

Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial
 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
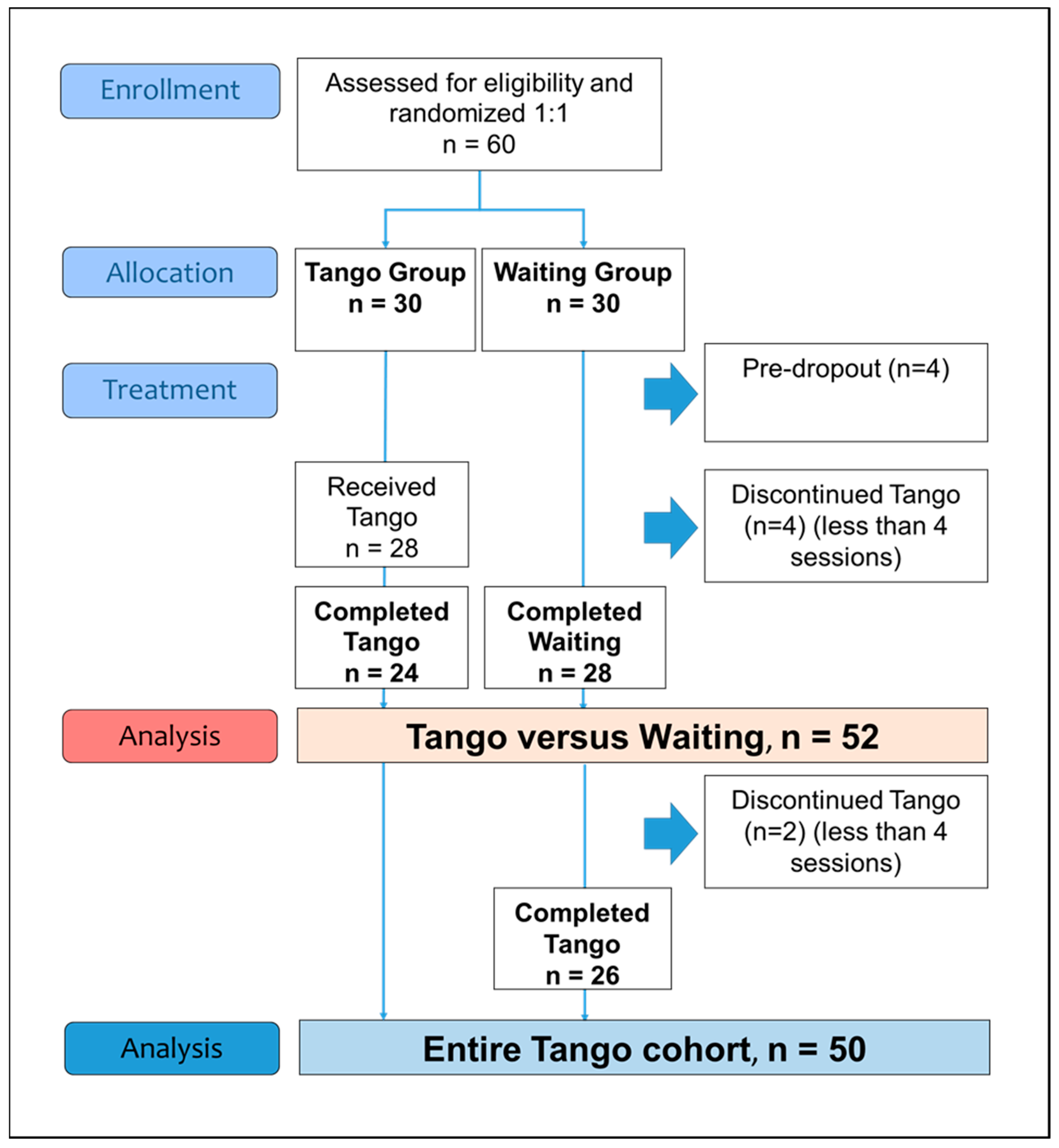
2.1. Participants, Study Design, and Procedure
2.2. Intervention
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
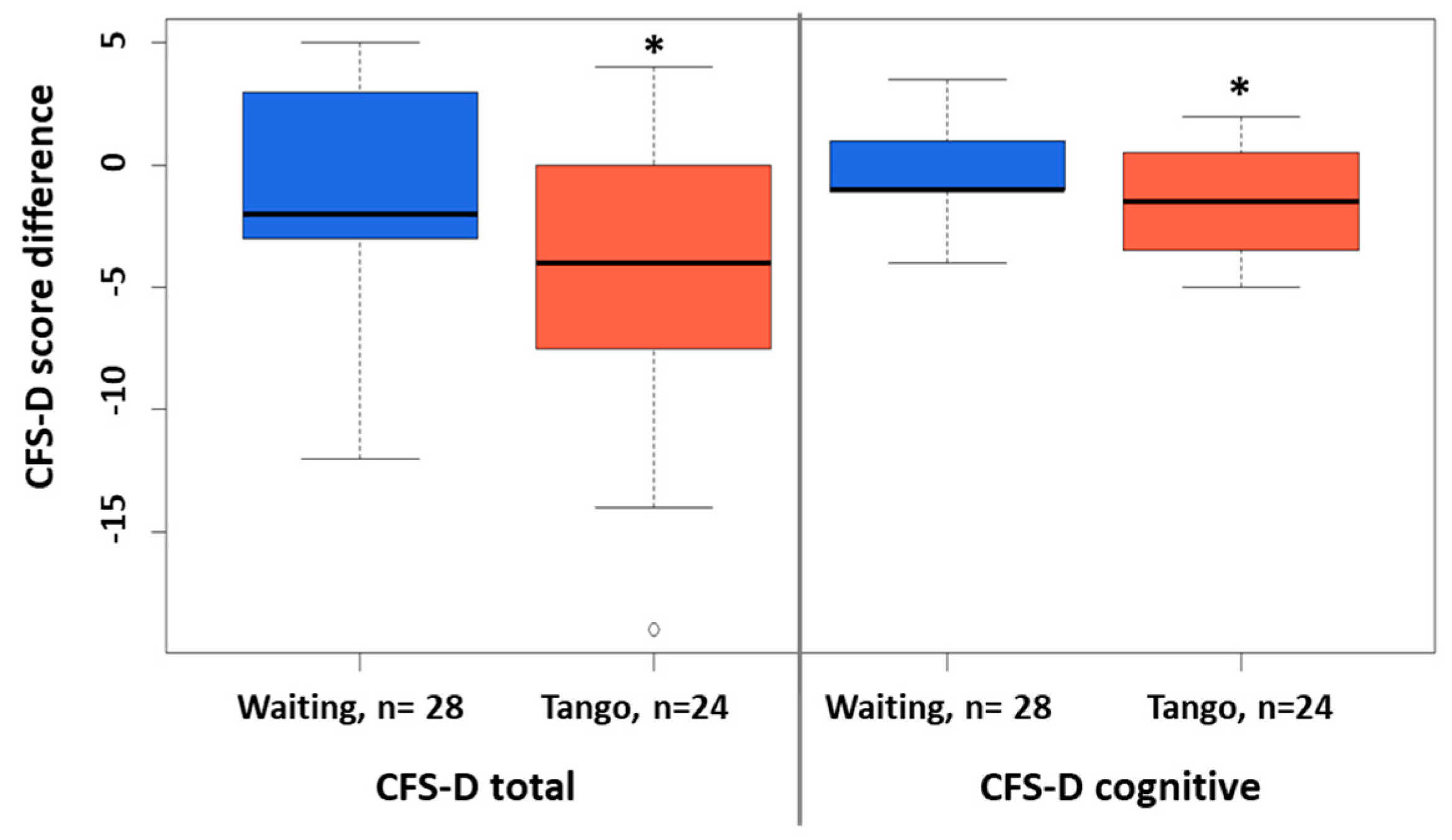
3.1. Group Comparisons
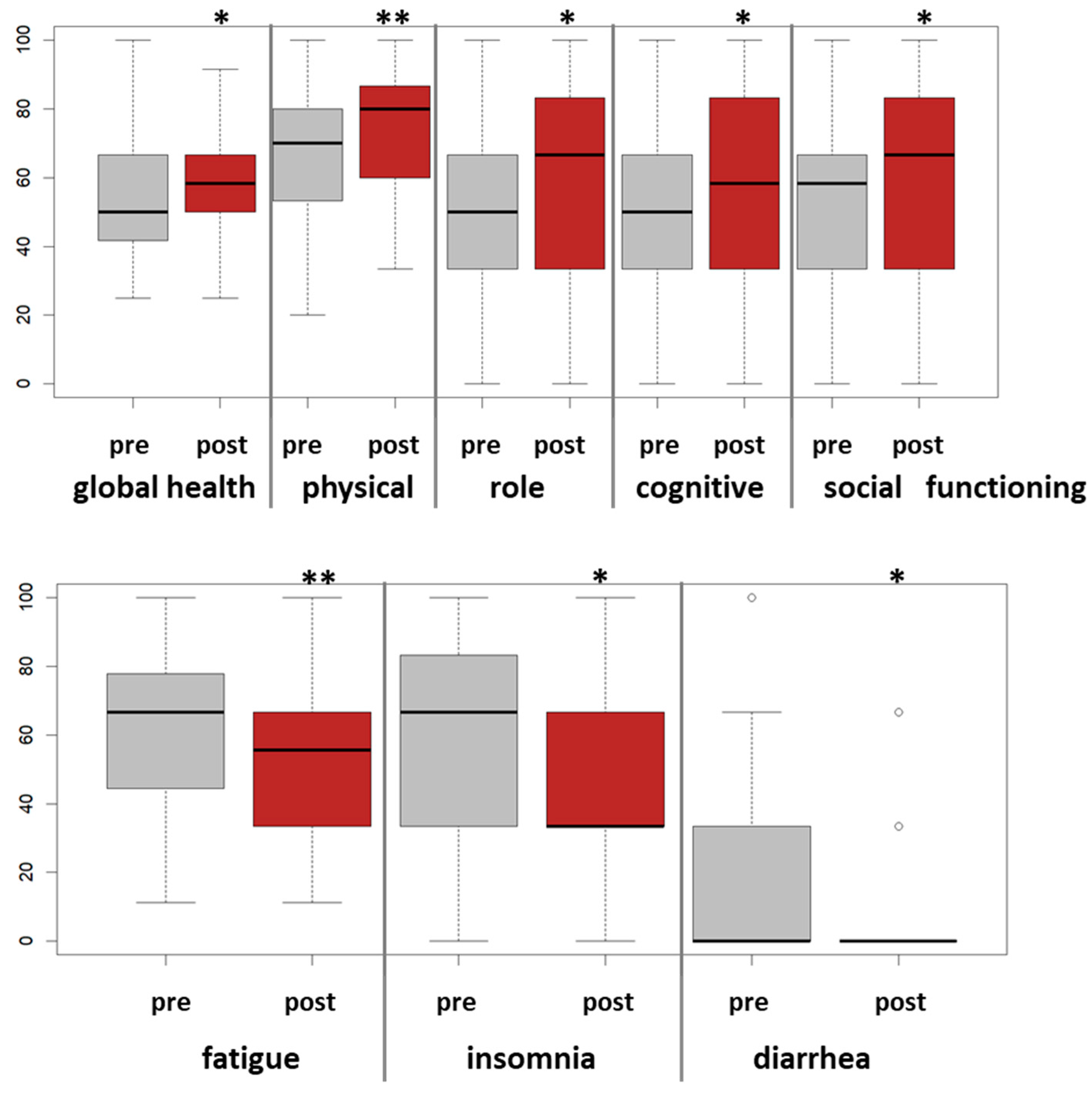
3.2. Pre-Postanalyses
3.3. Safety and Dropout
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Bower, J.E.; Ganz, P.A.; Desmond, K.A.; Bernaards, C.; Rowland, J.H.; Meyerowitz, B.E.; Belin, T.R. Fatigue in long-term breast carcinoma survivors: A longitudinal investigation. Cancer 2006, 106, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Falcicchio, C.; Giannarelli, D.; Maggi, G.; Cognetti, F.; Pugliese, P. The course of cancer related fatigue up to ten years in early breast cancer patients: What impact in clinical practice? Breast 2017, 34, 44–52. [Google Scholar] [CrossRef]
- Cella, D.; Peterman, A.; Passik, S.; Jacobsen, P.; Breitbart, W. Progress toward guidelines for the management of fatigue. Oncology 1998, 12, 369–377. [Google Scholar] [PubMed]
- Bower, J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef]
- Abrahams, H.J.G.; Gielissen, M.F.M.; Schmits, I.C.; Verhagen, C.; Rovers, M.M.; Knoop, H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: A meta-analysis involving 12 327 breast cancer survivors. Ann. Oncol. 2016, 27, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity for women with breast cancer after adjuvant therapy. Cochrane Database Syst. Rev. 2018, 1, CD011292. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari-Hessari, P.; Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual. Life Outcomes 2020, 18, 338. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Torres, D.M.; Koifman, R.J.; Santos, S.D.S. Impact on fatigue of different types of physical exercise during adjuvant chemotherapy and radiotherapy in breast cancer: Systematic review and meta-analysis. Support. Care Cancer Care Cancer 2022, 30, 4651–4662. [Google Scholar] [CrossRef]
- Greenlee, H.; DuPont-Reyes, M.J.; Rn, L.G.B.; Carlson, L.E.; Cohen, M.R.; Deng, G.; Johnson, J.A.; Mumber, M.; Seely, D.; Zick, S.M.; et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J. Clin. 2017, 67, 194–232. [Google Scholar] [CrossRef]
- Bradt, J.; Dileo, C.; Magill, L.; Teague, A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 2016, 8, CD006911. [Google Scholar] [CrossRef] [PubMed]
- Sturm, I.; Baak, J.; Storek, B.; Traore, A.; Thuss-Patience, P. Effect of dance on cancer-related fatigue and quality of life. Support. Care Cancer 2014, 22, 2241–2249. [Google Scholar] [CrossRef]
- Cillessen, L.; Johannsen, M.; Speckens, A.E.; Zachariae, R. Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and survivors: A systematic review and meta-analysis of randomized controlled trials. Psycho-Oncology 2019, 28, 2257–2269. [Google Scholar] [CrossRef]
- Sun, H.; Huang, H.; Ji, S.; Chen, X.; Xu, Y.; Zhu, F.; Wu, J. The Efficacy of Cognitive Behavioral Therapy to Treat Depression and Anxiety and Improve Quality of Life Among Early-Stage Breast Cancer Patients. Integr. Cancer Ther. 2019, 18, 1534735419829573. [Google Scholar] [CrossRef] [PubMed]
- Xunlin, N.; Lau, Y.; Klainin-Yobas, P. The effectiveness of mindfulness-based interventions among cancer patients and survivors: A systematic review and meta-analysis. Support. Care Cancer 2020, 28, 1563–1578. [Google Scholar] [CrossRef] [PubMed]
- Kaltsatou, A.; Mameletzi, D.; Douka, S. Physical and psychological benefits of a 24-week traditional dance program in breast cancer survivors. J. Bodyw. Mov. Ther. 2011, 15, 162–167. [Google Scholar] [CrossRef]
- Koch, S.C.; Riege, R.F.F.; Tisborn, K.; Biondo, J.; Martin, L.; Beelmann, A. Effects of Dance Movement Therapy and Dance on Health-Related Psychological Outcomes. A Meta-Analysis Update. Front. Psychol. 2019, 10, 1806. [Google Scholar] [CrossRef]
- Frikkel, J.; Götte, M.; Beckmann, M.; Kasper, S.; Hense, J.; Teufel, M.; Schuler, M.; Tewes, M. Fatigue, barriers to physical activity and predictors for motivation to exercise in advanced Cancer patients. BMC Palliat. Care 2020, 19, 43. [Google Scholar] [CrossRef]
- Hohmann, L.; Bradt, J.; Stegemann, T.; Koelsch, S. Effects of music therapy and music-based interventions in the treatment of substance use disorders: A systematic review. PLoS ONE 2017, 12, e0187363. [Google Scholar] [CrossRef]
- Karkou, V.; Dudley-Swarbrick, I.; Starkey, J.; Parsons, A.; Aithal, S.; Omylinska-Thurston, J.; Verkooijen, H.M.; Boogaard, R.v.D.; Dochevska, Y.; Djobova, S.; et al. Dancing with Health: Quality of Life and Physical Improvements from an EU Collaborative Dance Programme with Women Following Breast Cancer Treatment. Front. Psychol. 2021, 12, 635578. [Google Scholar] [CrossRef] [PubMed]
- Lötzke, D.; Ostermann, T.; Büssing, A. Argentine tango in Parkinson disease—A systematic review and meta-analysis. BMC Neurol. 2015, 15, 226. [Google Scholar] [CrossRef] [PubMed]
- Worthen-Chaudhari, L.; Lamantia, M.; Monfort, S.; Mysiw, W.; Chaudhari, A.; Lustberg, M. Partnered, adapted argentine tango dance for cancer survivors: A feasibility study and pilot study of efficacy. Clin. Biomech. 2019, 70, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Oei, S.L.; Rieser, T.; Becker, S.; Groß, J.; Matthes, H.; Schad, F.; Thronicke, A. TANGO: Effect of tango Argentino on cancer-associated fatigue in breast cancer patients—Study protocol for a randomized controlled trial. Trials 2021, 22, 866. [Google Scholar] [CrossRef]
- Kröz, M.; Zerm, R.; Reif, M.; VON Laue, H.; Schad, F.; Büssing, A.; Bartsch, C.; Feder, G.; Girke, M. Validation of the German version of the Cancer Fatigue Scale (CFS-D). Eur. J. Cancer Care 2008, 17, 33–41. [Google Scholar] [CrossRef]
- Twomey, R.; Yeung, S.T.; Wrightson, J.G.; Millet, G.Y.; Culos-Reed, S.N. Post-exertional Malaise in People with Chronic Cancer-Related Fatigue. J. Pain Symptom Manag. 2020, 60, 407–416. [Google Scholar] [CrossRef]
- Hackney, M.E.; Earhart, G.M. Recommendations for Implementing Tango Classes for Persons with Parkinson Disease. Am. J. Dance Ther. 2010, 32, 41–52. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; De Haes, J.C.J.M.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. JNCI J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Twomey, R.; Yeung, S.; Wrightson, J.G.; Sung, L.; Robinson, P.D.; Millet, G.Y.; Culos-Reed, S.N. Physical Activity in Adults With Fatigue After Cancer Treatment. Commun. Kinesiol. 2021, 1, 1–20. [Google Scholar] [CrossRef]
- Van Vulpen, J.K.; Sweegers, M.G.; Peeters, P.H.M.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.B.; Galvão, D.A.; Chinapaw, M.J.; Steindorf, K.; et al. Moderators of Exercise Effects on Cancer-related Fatigue: A Meta-analysis of Individual Patient Data. Med. Sci. Sports Exerc. 2020, 52, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Simard, S.; Ivers, H.; Morin, C.M. Randomized Study on the Efficacy of Cognitive-Behavioral Therapy for Insomnia Secondary to Breast Cancer, Part I: Sleep and Psychological Effects. J. Clin. Oncol. 2005, 23, 6083–6096. [Google Scholar] [CrossRef] [PubMed]
- Boing, L.; Fretta, T.D.B.; Lynch, B.M.; Dias, M.; da Rosa, L.M.; Baptista, F.; Bergmann, A.; Fausto, D.Y.; Martins, J.B.B.; Guimarães, A.C.D.A. Mat Pilates and belly dance: Effects on patient-reported outcomes among breast cancer survivors receiving hormone therapy and adherence to exercise. Complement. Ther. Clin. Pr. 2023, 50, 101683. [Google Scholar] [CrossRef]
- Cruz, E.I.d.S.; Cruz, A.H.D.S.; Ventura, J.A.; Marques, R.A.S.; Santos, R.D.S.; Reis, A.A.D.S. The impact of dance as a non-pharmacological adjuvant therapy cancer survivors: A clinical trial. Res. Soc. Dev. 2022, 11, e14411729714. [Google Scholar] [CrossRef]
- Peterson, L.L.; Ligibel, J.A. Physical Activity and Breast Cancer: An Opportunity to Improve Outcomes. Curr. Oncol. Rep. 2018, 20, 50. [Google Scholar] [CrossRef] [PubMed]
- Van Dijck, S.; Nelissen, P.; Verbelen, H.; Tjalma, W.; Gebruers, N. The effects of physical self-management on quality of life in breast cancer patients: A systematic review. Breast 2016, 28, 20–28. [Google Scholar] [CrossRef]
- Lipsett, A.; Barrett, S.; Haruna, F.; Mustian, K.; O’Donovan, A. The impact of exercise during adjuvant radiotherapy for breast cancer on fatigue and quality of life: A systematic review and meta-analysis. Breast 2017, 32, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Fabi, A.; Bhargava, R.; Fatigoni, S.; Guglielmo, M.; Horneber, M.; Roila, F.; Weis, J.; Jordan, K.; Ripamonti, C. Cancer-related fatigue: ESMO Clinical Practice Guidelines for diagnosis and treatment. Ann. Oncol. 2020, 31, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Greenlee, H.; Bohlke, K.; Bao, T.; DeMichele, A.M.; Deng, G.E.; Fouladbakhsh, J.M.; Gil, B.; Hershman, D.L.; Mansfield, S.; et al. Integrative Therapies During and After Breast Cancer Treatment: ASCO Endorsement of the SIO Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 2647–2655. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Pan, H.; Godwin, J.; Gray, R.; Arriagada, R.; Raina, V.; Abraham, M.; Medeiros Alencar, V.H.; Badran, A.; Bonfill, X.; et al. Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 2013, 381, 805–816. [Google Scholar] [CrossRef]
- Mausbach, B.T.; Schwab, R.B.; Irwin, S.A. Depression as a predictor of adherence to adjuvant endocrine therapy (AET) in women with breast cancer: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2015, 152, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Schilder, C.M.T.; Seynaeve, C.; Linn, S.C.; Boogerd, W.; Beex, L.V.A.M.; Gundy, C.M.; Nortier, J.W.R.; Van De Velde, C.J.H.; Van Dam, F.S.A.M.; Schagen, S.B. Self-reported cognitive functioning in postmenopausal breast cancer patients before and during endocrine treatment: Findings from the neuropsychological TEAM side-study. Psycho-Oncology 2012, 21, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Haggstrom, L.R.; Vardy, J.L.; Carson, E.-K.; Segara, D.; Lim, E.; Kiely, B.E. Effects of Endocrine Therapy on Cognitive Function in Patients with Breast Cancer: A Comprehensive Review. Cancers 2022, 14, 920. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Shao, T.; Kushi, L.H.; Buono, D.; Tsai, W.Y.; Fehrenbacher, L.; Kwan, M.; Gomez, S.L.; Neugut, A.I. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res. Treat. 2011, 126, 529–537. [Google Scholar] [CrossRef]
- Joly, F.; Lange, M.; Dos Santos, M.; Vaz-Luis, I.; Di Meglio, A. Long-Term Fatigue and Cognitive Disorders in Breast Cancer Survivors. Cancers 2019, 11, 1896. [Google Scholar] [CrossRef]
- Oberste, M.; Schaffrath, N.; Schmidt, K.; Bloch, W.; Jäger, E.; Steindorf, K.; Hartig, P.; Joisten, N.; Zimmer, P. Protocol for the “Chemobrain in Motion—Study” (CIM—Study): A randomized placebo-controlled trial of the impact of a high-intensity interval endurance training on cancer related cognitive impairments in women with breast cancer receiving first-line chemotherapy. BMC Cancer 2018, 18, 1071. [Google Scholar] [CrossRef]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; De Ruiter, M.; Castel, H. Cancer-related cognitive impairment: An update on state of the art, detection, and management strategies in cancer survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef]
- Oei, S.L.; Thronicke, A.; Kröz, M.; von Trott, P.; Schad, F.; Matthes, H. Impact of Oncological Therapy and Viscum album L Treatment on Cancer-Related Fatigue and Internal Coherence in Nonmetastasized Breast Cancer Patients. Integr. Cancer Ther. 2020, 19, 1534735420917211. [Google Scholar] [CrossRef]
- Witkoś, J.; Hartman-Petrycka, M. Implications of Argentine Tango for Health Promotion, Physical Well-Being as Well as Emotional, Personal and Social Life on a Group of Women Who Dance. Int. J. Environ. Res. Public Health 2021, 18, 5894. [Google Scholar] [CrossRef]
- Sodergren, S.C.; Copson, E.; White, A.; Efficace, F.; Sprangers, M.; Fitzsimmons, D.; Bottomley, A.; Johnson, C.D. Systematic Review of the Side Effects Associated with Anti-HER2-Targeted Therapies Used in the Treatment of Breast Cancer, on Behalf of the EORTC Quality of Life Group. Target. Oncol. 2016, 11, 277–292. [Google Scholar] [CrossRef]
- McKee, K.E.; Hackney, M.E. The Effects of Adapted Tango on Spatial Cognition and Disease Severity in Parkinson’s Disease. J. Mot. Behav. 2013, 45, 519–529. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | Waiting | Tango | p-Value | |
|---|---|---|---|---|
| Number of patients, n (%) | 60 (100) | 30 (100) | 30 (100) | |
| Age, years, mean (SD) | 60.5 (10.3) | 59.3 (11.0) | 61.7 (9.4) | 0.377 |
| Body mass index (BMI) | ||||
| Normal (18.5 ≤ BMI < 25) | 39 (65) | 21 (70) | 18 (60) | |
| Overweight (25 ≤ BMI < 30) | 13 (22) | 6 (20) | 7 (23) | 0.668 |
| Obese (BMI ≥ 30) | 8 (13) | 3 (10) | 5 (17) | |
| Currently employed, n (%) | 23 (38) | 12 (40) | 11 (37) | 1 |
| Living in partnership, n (%) | 39 (65) | 19 (63) | 20 (67) | 1 |
| Years since first diagnosis: mean (SD) | 1.7 (0.7) | 1.7 (0.7) | 1.6 (0.6) | 0.614 |
| UICC stages, n (%) | ||||
| I | 28 (47) | 12 (40) | 16 (53) | |
| II | 23 (38) | 14 (47) | 9 (30) | 0.413 |
| III | 9 (15) | 4 (13) | 5 (17) | |
| Hormonal status, n (%) | ||||
| Premenopausal | 3 (5) | 3 (10) | 0 | |
| Postmenopausal | 57 (95) | 27 (90) | 30 (100) | 0.236 |
| Triple-negative status, n (%) | 6 (10) | 2 (7) | 4 (13) | 0.667 |
| Oncological Interventions, n (%) | ||||
| Surgery | 60 (100) | 30 (100) | 30 (100) | 1 |
| Radiation | 52 (87) | 25 (83) | 27 (90) | 0.704 |
| Endocrine therapy | 39 (65) | 21 (70) | 18 (60) | 0.588 |
| Chemotherapy | 31 (52) | 16 (53) | 15 (50) | 1 |
| Immunotherapy | 6 (10) | 3 (10) | 3 (10) | 1 |
| Sportive activities, n (%) | ||||
| No | 9 (15) | 5 (17) | 4 (13) | |
| Occasionally | 13 (22) | 4 (13) | 9 (30) | 0.293 |
| Regularly | 38 (64) | 21 (70) | 17 (57) | |
| Dance experience, n (%) | ||||
| No | 19 (32) | 12 (40) | 7 (23) | |
| Yes, in the past | 38 (63) | 16 (53) | 22 (73) | 0.273 |
| Yes, current | 3 (5) | 2 (7) | 1 (3) | |
| CFS-D | ||||
| Total fatigue score, mean (SD) | 32.2 (9.0) | 33.7 (7.6) | 30.6 (10.0) | 0.195 |
| Physical fatigue, mean (SD) | 14.1 (4.1) | 14.9 (3.8) | 13.3 (4.2) | 0.109 |
| Affective fatigue, mean (SD) | 6.9 (2.6) | 7.3 (2.2) | 6.4 (2.8) | 0.196 |
| Cognitive fatigue, mean (SD) | 11.2 (3.5) | 11.4 (3.0) | 10.9 (4.0) | 0.605 |
| Tango, n = 24 | Waiting, n = 28 | Tango vs. Waiting | ||||
|---|---|---|---|---|---|---|
| dmean (SD) | p-Value | dmean (SD) | p-Value | p-Value | d [95% CI] | |
| CFS-D-total | −4.4 (5.4) | 0.001 * | −1.3 (4.4) | 0.14 | 0.03 * | −0.64 [−1.2; −0.08] |
| Physical fatigue | −1.9 (2.5) | 0.002 * | −0.78 (2.6) | 0.14 | 0.13 | −0.43 [−1.0; 0.12] |
| Affective fatigue | −1.0 (2.4) | 0.052 | −0.3 (1.3) | 0.32 | 0.15 | −0.42 [−1.0; 0.14] |
| Cognitive fatigue | −1.5 (2.2) | 0.004 * | −0.3 (1.8) | 0.44 | 0.03 * | −0.62 [−1.2; −0.06] |
| PSQI-total | −0.8 (2.5) | 0.16 | −0.8 (2.3) | 0.08 | 0.96 | 0.02 [−0.54; 0.57] |
| Sleep latency | −0.3 (0.8) | 0.04 * | −0.1 (0.8) | 0.36 | 0.39 | −0.25 [−0.79; 0.30] |
| Daytime sleepiness | −0.3 (0.5) | 0.03 * | −0.04 (0.6) | 0.75 | 0.16 | −0.41 [−0.97; 0.15] |
| EORTC QLQ C30 | ||||||
| Global health | 4.7 (16.2) | 0.18 | −1.9 (11.0) | 0.40 | 0.10 | 0.48 [−0.08; 1.03] |
| Physical functioning | 3.3 (12.3) | 0.21 | −4.1 (17.8) | 0.25 | 0.09 | 0.48 [−0.08; 1.03] |
| Cognitive functioning | 6.9 (17.3) | 0.07 | 0.6 (20.7) | 0.88 | 0.25 | 0.33 [−0.22; 0.88] |
| Social functioning | 14.9 (27.0) | 0.01 * | 3.6 (28.3) | 0.52 | 0.16 | 0.41 [−0.14; 0.96] |
| Appetite loss | 0.0 (16.7) | 1 | 8.3 (21.1) | 0.05 * | 0.13 | −0.43 [−0.98; −0.12] |
| Diarrhea | −8.3 (19.8) | 0.06 | 7.1 (24.2) | 0.14 | 0.02 * | −0.69 [−1.25; −0.13] |
| n = 50 | dmean | SD | p-Value |
|---|---|---|---|
| CFS-D-total | −3.6 | 5.8 | 0.01 * |
| Physical fatigue | −1.6 | 2.8 | 0.02 * |
| Affective fatigue | −1.0 | 2.3 | 0.06 * |
| Cognitive fatigue | −1.1 | 2.3 | 0.002 * |
| PSQI-total | −0.9 | 2.7 | 0.03 * |
| Daytime sleepiness | −0.2 | 0.6 | 0.02 * |
| EORTC QLQ-C30 | |||
| Global health status | 5.7 | 15.6 | 0.02 * |
| Physical functioning | 6.9 | 14.3 | 0.001 * |
| Role functioning | 8.2 | 25.9 | 0.03 * |
| Cognitive functioning | 6.3 | 19.7 | 0.03 * |
| Social functioning | 9.2 | 27.6 | 0.02 * |
| Fatigue | −9.8 | 17.5 | 0.0003 * |
| Insomnia | −10.2 | 25.6 | 0.008 * |
| Diarrhea | −8.7 | 23.9 | 0.01 * |
| CFS-D, n = 50 | Total | Physical Fatigue | Cognitive Fatigue | Affective Fatigue | |
|---|---|---|---|---|---|
| Adjusted for | age, cancer stage, T0-value, and menopausal status | ||||
| Endocrine therapy | −6.825 * | −7.725 * | −6.513 | −7.119 + | |
| Reference BMI normal | |||||
| BMI overweight | 2.350 | 0.900 | 3.159 | 5.239 | |
| BMI obese | −7.391 | −12.882 * | −5.695 | −6.478 | |
| Sports | −3.711 * | −4.732 * | −3.760 + | −3.234 | |
| Dance experience | 6.781 * | 6.890 * | 6.390+ | 6.930+ | |
| EORTC QLQ C30, n = 50 | QL | PF | EF | CF | FA |
| Adjusted for | age, cancer stage, T0-value, and menopausal status | ||||
| Endocrine therapy | −2.847 | −1.894 | 3.242 | 3.315 | −2.367 |
| Reference BMI normal | |||||
| BMI overweight | −0.940 | 0.624 | 5.318 | 8.703 | 5.516 |
| BMI obese | 3.106 | 12.775 + | 27.671 ** | 14.755 | −6.873 |
| Sports | 4.353 + | 0.941 | 3.609 | 8.44 0 ** | −5.485 * |
| Dance experience | −5.071 | 1.091 | −9.575+ | −15.511 ** | 13.107 ** |
| n = 56 | Completed Tango (89%) | Discontinued Tango (11%) | p-Value |
|---|---|---|---|
| Number of patients, n (%) | 50 (100) | 6 (100) | |
| Age, years, mean (SD) | 61.3 (9.9) | 60.5 (12.2) | 0.855 |
| Body mass index (BMI) | |||
| Normal (18.5 ≤ BMI < 25) | 36 (72) | 2 (33) | |
| Overweight (25 ≤ BMI < 30) | 10 (20) | 1 (17) | 0.012 * |
| Obese (BMI ≥ 30) | 4 (8) | 3 (50) | |
| Living in partnership, n (%) | 31 (62) | 5 (83) | 0.562 |
| Years since first diagnosis: mean (SD) | 1.7 (0.7) | 1.4 (0.1) | 0.328 |
| UICC stages, n (%) | |||
| I | 23 (46) | 2 (33) | |
| II | 20 (40) | 2 (33) | 0.473 |
| III | 7 (14) | 2 (33) | |
| Hormonal status, n (%) | |||
| Premenopausal | 2 (4) | 0 | |
| Postmenopausal | 48 (96) | 6 (100) | 1 |
| Triple-negative status, n (%) | 4 (8) | 2 (33) | 0.231 |
| Interventions, n (%) | |||
| Surgery | 50 (100) | 6 (100) | 1 |
| Radiation | 46 (92) | 5 (83) | 1 |
| Endocrine therapy | 34 (68) | 4 (67) | 1 |
| Chemotherapy | 24 (48) | 6 (100) | 0.048 * |
| Immunotherapy | 6 (12) | 0 | 0.841 |
| Sport activities, n (%) | |||
| No | 8 (16) | 1 (17) | |
| Occasionally | 11 (22) | 1 (17) | 0.955 |
| Regularly | 31 (62) | 4 (67) | |
| Dance experience, n (%) | |||
| No | 16 (32) | 1 (17) | |
| Yes, in the past | 32 (64) | 4 (67) | 0.363 |
| Yes, current | 2 (4) | 1 (17) | |
| QoL assessment at baseline | |||
| CFS-D total, mean (SD) | 31.01 (9.26) | 37.00 (5.23) | 0.133 |
| PSQI total, mean (SD) | 9.55 (3.43) | 11.50 (4.99) | 0.229 |
| EORTC QLQ C30 Global health, mean (SD) | 54.42 (16.84) | 51.67 (20.00) | 0.739 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schad, F.; Rieser, T.; Becker, S.; Groß, J.; Matthes, H.; Oei, S.L.; Thronicke, A. Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers 2023, 15, 2920. https://doi.org/10.3390/cancers15112920
Schad F, Rieser T, Becker S, Groß J, Matthes H, Oei SL, Thronicke A. Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers. 2023; 15(11):2920. https://doi.org/10.3390/cancers15112920
Chicago/Turabian StyleSchad, Friedemann, Thomas Rieser, Sarah Becker, Jessica Groß, Harald Matthes, Shiao Li Oei, and Anja Thronicke. 2023. "Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial" Cancers 15, no. 11: 2920. https://doi.org/10.3390/cancers15112920
APA StyleSchad, F., Rieser, T., Becker, S., Groß, J., Matthes, H., Oei, S. L., & Thronicke, A. (2023). Efficacy of Tango Argentino for Cancer-Associated Fatigue and Quality of Life in Breast Cancer Survivors: A Randomized Controlled Trial. Cancers, 15(11), 2920. https://doi.org/10.3390/cancers15112920