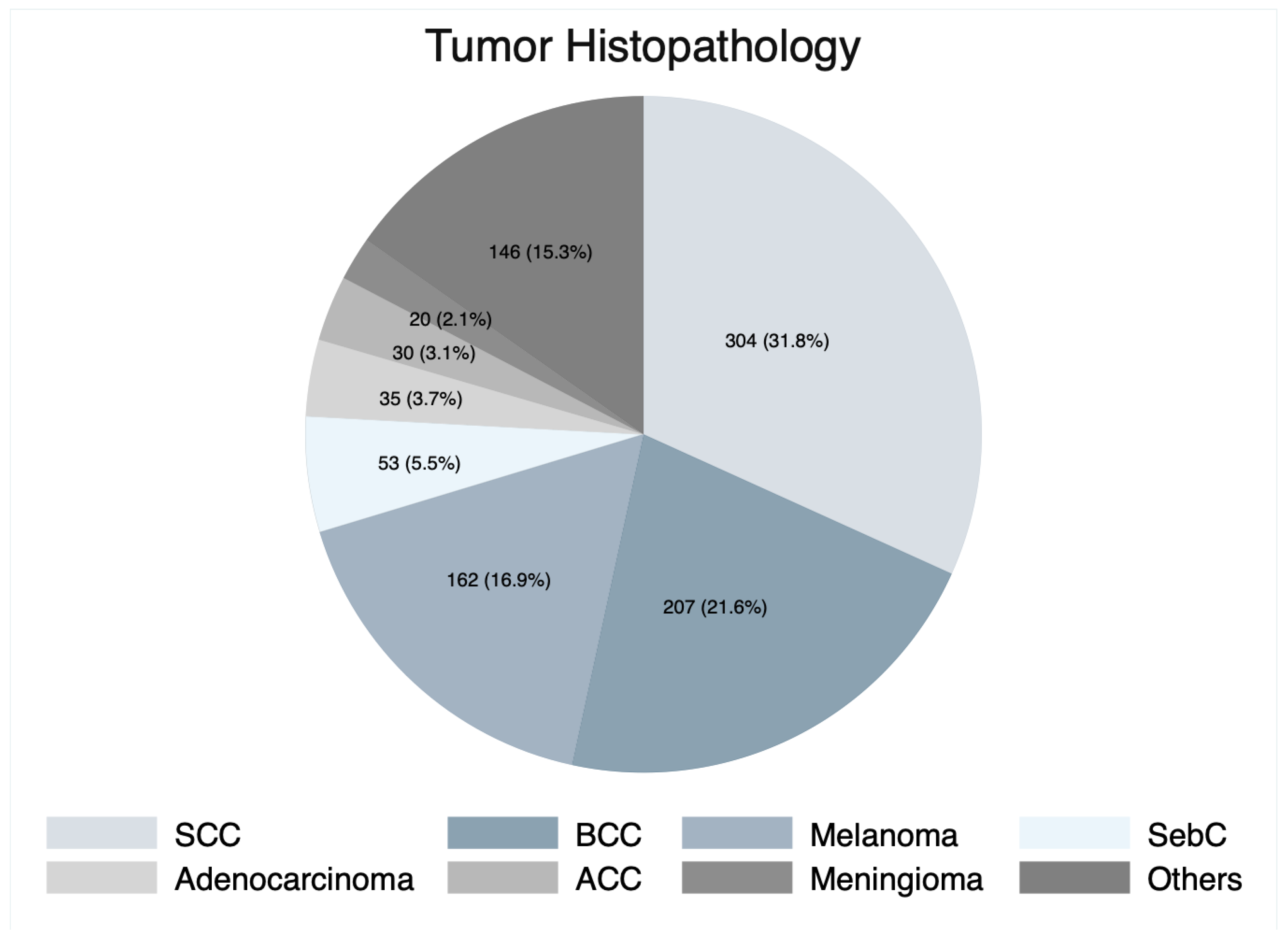
3.2. Demographics and Clinical Characteristics of the Cohort
3.3. Patient Management
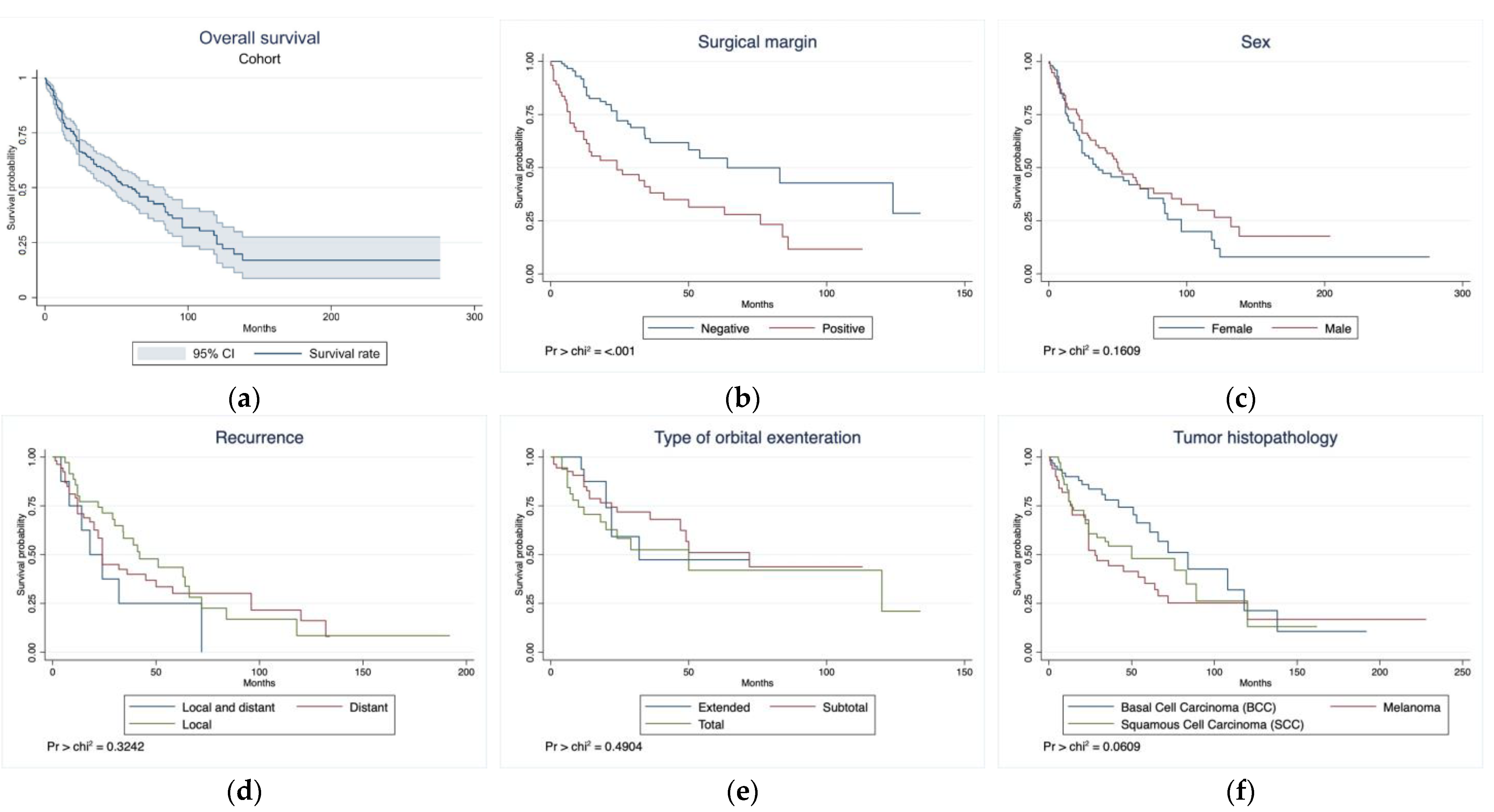
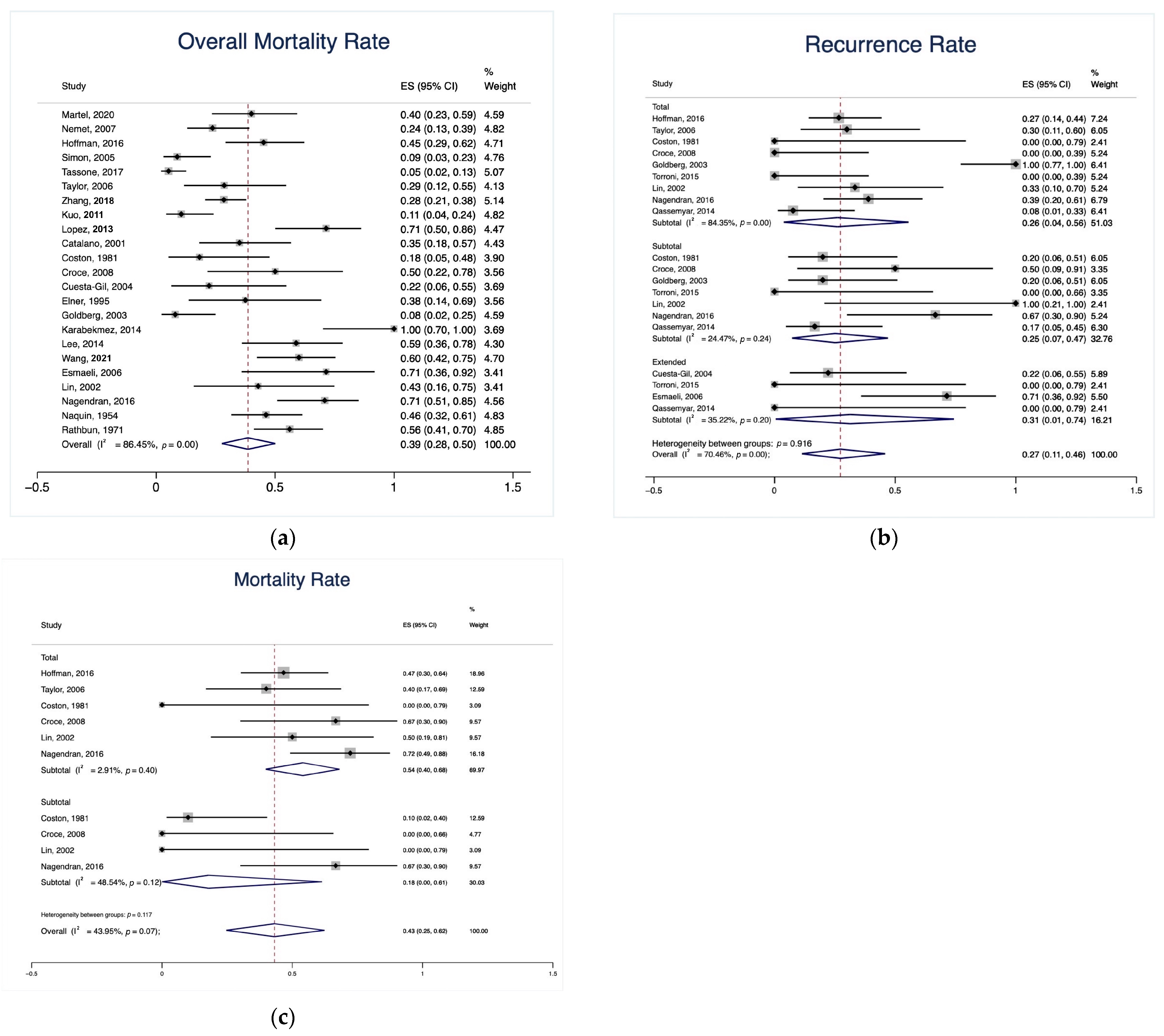
3.4. Clinical and Survival Outcomes
4. Discussion
4.1. Demographics and Clinical Characteristics of the Cohort
4.2. Management Paradigm and Complications
4.3. Clinical and Survival Outcomes
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sokoya, M.; Cohn, J.E.; Kohlert, S.; Lee, T.; Kadakia, S.; Ducic, Y. Orbital Reconstruction: Considerations in Orbital Exenteration. Semin. Plast. Surg. 2019, 33, 103–105. [Google Scholar] [CrossRef]
- Zhang, Z.; Ho, S.; Yin, V.; Varas, G.; Rajak, S.; Dolman, P.J.; McNab, A.; Heathcote, J.G.; Valenzuela, A. Multicentred International Review of Orbital Exenteration and Reconstruction in Oculoplastic and Orbit Practice. Br. J. Ophthalmol. 2018, 102, 654–658. [Google Scholar] [CrossRef]
- Simon, G.J.B.; Schwarcz, R.M.; Douglas, R.; Fiaschetti, D.; McCann, J.D.; Goldberg, R.A. Orbital Exenteration: One Size Does Not Fit All. Am. J. Ophthalmol. 2005, 139, 11–17. [Google Scholar] [CrossRef]
- Goldberg, R.A.; Kim, J.W.; Shorr, N. Orbital Exenteration: Results of an Individualized Approach. Ophthalmic Plast. Reconstr. Surg. 2003, 19, 229–236. [Google Scholar] [CrossRef]
- Kesting, M.R.; Koerdt, S.; Rommel, N.; Mücke, T.; Wolff, K.D.; Nobis, C.P.; Ringel, F.; Frohwitter, G. Classification of Orbital Exenteration and Reconstruction. J. Craniomaxillofac Surg. 2017, 45, 467–473. [Google Scholar] [CrossRef]
- Martel, A.; Oberic, A.; Moulin, A.; Zografos, L.; Bellini, L.; Almairac, F.; Hamedani, M. Orbital Exenteration and Conjunctival Melanoma: A 14-Year Study at the Jules Gonin Eye Hospital. Eye 2020, 34, 1897–1902. [Google Scholar] [CrossRef]
- Ali, M.J.; Pujari, A.; Dave, T.V.; Kaliki, S.; Naik, M.N. Clinicopathological Profile of Orbital Exenteration: 14 Years of Experience from a Tertiary Eye Care Center in South India. Int. Ophthalmol. 2016, 36, 253–258. [Google Scholar] [CrossRef]
- Nemet, A.Y.; Martin, P.; Benger, R.; Kourt, G.; Sharma, V.; Ghabrial, R.; Danks, J. Orbital Exenteration: A 15-Year Study of 38 Cases. Ophthalmic Plast. Reconstr. Surg. 2007, 23, 468–472. [Google Scholar] [CrossRef]
- Hoffman, G.R.; Jefferson, N.D.; Reid, C.B.A.; Eisenberg, R.L. Orbital Exenteration to Manage Infiltrative Sinonasal, Orbital Adnexal, and Cutaneous Malignancies Provides Acceptable Survival Outcomes: An Institutional Review, Literature Review, and Meta-Analysis. J. Oral. Maxillofac. Surg. 2016, 74, 631–643. [Google Scholar] [CrossRef]
- Kuo, C.H.; Gao, K.; Clifford, A.; Shannon, K.; Clark, J. Orbital Exenterations: An 18-Year Experience from a Single Head and Neck Unit. ANZ J. Surg. 2011, 81, 326–330. [Google Scholar] [CrossRef]
- Tassone, P.; Gill, K.S.; Hsu, D.; Nyquist, G.; Krein, H.; Bilyk, J.R.; Murchison, A.P.; Evans, J.J.; Heffelfinger, R.N.; Curry, J.M. Naso- or Orbitocutaneous Fistulas after Free Flap Reconstruction of Orbital Exenteration Defects: Retrospective Study, Systematic Review, and Meta-Analysis. J. Neurol. Surg. B Skull Base 2017, 78, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.; Roberts, F.; Kemp, E.G. Orbital Exenteration--a Retrospective Study over an 11 Year Period Analyzing All Cases from a Single Unit. Orbit 2006, 25, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Gill, K.S.; Hsu, D.; Tassone, P.; Pluta, J.; Nyquist, G.; Krein, H.; Bilyk, J.; Murchison, A.P.; Iloreta, A.; Evans, J.J.; et al. Postoperative Cerebrospinal Fluid Leak after Microvascular Reconstruction of Craniofacial Defects with Orbital Exenteration. Laryngoscope 2017, 127, 835–841. [Google Scholar] [CrossRef] [PubMed]
- López, F.; Suárez, C.; Carnero, S.; Martín, C.; Camporro, D.; Llorente, J.L. Free Flaps in Orbital Exenteration: A Safe and Effective Method for Reconstruction. Eur. Arch. Otorhinolaryngol. 2013, 270, 1947–1952. [Google Scholar] [CrossRef] [PubMed]
- Baum, S.; Klein, M.; Mohr, C.; Weischer, T. Long-Term Results of Endosseous Implants as Retention Elements of Orbital Epitheses, Reconstruction Techniques, and Aftercare after Radical Tumor Resection. Int. J. Oral. Maxillofac. Implants 2019, 34, 745–751. [Google Scholar] [CrossRef]
- Martel, A.; Baillif, S.; Nahon-Esteve, S.; Gastaud, L.; Bertolotto, C.; Lassalle, S.; Lagier, J.; Hamedani, M.; Poissonnet, G. Orbital Exenteration: An Updated Review with Perspectives. Surv. Ophthalmol. 2021, 66, 856–876. [Google Scholar] [CrossRef]
- Nagendran, S.T.; Lee, N.G.; Fay, A.; Lefebvre, D.R.; Sutula, F.C.; Freitag, S.K. Orbital Exenteration: The 10-Year Massachusetts Eye and Ear Infirmary Experience. Orbit 2016, 35, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.Y.; Liao, S.L.; Wei, Y.H. Orbital Exenteration: A 20-Year Experience from a Tertiary Center in Taiwan. J. Formos. Med. Assoc. 2021, 120, 1493–1499. [Google Scholar] [CrossRef]
- Qassemyar, A.; Aljudaibi, N.; Wavreille, O.; Mortier, L.; Martinot-Duquennoy, V.; Guerreschi, P. Orbital Exenteration and Periorbital Skin Cancers. J. Oral. Maxillofac. Surg. 2014, 72, 811–816. [Google Scholar] [CrossRef]
- Greig, A.V.H.; Jones, S.; Haylock, C.; Joshi, N.; McLellan, G.; Clarke, P.; Kirkpatrick, W.N.A. Reconstruction of the Exenterated Orbit with Osseointegrated Implants. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 1656–1665. [Google Scholar] [CrossRef]
- Van Den Elzen, M.E.P.; Versnel, S.L.; Hovius, S.E.R.; Passchier, J.; Duivenvoorden, H.J.; Mathijssen, I.M.J. Adults with Congenital or Acquired Facial Disfigurement: Impact of Appearance on Social Functioning. J. Craniomaxillofac Surg. 2012, 40, 777–782. [Google Scholar] [CrossRef]
- Ariani, N.; Visser, A.; van Oort, R.P.; Kusdhany, L.; Rahardjo, T.B.W.; Krom, B.P.; van der Mei, H.C.; Vissink, A. Current State of Craniofacial Prosthetic Rehabilitation. Int. J. Prosthodont. 2013, 26, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Nassab, R.S.; Thomas, S.S.; Murray, D. Orbital Exenteration for Advanced Periorbital Skin Cancers: 20 Years Experience. J. Plast. Reconstr. Aesthet. Surg. 2007, 60, 1103–1109. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- OCEBM Levels of Evidence—Centre for Evidence-Based Medicine (CEBM), University of Oxford. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 16 July 2023).
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological Quality of Case Series Studies: An Introduction to the JBI Critical Appraisal Tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Frezzotti, R.; Bonanni, R.; Nuti, A.; Polito, E. Radical Orbital Resections. Adv. Ophthalmic Plast. Reconstr. Surg. 1992, 9, 175–192. [Google Scholar] [PubMed]
- Rich, J.T.; Neely, J.G.; Paniello, R.C.; Voelker, C.C.J.; Nussenbaum, B.; Wang, E.W. A Practical guide to understanding kaplan-meier curves. Otolaryngol. Head. Neck Surg. 2010, 143, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Deo, S.V.; Deo, V.; Sundaram, V. Survival Analysis—Part 2: Cox Proportional Hazards Model. Indian. J. Thorac. Cardiovasc. Surg. 2021, 37, 229–233. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for Examining and Interpreting Funnel Plot Asymmetry in Meta-Analyses of Randomised Controlled Trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Cumming, B.; Sideris, A.; Holmes, T.R.; Jacobson, I.; Havas, T. Orbital Exenteration: Tumour Diversity and Survival in a Tertiary Referral Centre. Aust. J. Otolaryngol. 2019, 2, 23. [Google Scholar] [CrossRef]
- Gerring, R.C.; Ott, C.T.; Curry, J.M.; Sargi, Z.B.; Wester, S.T. Orbital Exenteration for Advanced Periorbital Non-Melanoma Skin Cancer: Prognostic Factors and Survival. Eye 2017, 31, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.J.; Laidlaw, D.; Sen, C. Globe Sparing Orbital Exenteration. Otolaryngol. Head. Neck Surg. 2001, 125, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Croce, A.; Moretti, A.; D’Agostino, L.; Zingariello, P. Orbital Exenteration in Elderly Patients: Personal Experience. Acta Otorhinolaryngol. Ital. 2008, 28, 193. [Google Scholar]
- Elkhamary, S.M.; Galindo-Ferreiro, A.; Akaishi, P.; Muiños-Diaz, Y.; Cechetti, S.P.; Cintra, M.B.; Cruz, A.A.V. Hyperostosis Following Orbital Exenteration. Ophthalmic Plast. Reconstr. Surg. 2017, 33, 241–243. [Google Scholar] [CrossRef]
- Lee, P.S.; Sedrak, P.; Guha-Thakurta, N.; Chang, E.I.; Ginsberg, L.E.; Esmaeli, B.; Debnam, J.M. Imaging Findings of Recurrent Tumors after Orbital Exenteration and Free Flap Reconstruction. Ophthalmic Plast. Reconstr. Surg. 2014, 30, 315–321. [Google Scholar] [CrossRef]
- Maheshwari, R. Review of Orbital Exenteration from an Eye Care Centre in Western India. Orbit 2010, 29, 35–38. [Google Scholar] [CrossRef]
- Ogun, G.O.; Ogun, O.A.; Bekibele, C.O.; Akang, E.E. Intraepithelial and Invasive Squamous Neoplasms of the Conjunctiva in Ibadan, Nigeria: A Clinicopathological Study of 46 Cases. Int. Ophthalmol. 2009, 29, 401–409. [Google Scholar] [CrossRef]
- Torroni, A.; Cervelli, D.; Gasparini, G.; Grussu, F.; Moro, A.; Marianetti, T.M.; Foresta, E.; Azzuni, C.; Pelo, S. Anterior Retrograde Approach to the Myofascial Temporalis Muscle for Orbital Reconstruction: Series of 9 Consecutive Cases. Ann. Plast. Surg. 2015, 74, 37–42. [Google Scholar] [CrossRef]
- Esmaeli, B.; Golio, D.; Kies, M.; DeMonte, F. Surgical Management of Locally Advanced Adenoid Cystic Carcinoma of the Lacrimal Gland. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 366–370. [Google Scholar] [CrossRef]
- Rathbun, J.E.; Beard, C.; Quickert, M.H. Evaluation of 48 Cases of Orbital Exenteration. Am. J. Ophthalmol. 1971, 72, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Coston, T.O.; Small, R.G. Orbital Exenteration--Simplified. Trans. Am. Ophthalmol. Soc. 1981, 79, 136–152. [Google Scholar] [PubMed]
- Lin, H.-F.; Lui, C.-C.; Hsu, H.-C.; Lin, S.-A. Orbital Exenteration for Secondary Orbital Tumors: A Series of Seven Cases. Chang. Gung Med. J. 2002, 25, 599–605. [Google Scholar] [PubMed]
- Naquin, H.A. Exenteration of the Orbit. AMA Arch. Ophthalmol. 1954, 51, 850–862. [Google Scholar] [CrossRef]
- Elner, V.M.; Burnstine, M.A.; Goodman, M.L.; Dortzbach, R.K. Inverted Papillomas That Invade the Orbit. Arch. Ophthalmol. 1995, 113, 1178–1183. [Google Scholar] [CrossRef]
- Karabekmez, F.E.; Selimoglu, M.N.; Duymaz, A.; Karamese, M.S.; Keskin, M.; Savaci, N. Management of Neglected Periorbital Squamous Cell Carcinoma Requiring Orbital Exenteration. J. Craniofac Surg. 2014, 25, 729–734. [Google Scholar] [CrossRef]
- Cuesta-Gil, M.; Concejo, C.; Acero, J.; Navarro-Vila, C.; Ochandiano, S. Repair of Large Orbito-Cutaneous Defects by Combining Two Classical Flaps. J. Cranio-Maxillofac. Surg. 2004, 32, 21–27. [Google Scholar] [CrossRef]
- Aryasit, O.; Preechawai, P.; Hirunpat, C.; Horatanaruang, O.; Singha, P. Factors Related to Survival Outcomes Following Orbital Exenteration: A Retrospective, Comparative, Case Series. BMC Ophthalmol. 2018, 18, 186. [Google Scholar] [CrossRef]
- Fleming, J.C.; Morley, I.; Malik, M.; Orfaniotis, G.; Daniel, C.; Townley, W.A.; Jeannon, J.P. Orbital Exenteration and Reconstruction in a Tertiary UK Institution: A 5-Year Experience. Orbit 2021, 40, 306–315. [Google Scholar] [CrossRef]
- Kato, J.M.; da Fonseca, F.L.; Matayoshi, S. Survival Following Orbital Exenteration at a Tertiary Brazilian Hospital. Rev. Col. Bras. Cir. 2016, 43, 042–047. [Google Scholar] [CrossRef][Green Version]
- Langlois, B.; Jacomet, P.V.; Putterman, M.; Morax, S.; Galatoire, O. Evaluation of Reconstructive Techniques after Orbital Exenteration in 56 Cases. J. Fr. Ophtalmol. 2012, 35, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Cinar, C.; Arslan, H.; Bingol, U.A.; Aydin, Y.; Cetinkale, O. The New Anatomical Classification System for Orbital Exenteration Defect. J. Craniofac Surg. 2017, 28, 1687–1693. [Google Scholar] [CrossRef] [PubMed]
- Dallan, I.; Picariello, M.; Fiacchini, G. Conservative Management of Orbital Involvement in Malignant Tumors: Is the Paradigm Evolving? A Critical Review. Curr. Opin. Otolaryngol. Head. Neck Surg. 2022, 30, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Mukoyama, N.; Nishio, N.; Kimura, H.; Kishi, S.; Tokura, T.; Kimura, H.; Hiramatsu, M.; Maruo, T.; Tsuzuki, H.; Fujii, M.; et al. Prospective Evaluation of Health-Related Quality of Life in Patients Undergoing Anterolateral Craniofacial Resection with Orbital Exenteration. J. Neurol. Surg. B Skull Base 2020, 81, 585–593. [Google Scholar] [CrossRef]
- Baum, S.H.; Oeverhaus, M.; Saxe, F.; Mohr, C. Modified Types of Orbital Exenteration, Survival, and Reconstruction. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2305–2312. [Google Scholar] [CrossRef]
- Fleming, J.C.; Linder, J.S.; Karcioglu, Z.A. Orbital Hyperostosis Following Exenteration. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 378–382. [Google Scholar] [CrossRef]
- Sugawara, T.; Aoyagi, M.; Ogishima, T.; Kawano, Y.; Tamaki, M.; Yano, T.; Tsunoda, A.; Ohno, K.; Maehara, T.; Kishimoto, S. Extended Orbital Exenteration for Sinonasal Malignancy with Orbital Apex Extension: Surgical Technique and Clinical Analysis. J. Neurosurg. 2015, 123, 52–58. [Google Scholar] [CrossRef]
- Badhey, A.; Haidar, Y.; Genden, E. Orbital Reconstruction: Soft Tissue Microvascular Reconstruction of Orbital Exenteration Defects. Semin. Plast. Surg. 2019, 33, 125–131. [Google Scholar] [CrossRef]
- Al-Hity, A.; Gregory, M.E.; Kemp, E.G. The Intraoperative Use of Polydioxanone Foil to Reduce the Risk of Sino-Orbital Fistula Formation in Orbital Exenteration. Orbit 2018, 37, 140–144. [Google Scholar] [CrossRef]
- Kiratli, H.; Koç, İ. Orbital Exenteration: Institutional Review of Evolving Trends in Indications and Rehabilitation Techniques. Orbit 2018, 37, 179–186. [Google Scholar] [CrossRef]
- Cocuzza, S.; Maniaci, A.; Di Luca, M.; Mantia, I.L.; Grillo, C.; Spinato, G.; Motta, G.; Testa, D.; Ferlito, S. Long-Term Results of Nasal Surgery: Comparison of Mini-Invasive Turbinoplasty. J. Biol. Regul. Homeost. Agents 2020, 34, 1203–1208. [Google Scholar] [CrossRef] [PubMed]
- Maniaci, A.; Merlino, F.; Cocuzza, S.; Iannella, G.; Vicini, C.; Cammaroto, G.; Lechien, J.R.; Calvo-Henriquez, C.; La Mantia, I. Endoscopic Surgical Treatment for Rhinogenic Contact Point Headache: Systematic Review and Meta-Analysis. Eur. Arch. Otorhinolaryngol. 2021, 278, 1743–1753. [Google Scholar] [CrossRef] [PubMed]
- Skinner, H.D.; Garden, A.S.; Rosenthal, D.I.; Ang, K.K.; Morrison, W.H.; Esmaeli, B.; Pinnix, C.C.; Frank, S.J. Outcomes of Malignant Tumors of the Lacrimal Apparatus: The University of Texas MD Anderson Cancer Center Experience. Cancer 2011, 117, 2801–2810. [Google Scholar] [CrossRef]
- Hsu, A.; Frank, S.J.; Ballo, M.T.; Garden, A.S.; Morrison, W.H.; Rosenthal, D.I.; Hatef, E.; Esmaeli, B. Postoperative Adjuvant External-Beam Radiation Therapy for Cancers of the Eyelid and Conjunctiva. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Rahman, I.; Maino, A.; Cook, A.E.; Leatherbarrow, B. Mortality Following Exenteration for Malignant Tumours of the Orbit. Br. J. Ophthalmol. 2005, 89, 1445–1448. [Google Scholar] [CrossRef]
- Roche, P.; Timon, C. Orbital Exenteration in Periorbital Malignancies. Surgeon 2012, 10, 189–193. [Google Scholar] [CrossRef]
- Patel, S.G.; Singh, B.; Polluri, A.; Bridger, P.G.; Cantu, G.; Cheesman, A.D.; DeSa, G.M.; Donald, P.; Fliss, D.; Gullane, P.; et al. Craniofacial Surgery for Malignant Skull Base Tumors: Report of an International Collaborative Study. Cancer 2003, 98, 1179–1187. [Google Scholar] [CrossRef]
- Wong, J.C.L.; Thampy, R.; Cook, A. Life Expectancy Following Orbital Exenteration. Br. J. Ophthalmol. 2015, 99, 1–4. [Google Scholar] [CrossRef]
- Traylor, J.I.; Christiano, L.D.; Esmaeli, B.; Hanasono, M.M.; Yu, P.; Suki, D.; Zhang, W.; Raza, S.M.; Hanna, E.Y.; DeMonte, F. Outcomes of Orbital Exenteration for Craniofacial Lesions. Cancer 2021, 127, 2465–2475. [Google Scholar] [CrossRef]
- Sullivan, C.B.; Andresen, N.S.; Kendell, N.; Al-Qurayshi, Z.; Pagedar, N.A. Survival Outcomes for Advanced Cutaneous Squamous Cell Carcinoma of the Head and Neck. Ann. Otol. Rhinol. Laryngol. 2019, 128, 949–955. [Google Scholar] [CrossRef]
- Mouriaux, F.; Martinot, V.; Pellerin, P.; Patenotre, P.; Rouland, J.F.; Constantinides, G. Survival after Malignant Tumors of the Orbit and Periorbit Treated by Exenteration. Acta Ophthalmol. Scand. 1999, 77, 326–330. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Involved structures | n = 989 |
| Eyelids | 160 (16.2%) |
| Orbit | 142 (14.4%) |
| Conjunctiva | 124 (12.5%) |
| Canthus | 79 (8.0%) |
| Sinuses | 59 (6.0%) |
| Face | 41 (4.1%) |
| Lacrimal gland | 37 (3.7%) |
| Choroid | 23 (2.3%) |
| Nose | 22 (2.2%) |
| Unspecified peri-oculus | 19 (2.0%) |
| Periorbital skin | 15 (1.5%) |
| Eye | 14 (1.4%) |
| Cheek | 10 (1.0%) |
| Brain | 9 (0.9%) |
| Supraorbital/brow | 8 (0.8%) |
| Lacrimal sac | 7 (0.7%) |
| Ethmoid bone | 6 (0.6%) |
| Lacrimal duct | 4 (0.4%) |
| Maxilla | 3 (0.3%) |
| Temporal skin | 3 (0.3%) |
| Extraocular muscles | 2 (0.2%) |
| Temple | 2 (0.2%) |
| Alveoli | 1 (0.1%) |
| Nasopharynx | 1 (0.1%) |
| Ophthalmic nerve | 1 (0.1%) |
| Optic nerve | 1 (0.1%) |
| Parotid | 1 (0.1%) |
| Periorbital fat | 1 (0.1%) |
| Others | 194 (19.6%) |
| Presenting signs and symptoms | n = 113 * |
| Disturbed vision | 47 (22.5%) |
| Facial mass | 37 (17.7%) |
| Conjunctival injection | 31 (14.7%) |
| Eye pain | 27 (13.0%) |
| Lesion discharge | 25 (12.0%) |
| Epiphora | 18 (8.6%) |
| Diplopia | 16 (7.7%) |
| Orbital discomfort | 8 (3.8%) |
| Variable | n (%) |
|---|---|
| Orbital exenteration extent of resection | n = 957 |
| Total | 302 (31.6%) |
| Extended | 248 (26.0%) |
| Subtotal | 87 (9.0%) |
| Unspecified | 320 (33.4%) |
| Additional surgical interventions | n = 146 |
| Maxillectomy | 57 (39.0%) |
| Lymph node resection | 36 (24.7%) |
| Ethmoidectomy | 17 (11.6%) |
| Craniotomy | 14 (9.6%) |
| Parotidectomy | 5 (3.4%) |
| Craniofacial resection | 4 (2.7%) |
| Enucleation | 4 (2.7%) |
| Rhinectomy | 3 (2.1%) |
| Tracheostomy | 3 (2.1%) |
| Posterior orbit sparing | 2 (1.4%) |
| Temporal bone resection | 1 (0.7%) |
| Complications | n = 168 * |
| Sino-orbital/nasal fistula | 40 (22.6%) |
| Flap/graft/implant failure (loss/necrosis/atrophy) | 30 (16.9%) |
| Hyperostosis | 23 (13.0%) |
| Wound dehiscence/non-healing | 19 (10.7%) |
| CSF leak | 15 (8.5%) |
| Surgical site infection | 12 (6.7%) |
| Brain invasion | 7 (4.0%) |
| Hematoma | 6 (3.3%) |
| Socket hemorrhage | 6 (3.3%) |
| Socket draining | 3 (1.7%) |
| Transient facial weakness | 3 (1.7%) |
| Myocardial infarction | 2 (1.1%) |
| Stroke | 2 (1.1%) |
| Pulmonary infection | 1 (0.6%) |
| Delirium tremens | 1 (0.6%) |
| Eyelid fistula | 1 (0.6%) |
| Meningitis | 1 (0.6%) |
| Orbital abscess | 1 (0.6%) |
| Osteitis | 1 (0.6%) |
| Permanent facial weakness | 1 (0.6%) |
| Pulmonary edema | 1 (0.6%) |
| Trigeminal neuralgia | 1 (0.6%) |
| Variable | n (%) |
|---|---|
| Reconstructive technique | n = 820 |
| Free flap | 273 (33.3%) |
| Endosseous implant | 187 (22.8%) |
| Split-thickness skin graft | 141 (17.2%) |
| Full-thickness skin graft | 65 (8.0%) |
| Facial prosthesis | 56 (6.8%) |
| Spontaneous granulation | 54 (6.6%) |
| Orbital implant | 24 (2.9%) |
| Surgical closure of the orbit | 10 (1.2%) |
| Titanium plates | 10 (1.2%) |
| Reconstructive material | n = 587 |
| Anterolateral thigh flap | 156 (26.6%) |
| Musculocutaneous flap | 127 (21.6%) |
| Radial forearm flap | 85 (14.5%) |
| Forehead flap | 39 (6.6%) |
| Temporalis myofascial flap | 39 (6.6%) |
| Lid flap | 23 (3.9%) |
| Rectus abdominis flap | 21 (3.6%) |
| Dermis-fat graft | 19 (3.2%) |
| Latissimus dorsi flap | 11 (1.9%) |
| Temporalis muscle flap | 11 (1.9%) |
| Cheek rotation flap | 10 (1.7%) |
| Facio-cervico-pectoral flap | 9 (1.5%) |
| Pericranial flap | 7 (1.2%) |
| Abdomen/sub-mammary skin | 6 (1.0%) |
| Mustarde flap | 4 (0.6%) |
| Cervicofacial flap | 3 (0.5%) |
| Fibula osteocutaneous flap | 2 (0.3%) |
| Lateral arm flap | 2 (0.3%) |
| Scalp flap | 2 (0.3%) |
| Buccal mucosa graft | 1 (0.2%) |
| Deep inferior epigastric perforators flap | 1 (0.2%) |
| Fasciocutaneous flap | 1 (0.2%) |
| Galea frontalis flap | 1 (0.2%) |
| Gastrocnemius flap | 1 (0.2%) |
| Gracilis flap | 1 (0.2%) |
| Parotid/left cheek skin | 1 (0.2%) |
| Pectoralis major flap | 1 (0.2%) |
| Temporoparietal fascia flap | 1 (0.2%) |
| Thoracodorsal artery perforator flap | 1 (0.2%) |
| Vastus lateralis flap | 1 (0.2%) |
| Variable | n (%) |
|---|---|
| Chemotherapy | n = 47 † |
| Neoadjuvant | 16 (31.4%) |
| Adjuvant | 35 (68.6%) |
| Radiotherapy | n = 414 † |
| Primary a | 106 (25.0%) |
| Neoadjuvant | 52 (12.3%) |
| Adjuvant | 266 (62.7%) |
| Patients had both chemotherapy and radiotherapy. | n = 29 |
| Variable | n (%)/n (95% CI) |
|---|---|
| Recurrence | n = 210 * |
| Local | 109 (38.6%) |
| Distant | 91 (32.3%) |
| Regional | 19 (6.7%) |
| Perineural invasion | 49 (17.4%) |
| Lymphovascular invasion | 14 (5.0%) |
| Surgical margins | n = 444 |
| Positive | 136 (30.6%) |
| Negative | 308 (69.4%) |
| Status | n = 587 |
| Alive | 372 (63.4%) |
| Dead | 215 (36.6%) |
| Death cause | n = 195 |
| Disease complication | 144 (73.8%) |
| Unrelated cause | 51 (26.2%) |
| Overall median survival time, months | 61 (95% CI: 46–83) |
| Overall survival rates | |
| 5-year | 50.0% |
| 10-year | 24.0% |
| Weighted mean follow-up time, months | 23.6 (95% CI: 13.8–33.4) |
| Predictor Variables | Overall Survival | |||
|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | |||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 1.01 (1.00–1.02) | 0.04 * | 1.03 (1.00–1.06) | 0.09 |
| Male (vs. female) | 0.78 (0.54–1.11) | 0.17 | NA | NA |
| SCC (vs. BCC) | 1.58 (0.92–2.72) | 0.10 | NA | NA |
| Melanoma (vs. BCC) | 1.90 (1.09–3.32) | 0.02 * | 2.88 (0.70–11.9) | 0.14 |
| Total (vs. Subtotal) OE | 1.25 (0.50–3.10) | 0.63 | NA | NA |
| Positive (vs. negative) margin | 2.39 (1.48–3.86) | <0.001 * | 2.04 (0.88–4.70) | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qedair, J.; Haider, A.S.; Balasubramanian, K.; Palmisciano, P.; Hassan, T.; Shahbandi, A.; Sabahi, M.; Kharbat, A.F.; Abou-Al-Shaar, H.; Yu, K.; et al. Orbital Exenteration for Craniofacial Lesions: A Systematic Review and Meta-Analysis of Patient Characteristics and Survival Outcomes. Cancers 2023, 15, 4285. https://doi.org/10.3390/cancers15174285
Qedair J, Haider AS, Balasubramanian K, Palmisciano P, Hassan T, Shahbandi A, Sabahi M, Kharbat AF, Abou-Al-Shaar H, Yu K, et al. Orbital Exenteration for Craniofacial Lesions: A Systematic Review and Meta-Analysis of Patient Characteristics and Survival Outcomes. Cancers. 2023; 15(17):4285. https://doi.org/10.3390/cancers15174285
Chicago/Turabian StyleQedair, Jumanah, Ali S. Haider, Kishore Balasubramanian, Paolo Palmisciano, Taimur Hassan, Ataollah Shahbandi, Mohammadmahdi Sabahi, Abdurrahman F. Kharbat, Hussam Abou-Al-Shaar, Kenny Yu, and et al. 2023. "Orbital Exenteration for Craniofacial Lesions: A Systematic Review and Meta-Analysis of Patient Characteristics and Survival Outcomes" Cancers 15, no. 17: 4285. https://doi.org/10.3390/cancers15174285
APA StyleQedair, J., Haider, A. S., Balasubramanian, K., Palmisciano, P., Hassan, T., Shahbandi, A., Sabahi, M., Kharbat, A. F., Abou-Al-Shaar, H., Yu, K., Cohen-Gadol, A. A., El Ahmadieh, T. Y., & Bin-Alamer, O. (2023). Orbital Exenteration for Craniofacial Lesions: A Systematic Review and Meta-Analysis of Patient Characteristics and Survival Outcomes. Cancers, 15(17), 4285. https://doi.org/10.3390/cancers15174285