
Prognostic Impact of EGFR Amplification and Visceral Pleural Invasion in Early Stage Pulmonary Squamous Cell Carcinomas Patients after Surgical Resection of Primary Tumor

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Tissue Microarray (TMA)
2.3. Immunohistochemistry
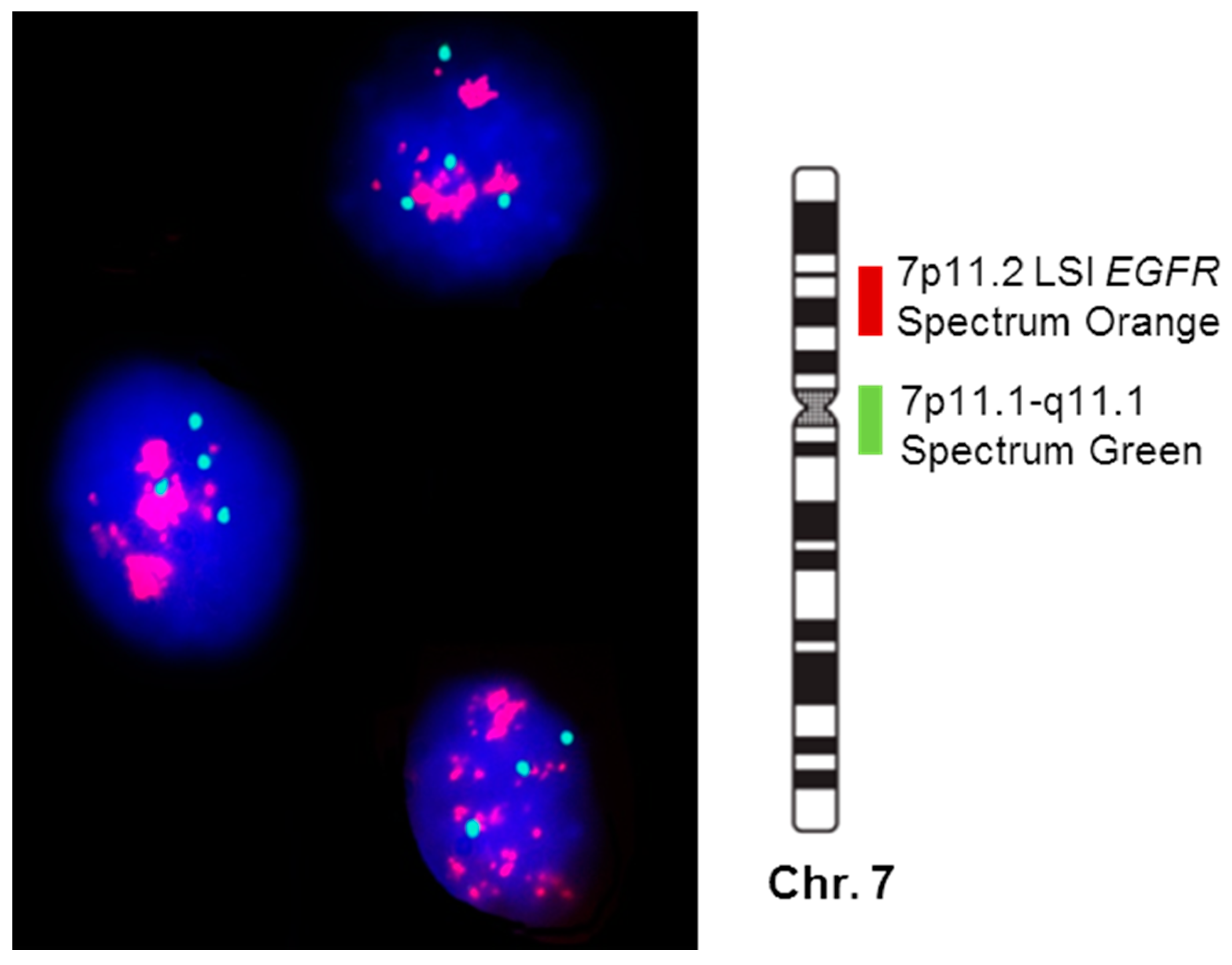
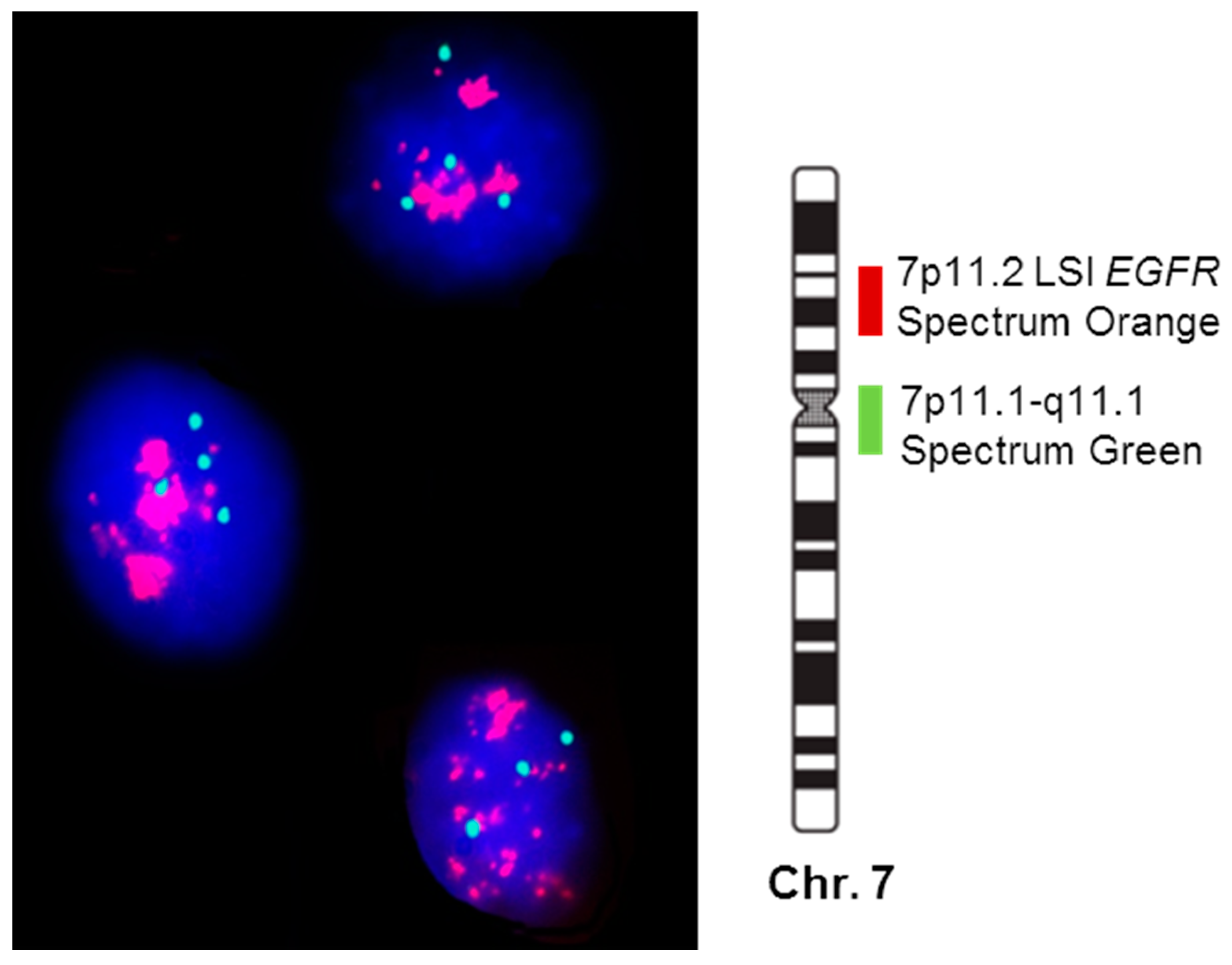
2.4. FISH Analysis
2.5. Statistical Analyses
3. Results
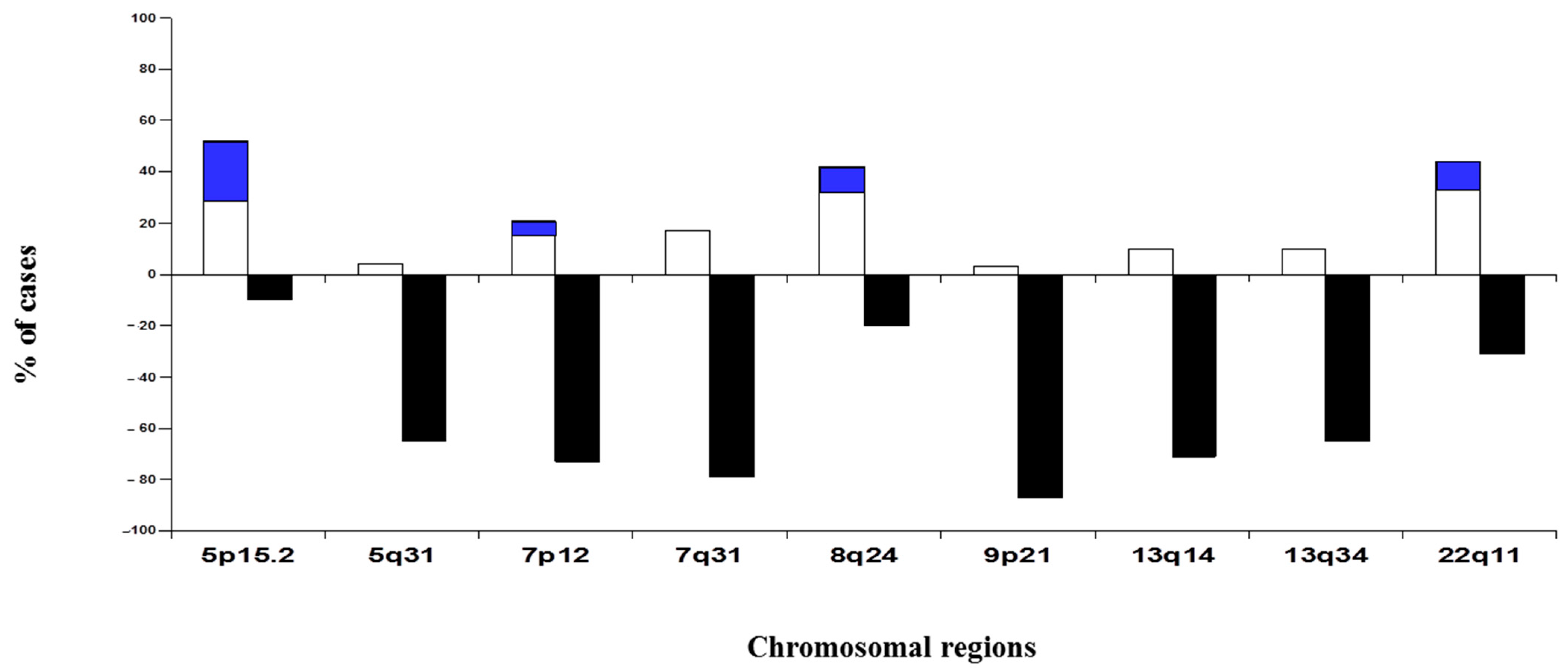
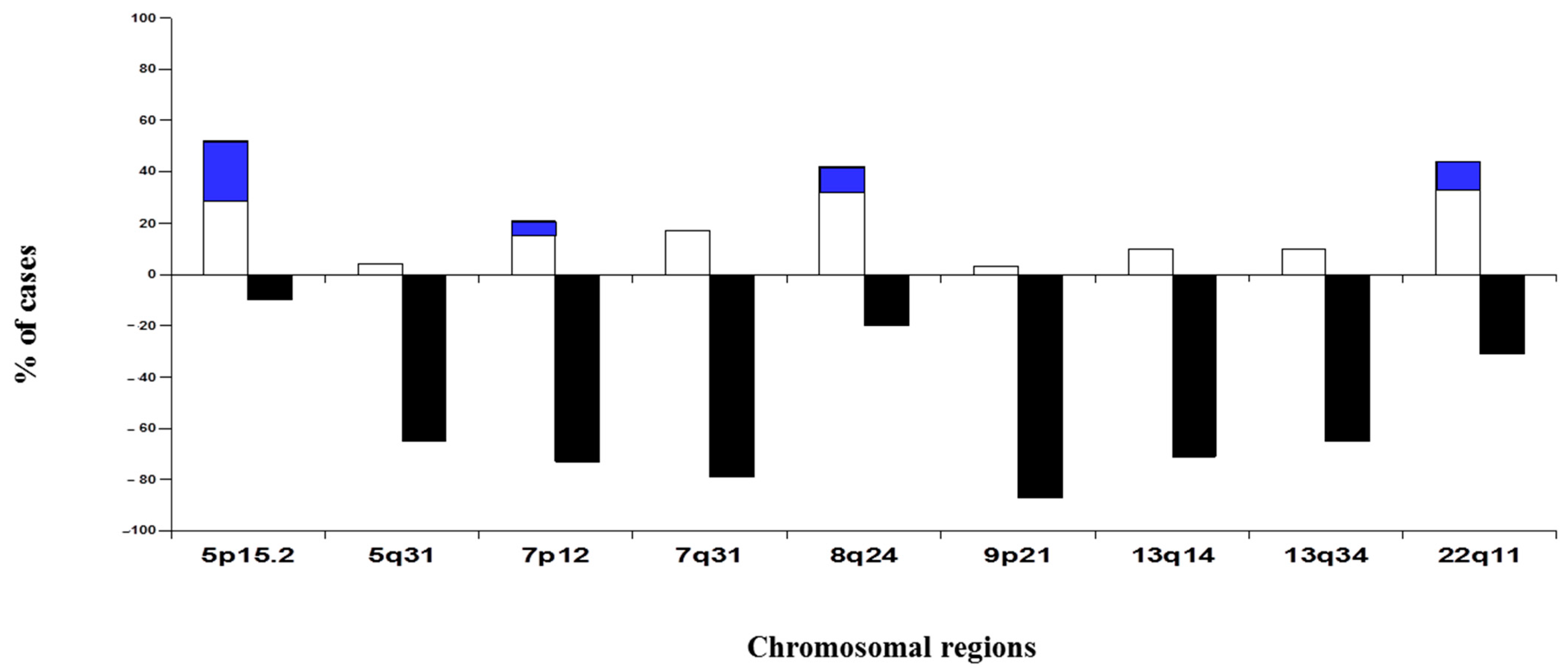
3.1. Chromosomal Alterations in SCC
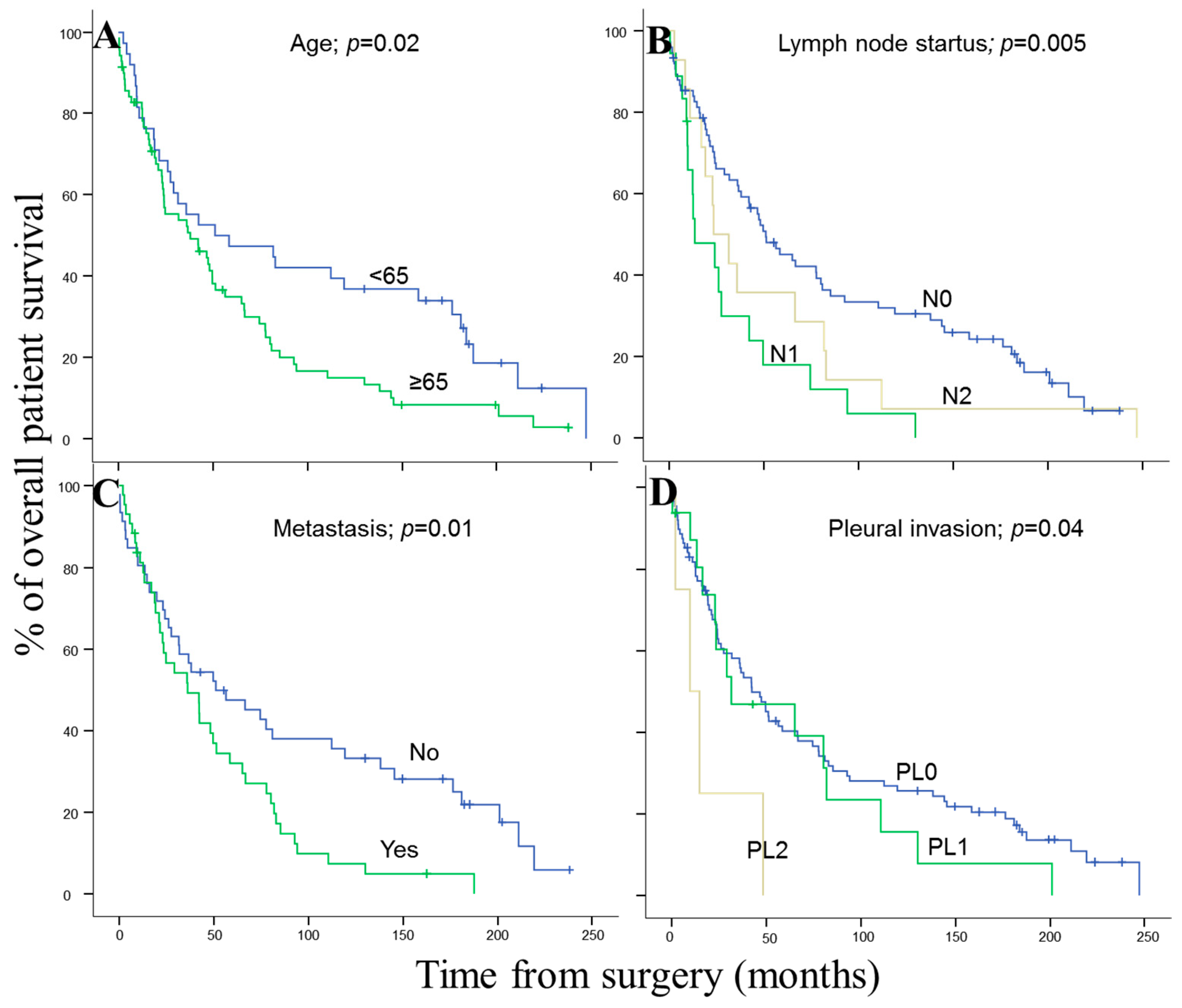
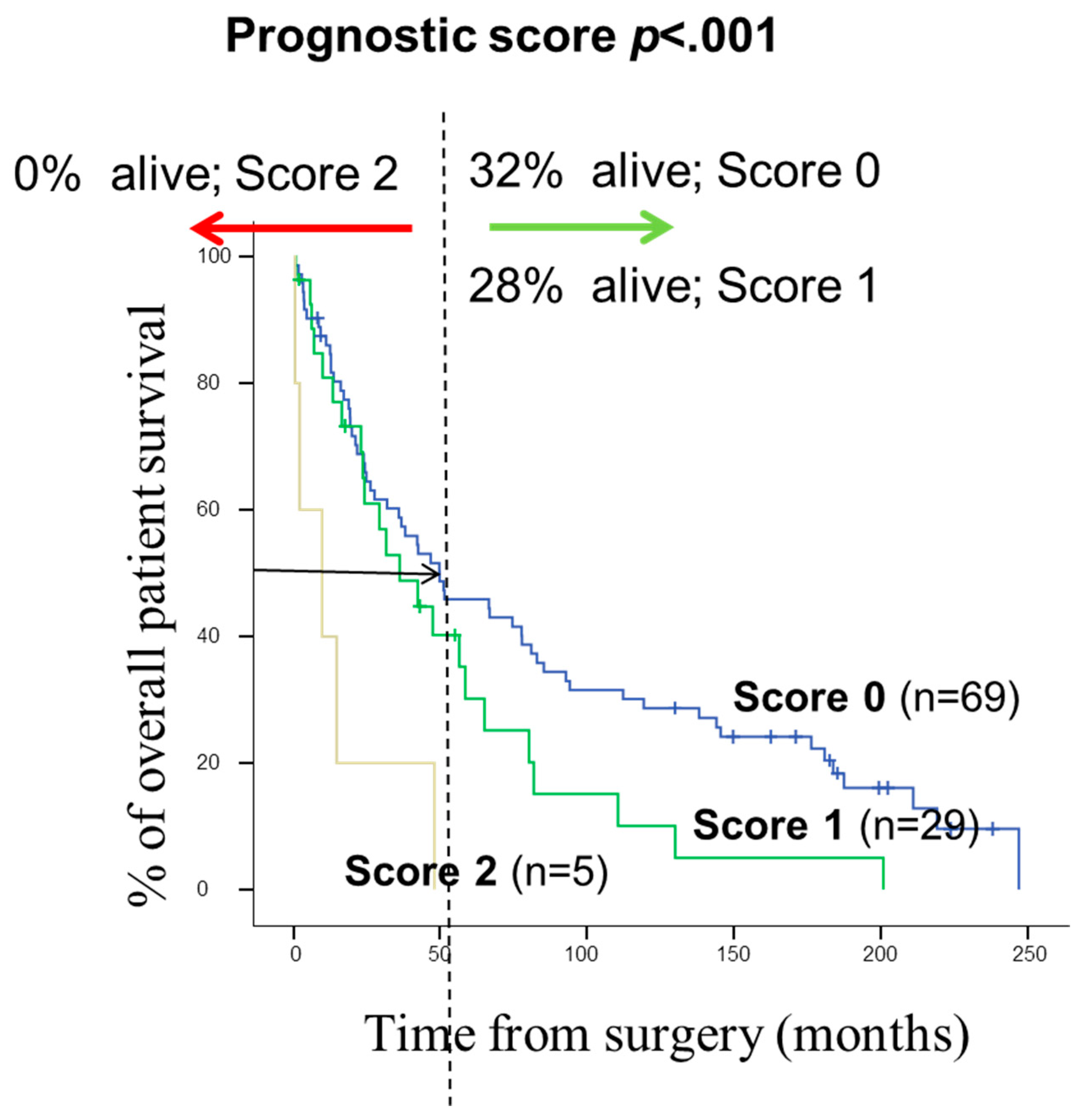
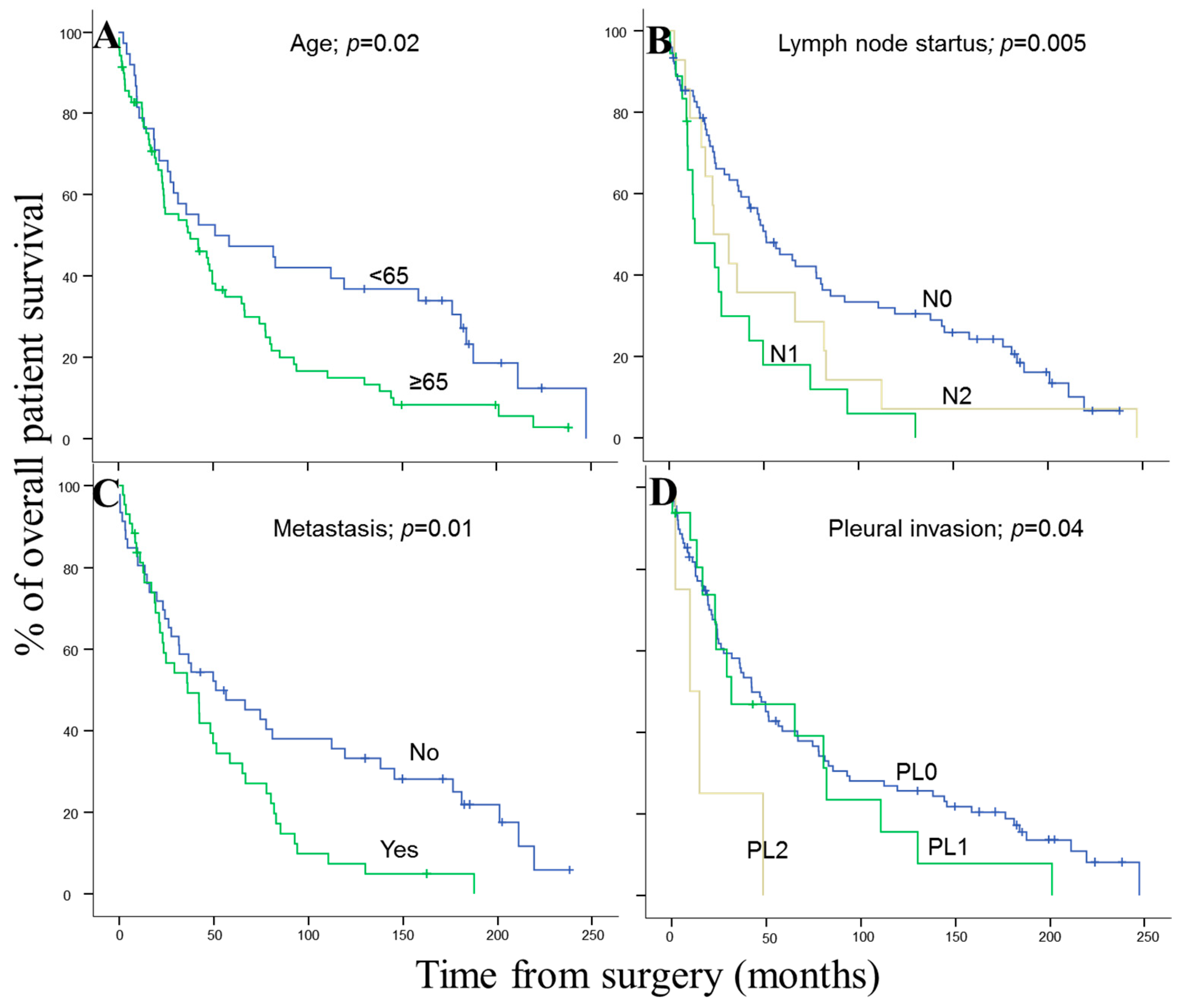
3.2. Prognostic Effect of Chromosomal Changes and Other Disease Features in SCC Patients
3.3. Clinical, Histopathological, and Biological Disease Characteristics of SCC Patients According to the Number of Copies of EGFR Gene Detected by FISH Techniques
3.4. EGFR Protein Expression and Copy Number
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Youlden, D.R.; Cramb, S.; Baade, P. The International Epidemiology of Lung Cancer: Geographical Distribution and Secular Trends. J. Thorac. Oncol. 2008, 3, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Imyanitov, E.N.; Iyevleva, A.G.; Levchenko, E.V. Molecular testing and targeted therapy for non-small cell lung cancer: Current status and perspectives. Crit. Rev. Oncol./Hematol. 2021, 157, 103194. [Google Scholar] [CrossRef] [PubMed]
- Kris, M.G.; Johnson, B.E.; Kwiatkowski, D.J.; Iafrate, A.J.; Wistuba, I.I.; Aronson, S.L.; Shyr, Y.; Khuri, F.R.; Rudin, C.M.; Garon, E.B.; et al. Identification of driver mutations in tumor specimens from 1,000 patients with lung adenocarcinoma: The NCI’s Lung Cancer Mutation Consortium (LCMC). J. Clin. Oncol. 2011, 29 (Suppl. 18), CRA7506. [Google Scholar] [CrossRef]
- Li, Y.; Gu, J.; Xu, F.; Zhu, Q.; Ge, D.; Lu, C. Transcriptomic and functional network features of lung squamous cell carcinoma through integrative analysis of GEO and TCGA data. Sci. Rep. 2018, 8, 15834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammerman, P.S.; Lawrence, M.S.; Voet, D.; Jing, R.; Cibulskis, K.; Sivachenko, A. Comprehensive genomic characterization of squamous cell lung cancers. Nature 2012, 489, 519–525. [Google Scholar]
- Lu, C.; Bera, K.; Wang, X.; Prasanna, P.; Xu, J.; Janowczyk, A.; Beig, N.; Yang, M.; Fu, P.; Lewis, J.; et al. A prognostic model for overall survival of patients with early-stage non-small cell lung cancer: A multicentre, retrospective study. Lancet Digit. Health 2020, 2, e594–e606. [Google Scholar] [CrossRef]
- López-Malpartida, A.V.; Ludeña, M.D.; Varela, G.; Pichel, J. Differential ErbB receptor expression and intracellular signaling activity in lung adenocarcinomas and squamous cell carcinomas. Lung Cancer 2009, 65, 25–33. [Google Scholar] [CrossRef]
- Han, B.; Tjulandin, S.; Hagiwara, K.; Normanno, N.; Wulandari, L.; Konstantinovich, L.K.; Hudoyo, A.; Ratcliffe, M.; McCormack, R.; Reck, M. Determining the Prevalence of EGFR Mutations in Asian and Russian Patients (PTS) with Advanced Non-Small-Cell Lung Cancer (ANSCLC) of Adenocarcinoma (ADC) and Non-Adc Histology: Ignite Study. Ann. Oncol. 2015, 26, i29–i30. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.U.; Koo, S.H.; Kwon, K.C.; Park, J.W.; Jung, S.S. Gain of the EGFR gene located on 7p12 is a frequent and early event in squamous cell carcinoma of the lung. Cancer Genet. Cytogenet. 2008, 184, 31–37. [Google Scholar] [CrossRef]
- Hirsch, F.R.; Redman, M.W.; Moon, J.; Agustoni, F.; Herbst, R.S.; Semrad, T.J.; Varella-Garcia, M.; Rivard, C.J.; Kelly, K.; Gandara, D.R.; et al. EGFR High Copy Number Together with High EGFR Protein Expression Predicts Improved Outcome for Cetuximab-based Therapy in Squamous Cell Lung Cancer: Analysis from swog s0819, a phase iii trial of chemotherapy with or without Cetuximab in Advanced NSCLC. Clin. Lung Cancer 2021, 1, 60–71. [Google Scholar] [CrossRef]
- Cappuzzo, F.; Hirsch, F.R.; Rossi, E.; Bartolini, S.; Ceresoli, G.L.; Bemis, L.; Haney, J.; Witta, S.; Danenberg, K.; Domenichini, I.; et al. Epidermal Growth Factor Receptor Gene and Protein and Gefitinib Sensitivity in Non–Small-Cell Lung Cancer. JNCI: J. Natl. Cancer Inst. 2005, 97, 643–655. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Okamura, R.; Mareboina, M.; Lee, S.; Goodman, A.; Patel, S.P.; Fanta, P.T.; Schwab, R.B.; Vu, P.; Raymond, V.M.; et al. Revisiting Epidermal Growth Factor Receptor (EGFR) Amplification as a Target for Anti-EGFR Therapy: Analysis of Cell-Free Circulating Tumor DNA in Patients with Advanced Malignancies. JCO Precis. Oncol. 2019, 3, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Liu, J.J.; Zhao, H. Correlation of EGFR gene amplification with invasion and metastasis of non-small cell lung cancer. Genet. Mol. Res. 2015, 14, 11006–11012. [Google Scholar] [CrossRef] [PubMed]
- Iida, K.; Nakayama, K.; Rahman, M.; Ishikawa, M.; Katagiri, A.; Yeasmin, S.; Otsuki, Y.; Kobayashi, H.; Miyazaki, K. EGFR gene amplification is related to adverse clinical outcomes in cervical squamous cell carcinoma, making the EGFR pathway a novel therapeutic target. Br. J. Cancer 2011, 105, 420–427. [Google Scholar] [CrossRef]
- Huang, S.-F.; Chien, H.-T.; Cheng, S.-D.; Chuang, W.-Y.; Liao, C.-T.; Wang, H.-M. EGFR copy number alterations in primary tumors, metastatic lymph nodes, and recurrent and multiple primary tumors in oral cavity squamous cell carcinoma. BMC Cancer 2017, 17, 592. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zhang, B.; Sun, Z. Spectrum of EGFR aberrations and potential clinical implications: Insights from integrative pan-cancer analysis. Cancer Commun. 2020, 40, 43–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, G.; Sun, X.-J.; Han, Q.-B.; Wang, Z.; Xu, Y.-P.; Gu, J.-L.; Wu, W.; Zhang, G.; Hu, J.-L.; Sun, W.-Y.; et al. Epidermal growth factor receptor protein overexpression and gene amplification are associated with aggressive biological behaviors of esophageal squamous cell carcinoma. Oncol. Lett. 2015, 10, 901–906. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Burke, A.; Nicholson, A.G. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th ed.; IARC Press: Lyon, France, 2015; p. 412. [Google Scholar]
- WHO. Classification of Tumours Editorial Board. In Thoracic Tumours, 5th ed.; IARC Press: Lyon, France, 2021; Volume 5, p. 500. [Google Scholar]
- Boelens, M.C.; Kok, K.; van der Vlies, P.; van der Vries, G.; Sietsma, H.; Timens, W.; Postma, D.S.; Groen, H.J.; Berg, A.V.D. Genomic aberrations in squamous cell lung carcinoma related to lymph node or distant metastasis. Lung Cancer 2009, 66, 372–378. [Google Scholar] [CrossRef]
- Rotolo, F.; Zhu, C.-Q.; Brambilla, E.; Graziano, S.L.; Olaussen, K.; Le-Chevalier, T.; Pignon, J.-P.; Robert Kratzke, R.; Soria, J.-C.; Shepherd, F.A.; et al. Genome-wide copy number analyses of samples from LACE-Bio project identify novel prognostic and predictive markers in early stage non-small cell lung cancer. Transl. Lung Cancer Res. 2018, 7, 416–427. Available online: https://tlcr.amegroups.com/article/view/21273. (accessed on 1 May 2018). [CrossRef]
- Yan, W.-S.; Song, L.-Y.; Wei, W.-D.; Li, A.; Liang, Q.-W.; Liu, J.-H.; Fang, Y. Chromosomal imbalance in primary lung squamous cell carcinoma and their relationship with smoking. Chin. J. Cancer 2005, 24, 47–52. [Google Scholar]
- Kang, J.U.; Koo, S.H.; Kwon, K.C.; Park, J.W.; Kim, J.M. Gain at chromosomal region 5p15.33, containing TERT, is the most frequent genetic event in early stages of non-small cell lung cancer. Cancer Genet. Cytogenet. 2008, 182, 1–11. [Google Scholar] [CrossRef]
- Guo, Y.; Song, J.; Wang, Y.; Huang, L.; Sun, L.; Zhao, J.; Zhang, S.; Jing, W.; Ma, J.; Han, C.; et al. Concurrent Genetic Alterations and Other Biomarkers Predict Treatment Efficacy of EGFR-TKIs in EGFR-Mutant Non-Small Cell Lung Cancer: A Review. Front. Oncol. 2020, 10, 610923. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, F.R.; Varella-Garcia, M.; Bunn, P.A., Jr.; Di Maria, M.V.; Veve, R.; Bremnes, R.M.; Barón, A.E.; Zeng, C.; Franklin, W.A. Epidermal Growth Factor Receptor in Non–Small-Cell Lung Carcinomas: Correlation Between Gene Copy Number and Protein Expression and Impact on Prognosis. J. Clin. Oncol. 2003, 21, 3798–3807. [Google Scholar] [CrossRef] [PubMed]
- Dacic, S.; Flanagan, M.; Cieply, K.; Ramalingam, S.; Luketich, J.; Belani, C.; Yousem, S.A. Significance of EGFR Protein Expression and Gene Amplification in Non–Small Cell Lung Carcinoma. Am. J. Clin. Pathol. 2006, 25, 860–865. [Google Scholar] [CrossRef]
- The AACR Project GENIE Consortium; André, F.; Arnedos, M.; Baras, A.S.; Baselga, J. AACR Project GENIE: Powering Precision Medicine through an International Consortium. Cancer Discov. 2017, 7, 818–831. [Google Scholar]
- Tuna, M.; Amos, C.I.; Mills, G.B. Whole-chromosome arm acquired uniparental disomy in cancer development is a consequence of isochromosome formation. Neoplasia 2022, 25, 9–17. [Google Scholar] [CrossRef]
- Sasaki, H.; Shitara, M.; Yokota, K.; Hikosaka, Y.; Moriyama, S.; Yano, M.; Fujii, Y. Increased FGFR1 copy number in lung squamous cell carcinomas. Mol. Med. Rep. 2011, 5, 725–728. [Google Scholar] [CrossRef]
- Lee, E.; Moon, J.W.; Wang, X.; Kim, C.; Li, S.; Shin, B.K.; Jung, W.; Kim, H.K.; Kim, H.K.; Lee, J.-Y. Genomic Copy Number Signatures Uncovered a Genetically Distinct Group from Adenocarcinoma and Squamous Cell Carcinoma in Non–Small Cell Lung Cancer. Hum. Pathol. 2015, 46, 1111–1120. [Google Scholar] [CrossRef]
- Craddock, K.J.; Lam, W.L.; Tsao, M.-S. Applications of Array-CGH for Lung Cancer. Methods Pharmacol. Toxicol. 2013, 973, 297–324. [Google Scholar] [CrossRef]
- Mapping of Genetic Abnormalities of Primary Tumours from Metastatic CRC by High-Resolution SNP Arrays. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0013752 (accessed on 4 March 2022).
- Fu, X.; Lei, H.; Tao, Y.; Heselmeyer-Haddad, K.; Torres, I.; Dean, M.; Ried, T.; Schwartz, R. Joint Clustering of Single-Cell Sequencing and Fluorescence In Situ Hybridization Data for Reconstructing Clonal Heterogeneity in Cancers. J. Comput. Biol. 2021, 28, 1035–1051. [Google Scholar] [CrossRef]
- Sayagués, J.M.; Abad, M.D.M.; Melchor, H.B.; Gutiérrez, M.L.; González-González, M.; Jensen, E.; Bengoechea, O.; Fonseca, E.; Orfao, P.A.; Muñoz-Bellvis, L. Intratumoural cytogenetic heterogeneity of sporadic colorectal carcinomas suggests several pathways to liver metastasis. J. Pathol. 2010, 221, 308–319. [Google Scholar] [CrossRef]
- Jiang, D.; Li, X.; Wang, H.; Shi, Y.; Xu, C.; Lu, S.; Huang, J.; Xu, Y.; Zeng, H.; Su, J.; et al. The prognostic value of EGFR overexpression and amplification in Esophageal squamous cell Carcinoma. BMC Cancer 2015, 15, 377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, H.-T.; Cheng, S.-D.; Liao, C.-T.; Wang, H.-M.; Huang, S.-F. Amplification of the EGFR and CCND1 Are Coordinated and Play Important Roles in the Progression of Oral Squamous Cell Carcinomas. Cancers 2019, 11, 760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Gao, C.; Du, Q.; Tang, L.; You, H.; Dong, Y. A prognostic model for elderly patients with squamous non-small cell lung cancer: A population-based study. J. Transl. Med. 2020, 18, 436. [Google Scholar] [CrossRef] [PubMed]
- Tas, F.; Ciftci, R.; Kilic, L.; Karabulut, S. Age is a prognostic factor affecting survival in lung cancer patients. Oncol. Lett. 2013, 6, 1507–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McWilliam, A.; Osorio, E.V.; Faivre-Finn, C.; van Herk, M. Influence of tumour laterality on patient survival in non-small cell lung cancer after radiotherapy. Radiother. Oncol. 2019, 137, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Dahabreh, I.J.; Linardou, H.; Kosmidis, P.; Bafaloukos, D.; Murray, S. EGFR gene copy number as a predictive biomarker for patients receiving tyrosine kinase inhibitor treatment: A systematic review and meta-analysis in non-small-cell lung cancer. Ann. Oncol. 2011, 22, 545–552. [Google Scholar] [CrossRef]
- Wang, F.; Fu, S.; Shao, Q.; Zhou, Y.-B.; Zhang, X.; Zhang, X.; Xue, C.; Lin, J.-G.; Huang, L.-X.; Zhang, L.; et al. High EGFR copy number predicts benefits from tyrosine kinase inhibitor treatment for non-small cell lung cancer patients with wild-type EGFR. J. Transl. Med. 2013, 11, 90. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, F.R.; Herbst, R.S.; Olsen, C.; Chansky, K.; Crowley, J.; Kelly, K.; Gandara, D.R. Increased EGFR Gene Copy Number Detected by Fluorescent In Situ Hybridization Predicts Outcome in Non–Small-Cell Lung Cancer Patients Treated with Cetuximab and Chemotherapy. J. Clin. Oncol. 2008, 26, 3351–3357. [Google Scholar] [CrossRef] [Green Version]
- Zhu, C.-Q.; da Cunha Santos, G.; Ding, K.; Sakurada, A.; Cutz, J.-C.; Liu, N.; Tsao, M.S. Role of KRAS and EGFR As Biomarkers of Response to Erlotinib in National Cancer Institute of Canada Clinical Trials Group Study BR.21. J. Clin. Oncol. 2008, 26, 4268–4275. [Google Scholar] [CrossRef]
- Hirsch, F.R.; Varella-Garcia, M.; Bunn, P.A.; Franklin, W.A.; Dziadziuszko, R.; Thatcher, N.; Chang, A.; Parikh, P.; Pereira, J.R.; Ciuleanu, T.E.; et al. Molecular Predictors of Outcome with Gefitinib in a Phase III Placebo-Controlled Study in Advanced Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2006, 24, 5034–5042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Zhang, Y.; Tang, H.; He, J. EGFR gene copy number as a predictive/biomarker for patients with non-small-cell lung cancer receiving tyrosine kinase inhibitor treatment: A systematic review and meta-analysis. J. Investig. Med. 2016, 65, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Kim, H.S.; Bae, Y.S.; Cheong, J.-H.; Rha, S.Y.; Noh, S.H.; Kim, H. Prognostic significance and frequency of EGFR expression and amplification in surgically resected advanced gastric cancer. Jpn. J. Clin. Oncol. 2016, 46, 507–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, K.; Yoshida, J.; Nagai, K.; Nishimura, M.; Ishii, G.; Morishita, Y.; Nishiwaki, Y. Visceral pleural invasion is an invasive and aggressive indicator of non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2005, 130, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Zhou, C.; Zhou, Q. Extent of Visceral Pleural Invasion Affects Prognosis of Resected Non-small Cell Lung Cancer: A meta-analysis. Sci. Rep. 2017, 7, 1527. [Google Scholar] [CrossRef] [PubMed]
- Heist, R.S.; Sequist, L.V.; Engelman, J.A. Genetic Changes in Squamous Cell Lung Cancer: A Review. J. Thorac. Oncol. 2012, 7, 924–933. [Google Scholar] [CrossRef] [Green Version]
- Friedlaender, A.; Banna, G.; Malapelle, U.; Pisapia, P.; Addeo, A. Next Generation Sequencing and Genetic Alterations in Squamous Cell Lung Carcinoma: Where Are We Today? Front. Oncol. 2019, 9, 166. [Google Scholar] [CrossRef] [Green Version]
- Stapelfeld, C.; Dammann, C.; Maser, E. Sex-specificity in lung cancer risk. Int. J. Cancer 2020, 146, 2376–2382. [Google Scholar] [CrossRef]
- Pesch, B.; Kendzia, B.; Gustavsson, P.; Jöckel, K.-H.; Johnen, G.; Pohlabeln, H.; Olsson, A.; Ahrens, W.; Gross, I.M.; Brüske, I.; et al. Cigarette smoking and lung cancer-relative risk estimates for the major histological types from a pooled analysis of case-control studies. Int. J. Cancer 2012, 131, 1210–1219. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N° of Cases (%) | Median OS, (Months) | p |
|---|---|---|---|
| Gender | |||
| Male | 47 (98) | 42 | NS |
| Female | 1 (2) | 18 | |
| Age | |||
| <65 | 16 (33) | 26 | NS |
| ≥65 | 32 (67) | 42 | |
| T-primary tumor stage | |||
| pT1–pT2 | 36 (75) | 59 | 0.001 |
| pT3–pT4 | 12 (25) | 22 | |
| Lymph node status | |||
| pN0 | 35 (73) | 42 | NS |
| pN1 | 8 (17) | 25 | |
| pN2 | 5 (10) | 39 | |
| pN3 | 0 (0) | 0 | |
| Pleural invasion | |||
| PL0 | 39 | 42 | NS |
| PL1 | 6 | 23 | |
| PL2 | 3 | 15 | |
| AJCC stage | |||
| I | 24 | 50 | |
| II | 14 | 26 | NS |
| III | 9 | 22 | |
| IV | 1 | 39 | |
| Type of surgery | |||
| R0 | 45 | 48 | 0.003 |
| R1 | 3 | 10 | |
| Local recurrence | |||
| No | 19 | 67 | 0.05 |
| Yes | 29 | 36 | |
| Metastasis | |||
| No | 26 | 52 | 0.05 |
| Yes | 22 | 39 |
| Chromosomal Region | Cases (%) | Median OS (Months) | p |
|---|---|---|---|
| Chr. 5p15.2 | |||
| Loss | 7 (10) | 81 | |
| Normal | 18 (38) | 48 | |
| Gain | 23 (52) | 42 | NS * |
| Polysomies | 13 (56) | 42 | |
| Amplified | 10 (44) | 42 | |
| Chr. 5q31 | |||
| Loss | 31 (65) | 31 | |
| Normal | 15 (31) | 50 | NS * |
| Gain * | 2 (4) | 36 | |
| Chr. 7p12 | |||
| Loss | 35 (73) | 24 | |
| Normal | 3 (6) | 42 | |
| Gain | 10 (21) | 36 | 0.02 |
| Polysomies | 5 (50) | 38 | |
| Amplified | 5 (50) | 32 | |
| Chr. 7q31 | |||
| Loss | 38 (79) | 31 | |
| Normal | 2 (4) | 49 | NS * |
| Gain * | 8 (17) | 58 | |
| Chr. 8q24 | |||
| Loss | 10 (20) | 25 | |
| Normal | 18 (38) | 31 | |
| Gain | 20 (42) | 42 | NS * |
| Polysomies | 16 (80) | 42 | |
| Amplified | 4 (20) | 42 | |
| Chr. 9p21.1 | |||
| Loss | 42 (87) | 36 | |
| Normal | 5 (10) | 36 | NS * |
| Gain * | 1 (3) | 42 | |
| Chr. 13q14 | |||
| Loss | 34 (71) | 49 | |
| Normal | 9 (19) | 55 | NS * |
| Gain * | 5 (10) | 49 | |
| Chr. 13q34 | |||
| Loss | 31 (65) | 42 | |
| Normal | 12 (25) | 55 | NS * |
| Gain * | 5 (10) | 49 | |
| Chr. 22q11 | |||
| Loss | 15 (31) | 74 | |
| Normal | 12 (25) | 31 | |
| Gain | 21 (44) | 26 | 0.09 |
| Polysomies | 17 (80) | 26 | |
| Amplified | 4 (20) | 14 |
| Characteristic | No. Patients [n (%)] Amplified EGFR | Total of Cases (n = 108) | ||
|---|---|---|---|---|
| Yes (n = 13) | No (n = 95) | p | ||
| Gender | ||||
| Male | 12 (92) | 93 (97) | NS | 105 (97) |
| Female | 1 (8) | 2 (3) | 3 (3) | |
| Age (years) | ||||
| <65 | 2 (15) | 35 (37) | 0.07 | 37 (34) |
| >65 | 11 (85) | 60 (63) | 71 (66) | |
| Tumor location | ||||
| Right upper lobe | 5 (38) | 28 (30) | NS | 33 (31) |
| Middle lobe | 1 (8) | 5 (5) | 6 (5) | |
| Right lower lobe | 4 (31) | 15 (16) | 19 (18) | |
| Left upper lobe | 2 (15) | 20 (21) | 22 (20) | |
| Left lower lobe | 1 (8) | 27 (28) | 28 (26) | |
| Tumor laterality | ||||
| Right | 10 (77) | 48 (51) | 0.05 | 58 (54) |
| Left | 3 (33) | 47 (49) | 50 (46) | |
| T-primary tumor stage | ||||
| pT1–pT2 | 13 (100) | 72 (76) | 0.03 | 85 (79) |
| pT3–pT4 | 0 (0) | 23 (24) | 23 (21) | |
| Lymph node status | ||||
| pN0 | 10 (77) | 66 (69) | NS | 76 (70) |
| pN1 | 3 (23) | 15 (16) | 18 (17) | |
| pN2 | 0 (0) | 14 (15) | 14 (13) | |
| pN3 | 0 (0) | 0 (0) | 0 (0) | |
| Pleural invasion | ||||
| pL0 | 12 (92) | 74 (89) | NS | 86 (80) |
| pL1 | 1 (8) | 17 (18) | 18 (17) | |
| pL2 | 0 (0) | 4 (4) | 4 (3) | |
| AJCC stage | ||||
| I | 7 (53) | 45 (47) | NS | 52 (48) |
| II | 6 (47) | 29 (30) | 35 (32) | |
| III | 0 (0) | 19 (20) | 19 (18) | |
| IV | 0 (0) | 2 (3) | 2 (2) | |
| Local recurrence | ||||
| No | 3 (33) | 27 (35) | NS | 30 (34) |
| Yes | 6 (76) | 51 (65) | 57 (66) | |
| Metastasis | ||||
| No | 3 (37) | 39 (50) | NS | 42 (49) |
| Yes | 5 (63) | 39 (50) | 44 (51) | |
| Exitus | ||||
| No | 2 (15) | 14 (15) | NS | 16 (15) |
| Yes | 11 (85) | 78 (85) | 89 (85) | |
| OS (months) | 36 (1.2–82.6) | 48 (32.7–63.6) | <0.001 | 47 (26.3–58.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chinchilla-Tábora, L.M.; Sayagués, J.M.; González-Morais, I.; Rodríguez, M.; Ludeña, M.D. Prognostic Impact of EGFR Amplification and Visceral Pleural Invasion in Early Stage Pulmonary Squamous Cell Carcinomas Patients after Surgical Resection of Primary Tumor. Cancers 2022, 14, 2174. https://doi.org/10.3390/cancers14092174
Chinchilla-Tábora LM, Sayagués JM, González-Morais I, Rodríguez M, Ludeña MD. Prognostic Impact of EGFR Amplification and Visceral Pleural Invasion in Early Stage Pulmonary Squamous Cell Carcinomas Patients after Surgical Resection of Primary Tumor. Cancers. 2022; 14(9):2174. https://doi.org/10.3390/cancers14092174
Chicago/Turabian StyleChinchilla-Tábora, Luís Miguel, José María Sayagués, Idalia González-Morais, Marta Rodríguez, and María Dolores Ludeña. 2022. "Prognostic Impact of EGFR Amplification and Visceral Pleural Invasion in Early Stage Pulmonary Squamous Cell Carcinomas Patients after Surgical Resection of Primary Tumor" Cancers 14, no. 9: 2174. https://doi.org/10.3390/cancers14092174
APA StyleChinchilla-Tábora, L. M., Sayagués, J. M., González-Morais, I., Rodríguez, M., & Ludeña, M. D. (2022). Prognostic Impact of EGFR Amplification and Visceral Pleural Invasion in Early Stage Pulmonary Squamous Cell Carcinomas Patients after Surgical Resection of Primary Tumor. Cancers, 14(9), 2174. https://doi.org/10.3390/cancers14092174