

Real-World Evidence on the Clinical Characteristics and Management of Patients with Chronic Lymphocytic Leukemia in Spain Using Natural Language Processing: The SRealCLL Study

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
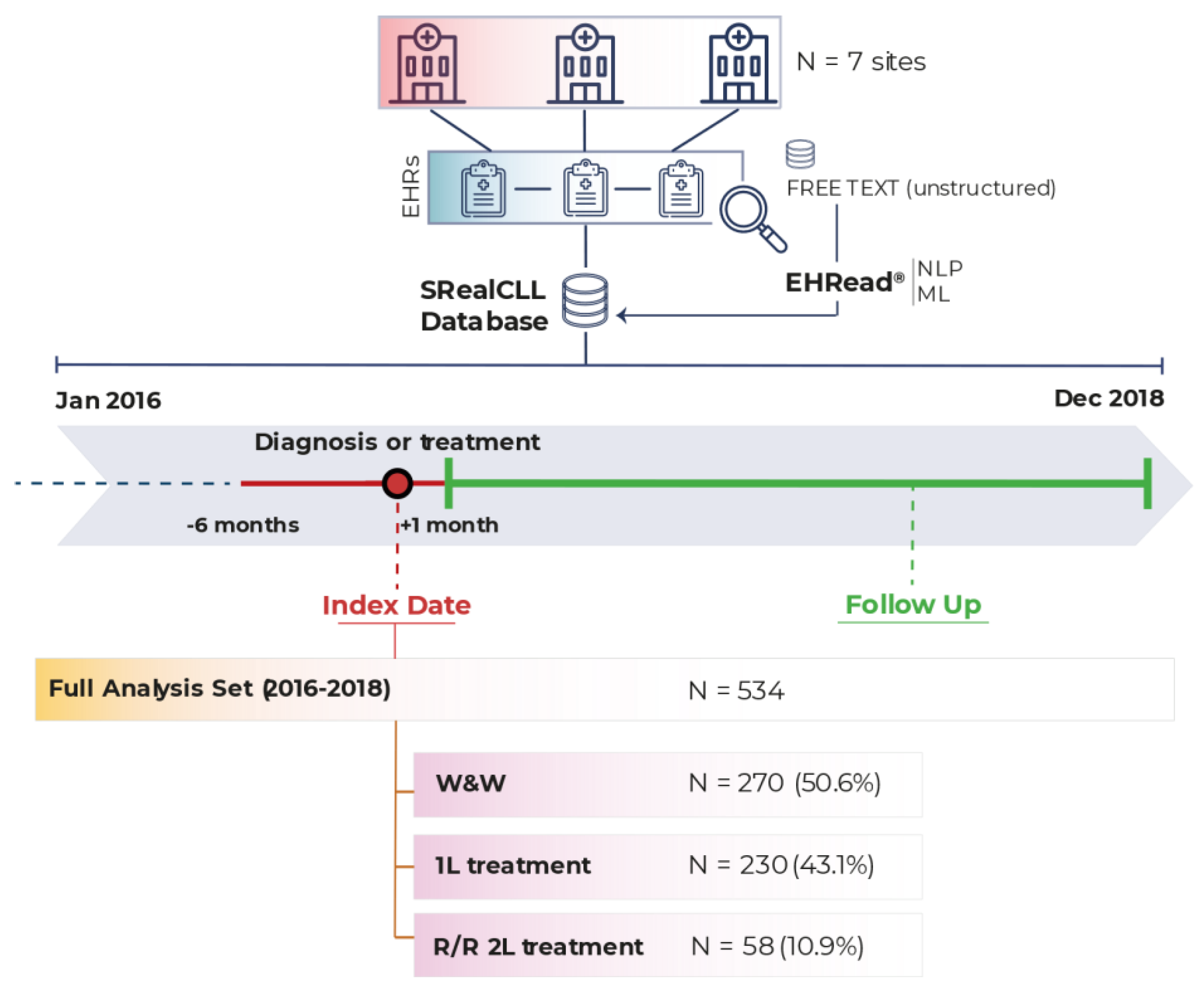
2. Methods
2.1. Study Design and Data Source
2.2. Study Population
2.3. Study Variables
2.4. Statistical Data Analyses
3. Results
3.1. Overall Population Description
3.2. Comorbidities and Concomitant Medication
3.3. Treatment Patterns and Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hallek, M. Chronic lymphocytic leukemia: 2020 update on diagnosis, risk stratification and treatment. Am. J. Hematol. 2019, 94, 1266–1287. [Google Scholar] [CrossRef]
- Campo, E.; Swerdlow, S.H.; Harris, N.L.; Pileri, S.; Stein, H.; Jaffe, E.S. The 2008 WHO classification of lymphoid neoplasms and beyond: Evolving concepts and practical applications. Blood 2011, 117, 5019–5032. [Google Scholar] [CrossRef] [PubMed]
- Kipps, T.J.; Stevenson, F.K.; Wu, C.J.; Croce, C.M.; Packham, G.; Wierda, W.G.; O’Brien, S.; Gribben, J.; Rai, K. Chronic lymphocytic leukaemia. Nat. Rev. Dis. Primers 2017, 3, 16096. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, Y.; Wang, Z.; Yi, D.; Ma, S. Racial differences in three major NHL subtypes: Descriptive epidemiology. Cancer Epidemiol. 2015, 39, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Pulte, D.; Redaniel, M.T.; Bird, J.; Jeffreys, M. Survival for patients with chronic leukemias in the US and Britain: Age-related disparities and changes in the early 21st century. Eur. J. Haematol. 2015, 94, 540–545. [Google Scholar] [CrossRef]
- Eichhorst, B.; Robak, T.; Montserrat, E.; Ghia, P.; Niemann, C.U.; Kater, A.P.; Gregor, M.; Cymbalista, F.; Buske, C.; Hillmen, P.; et al. Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 23–33. [Google Scholar] [CrossRef]
- Nabhan, C.; Rosen, S.T. Chronic lymphocytic leukemia: A clinical review. JAMA 2014, 312, 2265–2276. [Google Scholar] [CrossRef]
- Sant, M.; Allemani, C.; Tereanu, C.; De Angelis, R.; Capocaccia, R.; Visser, O.; Marcos-Gragera, R.; Maynadie, M.; Simonetti, A.; Lutz, J.M.; et al. Incidence of hematologic malignancies in Europe by morphologic subtype: Results of the HAEMACARE project. Blood 2010, 116, 3724–3734. [Google Scholar] [CrossRef]
- Hallek, M.; Cheson, B.D.; Catovsky, D.; Caligaris-Cappio, F.; Dighiero, G.; Döhner, H.; Hillmen, P.; Keating, M.; Montserrat, E.; Chiorazzi, N.; et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 2018, 131, 2745–2760. [Google Scholar] [CrossRef]
- Pérez-Carretero, C.; González-Gascón-Y-Marín, I.; Rodríguez-Vicente, A.E.; Quijada-Álamo, M.; Hernández-Rivas, J.-Á.; Hernández-Sánchez, M.; Hernández-Rivas, J.M. The Evolving Landscape of Chronic Lymphocytic Leukemia on Diagnosis, Prognosis and Treatment. Diagnostics 2021, 11, 853. [Google Scholar] [CrossRef]
- González-Gascón-Y-Marín, I.; Muñoz-Novas, C.; Rodríguez-Vicente, A.-E.; Quijada-Álamo, M.; Hernández-Sánchez, M.; Pérez-Carretero, C.; Ramos-Ascanio, V.; Hernández-Rivas, J.-Á. From Biomarkers to Models in the Changing Landscape of Chronic Lymphocytic Leukemia: Evolve or Become Extinct. Cancers 2021, 13, 1782. [Google Scholar] [CrossRef] [PubMed]
- Abrisqueta, P.; Loscertales, J.; Terol, M.J.; Ramírez Payer, Á.; Ortiz, M.; Pérez, I.; Cuellar-García, C.; Fernández de la Mata, M.; Rodríguez, A.; Lario, A.; et al. Real-World Characteristics and Outcome of Patients Treated With Single-Agent Ibrutinib for Chronic Lymphocytic Leukemia in Spain (IBRORS-LLC Study). Clin. Lymphoma Myeloma Leuk. 2021, 21, e985–e999. [Google Scholar] [CrossRef] [PubMed]
- GELLC. Guías de Tratamiento de LLC. Available online: https://www.gellc.es/images/pdf/guias_gellcv1.pdf (accessed on 8 March 2023).
- Cancer Stat Facts: Leukemia—Chronic Lymphocytic Leukemia (CLL). 2021. Available online: https://seer.cancer.gov/statfacts/html/clyl.html (accessed on 8 March 2023).
- Spacek, M.; Smolej, L.; Simkovic, M.; Nekvindova, L.; Kristkova, Z.; Brychtova, Y.; Panovska, A.; Maslejova, S.; Bezdekova, L.; Ecsiova, D.; et al. Idelalisib plus rituximab versus ibrutinib in the treatment of relapsed/refractory chronic lymphocytic leukaemia: A real-world analysis from the Chronic Lymphocytic Leukemia Patients Registry (CLLEAR). Br. J. Haematol. 2023, 202, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Laurenti, L.; Scarfo, L.; Frustaci, A.M.; Sanna, A.; Iannella, E.; Caira, M.; Finsinger, P.; Schifano, S.; Neri, B.; Molica, S.; et al. Real-world evidence on venetoclax in chronic lymphocytic leukemia: The Italian experience. Hematol. Oncol. 2023. [Google Scholar] [CrossRef]
- Mulligan, S.P.; Opat, S.; Cheah, C.Y.; Kuss, B.; Hertzberg, M.; Marlton, P.; Poplar, S.; Puig, A.; McGeachie, M.; Weinkove, R.; et al. Real-world experience of Australian and New Zealand patients with chronic lymphocytic leukemia and mantle cell lymphoma accessing ibrutinib through a Named Patient Program. Leuk. Lymphoma 2023, 64, 312–318. [Google Scholar] [CrossRef]
- Shadman, M.; Manzoor, B.S.; Sail, K.; Tuncer, H.H.; Allan, J.N.; Ujjani, C.; Emechebe, N.; Kamalakar, R.; Coombs, C.C.; Leslie, L.; et al. Treatment Discontinuation Patterns for Patients with Chronic Lymphocytic Leukemia in Real-World Settings: Results From a Multi-Center International Study. Clin. Lymphoma Myeloma Leuk. 2023, 23, 515–526. [Google Scholar] [CrossRef]
- Janssens, A.; Berneman, Z.N.; Offner, F.; Snauwaert, S.; Mineur, P.; Vanstraelen, G.; Meers, S.; Spoormans, I.; Bron, D.; Vande Broek, I.; et al. Effectiveness and Safety of Ibrutinib for Chronic Lymphocytic Leukemia in Routine Clinical Practice: 3-Year Follow-up of the Belgian Ibrutinib Real-World Data (BiRD) Study. Clin. Hematol. Int. 2022, 4, 133–143. [Google Scholar] [CrossRef]
- Huang, Q.; Deering, K.L.; Harshaw, Q.; Leslie, L.A. Real-world Clinical Outcomes of First-Line Ibrutinib or Chemoimmunotherapy in Patients with Chronic Lymphocytic Leukemia by Risk Status. Adv. Ther. 2022, 39, 3292–3307. [Google Scholar] [CrossRef]
- Dartigeas, C.; Slama, B.; Doyle, M.; Tapprich, C.; Albrecht, C.; Dupuis, S.; Wapenaar, R.; Schmidt-Hieber, C.; Leblond, V. FIRE Study: Real-World Effectiveness and Safety of Ibrutinib in Clinical Practice in Patients with CLL and MCL. Clin. Hematol. Int. 2022, 4, 65–74. [Google Scholar] [CrossRef]
- Goyal, R.K.; Nagar, S.P.; Kabadi, S.M.; Le, H.; Davis, K.L.; Kaye, J.A. Overall survival, adverse events, and economic burden in patients with chronic lymphocytic leukemia receiving systemic therapy: Real-world evidence from the medicare population. Cancer Med. 2021, 10, 2690–2702. [Google Scholar] [CrossRef]
- Hou, J.Z.; Ryan, K.; Du, S.; Fang, B.; Marks, S.; Page, R.; Peng, E.; Szymanski, K.; Winters, S.; Le, H. Real-world ibrutinib dose reductions, holds and discontinuations in chronic lymphocytic leukemia. Future Oncol. 2021, 17, 4959–4969. [Google Scholar] [CrossRef] [PubMed]
- Rigolin, G.M.; Cavazzini, F.; Piciocchi, A.; Arena, V.; Visentin, A.; Reda, G.; Zamprogna, G.; Cibien, F.; Vitagliano, O.; Coscia, M.; et al. Efficacy of idelalisib and rituximab in relapsed/refractory chronic lymphocytic leukemia treated outside of clinical trials. A report of the Gimema Working Group. Hematol. Oncol. 2021, 39, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.J.; Gerrie, A.S.; Young, S.; Tucker, T.; Bruyere, H.; Hrynchak, M.; Galbraith, P.; Al Tourah, A.J.; Dueck, G.; Noble, M.C.; et al. Comparison of real-world treatment patterns in chronic lymphocytic leukemia management before and after availability of ibrutinib in the province of British Columbia, Canada. Leuk. Res. 2020, 91, 106335. [Google Scholar] [CrossRef]
- Islam, P.; Mato, A.R. Utilizing Real-World Evidence (RWE) to Improve Care in Chronic Lymphocytic Leukemia: Challenges and Opportunities. Curr. Hematol. Malig. Rep. 2020, 15, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Sylvan, S.E.; Asklid, A.; Johansson, H.; Klintman, J.; Bjellvi, J.; Tolvgård, S.; Kimby, E.; Norin, S.; Andersson, P.O.; Karlsson, C.; et al. First-line therapy in chronic lymphocytic leukemia: A Swedish nation-wide real-world study on 1053 consecutive patients treated between 2007 and 2013. Haematologica 2019, 104, 797–804. [Google Scholar] [CrossRef]
- Ferra, C.M.; Encinas, M.P.; Jimenez, J.L.; Ortiz, M.; Osorio-Prendes, S.; Cordoba, R.; Payer, A.R.; González-Barca, E.; Sánchez, G.M.; Diaz, M.G.; et al. Retrospective Non-Interventional Assessment of the Use of Idelalisib in Relapsed/Refractory Chronic Lymphocytic Leukemia Patients in Spain. Blood 2019, 134, 5473. [Google Scholar] [CrossRef]
- Marchetti, M.; Vitale, C.; Rigolin, G.M.; Vasile, A.; Visentin, A.; Scarfo, L.; Coscia, M.; Cuneo, A. Old and New Drugs for Chronic Lymphocytic Leukemia: Lights and Shadows of Real-World Evidence. J. Clin. Med. 2022, 11, 2076. [Google Scholar] [CrossRef]
- Del Rio-Bermudez, C.; Medrano, I.H.; Yebes, L.; Poveda, J.L. Towards a symbiotic relationship between big data, artificial intelligence, and hospital pharmacy. J. Pharm. Policy Pract. 2020, 13, 75. [Google Scholar] [CrossRef]
- Divita, G.; Carter, M.; Redd, A.; Zeng, Q.; Gupta, K.; Trautner, B.; Samore, M.; Gundlapalli, A. Scaling-up NLP Pipelines to Process Large Corpora of Clinical Notes. Methods Inf. Med. 2015, 54, 548–552. [Google Scholar] [CrossRef][Green Version]
- Luo, Y.; Thompson, W.K.; Herr, T.M.; Zeng, Z.; Berendsen, M.A.; Jonnalagadda, S.R.; Carson, M.B.; Starren, J. Natural Language Processing for EHR-Based Pharmacovigilance: A Structured Review. Drug Saf. 2017, 40, 1075–1089. [Google Scholar] [CrossRef]
- Neuraz, A.; Lerner, I.; Digan, W.; Paris, N.; Tsopra, R.; Rogier, A.; Baudoin, D.; Cohen, K.B.; Burgun, A.; Garcelon, N.; et al. Natural Language Processing for Rapid Response to Emergent Diseases: Case Study of Calcium Channel Blockers and Hypertension in the COVID-19 Pandemic. J. Med. Internet Res. 2020, 22, e20773. [Google Scholar] [CrossRef] [PubMed]
- Sheikhalishahi, S.; Miotto, R.; Dudley, J.T.; Lavelli, A.; Rinaldi, F.; Osmani, V. Natural Language Processing of Clinical Notes on Chronic Diseases: Systematic Review. JMIR Med. Inform. 2019, 7, e12239. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, J.L.; Almonacid, C.; González, Y.; Del Rio-Bermúdez, C.; Ancochea, J.; Cárdenas, R.; Soriano, J.B. The Impact of COVID-19 on Patients with Asthma. Eur. Respir. J. 2021, 57, 2003142. [Google Scholar] [CrossRef] [PubMed]
- Ancochea, J.; Izquierdo, J.L.; Medrano, I.H.; Porras, A.; Serrano, M.; Lumbreras, S.; Del Rio-Bermudez, C.; Marchesseau, S.; Salcedo, I.; Zubizarreta, I.; et al. Evidence of gender differences in the diagnosis and management of COVID-19 patients: An analysis of Electronic Health Records using Natural Language Processing and machine learning. J. Womens Health 2021, 30, 393–404. [Google Scholar] [CrossRef]
- Espinosa-Anke, L.; Tello, J.; Pardo, A.; Medrano, I.; Ureña, A.; Salcedo, I.; Saggion, H. Savana: A Global Information Extraction and Terminology Expansion Framework in the Medical Domain. Proces. Leng. Nat. 2016, 57, 23–30. [Google Scholar]
- Hernandez Medrano, I.; Guijarro, J.T.; Belda, C.; Urena, A.; Salcedo, I.; Espinosa-Anke, L.; Saggion, H. Savana: Re-using Electronic Health Records with Artificial Intelligence. Int. J. Interact. Multimed. Artif. Intell. 2017, 4, 8–12. [Google Scholar] [CrossRef]
- Graziani, D.; Soriano, J.B.; Del Rio-Bermudez, C.; Morena, D.; Díaz, T.; Castillo, M.; Alonso, M.; Ancochea, J.; Lumbreras, S.; Izquierdo, J.L. Characteristics and Prognosis of COVID-19 in Patients with COPD. J. Clin. Med. 2020, 9, 3259. [Google Scholar] [CrossRef]
- Izquierdo, J.; Ancochea, J.; Savana COVID-19 Research Group; Soriano, J. Clinical Characteristics and Prognostic Factors for Intensive Care Unit Admission of Patients With COVID-19: Retrospective Study Using Machine Learning and Natural Language Processing. J. Med. Internet Res. 2020, 22, e21801. [Google Scholar] [CrossRef]
- Bhattacharyya, S.B. Overview of SNOMED CT. In Introduction to SNOMED CT; Springer: Singapore, 2016. [Google Scholar] [CrossRef]
- Canales, L.; Menke, S.; Marchesseau, S.; D’Agostino, A.; Del Rio-Bermudez, C.; Taberna, M.; Tello, J. Assessing the Performance of Clinical Natural Language Processing Systems: Development of an Evaluation Methodology. JMIR Med. Inform. 2021, 9, e20492. [Google Scholar] [CrossRef]
- Catovsky, D.; Wade, R.; Else, M. The clinical significance of patients’ sex in chronic lymphocytic leukemia. Haematologica 2014, 99, 1088–1094. [Google Scholar] [CrossRef]
- Molica, S. Sex differences in incidence and outcome of chronic lymphocytic leukemia patients. Leuk. Lymphoma 2006, 47, 1477–1480. [Google Scholar] [CrossRef]
- Seymour, E.K.; Ruterbusch, J.J.; Beebe-Dimmer, J.L.; Schiffer, C.A. Real-world testing and treatment patterns in chronic lymphocytic leukemia: A SEER patterns of care analysis. Cancer 2019, 125, 135–143. [Google Scholar] [CrossRef]
- Mato, A.; Jahnke, J.; Li, P.; Mehra, M.; Ladage, V.P.; Mahler, M.; Huntington, S.; Doshi, J.A. Real-world treatment and outcomes among older adults with chronic lymphocytic leukemia before the novel agents era. Haematologica 2018, 103, e462–e465. [Google Scholar] [CrossRef] [PubMed]
- Mato, A.; Nabhan, C.; Kay, N.E.; Weiss, M.A.; Lamanna, N.; Kipps, T.J.; Grinblatt, D.L.; Flinn, I.W.; Kozloff, M.F.; Flowers, C.R.; et al. Real-world clinical experience in the Connect® chronic lymphocytic leukaemia registry: A prospective cohort study of 1494 patients across 199 US centres. Br. J. Haematol. 2016, 175, 892–903. [Google Scholar] [CrossRef] [PubMed]
- E.M.A. EPAR Imbruvica. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/imbruvica (accessed on 15 July 2022).
- Miotto, R.; Li, L.; Kidd, B.A.; Dudley, J.T. Deep Patient: An Unsupervised Representation to Predict the Future of Patients from the Electronic Health Records. Sci. Rep. 2016, 6, 26094. [Google Scholar] [CrossRef] [PubMed]
- Zeiberg, D.; Prahlad, T.; Nallamothu, B.K.; Iwashyna, T.J.; Wiens, J.; Sjoding, M.W. Machine learning for patient risk stratification for acute respiratory distress syndrome. PLoS ONE 2019, 14, e0214465. [Google Scholar] [CrossRef]
- Moon, K.A.; Pollak, J.; Hirsch, A.G.; Aucott, J.N.; Nordberg, C.; Heaney, C.D.; Schwartz, B.S. Epidemiology of Lyme disease in Pennsylvania 2006-2014 using electronic health records. Ticks Tick-Borne Dis. 2019, 10, 241–250. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | W&W n = 270 | 1L Treatment n = 230 | R/R 2L Treatment n = 58 |
|---|---|---|---|
| Age (years) | |||
| Median (Q1, Q3) | 75.0 (65.0, 82.0) | 75.0 (67.0, 81.0) | 71.0 (61.5, 76.8) |
| <65 years, n (%) | 65 (24.1) | 46 (20.0) | 19 (32.8) |
| 65–79 years, n (%) | 111 (41.1) | 118 (51.3) | 29 (50.0) |
| ≥80 years, n (%) | 94 (34.8) | 66 (28.7) | 10 (17.2) |
| Sex | |||
| Male, n (%) | 148 (54.8) | 128 (55.7) | 37 (63.8) |
| Female, n (%) | 122 (45.2) | 102 (44.3) | 21 (36.2) |
| Family history of CLL, n (%) † | 10 (3.7) | 31 (13.5) | 8 (13.8) |
| Prior monoclonal B-cell lymphocytosis, n (%) † | 12 (4.4) | 3 (1.3) | 1 (1.7) |
| Comorbidity | W&W n = 270 | 1L Treatment n = 230 | R/R 2L Treatment n = 58 |
|---|---|---|---|
| Cardiovascular, n (%) | 117 (43.3) | 111 (48.3) | 30 (51.7) |
| Hypertension | 96 (35.6) | 88 (38.3) | 23 (39.7) |
| Cardiac arrhythmia | 45 (16.7) | 41 (17.8) | 10 (17.2) |
| Atrial fibrillation | 24 (8.9) | 19 (8.3) | 4 (6.9) |
| Atrial flutter | 5 (1.9) | 4 (1.7) | 2 (3.4) |
| Heart failure | 44 (16.3) | 40 (17.4) | 10 (17.2) |
| Ischemic heart disease | 28 (10.4) | 22 (9.6) | 6 (10.3) |
| Heart valve disorder | 18 (6.7) | 20 (8.7) | 6 (10.3) |
| Gastrointestinal and hepatobiliary, n (%) † | 105 (38.9) | 89 (38.7) | 17 (29.3) |
| Hepatomegaly | 16 (5.9) | 25 (10.9) | 6 (10.3) |
| Hepatitis C | 6 (2.2) | 4 (1.7) | 1 (1.7) |
| Peptic ulcer | 7 (2.6) | 4 (1.7) | 2 (3.4) |
| Hiatal hernia | 7 (2.6) | 9 (3.9) | 1 (1.7) |
| Endocrine, metabolism, and nutrition, n (%) | 82 (30.4) | 70 (30.4) | 23 (39.7) |
| Diabetes mellitus | 66 (24.4) | 56 (24.3) | 18 (31.0) |
| Dyslipidemia ‡ | 37 (13.7) | 43 (18.7) | 11 (19.0) |
| Musculoskeletal and connective tissue, n (%) | 81 (30.0) | 70 (30.4) | 22 (37.9) |
| Rheumatoid arthritis | 19 (7.0) | 19 (8.3) | 4 (6.9) |
| Osteoarthritis | 8 (3.0) | 4 (1.7) | 2 (3.4) |
| Renal and urinary system, n (%) | 42 (15.6) | 33 (14.3) | 7 (12.1) |
| Chronic renal failure | 29 (10.7) | 22 (9.6) | 5 (8.6) |
| Diabetic nephropathy | 4 (1.5) | 0 (0) | 0 (0) |
| Nephrolithiasis | 5 (1.9) | 1 (0.4) | 0 (0) |
| Urinary tract infectious disease | 15 (5.6) | 14 (6.1) | 3 (5.2) |
| Respiratory, n (%) | 26 (9.6) | 28 (12.2) | 3 (5.2) |
| COPD | 15 (5.6) | 18 (7.8) | 0 (0) |
| Bronchial asthma | 14 (5.2) | 12 (5.2) | 3 (5.2) |
| Pulmonary hypertension | 4 (1.5) | 4 (1.7) | 0 (0) |
| Concomitant Medication | W&W n = 270 | 1L Treatment n = 230 | R/R 2L Treatment n = 58 |
|---|---|---|---|
| Antihypertensive and/or antiarrhythmic drugs, n (%) | 80 (29.6) | 103 (44.8) | 18 (31.0) |
| Antithrombotic drugs, n (%) | 79 (29.3) | 98 (42.6) | 16 (27.6) |
| Diuretic drugs, n (%) | 38 (14.1) | 75 (32.6) | 20 (34.5) |
| Lipid-lowering drugs, n (%) | 37 (13.7) | 69 (30.0) | 12 (20.7) |
| Cardiotonic drugs, n (%) | 13 (4.8) | 6 (2.6) | 2 (3.4) |
| Antianginal/vasodilator drugs, n (%) | 8 (3.0) | 19 (8.3) | 5 (8.6) |
| Peripheral vasodilator drugs, n (%) | 1 (0.4) | 2 (0.9) | 0 (0) |
| Antineoplastic Treatments | 1L Treatment n = 230 | R/R 2L Treatment n = 58 |
|---|---|---|
| Ibrutinib, n (%) | 149 (64.8) | 36 (62.1) |
| Bendamustine + rituximab, n (%) | 29 (12.6) | 2 (3.5) |
| Obinutuzumab + chlorambucil, n (%) | 12 (5.2) | 3 (5.2) |
| Chlorambucil + rituximab, n (%) | 11 (4.8) | 1 (1.7) |
| Idelalisib + rituximab, n (%) | 9 (3.9) | 4 (6.9) |
| Fludarabine + cyclophosphamide + rituximab, n (%) | 8 (3.5) | 1 (1.7) |
| Ibrutinib + obinutuzumab, n (%) | 6 (2.6) | - |
| Venetoclax, n (%) | 5 (2.2) | 9 (15.5) |
| Venetoclax + rituximab, n (%) | 1 (0.4) | 2 (3.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loscertales, J.; Abrisqueta-Costa, P.; Gutierrez, A.; Hernández-Rivas, J.Á.; Andreu-Lapiedra, R.; Mora, A.; Leiva-Farré, C.; López-Roda, M.D.; Callejo-Mellén, Á.; Álvarez-García, E.; et al. Real-World Evidence on the Clinical Characteristics and Management of Patients with Chronic Lymphocytic Leukemia in Spain Using Natural Language Processing: The SRealCLL Study. Cancers 2023, 15, 4047. https://doi.org/10.3390/cancers15164047
Loscertales J, Abrisqueta-Costa P, Gutierrez A, Hernández-Rivas JÁ, Andreu-Lapiedra R, Mora A, Leiva-Farré C, López-Roda MD, Callejo-Mellén Á, Álvarez-García E, et al. Real-World Evidence on the Clinical Characteristics and Management of Patients with Chronic Lymphocytic Leukemia in Spain Using Natural Language Processing: The SRealCLL Study. Cancers. 2023; 15(16):4047. https://doi.org/10.3390/cancers15164047
Chicago/Turabian StyleLoscertales, Javier, Pau Abrisqueta-Costa, Antonio Gutierrez, José Ángel Hernández-Rivas, Rafael Andreu-Lapiedra, Alba Mora, Carolina Leiva-Farré, María Dolores López-Roda, Ángel Callejo-Mellén, Esther Álvarez-García, and et al. 2023. "Real-World Evidence on the Clinical Characteristics and Management of Patients with Chronic Lymphocytic Leukemia in Spain Using Natural Language Processing: The SRealCLL Study" Cancers 15, no. 16: 4047. https://doi.org/10.3390/cancers15164047
APA StyleLoscertales, J., Abrisqueta-Costa, P., Gutierrez, A., Hernández-Rivas, J. Á., Andreu-Lapiedra, R., Mora, A., Leiva-Farré, C., López-Roda, M. D., Callejo-Mellén, Á., Álvarez-García, E., & García-Marco, J. A. (2023). Real-World Evidence on the Clinical Characteristics and Management of Patients with Chronic Lymphocytic Leukemia in Spain Using Natural Language Processing: The SRealCLL Study. Cancers, 15(16), 4047. https://doi.org/10.3390/cancers15164047