
Automated Prediction of the Response to Neoadjuvant Chemoradiotherapy in Patients Affected by Rectal Cancer

 ,
,  , , ,
, , ,  , , ,
, , , 
 ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
- TRG0: no viable cancer cells (pathological complete response);
- TRG1: single or small groups of tumor cells (moderate response);
- TRG2: residual cancer outgrown by fibrosis (minimal response); and
- TRG3: minimal or no tumor cells killed (poor response).
2. Materials and Methods
2.1. Patient Selection
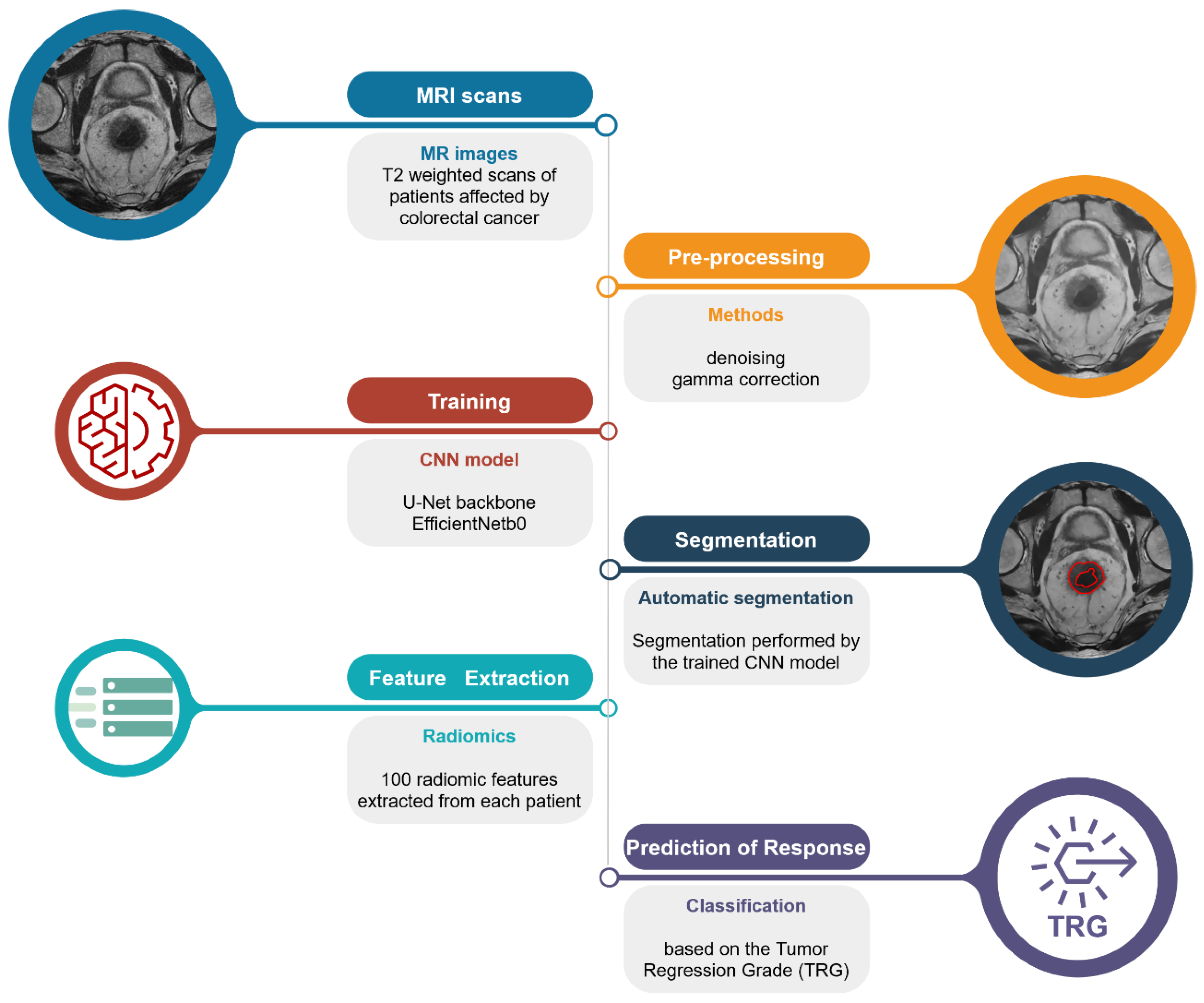
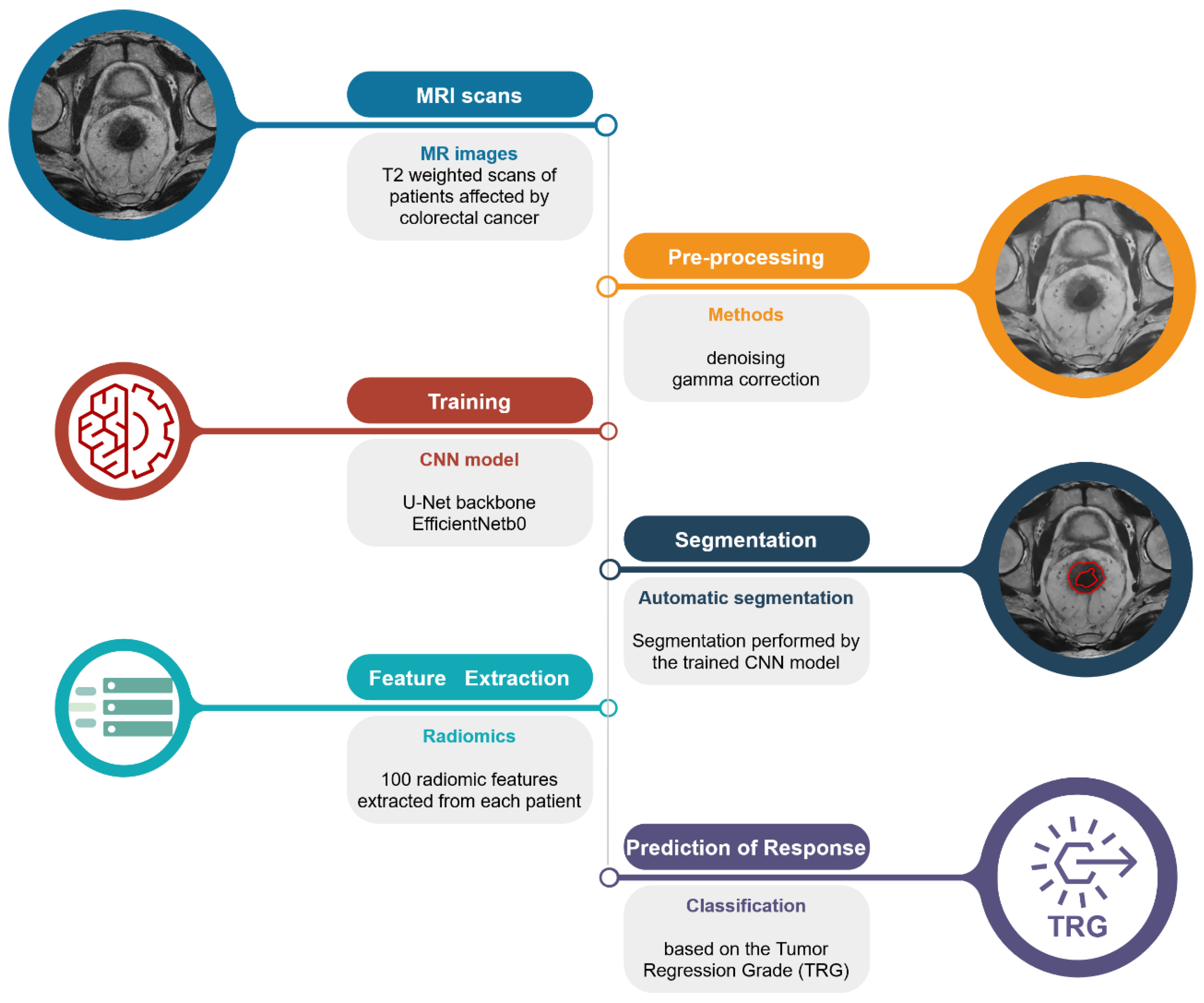
2.2. Pipeline Overview
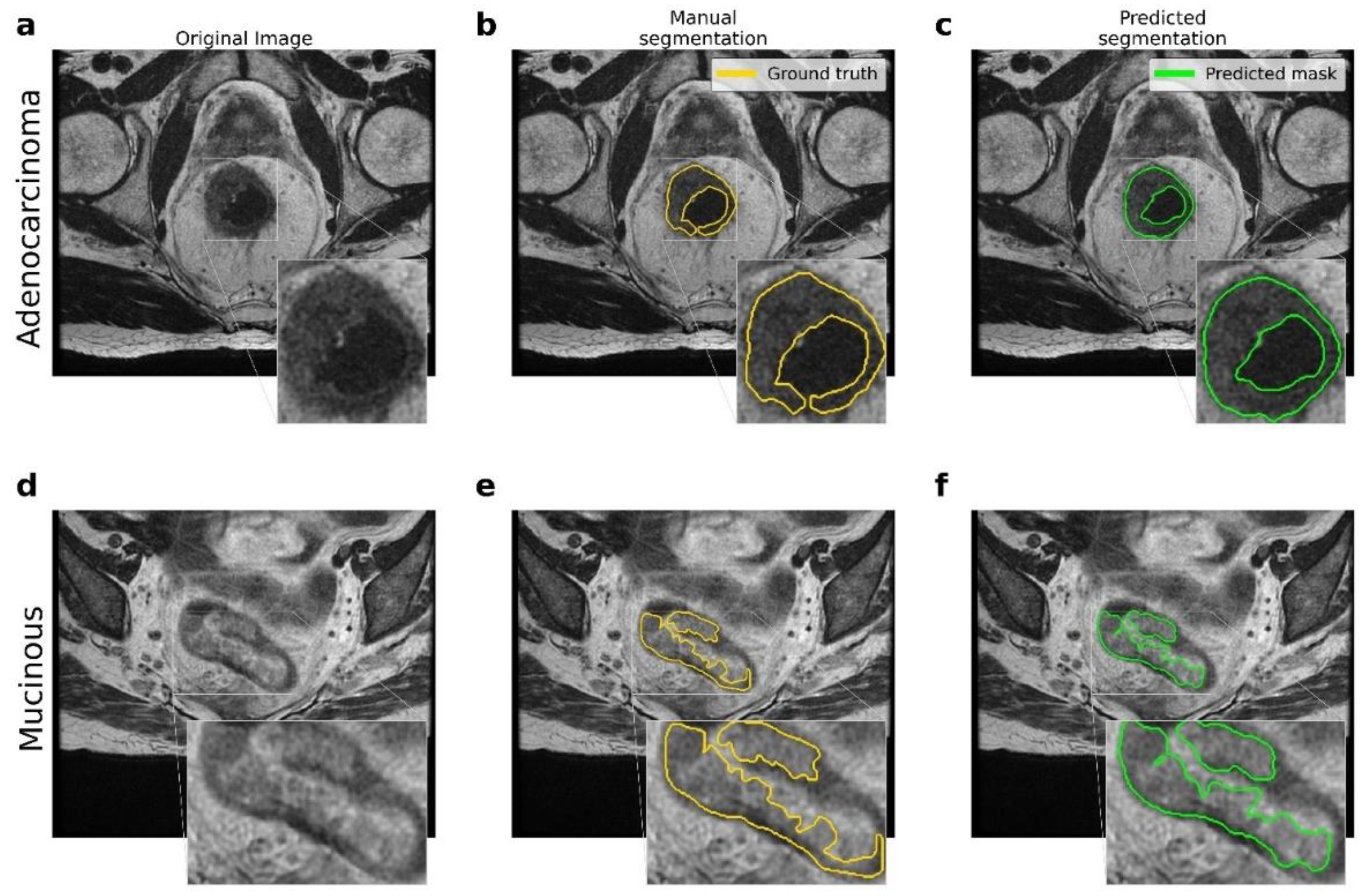
2.3. Rectal Segmentation
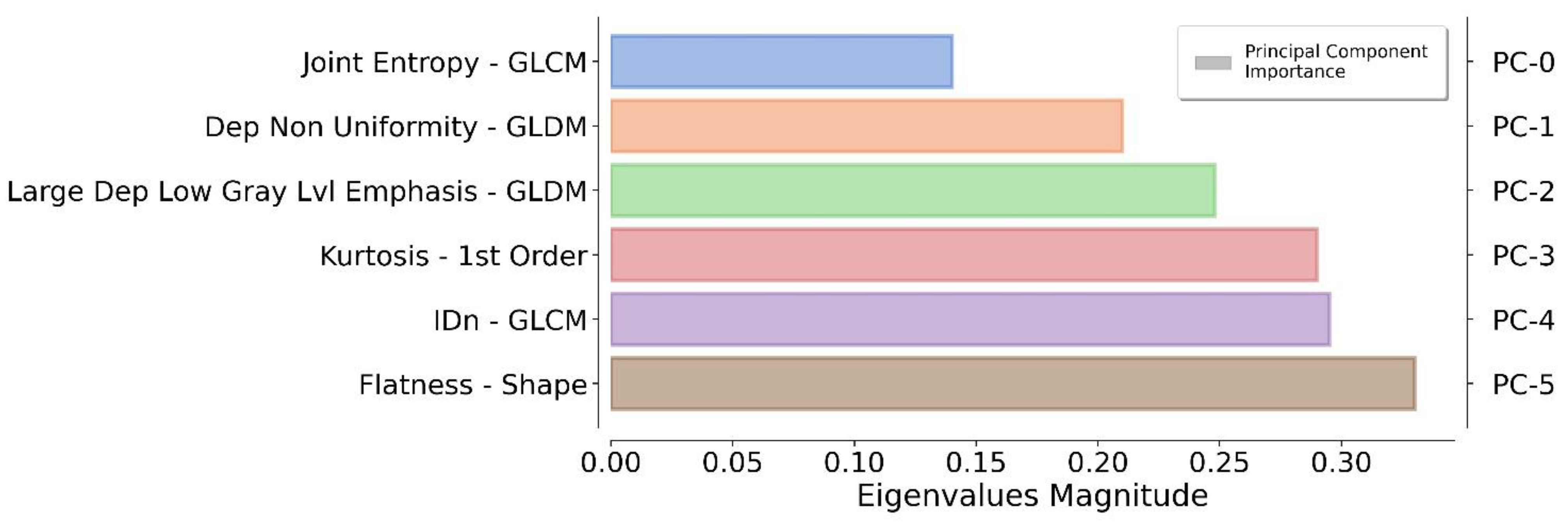
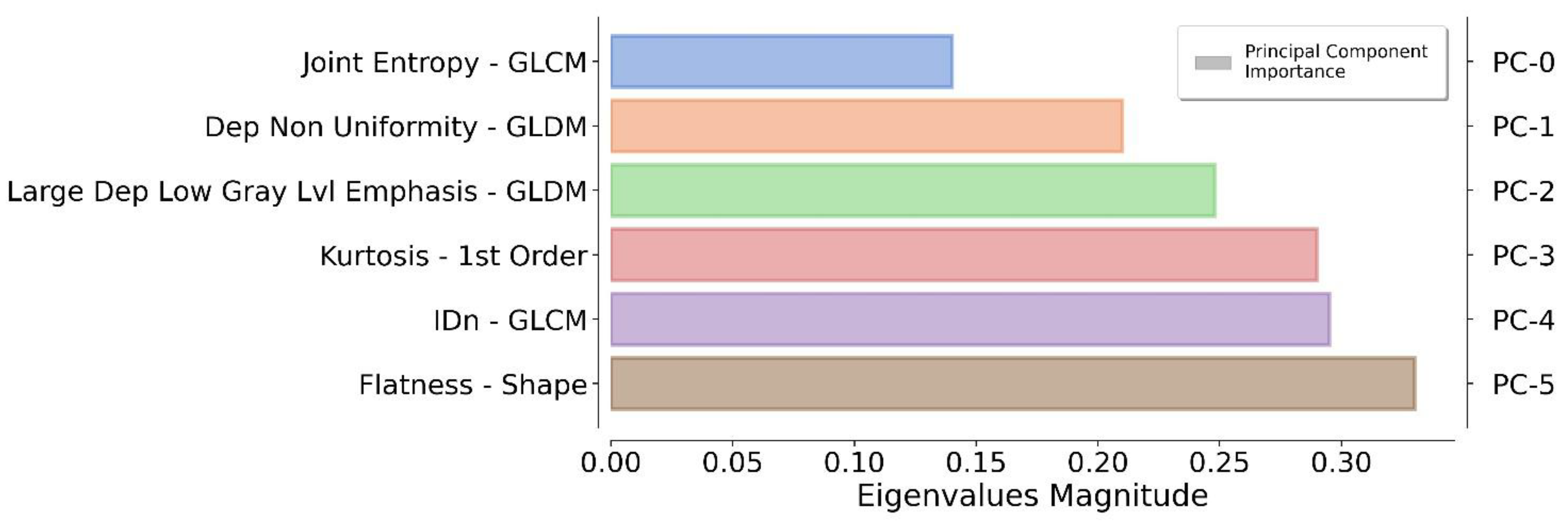
2.4. Feature Extraction
2.5. TRG Prediction
3. Results
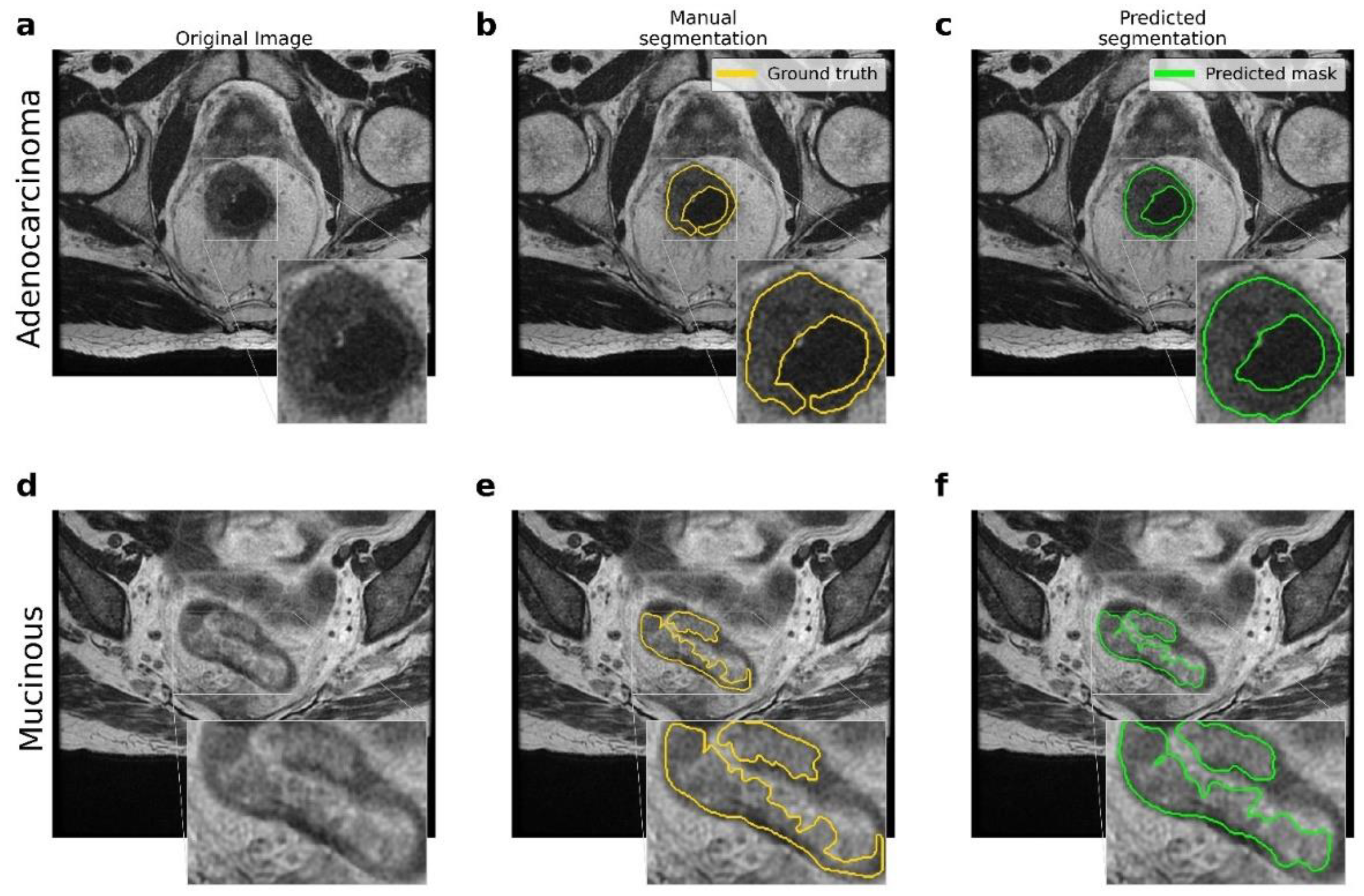
3.1. Rectal Segmentation
3.2. TRG Prediction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawes, D.; Boulos, P.B. Advances in the management of rectal cancer. J. R. Soc. Med. 2002, 95, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Arnoletti, J.P.; Bekaii-Saab, T.; Chan, E.; Chen, Y.J.; Choti, M.A.; Cooper, H.S.; Dilawari, R.A.; Engstrom, P.F.; Enzinger, P.C.; et al. Clinical practice guidelines in oncology. JNCCN J. Natl. Compr. Cancer Netw. 2011, 9, 1238–1289. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Caruso, D.; Grassi, R.; Cappabianca, S.; Reginelli, A.; Rizzati, R.; Masselli, G.; Golfieri, R.; Rengo, M.; Regge, D.; et al. Structured Reporting of Rectal Cancer Staging and Restaging: A Consensus Proposal. Cancers 2021, 13, 2135. [Google Scholar] [CrossRef] [PubMed]
- Gersak, M.M.; Badea, R.; Graur, F.; al Hajjar, N.; Furcea, L.E.; Dudea, S.M. Endoscopic ultrasound for the characterization and staging of rectal cancer. Current state of the method. Technological advances and perspectives. Med. Ultrason. 2015, 17, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Labianca, R.; Nordlinger, B.; Beretta, G.D.; Mosconi, S.; Mandalà, M.; Cervantes, A.; Arnold, D. Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi64–vi72. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, C.N.; Ganeshan, B.; Ciolina, M.; Rengo, M.; Meinel, F.G.; Musio, D.; De Felice, F.; Raffetto, N.; Tombolini, V.; Laghi, A. Texture Analysis as Imaging Biomarker of Tumoral Response to Neoadjuvant Chemoradiotherapy in Rectal Cancer Patients Studied with 3-T Magnetic Resonance. Investig. Radiol. 2014, 50, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Giannini, V.; Mazzetti, S.; Bertotto, I.; Chiarenza, C.; Cauda, S.; Delmastro, E.; Bracco, C.; Di Dia, A.; Leone, F.; Medico, E.; et al. Predicting locally advanced rectal cancer response to neoadjuvant therapy with 18F-FDG PET and MRI radiomics features. Eur. J. Pediatr. 2019, 46, 878–888. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Lamfichekh, N.; Etienne, P.L.; Rio, E.; Francois, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiation in patients with locally advanced rectal cancer: Final results of PRODIGE 23 phase III trial, a UNICANCER GI trial. J. Clin. Oncol. 2020, 38, 4007. [Google Scholar] [CrossRef]
- Coppola, F.; Giannini, V.; Gabelloni, M.; Panic, J.; Defeudis, A.; Monaco, S.L.; Cattabriga, A.; Cocozza, M.; Pastore, L.; Polici, M.; et al. Radiomics and Magnetic Resonance Imaging of Rectal Cancer: From Engineering to Clinical Practice. Diagnostics 2021, 11, 756. [Google Scholar] [CrossRef] [PubMed]
- Coppola, F.; Mottola, M.; Lo Monaco, S.; Cattabriga, A.; Cocozza, M.A.; Yuan, J.C.; De Benedittis, C.; Cuicchi, D.; Guido, A.; Rojas Llimpe, F.L.; et al. The Heterogeneity of Skewness in T2W-Based Radiomics Predicts the Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. Diagnostics 2021, 11, 795. [Google Scholar] [CrossRef] [PubMed]
- Trebeschi, S.; Van Griethuysen, J.J.M.; Lambregts, D.; Lahaye, M.J.; Parmar, C.; Bakers, F.C.H.; Peters, N.H.G.M.; Beets-Tan, R.G.H.; Aerts, H.J.W.L. Deep Learning for Fully-Automated Localization and Segmentation of Rectal Cancer on Multiparametric MR. Sci. Rep. 2017, 7, 5301. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-J.; Dou, Q.; Wang, Z.-X.; Liu, L.-Z.; Jin, Y.; Li, C.-F.; Wang, L.; Chen, H.; Xu, R.-H. 3-D RoI-Aware U-Net for Accurate and Efficient Colorectal Tumor Segmentation. IEEE Trans. Cybern. 2020, 51, 5397–5408. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Yu, M.; Chen, D.; Li, P.; Tang, B.; Li, J. Role of MRI-based radiomics in locally advanced rectal cancer (Review). Oncol. Rep. 2021, 47, 34. [Google Scholar] [CrossRef] [PubMed]
- Panic, J.; Defeudis, A.; Mazzetti, S.; Rosati, S.; Giannetto, G.; Vassallo, L.; Regge, D.; Balestra, G.; Giannini, V. A Convolutional Neural Network based system for Colorectal cancer segmentation on MRI images. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; Volume 2020, pp. 1675–1678. [Google Scholar] [CrossRef]
- Pang, X.; Wang, F.; Zhang, Q.; Li, Y.; Huang, R.; Yin, X.; Fan, X. A Pipeline for Predicting the Treatment Response of Neoadjuvant Chemoradiotherapy for Locally Advanced Rectal Cancer Using Single MRI Modality: Combining Deep Segmentation Network and Radiomics Analysis Based on “Suspicious Region”. Front. Oncol. 2021, 11, 711747. [Google Scholar] [CrossRef] [PubMed]
- Bulens, P.; Couwenberg, A.; Intven, M.; Debucquoy, A.; Vandecaveye, V.; Van Cutsem, E.; D’Hoore, A.; Wolthuis, A.; Mukherjee, P.; Gevaert, O.; et al. Predicting the tumor response to chemoradiotherapy for rectal cancer: Model development and external validation using MRI radiomics. Radiother. Oncol. 2020, 142, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Soomro, M.H.; Giunta, G.; Laghi, A.; Caruso, D.; Ciolina, M.; De Marchis, C.; Conforto, S.; Schmid, M. Haralick’s Texture Analysis Applied to Colorectal T2-Weighted MRI: A Preliminary Study of Significance for Cancer Evolution. In Proceedings of the 2017 13th IASTED International Conference on Biomedical Engineering (BioMed), Innsbruck, Austria, 20–21 February 2017. [Google Scholar] [CrossRef]
- Li, Z.; Ma, X.; Shen, F.; Lu, H.; Xia, Y.; Lu, J. Evaluating treatment response to neoadjuvant chemoradiotherapy in rectal cancer using various MRI-based ra-diomics models. BMC Med. Imaging 2021, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Beets-Tan, R.G.H.; Lambregts, D.M.J.; Maas, M.; Bipat, S.; Barbaro, B.; Curvo-Semedo, L.; Fenlon, H.M.; Gollub, M.J.; Gourtsoyianni, S.; Halligan, S.; et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur. Radiol. 2018, 28, 1465–1475. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Le, Q.V. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. In Proceedings of the 36th International Conference on Machine Learning, Long Beach, CA, USA, 9–15 June 2019. [Google Scholar]
- Filitto, G. MRI Colorectal Cancer Segmentation. Github–Online Resource. 2021. Available online: https://github.com/giuseppefilitto/img-segm (accessed on 28 February 2022).
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- TensorFlow: Large-Scale Machine Learning on Heterogeneous Systems. Github–Online Resource. 2015. Available online: https://github.com/tensorflow/tensorflow (accessed on 28 February 2022).

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Responder TRG 0–1 (n = 16) | Non-Responder TRG 2–3 (n = 23) | Total (n = 39) |
|---|---|---|---|
| Sex, males/females, n | 12/4 | 15/8 | 27/12 |
| % | 75/25 | 65/35 | 69/31 |
| Median age (range), years | 66 (33–85) | 63 (46–82) | 65 (33–85) |
| ECOG-PS 0 | 13 (81%) | 19 (82%) | 32 (82%) |
| ECOG-PS 1 | 2 (12.5%) | 3 (13%) | 5 (13%) |
| ECOG-PS 2 | 1 (6.5%) | 1 (5%) | 2 (5%) |
| cT | T2 2 (12.5%) | T2 1 (4%) | T2 3 (8%) |
| T3 13 (81%) | T3 17 (74%) | T3 30 (77%) | |
| T4 1 (6.5%) | T4 5 (22%) | T4 6 (15%) | |
| cN | N− 3 (19%) | N− 5 (20.0%) | N− 8 (20%) |
| N+ 13 (81%) | N+ 18 (80:0%) | N+ 31 (80%) |
| Trebeschi et al. [11] | Panic et al. [14] | Yi-Jie Huang et al. [12] | Xiaoling Pang et al. [15] | The Authors’ Pipeline |
|---|---|---|---|---|
| * DSC = 0.68 ** DSC = 0.70 | DSC = 0.58 | DSC = [0.66–0.72] | DSC = 0.66 | DSC = [0.73–0.75] |
| 140 patients | 33 patients (5 mucinous) | 64 patients (adenocarcinoma) | 275 patients (no mucinous) | 43 patients (1 mucinous) |
| MRI T2w + DWI | MRI T2w + DWI | MRI T2w | MRI T2w | MRI T2w |
| Custom CNN | Custom CNN | Custom ensemble of CNN and losses | U-Net | U-Net + EfficientNetb0 backbone |
| Support | Precision | Recall | F1-Score | MCC | |
|---|---|---|---|---|---|
| TRG ∈ [0, 1] | 13 (41%) | 0.70 ± 0.05 | 0.79 ± 0.07 | 0.74 ± 0.05 | 0.55 ± 0.09 |
| TRG ∈ [2, 3] | 19 (59%) | 0.84 ± 0.05 | 0.77 ± 0.05 | 0.80 ± 0.04 |
| Zhihui Li et al. (2021) [18] | The Authors’ Pipeline | |
|---|---|---|
| Number of patients | 80 patients | 39 patients |
| Segmentation | Manual | Automated |
| Radiomic pipeline |
|
|
| Area Under the Curve | AUC = [0.76, 0.93, 0.63, 0.84] * | AUC = 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filitto, G.; Coppola, F.; Curti, N.; Giampieri, E.; Dall'Olio, D.; Merlotti, A.; Cattabriga, A.; Cocozza, M.A.; Taninokuchi Tomassoni, M.; Remondini, D.; et al. Automated Prediction of the Response to Neoadjuvant Chemoradiotherapy in Patients Affected by Rectal Cancer. Cancers 2022, 14, 2231. https://doi.org/10.3390/cancers14092231
Filitto G, Coppola F, Curti N, Giampieri E, Dall'Olio D, Merlotti A, Cattabriga A, Cocozza MA, Taninokuchi Tomassoni M, Remondini D, et al. Automated Prediction of the Response to Neoadjuvant Chemoradiotherapy in Patients Affected by Rectal Cancer. Cancers. 2022; 14(9):2231. https://doi.org/10.3390/cancers14092231
Chicago/Turabian StyleFilitto, Giuseppe, Francesca Coppola, Nico Curti, Enrico Giampieri, Daniele Dall'Olio, Alessandra Merlotti, Arrigo Cattabriga, Maria Adriana Cocozza, Makoto Taninokuchi Tomassoni, Daniel Remondini, and et al. 2022. "Automated Prediction of the Response to Neoadjuvant Chemoradiotherapy in Patients Affected by Rectal Cancer" Cancers 14, no. 9: 2231. https://doi.org/10.3390/cancers14092231
APA StyleFilitto, G., Coppola, F., Curti, N., Giampieri, E., Dall'Olio, D., Merlotti, A., Cattabriga, A., Cocozza, M. A., Taninokuchi Tomassoni, M., Remondini, D., Pierotti, L., Strigari, L., Cuicchi, D., Guido, A., Rihawi, K., D'Errico, A., Di Fabio, F., Poggioli, G., Morganti, A. G., ... Castellani, G. (2022). Automated Prediction of the Response to Neoadjuvant Chemoradiotherapy in Patients Affected by Rectal Cancer. Cancers, 14(9), 2231. https://doi.org/10.3390/cancers14092231