
Fear of Recurrence in Young Adult Cancer Patients—A Network Analysis

Abstract
:Simple Summary
Abstract
1. Introduction
- What is the prevalence of FCR in a German sample of young adult cancer patients?
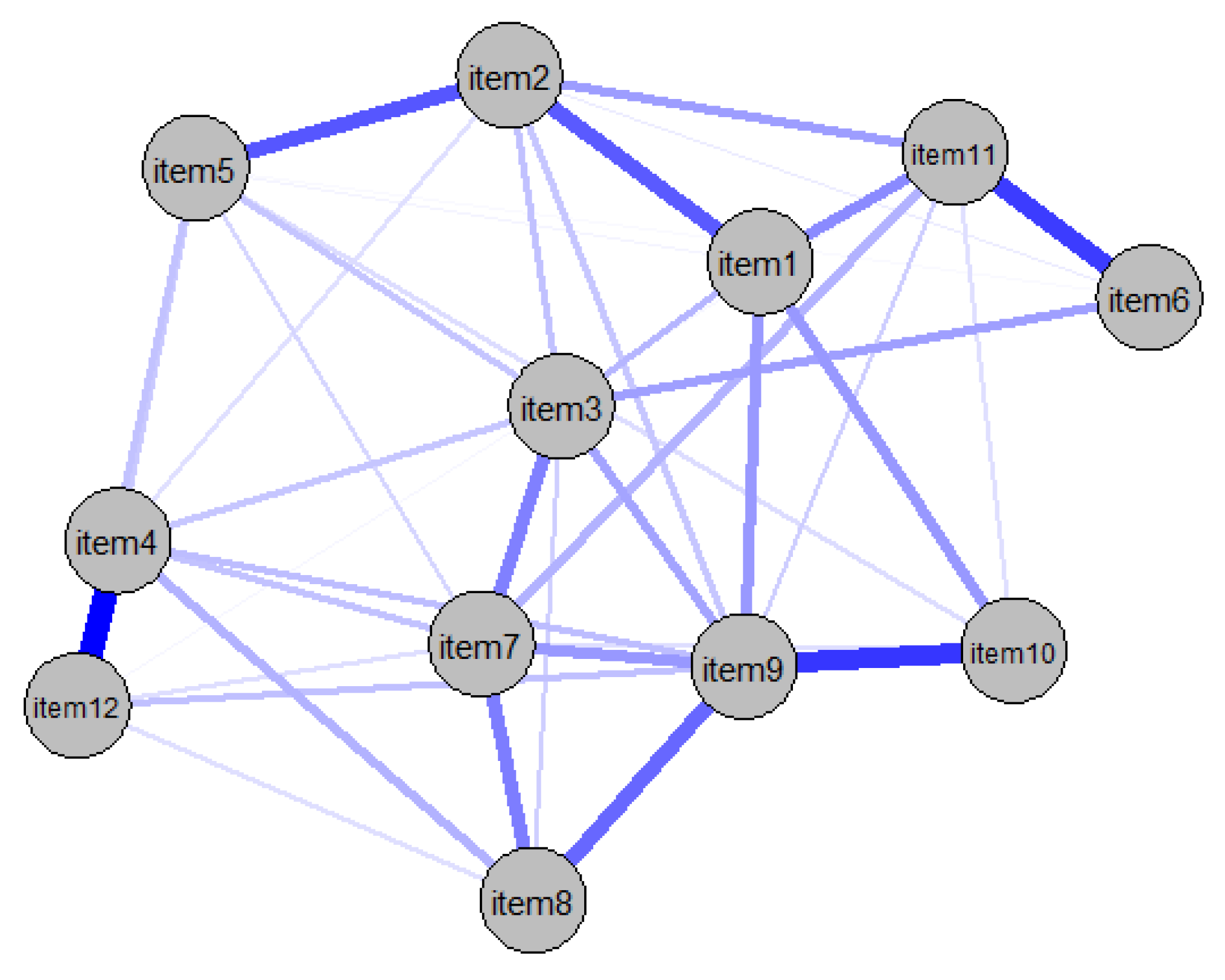
- What are the most important symptoms in the network of FCR symptoms?
- How are these symptoms related to one another?
2. Materials and Methods
2.1. Data Collection
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Participants
3.2. Prevalence of FCR
3.3. Network Estimation
3.4. Network Centrality and Stability
4. Discussion
4.1. General Results
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Butow, P.; Sharpe, L.; Thewes, B.; Turner, J.; Gilchrist, J.; Beith, J. Fear of Cancer Recurrence: A Practical Guide for Clinicians. Oncology 2018, 32, 32–38. [Google Scholar] [PubMed]
- Hodges, L.J.; Humphris, G.M. Fear of recurrence and psychological distress in head and neck cancer patients and their carers. Psychooncology 2009, 18, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Vickberg, S.M.J. The Concerns About Recurrence Scale (CARS): A systematic measure of women’s fears about the possibility of breast cancer recurrence. Ann. Behav. Med. 2003, 25, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Dankert, A.; Duran, G.; Engst-Hastreiter, U.; Keller, M.; Waadt, S.; Henrich, G.; Herschbach, P. Fear of progression in patients with cancer, diabetes mellitus and chronic arthritis. Rehabilitation 2003, 42, 155–163. [Google Scholar] [CrossRef]
- Hall, D.L.; Jimenez, R.B.; Perez, G.K.; Rabin, J.; Quain, K.; Yeh, G.Y.; Park, E.R.; Peppercorn, J.M. Fear of Cancer Recurrence: A Model Examination of Physical Symptoms, Emotional Distress, and Health Behavior Change. J. Oncol. Pract. 2019, 15, e787–e797. [Google Scholar] [CrossRef]
- Vachon, E.; Krueger, E.; Champion, V.L.; Haggstrom, D.A.; Cella, D.; Cohee, A.A. The impact of fear of cancer recurrence on healthcare utilization among long-term breast cancer survivors recruited through ECOG-ACRIN trials. Psychooncology 2021, 30, 279–286. [Google Scholar] [CrossRef]
- Krok-Schoen, J.L.; Naughton, M.J.; Bernardo, B.M.; Young, G.S.; Paskett, E.D. Fear of recurrence among older breast, ovarian, endometrial, and colorectal cancer survivors: Findings from the WHI LILAC study. Psychooncology 2018, 27, 1810–1815. [Google Scholar] [CrossRef]
- Lebel, S.; Mutsaers, B.; Tomei, C.; Leclair, C.S.; Jones, G.; Petricone-Westwood, D.; Rutkowski, N.; Ta, V.; Trudel, G.; Laflamme, S.Z.; et al. Health anxiety and illness-related fears across diverse chronic illnesses: A systematic review on conceptualization, measurement, prevalence, course, and correlates. PLoS ONE 2020, 15, e0234124. [Google Scholar] [CrossRef]
- Simard, S.; Thewes, B.; Humphris, G.; Dixon, M.; Hayden, C.; Mireskandari, S.; Ozakinci, G. Fear of cancer recurrence in adult cancer survivors: A systematic review of quantitative studies. J. Cancer Surviv. 2013, 7, 300–322. [Google Scholar] [CrossRef]
- Jones, J.M.; Fitch, M.; Bongard, J.; Maganti, M.; Gupta, A.; D’Agostino, N.; Korenblum, C. The Needs and Experiences of Post-Treatment Adolescent and Young Adult Cancer Survivors. J. Clin. Med. 2020, 9, 1444. [Google Scholar] [CrossRef]
- Adams, S.C.; Petrella, A.; Sabiston, C.M.; Vani, M.F.; Gupta, A.; Trinh, L.; Matthew, A.G.; Hamilton, R.J.; Mina, D.S. Preferences for exercise and physical activity support in adolescent and young adult cancer survivors: A cross-sectional survey. Supportive Care Cancer 2021, 29, 4113–4127. [Google Scholar] [CrossRef] [PubMed]
- Dewar, E.O.; Ahn, C.; Eraj, S.; Mahal, B.A.; Sanford, N.N. Psychological distress and cognition among long-term survivors of adolescent and young adult cancer in the USA. J. Cancer Surviv. 2021, 15, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Fidler, M.M.; Frobisher, C.; Hawkins, M.M.; Nathan, P.C. Challenges and opportunities in the care of survivors of adolescent and young adult cancers. Pediatr. Blood Cancer 2019, 66, e27668. [Google Scholar] [CrossRef] [PubMed]
- Keegan, T.H.M.; Parsons, H.M. Adolescent angst: Enrollment on clinical trials. Hematol. Am. Soc. Hematol. Educ. Program 2018, 2018, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; DuBois, S.G.; Coccia, P.F.; Bleyer, A.; Olin, R.L.; Goldsby, R.E. Increased risk of second malignant neoplasms in adolescents and young adults with cancer. Cancer 2016, 122, 116–123. [Google Scholar] [CrossRef]
- Chao, C.; Bhatia, S.; Xu, L.; Cannavale, K.L.; Wong, F.L.; Huang, P.-Y.S.; Cooper, R.; Armenian, S.H. Incidence, Risk Factors, and Mortality Associated with Second Malignant Neoplasms among Survivors of Adolescent and Young Adult Cancer. JAMA Netw. Open 2019, 2, e195536. [Google Scholar] [CrossRef]
- Janssen, S.H.M.; van der Graaf, W.T.A.; van der Meer, D.J.; Manten-Horst, E.; Husson, O. Adolescent and Young Adult (AYA) Cancer Survivorship Practices: An Overview. Cancers 2021, 13, 4847. [Google Scholar] [CrossRef]
- Shaw, P.H.; Reed, D.R.; Yeager, N.; Zebrack, B.; Castellino, S.M.; Bleyer, A. Adolescent and Young Adult (AYA) Oncology in the United States: A Specialty in Its Late Adolescence. J. Pediatr. Hematol. Oncol. 2015, 37, 161–169. [Google Scholar] [CrossRef]
- Geue, K.; Göbel, P.; Leuteritz, K.; Nowe, E.; Sender, A.; Stöbel-Richter, Y.; Friedrich, M. Anxiety and depression in young adult German cancer patients: Time course and associated factors. Psycho-Oncol. 2019, 28, 2083–2090. [Google Scholar] [CrossRef]
- Quinn, G.P.; Gonçalves, V.; Sehovic, I.; Bowman, M.L.; Reed, D.R. Quality of life in adolescent and young adult cancer patients: A systematic review of the literature. Patient Relat. Outcome Meas. 2015, 6, 19–51. [Google Scholar] [CrossRef] [Green Version]
- Zebrack, B.; Kwak, M.; Salsman, J.; Cousino, M.; Meeske, K.; Aguilar, C.; Embry, L.; Block, R.; Hayes-Lattin, B.; Cole, S. The relationship between posttraumatic stress and posttraumatic growth among adolescent and young adult (AYA) cancer patients. Psychooncology 2015, 24, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Götze, H.; Taubenheim, S.; Dietz, A.; Lordick, F.; Mehnert-Theuerkauf, A. Fear of cancer recurrence across the survivorship trajectory: Results from a survey of adult long-term cancer survivors. Psychooncology 2019, 28, 2033–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, R.; Næss-Andresen, T.F.; Myklebust, T.Å.; Bernklev, T.; Kersten, H.; Haug, E.S. Fear of Recurrence in Prostate Cancer Patients: A Cross-sectional Study After Radical Prostatectomy or Active Surveillance. Eur. Urol. Open Sci. 2021, 25, 44–51. [Google Scholar] [CrossRef] [PubMed]
- van de Wal, M.; van Oort, I.; Schouten, J.; Thewes, B.; Gielissen, M.; Prins, J. Fear of cancer recurrence in prostate cancer survivors. Acta Oncol. 2016, 55, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.; Humphris, G. The relationship between fears of cancer recurrence and patient age: A systematic review and meta-analysis. Cancer Rep. 2020, 3, e1235. [Google Scholar] [CrossRef] [PubMed]
- Lane, B.E.; Garland, S.N.; Chalifour, K.; Eaton, G.; Lebel, S.; Galica, J.; Maheu, C.; Simard, S. Prevalence and factors associated with fear of recurrence in a mixed sample of young adults with cancer. J. Cancer Surviv. 2019, 13, 842–851. [Google Scholar] [CrossRef]
- Mattsson, E.; Einhorn, K.; Ljungman, L.; Sundström-Poromaa, I.; Stålberg, K.; Wikman, A. Women treated for gynaecological cancer during young adulthood—A mixed-methods study of perceived psychological distress and experiences of support from health care following end-of-treatment. Gynecol. Oncol. 2018, 149, 464–469. [Google Scholar] [CrossRef]
- Thewes, B.; Kaal, S.E.J.; Custers, J.A.E.; Manten-Horst, E.; Jansen, R.; Servaes, P.; van der Graaf, W.T.A.; Prins, J.B.; Husson, O. Prevalence and correlates of high fear of cancer recurrence in late adolescents and young adults consulting a specialist adolescent and young adult (AYA) cancer service. Supportive Care Cancer 2018, 26, 1479–1487. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Yang, Y.; Zhang, J.; Liu, T.; Wang, H.; Garg, S.; Zhang, B. Fear of cancer recurrence, anxiety and depressive symptoms in adolescent and young adult cancer patients. Neuropsychiatr. Dis. Treat. 2019, 15, 857–865. [Google Scholar] [CrossRef] [Green Version]
- Cho, D.; Park, C.L. Moderating effects of perceived growth on the association between fear of cancer recurrence and health-related quality of life among adolescent and young adult cancer survivors. J. Psychosoc. Oncol. 2017, 35, 148–165. [Google Scholar] [CrossRef]
- Yang, Y.; Li, W.; Wen, Y.; Wang, H.; Sun, H.; Liang, W.; Zhang, B.; Humphris, G. Fear of cancer recurrence in adolescent and young adult cancer survivors: A systematic review of the literature. Psychooncology 2019, 28, 675–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonelli, L.E.; Siegel, S.D.; Duffy, N.M. Fear of cancer recurrence: A theoretical review and its relevance for clinical presentation and management. Psychooncology 2017, 26, 1444–1454. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.B.; Costa, D.; Galica, J.; Lebel, S.; Tauber, N.; van Helmondt, S.J.; Zachariae, R. Spotlight on the Fear of Cancer Recurrence Inventory (FCRI). Psychol. Res. Behav. Manag. 2020, 13, 1257–1268. [Google Scholar] [CrossRef] [PubMed]
- Thewes, B.; Butow, P.; Zachariae, R.; Christensen, S.; Simard, S.; Gotay, C. Fear of cancer recurrence: A systematic literature review of self-report measures. Psychooncology 2012, 21, 571–587. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.; Kamphuis, H.; Sharpe, L.; Lebel, S.; Smith, A.B.; Hulbert-Williams, N.; Dhillon, H.M.; Butow, P. Setting an International Research Agenda for Fear of Cancer Recurrence: An Online Delphi Consensus Study. Front. Psychol. 2021, 12, 596682. [Google Scholar] [CrossRef] [PubMed]
- Gormley, M.; Ghazal, L.; Fu, M.R.; van Cleave, J.H.; Knobf, T.; Hammer, M. An Integrative Review on Factors Contributing to Fear of Cancer Recurrence Among Young Adult Breast Cancer Survivors. Cancer Nurs. 2022, 45, E10–E26. [Google Scholar] [CrossRef]
- Tauber, N.M.; O’Toole, M.S.; Dinkel, A.; Galica, J.; Humphris, G.; Lebel, S.; Maheu, C.; Ozakinci, G.; Prins, J.; Sharpe, L.; et al. Effect of Psychological Intervention on Fear of Cancer Recurrence: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2019, 37, 2899–2915. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef] [Green Version]
- Hartung, T.J.; Fried, E.I.; Mehnert, A.; Hinz, A.; Vehling, S. Frequency and network analysis of depressive symptoms in patients with cancer compared to the general population. J. Affect. Disord. 2019, 256, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Hevey, D. Network analysis: A brief overview and tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef] [Green Version]
- Mehnert, A.; Herschbach, P.; Berg, P.; Henrich, G.; Koch, U. Fear of progression in breast cancer patients--validation of the short form of the Fear of Progression Questionnaire (FoP-Q-SF). Z. Psychosom. Med. Psychother. 2006, 52, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Luz, J.K.; Martini, J.; Clever, K.; Herschbach, P.; Christiansen, H.; Schepper, F. Psychometrische Eigenschaften des Progredienzangst-Fragebogens für Kinder (FoP-Q-SF/C). Klin. Padiatr. 2020, 232, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Clever, K.; Schepper, F.; Maier, S.; Christiansen, H.; Martini, J. Individual and Dyadic Coping and Fear of Progression in Mothers and Fathers of Children with Hematologic Cancer. Fam. Process 2020, 59, 1225–1242. [Google Scholar] [CrossRef] [PubMed]
- Hanprasertpong, J.; Geater, A.; Jiamset, I.; Padungkul, L.; Hirunkajonpan, P.; Songhong, N. Fear of cancer recurrence and its predictors among cervical cancer survivors. J. Gynecol. Oncol. 2017, 28, e72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, S.; Scherwath, A.; Schirmer, L.; Schulz-Kindermann, F.; Neumann, K.; Kruse, M.; Dinkel, A.; Kunze, S.; Balck, F.; Kröger, N.; et al. Fear of recurrence and its impact on quality of life in patients with hematological cancers in the course of allogeneic hematopoietic SCT. Bone Marrow Transplant. 2014, 49, 1217–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herschbach, P.; Dinkel, A. Bewältigung chronischer Krankheiten. Was lindert die Progredienzangst? MMW Fortschr. Med. 2011, 153, 40–41. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H.; Grolemund, G. R for Data Science: Import, Tidy, Transform, Visualize, and Model Data; O’Reilly Media Inc.: Sebastopol, CA, USA, 2017; ISBN 9781491910368. [Google Scholar]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. qgraph: Network Visualizations of Relationships in Psychometric Data. J. Stat. Soft. 2012, 48, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.; Hastie, T.; Tibshirani, R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics 2008, 9, 432–441. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Chen, Z. Extended Bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef] [Green Version]
- McNally, R.J. Can network analysis transform psychopathology? Behav. Res. Ther. 2016, 86, 95–104. [Google Scholar] [CrossRef]
- Shay, L.A.; Carpentier, M.Y.; Vernon, S.W. Prevalence and correlates of fear of recurrence among adolescent and young adult versus older adult post-treatment cancer survivors. Supportive Care Cancer 2016, 24, 4689–4696. [Google Scholar] [CrossRef] [PubMed]
- Maheu, C.; Singh, M.; Tock, W.L.; Eyrenci, A.; Galica, J.; Hébert, M.; Frati, F.; Estapé, T. Fear of Cancer Recurrence, Health Anxiety, Worry, and Uncertainty: A Scoping Review About Their Conceptualization and Measurement Within Breast Cancer Survivorship Research. Front. Psychol. 2021, 12, 644932. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, C.E.; Fardell, J.E.; Doolan, E.L.; Aaronson, N.K.; Jacobsen, P.B.; Cohn, R.J.; King, M. Participation in psychosocial oncology and quality-of-life research: A systematic review. Lancet Oncol. 2017, 18, e153–e165. [Google Scholar] [CrossRef]
- Clover, K.A.; Mitchell, A.J.; Britton, B.; Carter, G. Why do oncology outpatients who report emotional distress decline help? Psychooncology 2015, 24, 812–818. [Google Scholar] [CrossRef]
- Li, S.H.; Graham, B.M. Why are women so vulnerable to anxiety, trauma-related and stress-related disorders? The potential role of sex hormones. Lancet Psychiatry 2017, 4, 73–82. [Google Scholar] [CrossRef]
- Pang, C.; Humphris, G. The Relationship Between Fears of Cancer Recurrence and Patient Gender: A Systematic Review and Meta-Analysis. Front. Psychol. 2021, 12, 640866. [Google Scholar] [CrossRef]
- Hernández, R.; Calderon, C.; Carmona-Bayonas, A.; Rodríguez Capote, A.; Jara, C.; Padilla Álvarez, A.; Gómez-Camacho, M.d.L.N.; Beato, C.; Castelo, B.; Majem, M.; et al. Differences in coping strategies among young adults and the elderly with cancer. Psychogeriatrics 2019, 19, 426–434. [Google Scholar] [CrossRef]
- Fitch, M.I. Perspectives of survivors: Coping with lifestyle adjustments following cancer diagnosis and treatment. Can. Oncol. Nurs. J. 2021, 31, 235–238. [Google Scholar]
- Champagne, A.; Ivers, H.; Savard, J. Utilization of health care services in cancer patients with elevated fear of cancer recurrence. Psychooncology 2018, 27, 1958–1964. [Google Scholar] [CrossRef]
- Park, K.A.; Kim, S.; Oh, E.G.; Kim, H.; Chang, H.-S.; Kim, S.H. Factors affecting the health-promoting behavior of thyroid cancer survivors: Comparison by stage of cancer survivorship. Supportive Care Cancer 2022, 30, 3429–3439. [Google Scholar] [CrossRef]
- Schapira, L.; Zheng, Y.; Gelber, S.I.; Poorvu, P.; Ruddy, K.J.; Tamimi, R.M.; Peppercorn, J.; Come, S.E.; Borges, V.F.; Partridge, A.H.; et al. Trajectories of fear of cancer recurrence in young breast cancer survivors. Cancer 2022, 128, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Melendro, M.; Campos, G.; Rodríguez-Bravo, A.E.; Arroyo Resino, D. Young People’s Autonomy and Psychological Well-Being in the Transition to Adulthood: A Pathway Analysis. Front. Psychol. 2020, 11, 1946. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Kelly, D.; Hannigan, B. Autonomy and dependence: A discussion paper on decision-making in teenagers and young adults undergoing cancer treatment. J. Adv. Nurs. 2015, 71, 2031–2040. [Google Scholar] [CrossRef] [PubMed]
- Lidington, E.; Darlington, A.-S.; Din, A.; Stanway, S.; Banerjee, S.; Szucs, Z.; Gonzalez, M.; Sharma, A.; Sirohi, B.; van der Graaf, W.T.A.; et al. Describing Unmet Supportive Care Needs among Young Adults with Cancer (25–39 Years) and the Relationship with Health-Related Quality of Life, Psychological Distress, and Illness Cognitions. J. Clin. Med. 2021, 10, 4449. [Google Scholar] [CrossRef]
- Thorsen, L.; Bøhn, S.-K.H.; Lie, H.C.; Fosså, S.D.; Kiserud, C.E. Needs for information about lifestyle and rehabilitation in long-term young adult cancer survivors. Supportive Care Cancer 2022, 30, 521–533. [Google Scholar] [CrossRef]
- Lin, M.; Sansom-Daly, U.M.; Wakefield, C.E.; McGill, B.C.; Cohn, R.J. Health Literacy in Adolescents and Young Adults: Perspectives from Australian Cancer Survivors. J. Adolesc. Young Adult Oncol. 2017, 6, 150–158. [Google Scholar] [CrossRef]
- Richter, D.; Mehnert, A.; Forstmeyer, D.; Ernst, J.; Geue, K. Health Literacy in Adolescent and Young Adult Cancer Patients and Its Association with Health Outcomes. J. Adolesc. Young Adult Oncol. 2019, 8, 451–457. [Google Scholar] [CrossRef]
- Ellegaard, M.-B.B.; Grau, C.; Zachariae, R.; Bonde Jensen, A. Fear of cancer recurrence and unmet needs among breast cancer survivors in the first five years. A cross-sectional study. Acta Oncol. 2017, 56, 314–320. [Google Scholar] [CrossRef] [Green Version]
- Kelada, L.; Wakefield, C.E.; Heathcote, L.C.; Jaaniste, T.; Signorelli, C.; Fardell, J.E.; Donoghoe, M.; McCarthy, M.C.; Gabriel, M.; Cohn, R.J. Perceived cancer-related pain and fatigue, information needs, and fear of cancer recurrence among adult survivors of childhood cancer. Patient Educ. Couns. 2019, 102, 2270–2278. [Google Scholar] [CrossRef]
- Grace, J.G.; Schweers, L.; Anazodo, A.; Freyer, D.R. Evaluating and providing quality health information for adolescents and young adults with cancer. Pediatr. Blood Cancer 2019, 66, e27931. [Google Scholar] [CrossRef]
- Lea, S.; Martins, A.; Morgan, S.; Cargill, J.; Taylor, R.M.; Fern, L.A. Online information and support needs of young people with cancer: A participatory action research study. Adolesc. Health Med. Ther. 2018, 9, 121–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlooswijk, C.; Husson, O.; Krahmer, E.J.; Bijlsma, R.; Kaal, S.E.J.; Sleeman, S.H.E.; van de Poll-Franse, L.V.; van der Graaf, W.T.A.; Bol, N.; van Eenbergen, M.C. Differences in Internet Use and eHealth Needs of Adolescent and Young Adult Versus Older Cancer Patients; Results from the PROFILES Registry. Cancers 2021, 13, 6308. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | n | % 1 | |
|---|---|---|---|
| Age in years (median (interquartile range)) | (31.0 [9]) | ||
| Gender | Female | 202 | 81.8 |
| Male | 45 | 18.2 | |
| Partnership/Cohabiting (yes) | 160 | 64.8 | |
| Children (yes) | 67 | 27.1 | |
| Educational level | Junior high school or below | 64 | 25.9 |
| High school degree | 178 | 72.1 | |
| Employment status | Employed | 174 | 70.4 |
| Unemployed | 53 | 21.5 | |
| Students | 20 | 8.1 | |
| Off treatment (yes) | 213 | 86.2 | |
| Comorbidities (yes) | 130 | 52.6 | |
| Tumor site | Hematological malignancies | 78 | 31.6 |
| Solid tumors Breast cancer Gynecological cancer Sarcoma Other | - 70 30 19 50 | - 28.3 12.1 7.7 20.2 | |
| Time since diagnosis in months (median (interquartile range)) | (35.2 [41.0]) | ||
| Cancer treatments | Surgery | 185 | 74.9 |
| (multiple responses possible) | Radiation therapy | 127 | 51.4 |
| Chemotherapy | 200 | 81.0 | |
| Bone marrow/stem cell transplantation | 14 | 5.7 | |
| Hormonal therapy | 46 | 18.6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, D.; Clever, K.; Mehnert-Theuerkauf, A.; Schönfelder, A. Fear of Recurrence in Young Adult Cancer Patients—A Network Analysis. Cancers 2022, 14, 2092. https://doi.org/10.3390/cancers14092092
Richter D, Clever K, Mehnert-Theuerkauf A, Schönfelder A. Fear of Recurrence in Young Adult Cancer Patients—A Network Analysis. Cancers. 2022; 14(9):2092. https://doi.org/10.3390/cancers14092092
Chicago/Turabian StyleRichter, Diana, Katharina Clever, Anja Mehnert-Theuerkauf, and Antje Schönfelder. 2022. "Fear of Recurrence in Young Adult Cancer Patients—A Network Analysis" Cancers 14, no. 9: 2092. https://doi.org/10.3390/cancers14092092
APA StyleRichter, D., Clever, K., Mehnert-Theuerkauf, A., & Schönfelder, A. (2022). Fear of Recurrence in Young Adult Cancer Patients—A Network Analysis. Cancers, 14(9), 2092. https://doi.org/10.3390/cancers14092092