
Belantamab Mafodotin in Patients with Relapsed/Refractory Multiple Myeloma: Results of the Compassionate Use or the Expanded Access Program in Spain

 , , , , , , ,
, , , , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods and Patients
Statistical Analysis
3. Results
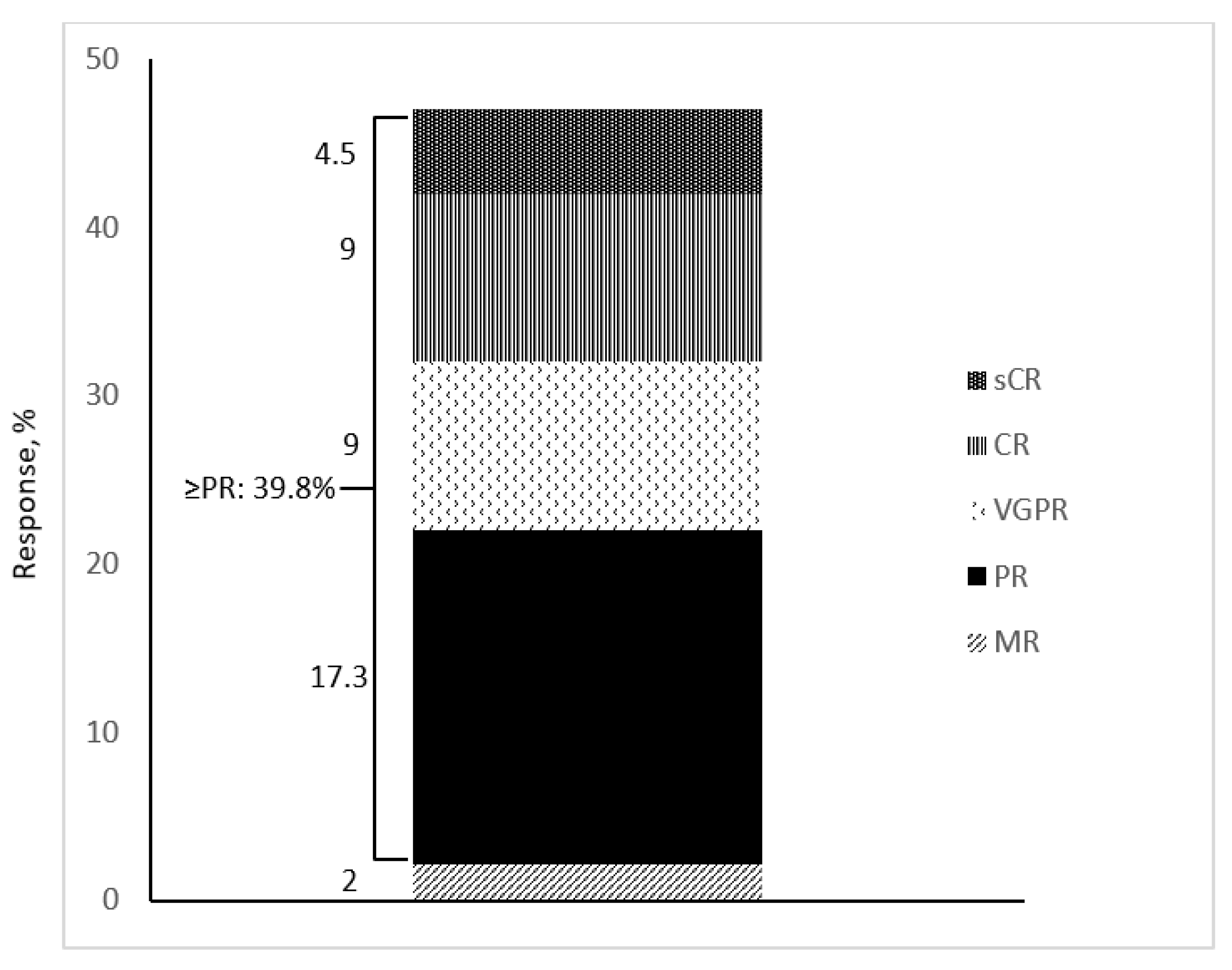
3.1. Efficacy
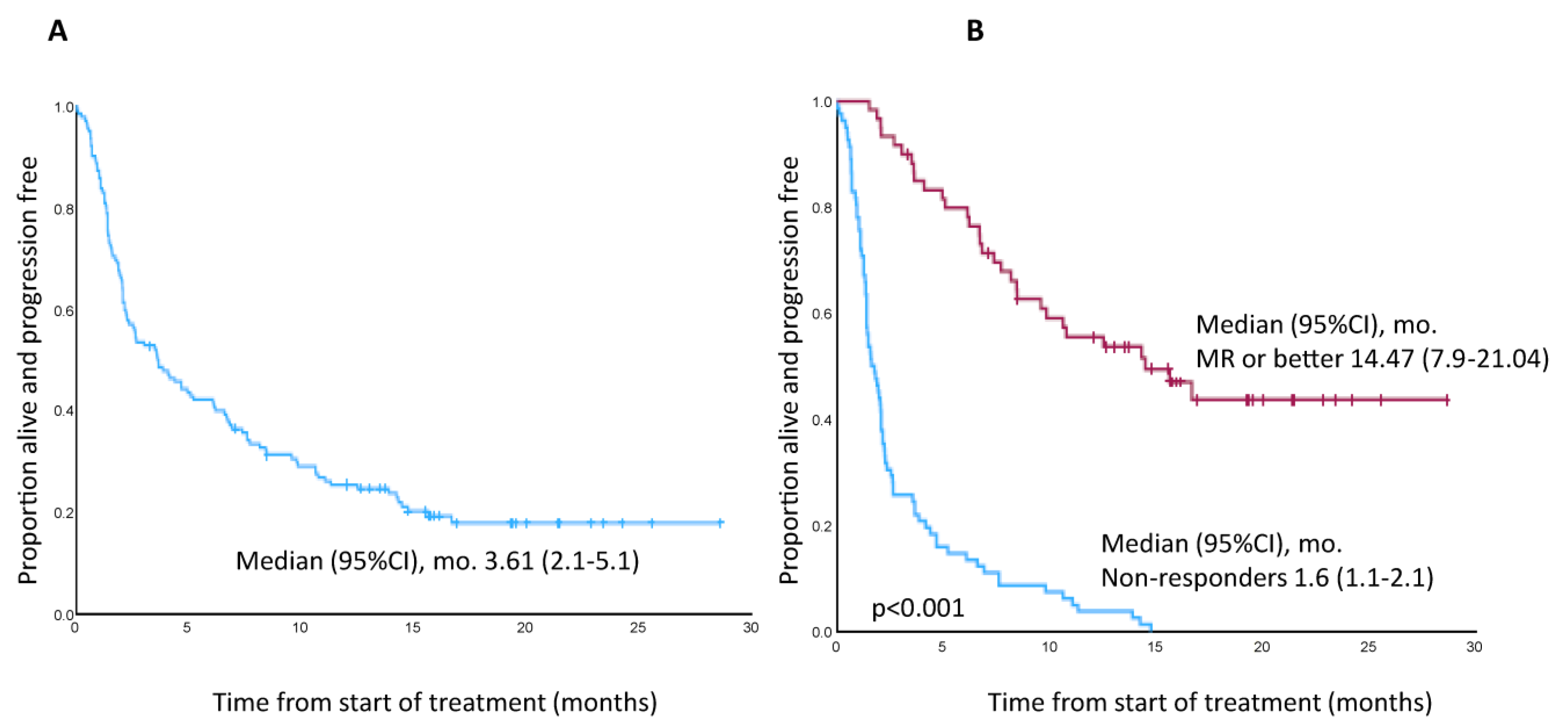
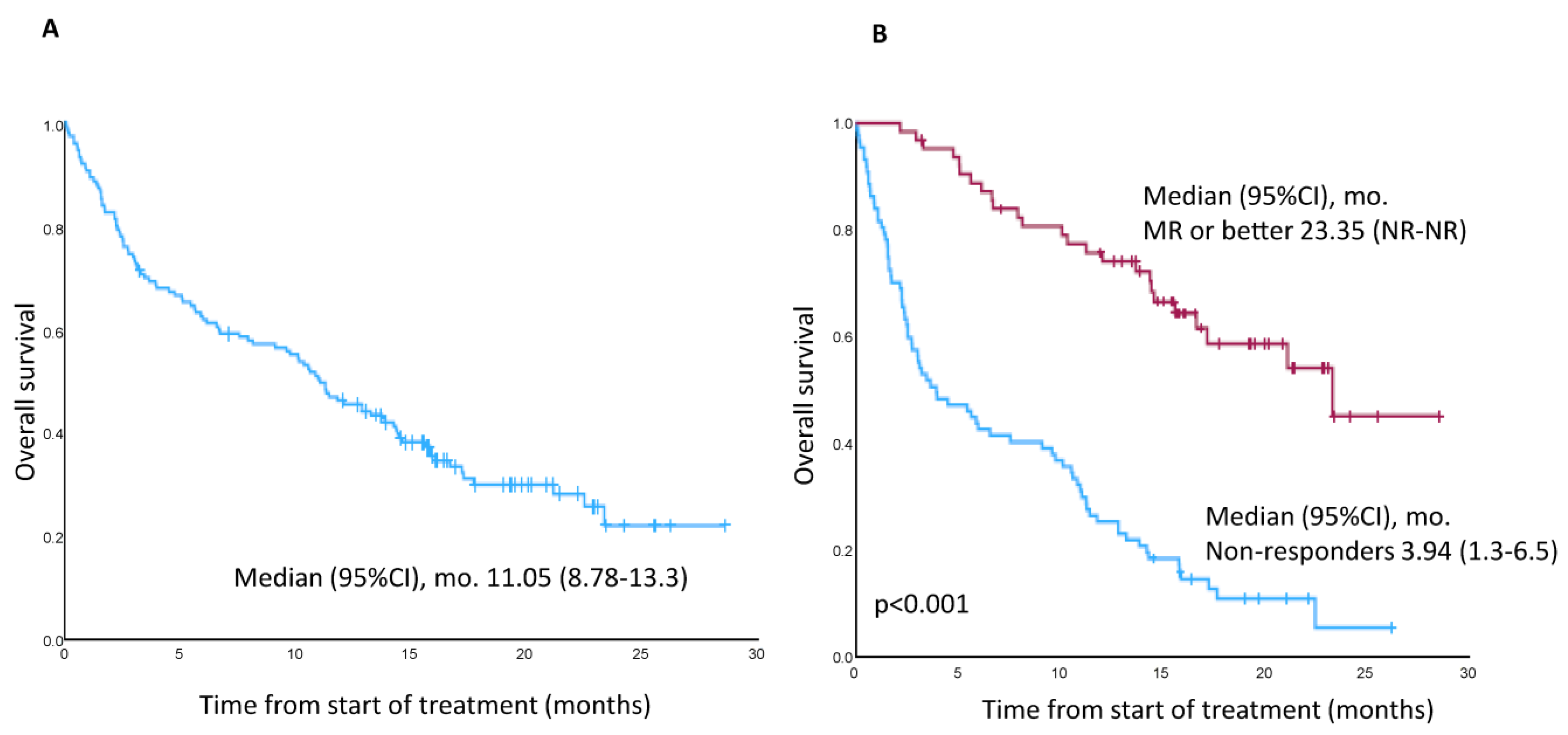
3.2. PFS, DoR, OS, and TTNT
3.3. Safety
3.3.1. Ocular Toxicity
3.3.2. Non-Ocular Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, B.; Wu, C.; Zhong, Q. Belantamab mafodotin for the treatment of multiple myeloma. Drugs Today 2021, 57, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Trudel, S.; Lendvai, N.; Popat, R.; Voorhees, P.M.; Reeves, B.; Libby, E.N.; Richardson, P.G.; Hoos, A.; Gupta, I.; Bragulat, V.; et al. Antibody-drug conjugate, GSK2857916, in relapsed/refractory multiple myeloma: An update on safety and efficacy from dose expansion phase I study. Blood Cancer J. 2019, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Lonial, S.; Lee, H.C.; Badros, A.; Trudel, S.; Nooka, A.K.; Chari, A.; Abdallah, A.O.; Callander, N.; Lendvai, N.; Sborov, D.; et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2) study: A two-arm, randomized, open-label, phase 2 study. Lancet 2020, 21, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Lonial, S.; Lee, H.C.; Badros, A.; Trudel, S.; Nooka, A.K.; Chari, A.; Abdallah, A.O.; Callander, N.; Sborov, D.; Suvannasankha, A.; et al. Long term outcomes with single-agent belantamab mafodotin in patients with relapsed or refractory multiple myeloma: 13-month follow-up from the pivotal DREAMM-2 study. Cancer 2021, 127, 4198–4212. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.J.; Abonour, R.; Gasparetto, C.; Hardin, J.W.; Toomey, K.; Narang, M.; Srinivasan, S.; Kitali, A.; Zafar, F.; Flick, E.D.; et al. Analysis of common eligibility criteria of randomized controlled trials in newly diagnosed multiple myeloma patients and extrapolating outcomes. Clin. Lymphoma Myeloma Leuk. 2017, 17, 575–583.e572. [Google Scholar] [CrossRef] [PubMed]
- Chari, A.; Romanus, D.; Palumbo, A.; Blazer, M.; Farrelly, E.; Raju, A.; Huang, H.; Richardson, P. Randomized clinical trial representativeness and outcomes in real-world patients: Comparison of 6 hallmark randomized clinical trials of relapsed/refractory multiple myeloma. Clin. Lymphoma Myeloma Leuk. 2020, 20, 8–17.e16. [Google Scholar] [CrossRef]
- Fiala, M.A.; Dukeman, J.; Stockerl-Goldstein, K.; Tomasson, M.H.; Wildes, T.M.; Vij, R. The real-world characteristics and outcomes of newly diagnosed myeloma patients ineligible for clinical trials. Clin. Lymphoma Myeloma Leuk. 2017, 17, e55–e56. [Google Scholar] [CrossRef]
- Bergin, K.; McQuilten, Z.; Moore, E.; Wood, E.; Spencer, A. Myeloma in the real world: What is really happening? Clin. Lymphoma Myeloma Leuk. 2017, 17, 133–144.e1. [Google Scholar] [CrossRef]
- Vaxman, I.; Abeykoon, J.; Dispenzieri, A.; Kumar, S.K.; Buadi, F.; Lacy, M.Q.; Dingli, D.; Hwa, Y.; Fonder, A.; Hobbs, M.; et al. “Real-life” data of the efficacy and safety of belantamab mafodotin in relapsed multiple myeloma—The Mayo Clinic experience. Blood Cancer J. 2021, 11, 196. [Google Scholar] [CrossRef]
- Iula, R.; De Novellis, D.; Trastulli, F.; Della Pepa, R.; Fontana, R.; Carobene, A.; Di Perna, M.; D’Ambrosio, A.; Romano, M.; Leone, A.; et al. Efficacy and safety of belantamab mafodotin in triple-refractory multiple myeloma patients. Front. Oncol. 2022, 12, 1026251. [Google Scholar] [CrossRef]
- Shragai, T.; Magen, H.; Lavi, N.; Gatt, M.; Trestman, S.; Zektser, M.; Ganzel, C.; Jarchowsky, O.; Berger, T.; Tadmor, T.; et al. Real-world experience with belantamab mafodotin therapy for relapsed/refractory multiple myeloma: A multicenter retrospective study. Br. J. Haematol. 2022, 200, 45–53. [Google Scholar] [CrossRef]
- Atieh, T.; Atrash, S.; Mohan, M.; Shune, L.; Mahmoudjafari, Z.; Quick, J.; Riffel, J.; McGuirk, J.P.; Mohyuddin, G.R.; Abdallah, A.O.; et al. Belantamab in combination with dexamethasone in patients with triple-class relapsed/refractory multiple myeloma. Blood 2021, 138 (Suppl. S1). [Google Scholar] [CrossRef]
- Roussel, M.; Texier, N.; Germain, R.; Sapra, S.; Paka, P.; Kerbouche, N.; Colin, X.; Leleu, X. Effectiveness and safety of belantamab mafodotin in patients with relapsed or refractory multiple myeloma in real-life setting: The ALFA study. Blood 2022, 140 (Suppl. S1), 1856. [Google Scholar] [CrossRef]
- Offidani, M.; Cavo, M.; Derudas, D.; Di Raimondo, F.; Cuneo, A.; Baldini, L.; Della Pepa, R.; Musso, M.; Boccadoro, M.; Musto, P.; et al. Belantamab mafodotin in patients with relapsed and refractory multiple myeloma who have received at least one proteasome inhibitor, one immunomodulatory agent and one anti-CD38 monoclonal antibody: A retrospective Italian observational study. Blood 2022, 140 (Suppl. S1), 7222–7223. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Orozco, J.; Peterson, T.J.; Derkach, A.; Hassoun, H.; Korde, N.; Lu, S.X.; Mailankody, S.; Patel, D.; Shah, U.A.; et al. Belantamab mafodotin in patients with relapsed/refractory multiple myeloma, a real-world single-center experience. Blood 2022, 140 (Suppl. S1), 3225. [Google Scholar] [CrossRef]
- Kumar, S.; Paiva, B.; Anderson, K.C.; Durie, B.; Landgren, O.; Moreau, P.; Munshi, N.; Lonial, S.; Bladé, J.; Mateos, M.-V.; et al. International myeloma working group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016, 17, e228–e346. [Google Scholar] [CrossRef]
- Talbot, A.; Bobin, A.; Tabone, L.; Lambert, J.; Boccaccio, C.; Deal, C.; Petillon, M.O.; Allangba, O.; Agape, P.; Arnautou, P.; et al. Real-world study of the efficacy and safety of belantamab mafodotin (GSK2857916) in relapsed or refractory multiple myeloma based on data from the nominative ATU in France: IFM 2020-04 study. Haematologica, 2023; ahead of print. [Google Scholar] [CrossRef]
- Masters, J.C.; Nickens, D.J.; Xuan, D.; Shazer, R.L.; Amantea, M. Clinical toxicity of antibody drug conjugates: A meta-analysis of payloads. Investig. New Drugs 2018, 36, 121–135. [Google Scholar] [CrossRef]
- Farooq, A.V.; Degli Esposti, S.; Popat, R.; Thulasi, P.; Lonial, S.; Nooka, A.K.; Jakubowiak, A.; Sborov, D.; Zaugg, B.E.; Badros, A.Z. Corneal epithelial findings in patients with multiple myeloma treated with antibody-drug conjugate belantamab mafodotin in the pivotal, randomized, DREAMM-2 study. Ophthalmol. Ther. 2020, 9, 889–911. [Google Scholar] [CrossRef]
- Abeykoon, J.P.; Vaxman, J.; Patel, S.V.; Kumar, S.; Malave, G.C.; Young, K.S.; Ailawadhi, S.; Larsen, J.T.; Dispenzieri, A.; Muchtar, E.; et al. Impact of belantamab mafodotin-induced ocular toxicity on outcomes of patients with advanced multiple myeloma. Br. J. Haematol. 2022, 199, 95–99. [Google Scholar] [CrossRef]
- Terpos, E.; Kastritis, E.; Gavriatopoulou, M.; Stathopoulos, I.; Malandrakis, P.; Fotiou, D.; Kanellias, N.; Gkolfinopoulos, S.; Manousou, K.; Kastritis, E.; et al. A Phase I/II, Dose and Schedule Evaluation Study to Investigate the Safety and Clinical Activity of Belantamab Mafodotin Administered in Combination with Lenalidomide and Dexamethasone in Transplant-Ineligible NDMM. Blood 2022, 140 (Suppl. S1), 12616–12617. [Google Scholar] [CrossRef]
- Xing, L.; Liu, Y.; Liu, J. Targeting BCMA in Multiple Myeloma: Advances in Antibody-Drug Conjugate Therapy. Cancers 2023, 15, 2240. [Google Scholar] [CrossRef] [PubMed]
- Hultcrantz, M.; Kleinman, D.; Ghataorhe, P.; McKeown, A.; He, W.; Ling, T.; Jewell, R.C.; Byrne, J.; Eliason, L.; Scott, E.C.; et al. Exploring alternative dosing regimens of single-agent belantamab mafodotin on safety and efficacy in patients with relapsed or refractory multiple myeloma: DREAMM-14. Blood 2021, 138 (Suppl. S1), 1645. [Google Scholar] [CrossRef]
- GSK Provides Update on DREAMM-3 Phase III Trial for Blenrep in Relapsed/Refractory Multiple Myeloma. News Release. GSK. 7 November 2022. Available online: https://bit.ly/3FYNEnB (accessed on 8 November 2022).
- Gandhi, U.H.; Cornell, R.F.; Lakshman, A.; Gahvari, Z.J.; McGehee, E.; Jagosky, M.H.; Gupta, R.; Varnado, W.; Fiala, M.A.; Chhabra, S.; et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia 2019, 33, 2266–2675. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Ailawadhi, M.; Dutta, N.; Abdulazeez, M.; Aggarwal, C.S.; Quintero, G.; Baksh, M.; Roy, V.; Sher, T.; Alegria, V.; et al. Trends in early mortality from multiple myeloma: A population-based analysis. Clin. Lymphoma Myeloma Leuk. 2021, 21, e449–e455. [Google Scholar] [CrossRef]
- Robak, P.; Drozdz, I.; Szemraj, J.; Robak, T. Drug resistance in multiple myeloma. Cancer Treat Rev. 2018, 70, 199–208. [Google Scholar] [CrossRef]
- Moreau, P.; Touzeau, C. T-cell-redirecting bispecific antibodies in multiple myeloma: A revolution? Blood 2022, 139, 3681–3687. [Google Scholar] [CrossRef]
- Moreau, P.; Garfall, A.L.; van de Donk, N.W.; Nahi, H.; San-Miguel, J.F.; Oriol, A.; Nooka, A.K.; Martin, T.; Rosinol, L.; Chari, A.; et al. Teclistamab in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2022, 387, 495–505. [Google Scholar] [CrossRef]
- Moreau, P.; van de Donk, N.W.; Delforge, M.; Einsele, H.; De Stefano, V.; Perrot, A.; Besemer, B.; Pawlyn, C.; Karlin, L.; Manier, S.; et al. Comparative Efficacy of Teclistamab Versus Current Treatments in Real-World Clinical Practice in the Prospective LocoMMotion Study in Patients with Triple-Class-Exposed Relapsed and/or Refractory Multiple Myeloma. Adv. Ther. 2023, 40, 2412–2425. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 156 | |
|---|---|---|
| Age at diagnosis, median (IQR) | 70 (64–76.8) | |
| Sex (female), no. (%) | 84 (53.8) | |
| Time from diagnosis, years, median (IQR) | 6.4 (3.7–8.3) | |
| Creatinine clearance (mL/min), no./total no. (%) | ||
| ≥30/<30 | 130 (83.3)/19 (12.2) | |
| Type of MM, no. (%) | ||
| IgG/Non-IgG | 84 (53.9)/72 (46.1) | |
| ECOG performance status score, no./total no. (%) | ||
| 0/≥1 | 34 (21.8)/104 (66.7) | |
| ISS at diagnosis, no./total no. (%) | ||
| I/II/III | 45 (28.8)/49 (31.4)/52 (33.3) | |
| R-ISS at diagnosis, no./total no. (%) | ||
| I/II/III | 33 (21.2)/53 (34.0)/32 (20.5) | |
| EMD, no./total no. (%) | 49 (31.4) | |
| High-risk cytogenetics, no./total no. (%) | ||
| del(17p) | 17/73 (23.3) | |
| t(4;14) | 15/69 (21.7) | |
| t(14;20) | 1/51 (2) | |
| 1q21+ | 28/60 (46.7) | |
| Prior treatments, median (IQR) | 5 (4–6) | |
| Refractory status, no. (%) | ||
| Refractory to ≥1 line of treatment, no. (%) | 146 (93.6%) | |
| To IMiDs | 133 (85.3) | |
| To PI | 131 (84) | |
| To anti-CD38 MoAbs | 129 (82.7) | |
| Triple-refractory | 125 (80.1) | |
| Penta-refractory | 54 (34.6) | |
| Refractory to last line of therapy | 123 (83.1) | |
| Previous HSCT, no. (%) | 101 (64.7) a | |
| Subgroup, No. | ORR, % | PFS (95% CI), mo. | OS (95% CI), mo. | |
|---|---|---|---|---|
| Refractoriness | ||||
| Triple-refractory, 125 | 60.8 | 2.6 (1.5–3.8) | 10.62 (7.4–13.8) | |
| Non-triple refractory, 23 | 69.6 | 6.9 (1.1–12.6) | 11.4 (8.2–14.7) | |
| Penta-refractory, 54 | 62.8 | 2.2 (0.5–3.8) | 9.77 (0.6–18.8) | |
| Non-penta refractory, 94 | 61.1 | 4.9 (2.3–7.4) | 11.05 (9.4–12.6) | |
| Age | ||||
| ≤70 years, 71 | 62 | 2.6 (0.7–4.5) | 10.01 (5.4–14.7) | |
| >70 years, 83 | 62.7 | 3.6 (1.9–5.3) | 12.07 (9.1–14.9) | |
| CrCl | ||||
| <30 mL/min, 17 | 41.2 | 2.07 (1.7–2.3) | 5.09 (0–21.1) | |
| ≥30 mL/min, 130 | 43.8 | 4.1 (2.7–5.5) | 11.05 (8.7–13.3) | |
| EMD | ||||
| No, 106 | 44.3 | 4.67 (2.4–6.8) | 13.2 (10.3–16.1) | |
| Yes, 49 | 37.5 | 2.1 (1.3–2.8) | 4.7 (0–10.3) | |
| All Grades, No. (%) | ≥Grade 3, No. (%) | ||
|---|---|---|---|
| Hematologic | |||
| Thrombocytopenia | 24 (15.4) | 17 (10.9) | |
| Neutropenia | 7 (3.8) | 5 (3.1) | |
| Anemia | 6 (3.9) | 2 (1.3) | |
| Non-hematologic | |||
| Infections | 25 (15) | 10 (5.6) | |
| Gastrointestinal | 9 (5.8) | 2 (1.2) | |
| Hepatobiliary | 8 (5.1) | 3 (1.8) | |
| Neurological | 6 (3.9) | 2 (1.2) | |
| Fatigue | 5 (3.2) | 0 | |
| Cardiac & Vascular | 5 (3.2) | 1 (0.6) | |
| Respiratory | 4 (2.4) | 2 (1.2) | |
| Metabolic | 3 (1.9) | 0 | |
| Renal | 3 (1.9) | 2 (1.2) | |
| Other | 10 (6.2) | 1 (0.6) | |
| Ocular a | |||
| Corneal events | 73 (87.9) | 28 (33.7) | |
| Reduced visual acuity | 50 (60.2) | 7 (8.4) | |
| Blurry vision | 31 (37.3) | 0 | |
| Dry eye | 27 (32.5) | 0 | |
| Foreign body sensation | 16 (19.2) | 0 | |
| Ocular discomfort | 15 (18.1) | 0 | |
| Photophobia | 10 (12) | 0 | |
| Other | 7 (8.4) | 0 | |
| Author, Year | No. of Patients | Age, Years (Range) | No. of Lines (Range) | Triple-ref, % | Penta-refr, % | ORR, % a | ≥PR, % | PFS (95% CI), mo. | DoR (95% CI), mo. | OS (95% CI), mo. |
|---|---|---|---|---|---|---|---|---|---|---|
| Lonial, 2020 [3] | 97 | 65 (60–70) | 7 (3–21) | 100 | NA | 35 | 31 b | 2.8 (1.6–3.6) | 11 (4.2–NR) | 13.7 (9.9–NR) |
| Vaxman, 2021 [9] | 36 | 61 (37–83) | 8 (7–11) | 100 | 100 | NA | 33 | 2 (NA) | NA | 6.5 (NA) |
| Iula, 2022 [10] | 28 | 67.5 (51–83) | 6 (3–14) | 100 | NA | NA | 40 | 3 (0–23)c | NR (2–23) | 8 (0–23) |
| Shragai, 2022 [11] | 106 | 69.4 (36.3–80) | 6 (2–11) | 72.6 | 32 | NA | 45.5 | 4.7 (3.5–5.9) | 8.1 (5.7–10.5) | 14.5 (9.5–19.6) |
| Atieh, 2021 12] | 28 | 67 (24–85) | 5 (3–15) | 100 | 54 | 46 | 46 | 4.9 (NA) | NA | 7.4 (NA) |
| Rousell, 2022 [13] | 184 | 70.3 (63.3–75.9) | 5 (2->5) | NA | NA | 36.4 | 32.7 | 2.4 (1.9–3.2) | NA | 8.8 (6.3–11.6) |
| Offidani, 2022 [14] | 67 | 66 (42–82) | 5 (2–10) | NA | NA | 37 | 31 | 3.7 (NA) | 13.8 (NA) | 12.9 (NA) |
| Hultcrantz, 2022 [15] | 90 | 66 (37–88) | 6 (2–14) | NA | NA | 63 d | 42 | 4 (NA) | 13.1 (NA) | 20.5 (NA) |
| Talbot, 2023 [17] | 106 | 66 (37–82) | 5 (3–12) | 56.7 | 11.3 | 38.1 | NA | 3.5 (1.9–4.7) | 9 (4.65–10.4) c | 9.3 (5.9.15.3) |
| This series, 2023 | 156 | 72.5 (40–89) | 5 (2–10) | 80.1 | 34.6 | 41.8 | 39.8 | 3.6 (2.1–5.1) | 13.9 (8.3–19.4) | 11.05 (8.7–13.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Rubia, J.; Alonso, R.; Clavero, M.E.; Askari, E.; García, A.; Antón, C.; Fernández, M.; Escalante, F.; García, A.; Rios-Tamayo, R.; et al. Belantamab Mafodotin in Patients with Relapsed/Refractory Multiple Myeloma: Results of the Compassionate Use or the Expanded Access Program in Spain. Cancers 2023, 15, 2964. https://doi.org/10.3390/cancers15112964
de la Rubia J, Alonso R, Clavero ME, Askari E, García A, Antón C, Fernández M, Escalante F, García A, Rios-Tamayo R, et al. Belantamab Mafodotin in Patients with Relapsed/Refractory Multiple Myeloma: Results of the Compassionate Use or the Expanded Access Program in Spain. Cancers. 2023; 15(11):2964. https://doi.org/10.3390/cancers15112964
Chicago/Turabian Stylede la Rubia, Javier, Rafael Alonso, María Esther Clavero, Elham Askari, Alfonso García, Cristina Antón, Margarita Fernández, Fernando Escalante, Ana García, Rafael Rios-Tamayo, and et al. 2023. "Belantamab Mafodotin in Patients with Relapsed/Refractory Multiple Myeloma: Results of the Compassionate Use or the Expanded Access Program in Spain" Cancers 15, no. 11: 2964. https://doi.org/10.3390/cancers15112964
APA Stylede la Rubia, J., Alonso, R., Clavero, M. E., Askari, E., García, A., Antón, C., Fernández, M., Escalante, F., García, A., Rios-Tamayo, R., Conesa, V., Bermúdez, M. A., Merchán, B., Velasco, A. E., Blanchard, M. J., Sampol, A., Gainza, E., Hernández, P. M., & Alegre, A. (2023). Belantamab Mafodotin in Patients with Relapsed/Refractory Multiple Myeloma: Results of the Compassionate Use or the Expanded Access Program in Spain. Cancers, 15(11), 2964. https://doi.org/10.3390/cancers15112964