
Are CT-Derived Muscle Measurements Prognostic, Independent of Systemic Inflammation, in Good Performance Status Patients with Advanced Cancer?


 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
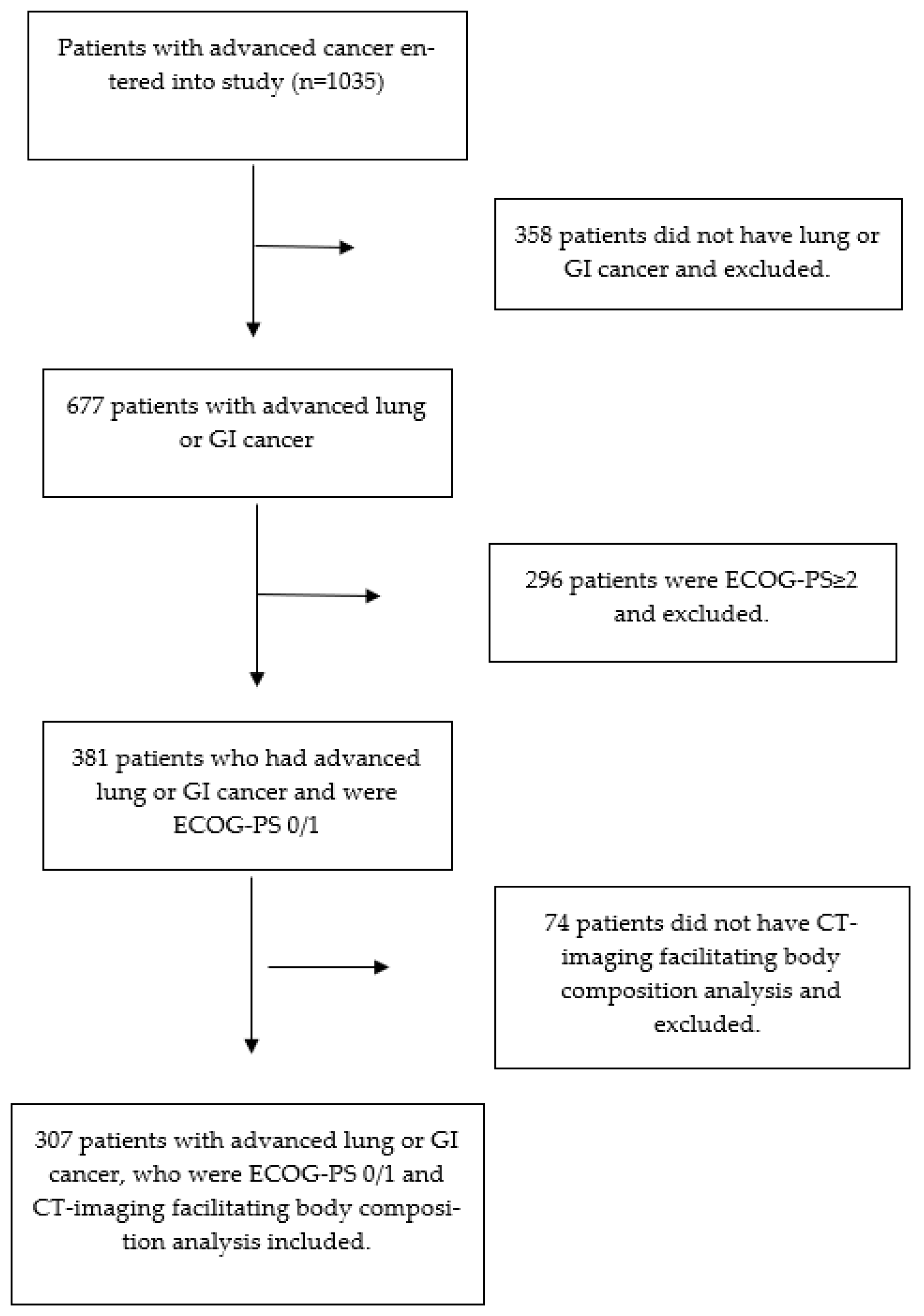
2.1. Patients
2.2. CT-Body Composition Analysis
2.3. Statistical Analysis
3. Results

{kind=link}
| CT-SS 0 | CT-SS 1 | CT-SS 2 | p Value 1 | |
|---|---|---|---|---|
| (n = 189) | (n = 48) | (n = 70) | ||
| Age | 0.042 | |||
| <65 | 105 (56%) | 32 (67%) | 26 (37%) | |
| 65–74 | 56 (30%) | 9 (19%) | 29 (42%) | |
| >74 | 28 (15%) | 7 (15%) | 15 (21%) | |
| Sex | <0.001 | |||
| Female | 55 (29%) | 23 (48%) | 39 (56%) | |
| Male | 134 (71%) | 25 (52%) | 31 (44%) | |
| Cancer Type | 0.431 | |||
| Lung | 60 (32%) | 12 (25%) | 27 (38%) | |
| GI | 129 (68%) | 36 (75%) | 43 (61%) | |
| Metastatic disease | 0.157 | |||
| No | 29 (15%) | 3 (6%) | 7 (10%) | |
| Yes | 160 (85%) | 45 (94%) | 63 (90%) | |
| Chemotherapy | 0.859 | |||
| Yes | 174 (92%) | 44 (92%) | 65 (93%) | |
| No | 15 (8%) | 4 (8%) | 5 (7%) | |
| Radiotherapy | 0.339 | |||
| Yes | 10 (5%) | 3 (6%) | 6 (9%) | |
| No | 179 (95%) | 45 (94%) | 64 (91%) | |
| BMI (kg/m2) | 0.014 | |||
| <25 | 86 (46%) | 21 (44%) | 45 (64%) | |
| ≥25 | 103 (54%) | 27 (56%) | 25 (36%) | |
| Low SMI | <0.001 | |||
| No | 189 (100%) | 0 (0%) | 0 (0%) | |
| Yes | 0 (0%) | 48 (100%) | 70 (100%) | |
| Low SMD | <0.001 | |||
| No | 109 (60%) | 46 (100%) | 0 (0%) | |
| Yes | 72 (40%) | 0 (0%) | 70 (100%) | |
| ECOG-PS | 0.197 | |||
| 0 | 93 (49%) | 26 (54%) | 27 (39%) | |
| 1 | 96 (51%) | 22 (46%) | 43 (61%) | |
| mGPS 2 | 0.058 | |||
| 0 | 78 (55%) | 24 (62%) | 26 (44%) | |
| 1 | 23 (16%) | 3 (8%) | 5 (8%) | |
| 2 | 41 (29%) | 12 (31%) | 28 (48%) | |
| Overall survival | 0.548 | |||
| Yes | 43 (23%) | 12 (25%) | 13 (19%) | |
| No | 146 (77%) | 36 (75%) | 57 (81%) |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Research UK. Cancer Statistics for the UK. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics-for-the-uk#heading-Four (accessed on 23 February 2023).
- Simmons, C.P.; McMillan, D.C.; McWilliams, K.; Sande, T.A.; Fearon, K.C.; Tuck, S.; Fallon, M.T.; Laird, B.J. Prognostic Tools in Patients with Advanced Cancer: A Systematic Review. J. Pain Symptom Manag. 2017, 53, 962–970.e10. [Google Scholar] [CrossRef] [PubMed]
- Abbass, T.; Dolan, R.D.; McMillan, D.C. Computed tomography-derived body composition analysis in patients with advanced cancer: Clinical utility and future research. Curr. Opin. Support. Palliat. Care 2020, 14, 309–315. [Google Scholar] [CrossRef] [PubMed]
- McGovern, J.; Dolan, R.D.; Horgan, P.G.; Laird, B.J.; McMillan, D.C. Computed tomography-defined low skeletal muscle index and density in cancer patients: Observations from a systematic review. J. Cachex Sarcopenia Muscle 2021, 12, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Skipworth, R.J. A tale of two CT studies: The combined impact of multiple human body composition projects in cancer. J. Cachex Sarcopenia Muscle 2019, 10, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Hacker, U.; Hasenclever, D.; Baber, R.; Linder, N.; Busse, H.; Obermannova, R.; Zdrazilova-Dubska, L.; Valik, D.; Lordick, F. Modified Glasgow prognostic score (mGPS) is correlated with sarcopenia and dominates the prognostic role of baseline body composition parameters in advanced gastric and esophagogastric junction cancer patients undergoing first-line treatment from the phase III EXPAND trial. Ann. Oncol. 2022, 33, 685–692. [Google Scholar] [CrossRef]
- Laird, B.J.; Kaasa, S.; McMillan, D.C.; Fallon, M.T.; Hjermstad, M.J.; Fayers, P.; Klepstad, P. Prognostic Factors in Patients with Advanced Cancer: A Comparison of Clinicopathological Factors and the Development of an Inflammation-Based Prognostic System. Clin. Cancer Res. 2013, 19, 5456–5464. [Google Scholar] [CrossRef]
- McGovern, J.; Dolan, R.D.; Skipworth, R.J.; Laird, B.J.; McMillan, D.C. Cancer cachexia: A nutritional or a systemic inflammatory syndrome? Br. J. Cancer 2022, 127, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Dolan, R.D.; Daly, L.E.; Simmons, C.P.; Ryan, A.M.; Sim, W.M.; Fallon, M.; Power, D.G.; Wilcock, A.; Maddocks, M.; Bennett, M.I.; et al. The Relationship between ECOG-PS, mGPS, BMI/WL Grade and Body Composition and Physical Function in Patients with Advanced Cancer. Cancers 2020, 12, 1187. [Google Scholar] [CrossRef]
- Dolan, R.D.; Daly, L.; Sim, W.M.; Fallon, M.; Ryan, A.; McMillan, D.C.; Laird, B.J. Comparison of the prognostic value of ECOG-PS, mGPS and BMI/WL: Implications for a clinically important framework in the assessment and treatment of advanced cancer. Clin. Nutr. 2020, 39, 2889–2895. [Google Scholar] [CrossRef]
- Daly, L.E.; Dolan, R.D.; Power, D.G.; Ní Bhuachalla, É.; Sim, W.; Cushen, S.J.; Fallon, M.; Simmons, C.; McMillan, D.C.; Laird, B.J.; et al. Determinants of quality of life in patients with incurable cancer. Cancer 2020, 126, 2872–2882. [Google Scholar] [CrossRef]
- McMillan, D.C. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc. Nutr. Soc. 2008, 67, 257–262. [Google Scholar] [CrossRef]
- Richards, C.H.; Roxburgh, C.S.D.; MacMillan, M.T.; Isswiasi, S.; Robertson, E.G.; Guthrie, G.K.; Horgan, P.G.; McMillan, D.C. The Relationships between Body Composition and the Systemic Inflammatory Response in Patients with Primary Operable Colorectal Cancer. PLoS ONE 2012, 7, e41883. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; MacDonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer Cachexia in the Age of Obesity: Skeletal Muscle Depletion is a Powerful Prognostic Factor, Independent of Body Mass Index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- McGovern, J.; Delaney, J.; Forshaw, M.J.; McCabe, G.; Crumley, A.B.; McIntosh, D.; Laird, B.J.; Horgan, P.G.; McMillan, D.C.; McSorley, S.T.; et al. The relationship between computed tomography-derived sarcopenia, cardiopulmonary exercise testing performance, systemic inflammation, and survival in good performance status patients with oesophago-gastric cancer undergoing neoadjuvant treatment. JCSM Clin. Rep. 2022, 8, 3–11. [Google Scholar] [CrossRef]
- McGovern, J.; Golder, A.M.; Dolan, R.D.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C. The combination of computed tomography-derived muscle mass and muscle density and relationship with clinicopathological characteristics and survival in patients undergoing potentially curative surgery for colorectal cancer. JCSM Clin. Rep. 2022, 7, 65–76. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E.; Mazurak, V.C.; Bhullar, A.S. Cancer cachexia is defined by an ongoing loss of skeletal muscle mass. Ann. Palliat. Med. 2019, 8, 3–12. [Google Scholar] [CrossRef]
- Arulananda, S.; Segelov, E. Sarcopenia and cancer-related inflammation measurements in advanced gastric and junctional cancers—Ready for prime time? Ann. Oncol. 2022, 33, 669–671. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Vitale, J.; Sconfienza, L.M. Imaging of sarcopenia: Old evidence and new insights. Eur. Radiol. 2020, 30, 2199–2208. [Google Scholar] [CrossRef]
- da Silva, G.A.; Wiegert, E.V.M.; Calixto-Lima, L.; Oliveira, L.C. Clinical utility of the modified Glasgow Prognostic Score to classify cachexia in patients with advanced cancer in palliative care. Clin. Nutr. 2020, 39, 1587–1592. [Google Scholar] [CrossRef]
- Bretscher, C.; Boesiger, F.; Kaegi-Braun, N.; Hersberger, L.; Lobo, D.N.; Evans, D.C.; Tribolet, P.; Gomes, F.; Hoess, C.; Pavlicek, V.; et al. Admission serum albumin concentrations and response to nutritional therapy in hospitalised patients at malnutrition risk: Secondary analysis of a randomised clinical trial. Eclinicalmedicine 2022, 45, 101301. [Google Scholar] [CrossRef] [PubMed]
- Merker, M.; Felder, M.; Gueissaz, L.; Bolliger, R.; Tribolet, P.; Kägi-Braun, N.; Gomes, F.; Hoess, C.; Pavlicek, V.; Bilz, S.; et al. Association of baseline inflammation with effectiveness of nutritional support among patients with disease-related malnutrition: A secondary analysis of a randomized clinical trial. JAMA Netw. Open 2020, 3, e200663. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, F.; Keller, B.; Gressies, C.; Schuetz, P. Inflammation and Nutrition: Friend or Foe? Nutrients 2023, 15, 1159. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Gong, Y.; Roy, P.; King-Kallimanis, B.; Bhatnagar, V.; Pazdur, R.; Kluetz, P.G. FDA analysis of ECOG performance status and safety outcomes. J. Clin. Oncol. 2020, 38, 12024. [Google Scholar] [CrossRef]
- Kouzy, R.; Jaoude, J.A.; Mainwaring, W.; Lin, T.; Miller, A.B.; Jethanandani, A.; Espinoza, A.F.; Taniguchi, C.M.; Ludmir, E.B. Performance status restriction in phase III cancer clinical trials. J. Clin. Oncol. 2020, 38, 2059. [Google Scholar] [CrossRef]
- Yang, F.; Markovic, S.N.; Molina, J.R.; Halfdanarson, T.R.; Pagliaro, L.C.; Chintakuntlawar, A.V.; Li, R.; Wei, J.; Wang, L.; Liu, B.; et al. Association of sex, age, and eastern cooperative oncology group performance status with survival benefit of cancer immunotherapy in randomized clinical trials: A systematic review and meta-analysis. JAMA Netw. Open 2020, 3, e2012534. [Google Scholar] [CrossRef]
- Mojsak, D.; Kuklińska, B.; Minarowski, Ł.; Mróz, R.M. Current state of knowledge on immunotherapy in ECOG PS 2 patients. A systematic review. Adv. Med. Sci. 2021, 66, 381–387. [Google Scholar] [CrossRef]
- Saal, J.; Bald, T.; Eckstein, M.; Ralser, D.J.; Ritter, M.; Brossart, P.; Grünwald, V.; Hölzel, M.; Ellinger, J.; Klümper, N. Integrating On-Treatment Modified Glasgow Prognostic Score and Imaging to Predict Response and Outcomes in Metastatic Renal Cell Carcinoma. JAMA Oncol. 2023; online ahead of print. [Google Scholar] [CrossRef]

| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Hazard Ratio (95% Confidence Interval) | p-Value | Hazard Ratio (95% Confidence Interval) | p-Value | |
| Age (<65/65–74/>74) | 0.88 (0.74–1.05) | 0.146 | - | - |
| Sex (Female/Male) | 0.95 (0.73–1.23) | 0.691 | - | - |
| Cancer type (Lung/GI) | 0.66 (0.50–0.87) | 0.003 | - | 0.119 |
| Metastatic disease (No/Yes) | 1.00 (0.69–1.46) | 0.995 | - | - |
| Chemotherapy (No/Yes) | 0.87 (0.50–1.49) | 0.606 | - | - |
| Radiotherapy (No/Yes) | 1.79 (0.87–3.68) | 0.112 | - | - |
| BMI (<25/≥25, kg/m2) | 0.97 (0.75–1.25) | 0.805 | - | - |
| CT-SS (0/1/2) | 1.06 (0.92–1.24) | 0.421 | - | - |
| ECOG-PS (0/1) | 1.21 (0.94–1.56) | 0.142 | - | - |
| mGPS (0/1/2) | 1.33 (1.13–1.55) | <0.001 | 1.33 (1.13–1.55) | 0.001 |
| mGPS 0 (n = 128) | mGPS 1 (n = 31) | mGPS 2 (n = 81) | p Value 1 | |
|---|---|---|---|---|
| ECOG-PS 0 (n = 146) | CT-SS 0 37 (65%) CT-SS 1 11 (19%) CT-SS 2 9 (16%) | CT-SS 0 11 (73%) CT-SS 1 1 (7%) CT-SS 2 3 (20%) | CT-SS 0 11 (39%) CT-SS 1 6 (21%) CT-SS 2 11 (39%) | 0.016 |
| ECOG-PS 1 (n = 161) | CT-SS 0 41 (57%) CT-SS 1 13 (18%) CT-SS 2 17 (24%) | CT-SS 0 12 (76%) CT-SS 1 2 (12%) CT-SS 2 2 (12%) | CT-SS 0 30 (57%) CT-SS 1 6 (11%) CT-SS 2 17 (32%) | 0.602 |
| p value 1 | 0.286 | 0.739 | 0.251 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGovern, J.; Dolan, R.D.; Simmons, C.; Daly, L.E.; Ryan, A.M.; Power, D.G.; Fallon, M.T.; Laird, B.J.; McMillan, D.C. Are CT-Derived Muscle Measurements Prognostic, Independent of Systemic Inflammation, in Good Performance Status Patients with Advanced Cancer? Cancers 2023, 15, 3497. https://doi.org/10.3390/cancers15133497
McGovern J, Dolan RD, Simmons C, Daly LE, Ryan AM, Power DG, Fallon MT, Laird BJ, McMillan DC. Are CT-Derived Muscle Measurements Prognostic, Independent of Systemic Inflammation, in Good Performance Status Patients with Advanced Cancer? Cancers. 2023; 15(13):3497. https://doi.org/10.3390/cancers15133497
Chicago/Turabian StyleMcGovern, Josh, Ross D. Dolan, Claribel Simmons, Louise E. Daly, Aoife M. Ryan, Derek G. Power, Marie T. Fallon, Barry J. Laird, and Donald C. McMillan. 2023. "Are CT-Derived Muscle Measurements Prognostic, Independent of Systemic Inflammation, in Good Performance Status Patients with Advanced Cancer?" Cancers 15, no. 13: 3497. https://doi.org/10.3390/cancers15133497
APA StyleMcGovern, J., Dolan, R. D., Simmons, C., Daly, L. E., Ryan, A. M., Power, D. G., Fallon, M. T., Laird, B. J., & McMillan, D. C. (2023). Are CT-Derived Muscle Measurements Prognostic, Independent of Systemic Inflammation, in Good Performance Status Patients with Advanced Cancer? Cancers, 15(13), 3497. https://doi.org/10.3390/cancers15133497