
Perioperative Blood Transfusion Is Dose-Dependently Associated with Cancer Recurrence and Mortality after Head and Neck Cancer Surgery

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Collection
2.3. Statistical Analysis
3. Results
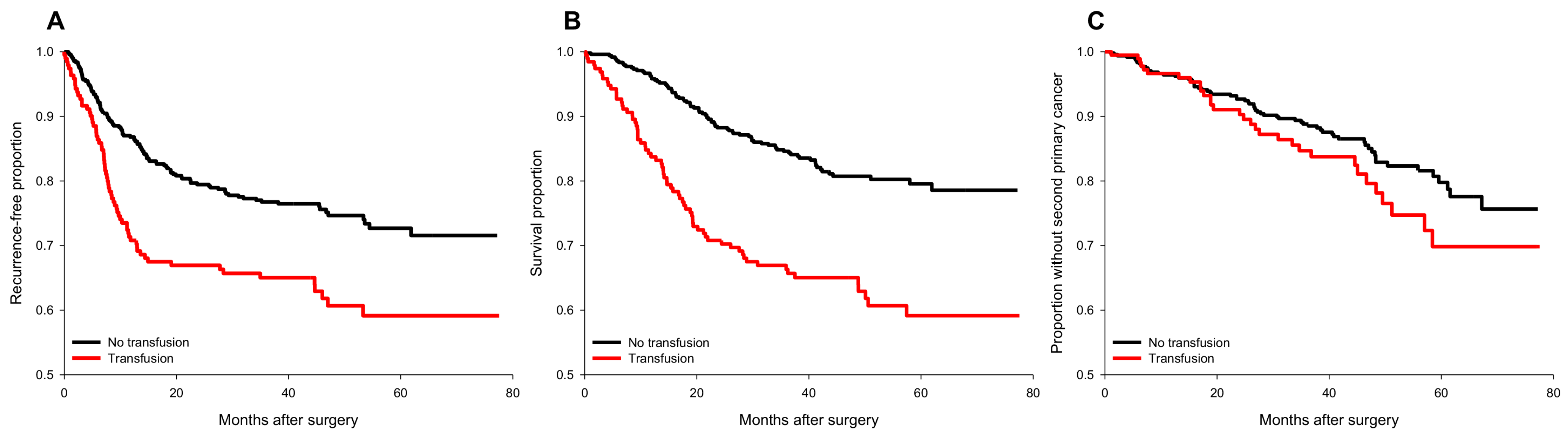
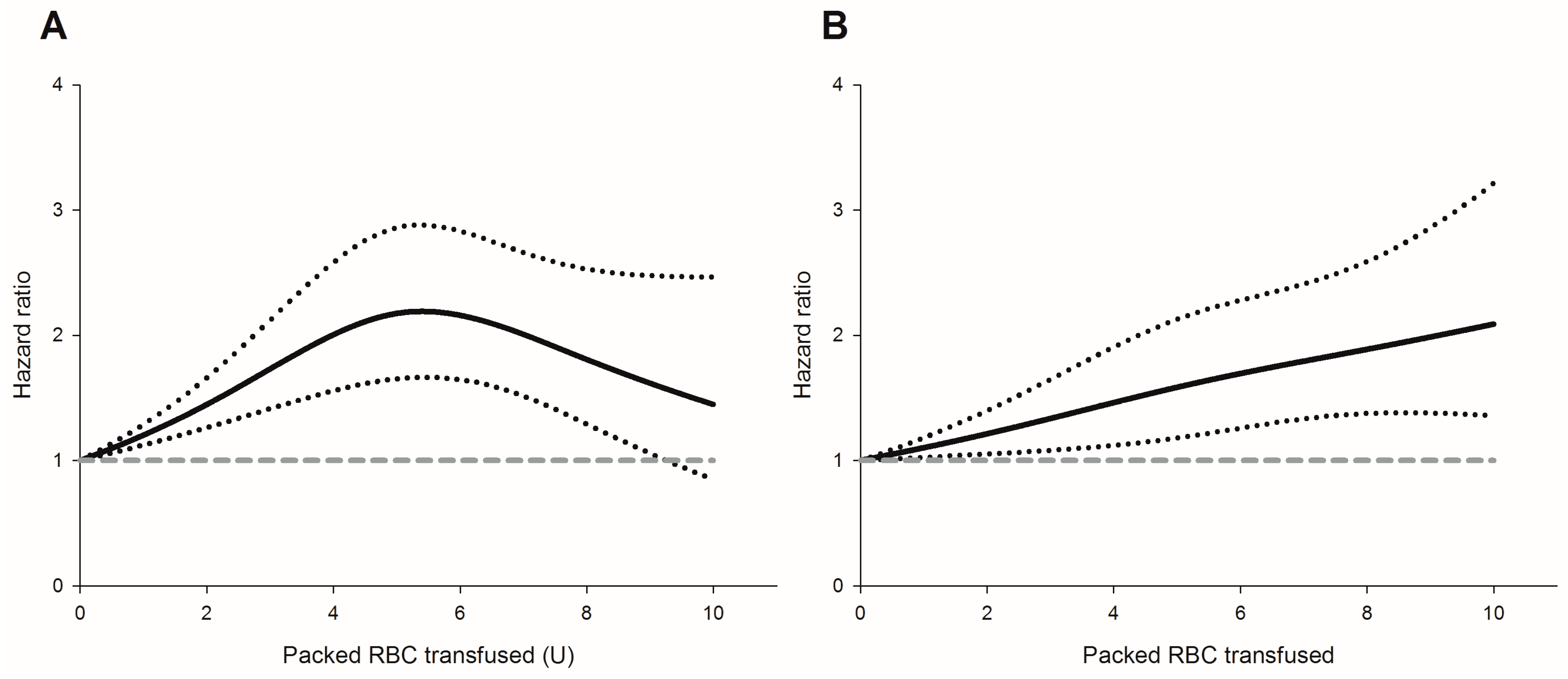
3.1. Perioperative Transfusion and Recurrence Risk
3.2. The risk of Perioperative Transfusion and Mortality
3.3. Perioperative Transfusion and Occurrence of a Second Primary Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q. Head and neck cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Nair, R.; Jamieson, L.; Liu, Z.; Bi, P. Incidence Trends of Lip, Oral Cavity, and Pharyngeal Cancers: Global Burden of Disease 1990-2017. J. Dent. Res. 2020, 99, 143–151. [Google Scholar] [CrossRef]
- Hsu, W.-L.; Yu, K.J.; Chiang, C.-J.; Chen, T.-C.; Wang, C.-P. Head and neck cancer incidence trends in Taiwan, 1980~2014. Int. J. Head Neck Sci. 2017, 1, 180–189. [Google Scholar]
- Grégoire, V.; Lefebvre, J.L.; Licitra, L.; Felip, E. Squamous cell carcinoma of the head and neck: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v184–v186. [Google Scholar] [CrossRef] [PubMed]
- Sturgis, E.M.; Miller, R.H. Second primary malignancies in the head and neck cancer patient. Ann. Otol. Rhinol. Laryngol. 1995, 104, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Noble, A.R.; Greskovich, J.F.; Han, J.; Reddy, C.A.; Nwizu, T.I.; Khan, M.F.; Scharpf, J.; Adelstein, D.J.; Burkey, B.B.; Koyfman, S.A. Risk Factors Associated with Disease Recurrence in Patients with Stage III/IV Squamous Cell Carcinoma of the Oral Cavity Treated with Surgery and Postoperative Radiotherapy. Anticancer Res. 2016, 36, 785–792. [Google Scholar]
- Chau, J.K.; Harris, J.R.; Seikaly, H.R. Transfusion as a predictor of recurrence and survival in head and neck cancer surgery patients. J. Otolaryngol.-Head Neck Surg. 2010, 39, 516–522. [Google Scholar]
- Szakmany, T.; Dodd, M.; Dempsey, G.; Lowe, D.; Brown, J.; Vaughan, E.; Rogers, S. The influence of allogenic blood transfusion in patients having free-flap primary surgery for oral and oropharyngeal squamous cell carcinoma. Br. J. Cancer 2006, 94, 647–653. [Google Scholar] [CrossRef]
- Jackson, R.M.; Rice, D.H. Blood Transfusions and Recurrence in Head and Neck Cancer. Ann. Otol. Rhinol. Laryngol. 1989, 98, 171–173. [Google Scholar] [CrossRef]
- Jones, K.R.; Weissler, M.C. Blood Transfusion and Other Risk Factors for Recurrence of Cancer of the Head and Neck. Arch. Otolaryngol.–Head Neck Surg. 1990, 116, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Talari, K.; Goyal, M. Retrospective studies - utility and caveats. J. R. Coll. Physicians Edinb. 2020, 50, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Mansournia, M.A.; Altman, D.G. Inverse probability weighting. BMJ 2016, 352, i189. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, J.; Wu, Q.V.; Gooley, T.A. Cubic splines to model relationships between continuous variables and outcomes: A guide for clinicians. Bone Marrow Transplant. 2020, 55, 675–680. [Google Scholar] [CrossRef]
- Perisanidis, C.; Mittlböck, M.; Dettke, M.; Schopper, C.; Schoppmann, A.; Kostakis, G.C.; Russmüller, G.; Stift, A.; Kanatas, A.; Seemann, R.; et al. Identifying Risk Factors for Allogenic Blood Transfusion in Oral and Oropharyngeal Cancer Surgery With Free Flap Reconstruction. J. Oral Maxillofac. Surg. 2013, 71, 798–804. [Google Scholar] [CrossRef]
- Perisanidis, C.; Dettke, M.; Papadogeorgakis, N.; Schoppmann, A.; Mittlböck, M.; Kyzas, P.A.; Ewers, R.; Seemann, R. Transfusion of allogenic leukocyte-depleted packed red blood cells is associated with postoperative morbidity in patients undergoing oral and oropharyngeal cancer surgery. Oral Oncol. 2012, 48, 372–378. [Google Scholar] [CrossRef]
- Fenner, M.; Vairaktaris, E.; Nkenke, E.; Weisbach, V.; Neukam, F.W.; Radespiel-Tröger, M. Prognostic impact of blood transfusion in patients undergoing primary surgery and free-flap reconstruction for oral squamous cell carcinoma. Cancer 2009, 115, 1481–1488. [Google Scholar] [CrossRef]
- Chesnaye, N.C.; Stel, V.S.; Tripepi, G.; Dekker, F.W.; Fu, E.L.; Zoccali, C.; Jager, K.J. An introduction to inverse probability of treatment weighting in observational research. Clin. Kidney J. 2022, 15, 14–20. [Google Scholar] [CrossRef]
- Cata, J.P.; Wang, H.; Gottumukkala, V.; Reuben, J.; Sessler, D.I. Inflammatory response, immunosuppression, and cancer recurrence after perioperative blood transfusions. Br. J. Anaesth. 2013, 110, 690–701. [Google Scholar] [CrossRef]
- Tzounakas, V.L.; Seghatchian, J.; Grouzi, E.; Kokoris, S.; Antonelou, M.H. Red blood cell transfusion in surgical cancer patients: Targets, risks, mechanistic understanding and further therapeutic opportunities. Transfus. Apher. Sci. 2017, 56, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.M.; Wang, M.Z. Overview of Extracellular Vesicles, Their Origin, Composition, Purpose, and Methods for Exosome Isolation and Analysis. Cells 2019, 8, 727. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Liu, Y.; Han, Q.; Han, Y.; Wang, J.; Zhang, H. Transfusion-related immunomodulation in patients with cancer: Focus on the impact of extracellular vesicles from stored red blood cells. Int. J. Oncol. 2021, 59, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Goubran, H.; Sheridan, D.; Radosevic, J.; Burnouf, T.; Seghatchian, J. Transfusion-related immunomodulation and cancer. Transfus. Apher. Sci. 2017, 56, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Remy, K.E.; Hall, M.W.; Cholette, J.; Juffermans, N.P.; Nicol, K.; Doctor, A.; Blumberg, N.; Spinella, P.C.; Norris, P.J.; Dahmer, M.K. Mechanisms of red blood cell transfusion-related immunomodulation. Transfusion 2018, 58, 804–815. [Google Scholar] [CrossRef]
- Aguilar-Nascimento, J.E.; Zampieri-Filho, J.P.; Bordin, J.O. Implications of perioperative allogeneic red blood cell transfusion on the immune-inflammatory response. Hematol. Transfus. Cell Ther. 2020. [Google Scholar] [CrossRef]
- Liu, L.; Wang, Z.; Jiang, S.; Shao, B.; Liu, J.; Zhang, S.; Zhou, Y.; Zhou, Y.; Zhang, Y. Perioperative allogenenic blood transfusion is associated with worse clinical outcomes for hepatocellular carcinoma: A meta-analysis. PloS ONE 2013, 8, e64261. [Google Scholar] [CrossRef]
- Acheson, A.G.; Brookes, M.J.; Spahn, D.R. Effects of Allogeneic Red Blood Cell Transfusions on Clinical Outcomes in Patients Undergoing Colorectal Cancer Surgery: A Systematic Review and Meta-Analysis. Ann. Surg. 2012, 256, 235–244. [Google Scholar] [CrossRef]
- Blumberg, N.; Heal, J.M.; Murphy, P.; Agarwal, M.M.; Chuang, C. Association between transfusion of whole blood and recurrence of cancer. Br. Med. J. 1986, 293, 530–533. [Google Scholar] [CrossRef]
- Reeh, M.; Ghadban, T.; Dedow, J.; Vettorazzi, E.; Uzunoglu, F.G.; Nentwich, M.; Kluge, S.; Izbicki, J.R.; Vashist, Y.K. Allogenic blood transfusion is associated with poor perioperative and long-term outcome in esophageal cancer. World J. Surg. 2017, 41, 208–215. [Google Scholar] [CrossRef]
- Latif, M.J.; Tan, K.S.; Molena, D.; Huang, J.; Bott, M.J.; Park, B.J.; Adusumilli, P.S.; Rusch, V.W.; Bains, M.S.; Downey, R.J. Perioperative blood transfusion has a dose-dependent relationship with disease recurrence and survival in patients with non–small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2019, 157, 2469–2477.e2410. [Google Scholar] [CrossRef] [PubMed]
- Tai, Y.H.; Wu, H.L.; Mandell, M.S.; Lin, S.P.; Tsou, M.Y.; Chang, K.Y. The association of non-small cell lung cancer recurrence with allogenic blood transfusion after surgical resection: A propensity score analysis of 1803 patients. Eur. J. Cancer 2020, 140, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Tai, Y.H.; Wu, H.L.; Mandell, M.S.; Tsou, M.Y.; Chang, K.Y. The association of allogeneic blood transfusion and the recurrence of hepatic cancer after surgical resection. Anaesthesia 2020, 75, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.L.; Tai, Y.H.; Lin, S.P.; Chan, M.Y.; Chen, H.H.; Chang, K.Y. The Impact of Blood Transfusion on Recurrence and Mortality Following Colorectal Cancer Resection: A Propensity Score Analysis of 4030 Patients. Sci. Rep. 2018, 8, 13345. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Wakai, K.; Matsuo, K.; Hirose, K.; Ito, H.; Kuriki, K.; Sato, S.; Ueda, R.; Hasegawa, Y.; Tajima, K. Effect of dietary antioxidants and risk of oral, pharyngeal and laryngeal squamous cell carcinoma according to smoking and drinking habits. Cancer Sci. 2006, 97, 760–767. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Giovannucci, E.L. Diet and cancer prevention. Oncogene 2004, 23, 6349–6364. [Google Scholar] [CrossRef]
- Ravasco, P.; Monteiro-Grillo, I.; Marques Vidal, P.; Camilo, M.E. Impact of nutrition on outcome: A prospective randomized controlled trial in patients with head and neck cancer undergoing radiotherapy. Head Neck: J. Sci. Spec. Head Neck 2005, 27, 659–668. [Google Scholar] [CrossRef]
- Orell-Kotikangas, H.; Österlund, P.; Mäkitie, O.; Saarilahti, K.; Ravasco, P.; Schwab, U.; Mäkitie, A.A. Cachexia at diagnosis is associated with poor survival in head and neck cancer patients. Acta Oto-Laryngol. 2017, 137, 778–785. [Google Scholar] [CrossRef]
- Baptistella, A.R.; Hilleshein, K.D.; Beal, C.; Brambatti, J.S.; Caron, R.; Baptistella, S.F.; Zuquello, R.Á.; Rossoni, C.; Manfro, G. Weight loss as a prognostic factor for recurrence and survival in oropharyngeal squamous cell carcinoma patients. Mol. Clin. Oncol. 2018, 9, 666–672. [Google Scholar] [CrossRef]
- van de Watering, L.M.; Brand, A.; Houbiers, J.G.; Klein Kranenbarg, W.M.; Hermans, J.; van de Velde, C. Perioperative blood transfusions, with or without allogeneic leucocytes, relate to survival, not to cancer recurrence. Br. J. Surg. 2001, 88, 267–272. [Google Scholar] [CrossRef]
- Lange, M.M.; van Hilten, J.A.; van de Watering, L.M.; Bijnen, B.A.; Roumen, R.M.; Putter, H.; Brand, A.; van de Velde, C.J. Leucocyte depletion of perioperative blood transfusion does not affect long-term survival and recurrence in patients with gastrointestinal cancer. Br. J. Surg. 2009, 96, 734–740. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, G.S., Jr.; Schink, J.C.; Buoy, C.; Ahmad, S.; Fitzgerald, P.C.; McCarthy, R.J. The association between allogeneic perioperative blood transfusion on tumour recurrence and survival in patients with advanced ovarian cancer. Transfus. Med. 2012, 22, 97–103. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Original Data | After IPTW | |||||
|---|---|---|---|---|---|---|
| No Transfusion (n = 491) | Transfusion (n = 192) | SDD | No Transfusion | Transfusion | SDD | |
| Age | 58 ± 13 | 57 ± 11 | 8.9 | 58 ± 12 | 57 ± 11 | 4.8 |
| Sex, male | 417 (84.9%) | 172 (89.6%) | 14.0 | 560 (86.8%) | 434 (91.3%) | 14.6 |
| BMI, kg·m−2 | 25.0 ± 4.3 | 24.15 ± 3.68 | 21.6 | 24.87 ± 4.18 | 25.22 ± 3.93 | 8.5 |
| ASA physical status > 3 | 112 (22.8%) | 67 (34.9%) | 26.9 | 179 (27.7%) | 175 (36.9%) | 19.8 |
| Smoking | 358 (72.9%) | 151 (78.6%) | 13.4 | 489 (75.8%) | 396 (83.4%) | 19.2 |
| Betel nut chewing | 237 (48.3%) | 138 (71.9%) | 49.7 | 354 (54.8%) | 323 (68.1%) | 27.5 |
| Alcohol | 293 (59.7%) | 123 (64.1%) | 9.0 | 397 (61.5%) | 338 (71.1%) | 20.3 |
| Preoperative haemoglobin, g·dL−1 | 13.9 ± 1.6 | 13.1 ± 1.7 | 48.7 | 13.8 ± 1.7 | 13.5 ± 1.5 | 18.6 |
| Anesthesia time, min * | 8.15 ± 0.97 | 9.67 ± 0.71 | 178.4 | 8.49 ± 1.09 | 8.90 ± 1.14 | 36.8 |
| Blood loss during surgery, mL * | 5.60 ± 2.10 | 8.87 ± 1.48 | 179.9 | 6.33 ± 2.32 | 7.41 ± 2.15 | 48.5 |
| Positive surgical margin | 315 (64.2%) | 113 (58.9%) | 10.9 | 380 (58.8%) | 244 (51.4%) | 14.9 |
| Primary tumour | 117.6 | 15.1 | ||||
| T1 and T2 | 300 (61.1%) | 27 (14.1%) | 408 (63.3%) | 265 (55.9%) | ||
| T3 and T4 | 191 (38.9%) | 165 (85.9%) | 237 (36.7%) | 210 (44.1%) | ||
| Histologic differentiation | 8.1 | 5.6 | ||||
| Well | 213 (43.4%) | 91 (47.4%) | 305 (47.3%) | 238 (50.1%) | ||
| Moderate to severe | 278 (56.6%) | 101 (52.6%) | 340 (52.7%) | 237 (49.9%) | ||
| Lymph node involvement | 127 (25.9%) | 99 (51.6%) | 54.7 | 199 (30.8%) | 183 (38.5%) | 16.1 |
| Adjunct radiotherapy | 181 (36.9%) | 136 (70.8%) | 72.5 | 293 (45.4%) | 228 (48.0%) | 5.1 |
| Adjunct chemotherapy | 143 (29.1%) | 125 (65.1%) | 77.3 | 244 (37.9%) | 207 (43.6%) | 11.7 |
| Linear Effect | Nonlinear Effect | |||||
|---|---|---|---|---|---|---|
| Estimate | SE | p | Estimate | SE | p | |
| Recurrence-free survival | 0.185 | 0.035 | <0.001 | −0.033 | 0.010 | 0.001 |
| Overall survival | 0.097 | 0.036 | 0.008 | −0.005 | 0.009 | 0.557 |
| HR | 95% CI | p | |
|---|---|---|---|
| Blood transfusion | 1.40 | 0.99~1.97 | 0.059 |
| Positive surgical margin | 1.63 | 1.15~2.30 | 0.006 |
| Primary tumor (T3,4 vs. T1,2) | 1.59 | 1.12~2.27 | 0.010 |
| Lymph node involvement | 1.96 | 1.39~2.78 | <0.001 |
| Adjunct radiotherapy | 0.61 | 0.42~0.88 | 0.007 |
| HR | 95% CI | p | |
|---|---|---|---|
| Blood transfusion | 1.39 | 0.98~1.97 | 0.067 |
| Age | 1.02 | 0.84~0.94 | 0.002 |
| BMI | 0.94 | 1.12~1.37 | 0.002 |
| Primary tumor (T3,4 vs. T1,2) | 1.77 | 1.07~1.25 | 0.002 |
| Lymph node involvement | 3.44 | 1.85~5.24 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hee, H.-Z.; Chang, K.-Y.; Huang, C.-Y.; Chang, W.-K.; Tsou, M.-Y.; Lin, S.-P. Perioperative Blood Transfusion Is Dose-Dependently Associated with Cancer Recurrence and Mortality after Head and Neck Cancer Surgery. Cancers 2023, 15, 99. https://doi.org/10.3390/cancers15010099
Hee H-Z, Chang K-Y, Huang C-Y, Chang W-K, Tsou M-Y, Lin S-P. Perioperative Blood Transfusion Is Dose-Dependently Associated with Cancer Recurrence and Mortality after Head and Neck Cancer Surgery. Cancers. 2023; 15(1):99. https://doi.org/10.3390/cancers15010099
Chicago/Turabian StyleHee, Hui-Zen, Kuang-Yi Chang, Chii-Yuan Huang, Wen-Kuei Chang, Mei-Yung Tsou, and Shih-Pin Lin. 2023. "Perioperative Blood Transfusion Is Dose-Dependently Associated with Cancer Recurrence and Mortality after Head and Neck Cancer Surgery" Cancers 15, no. 1: 99. https://doi.org/10.3390/cancers15010099
APA StyleHee, H.-Z., Chang, K.-Y., Huang, C.-Y., Chang, W.-K., Tsou, M.-Y., & Lin, S.-P. (2023). Perioperative Blood Transfusion Is Dose-Dependently Associated with Cancer Recurrence and Mortality after Head and Neck Cancer Surgery. Cancers, 15(1), 99. https://doi.org/10.3390/cancers15010099