
Incidence and Risk Factors for Cerebrovascular-Specific Mortality in Patients with Colorectal Cancer: A Registry-Based Cohort Study Involving 563,298 Patients


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods and Materials
2.1. Data Sources
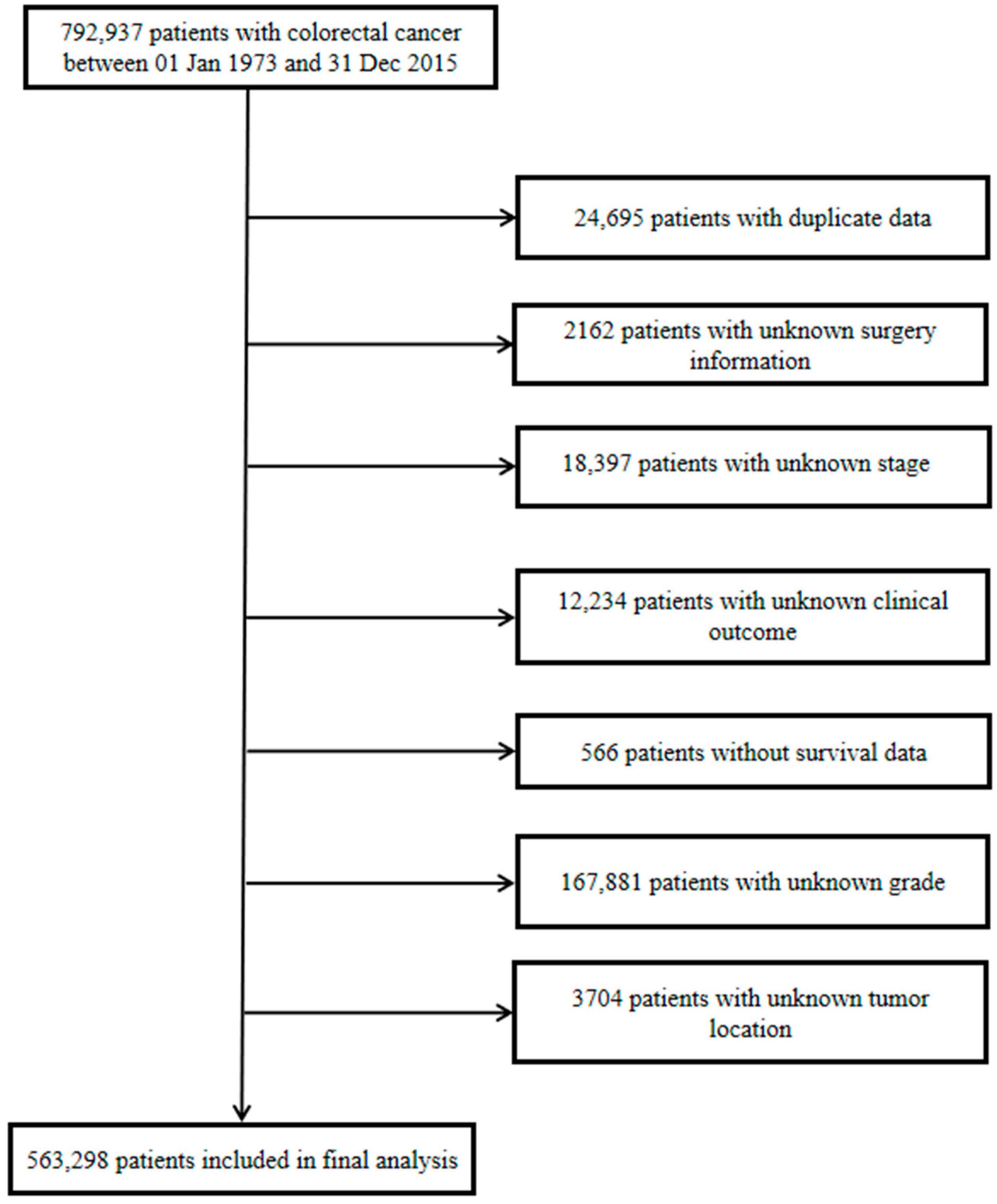
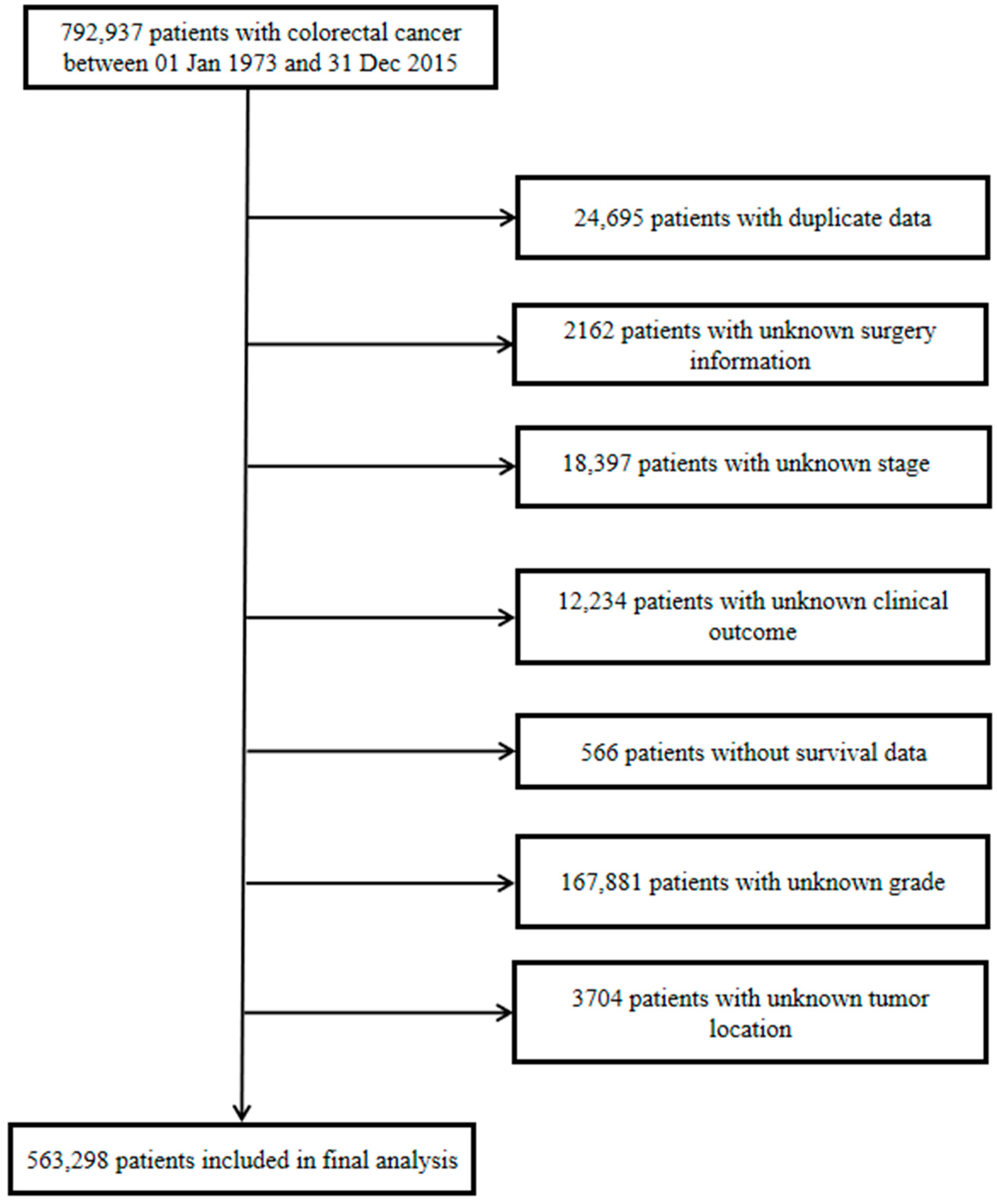
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
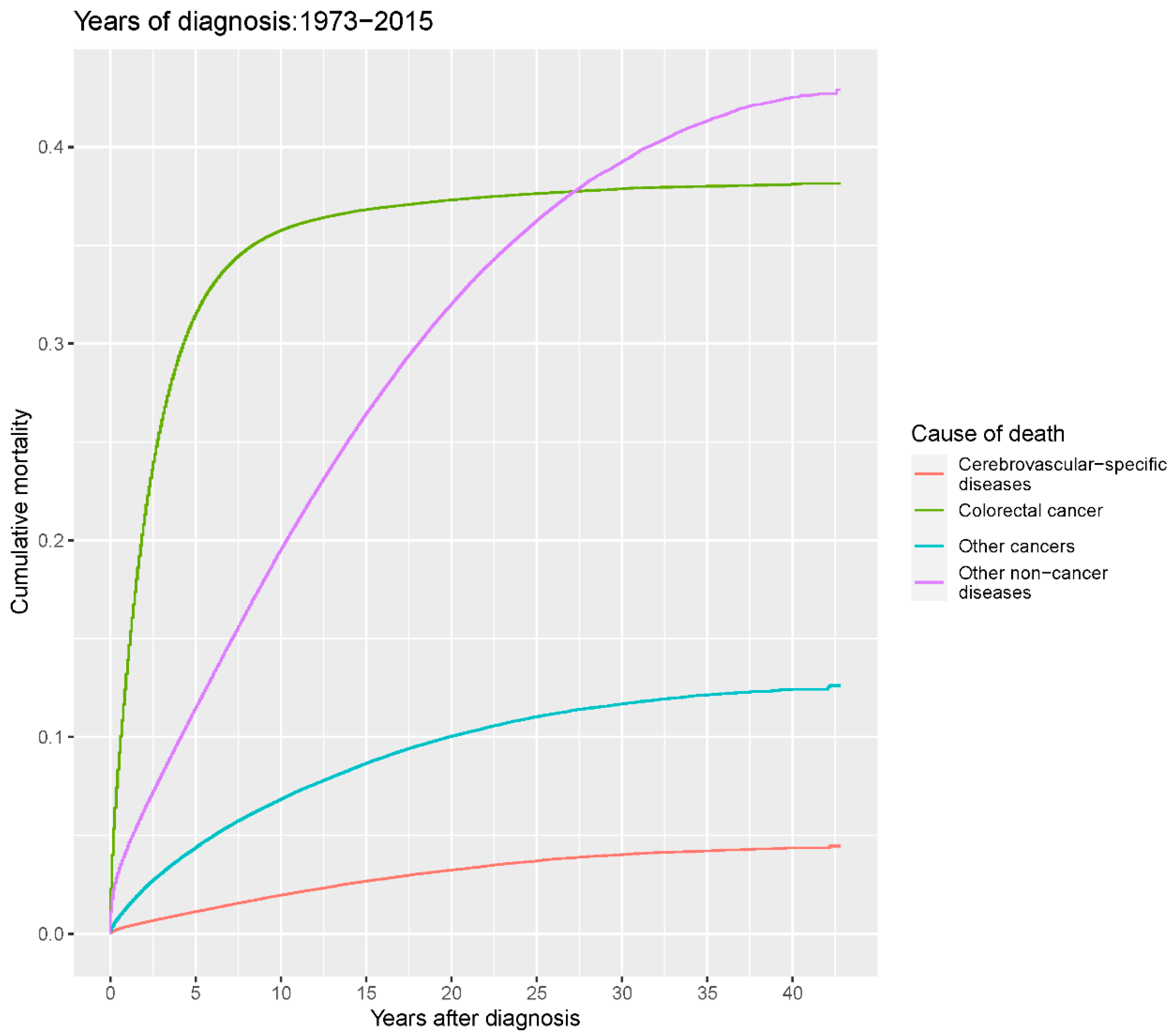
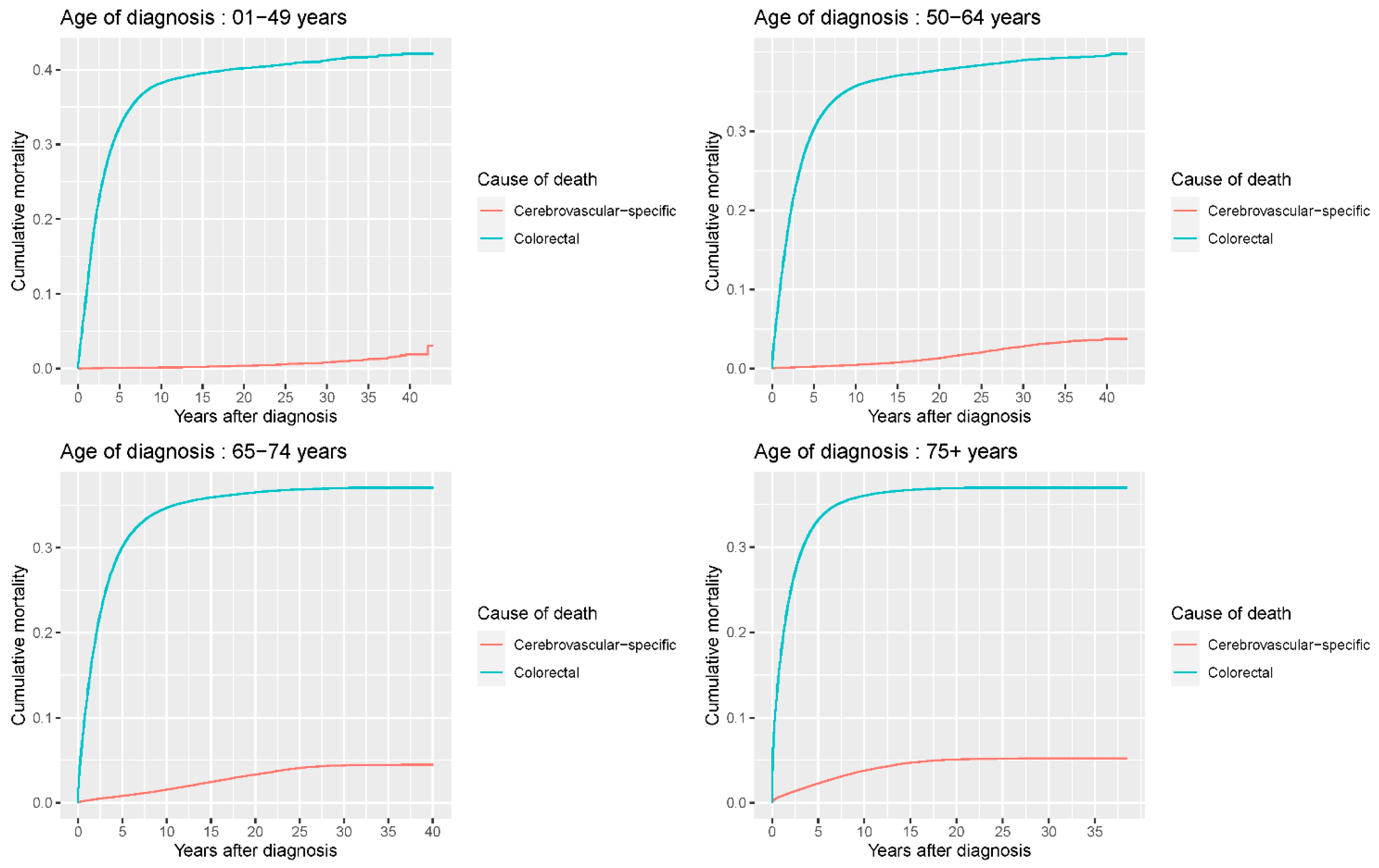
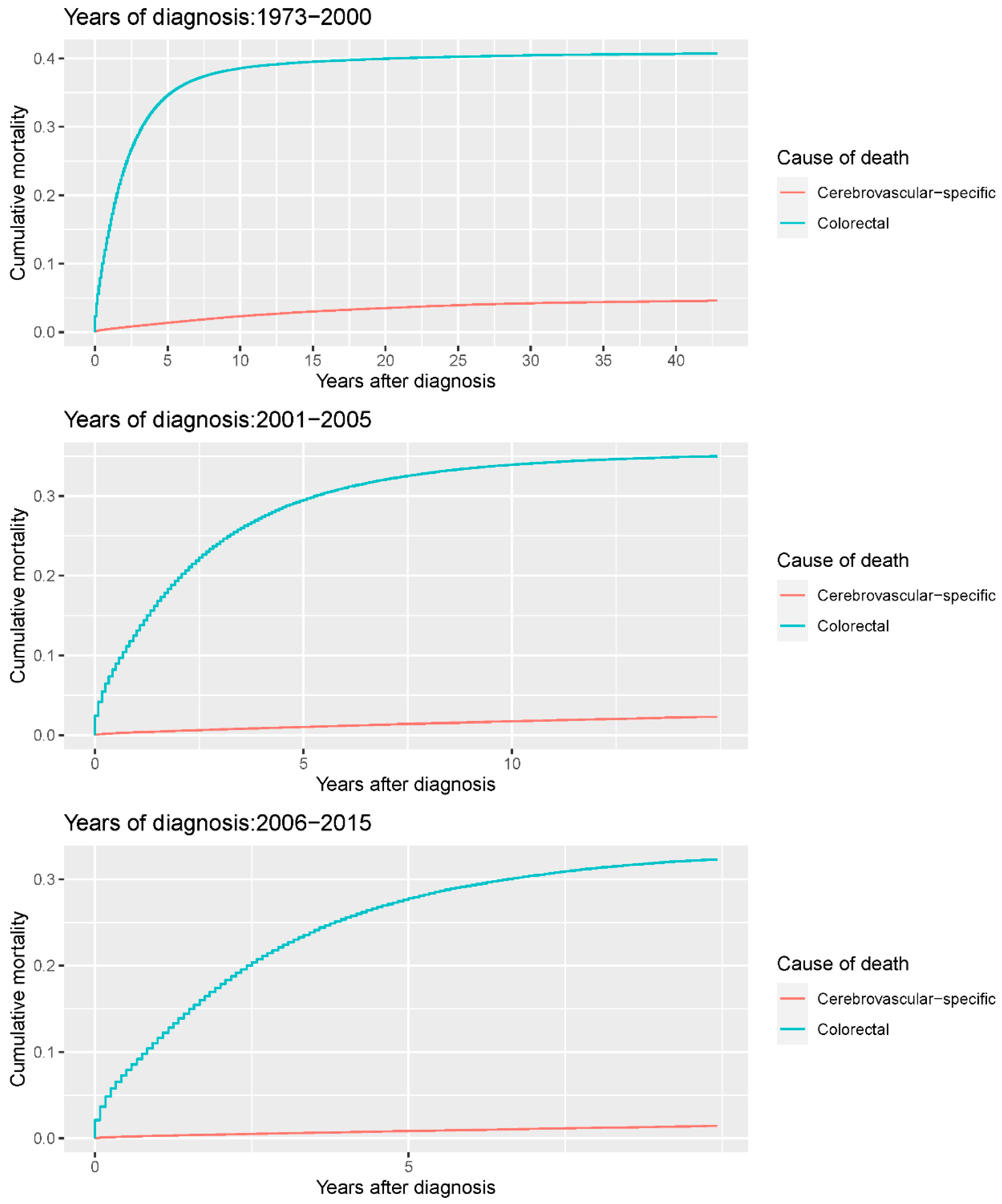
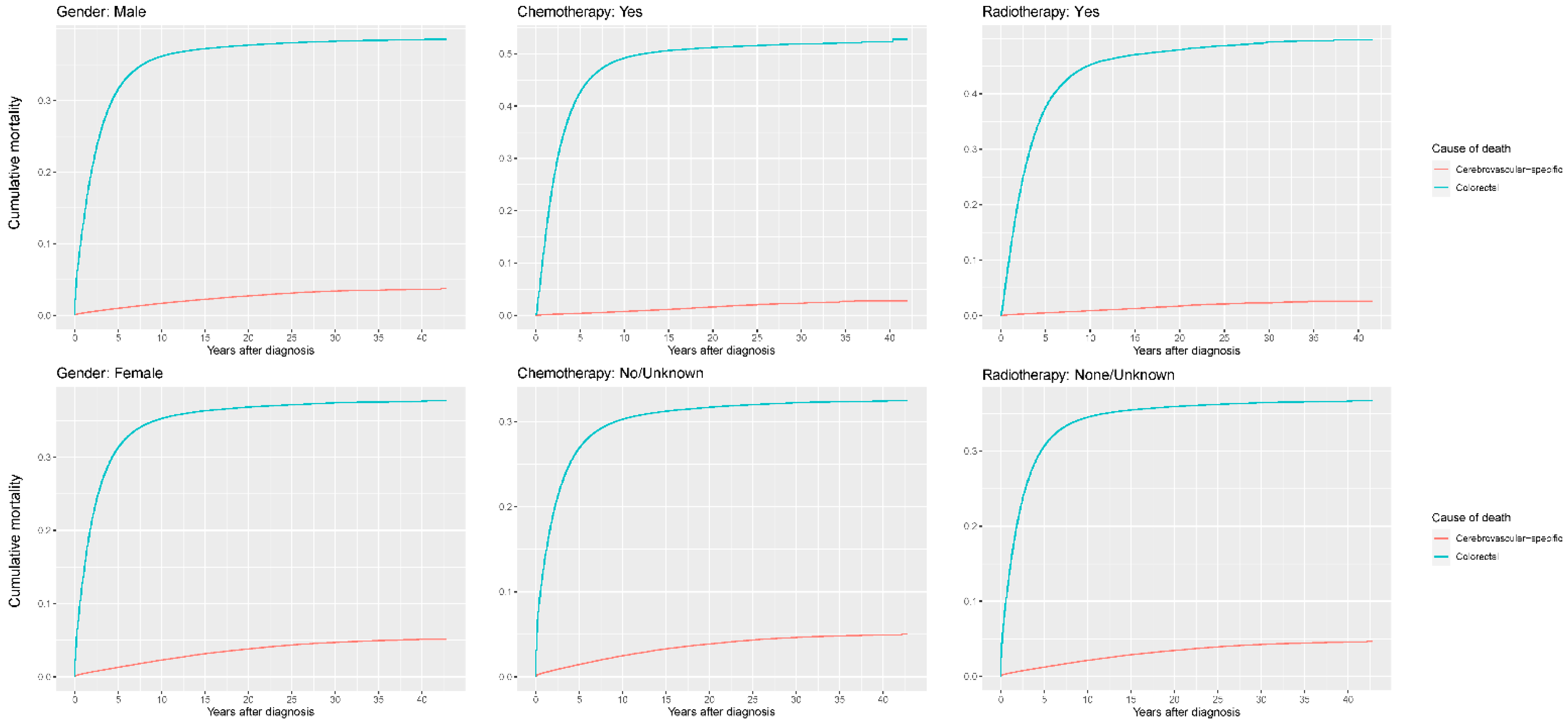
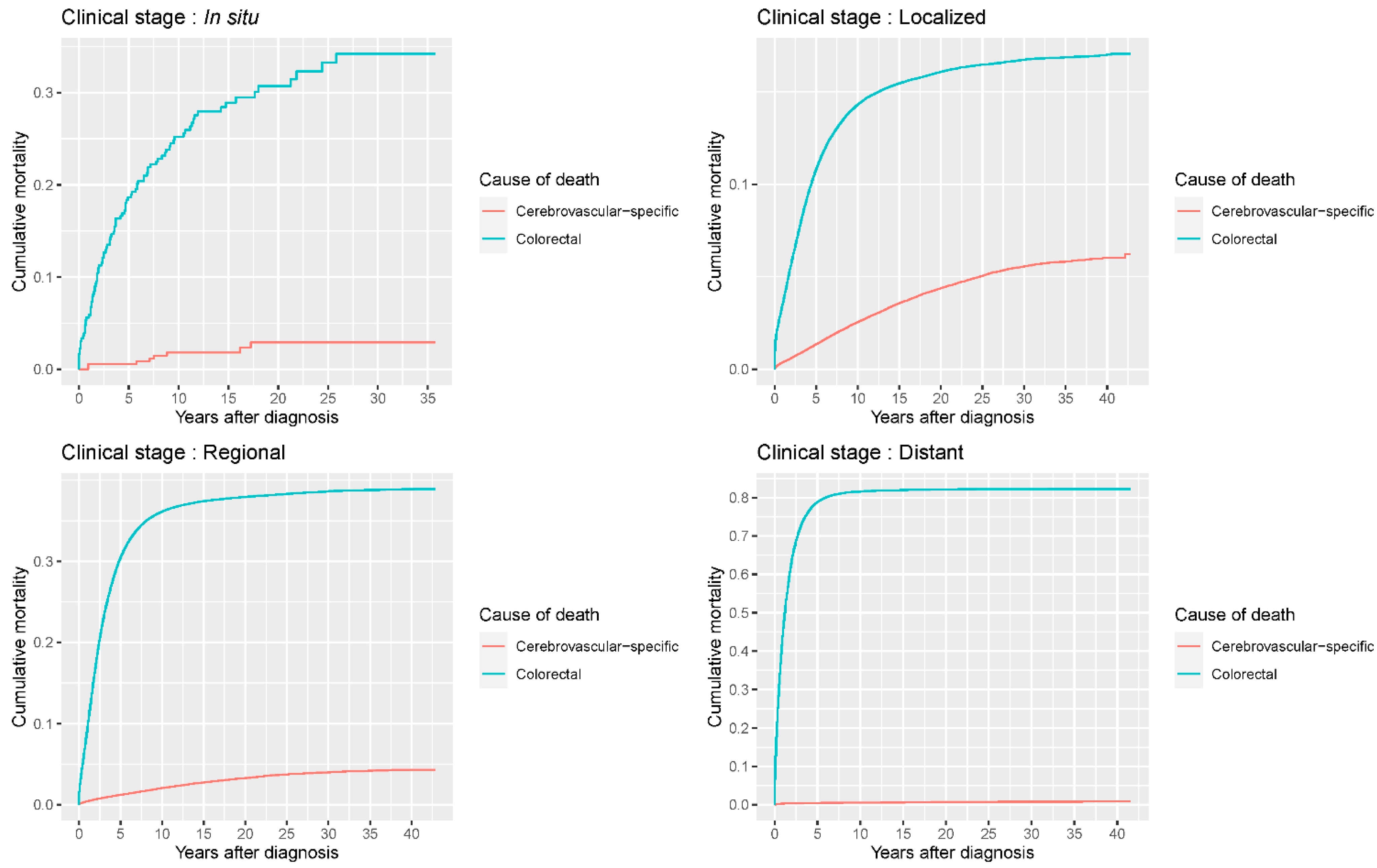
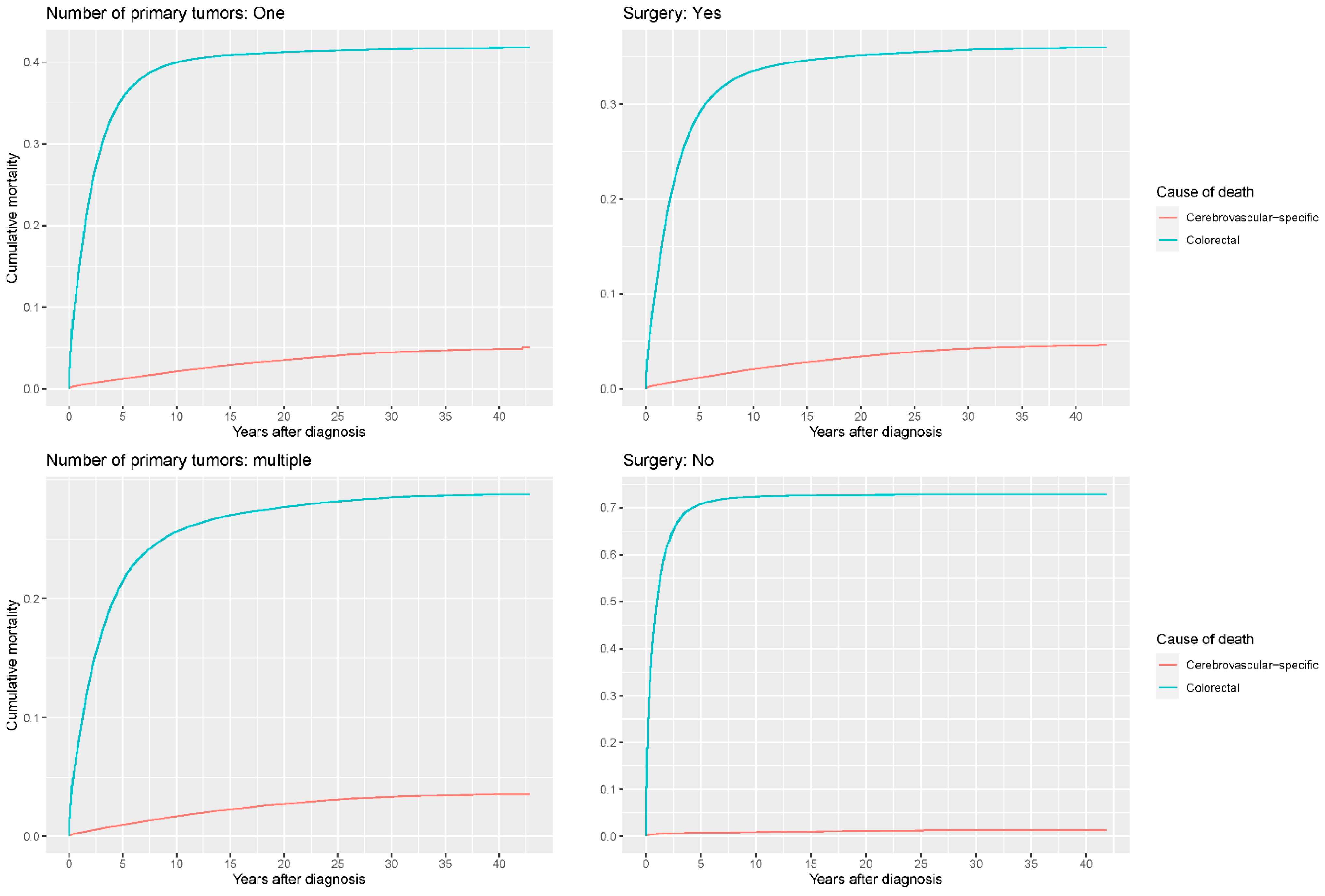
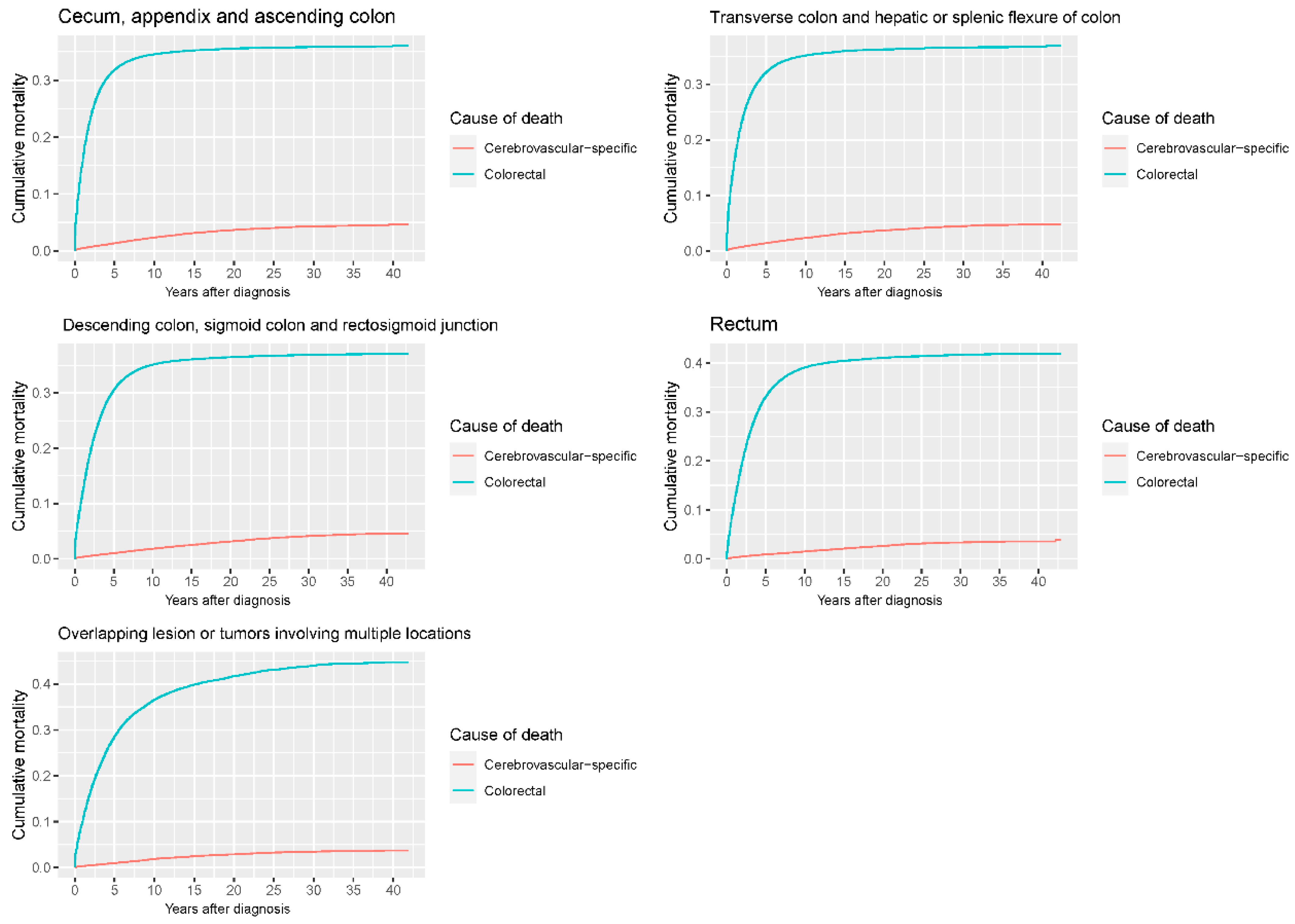
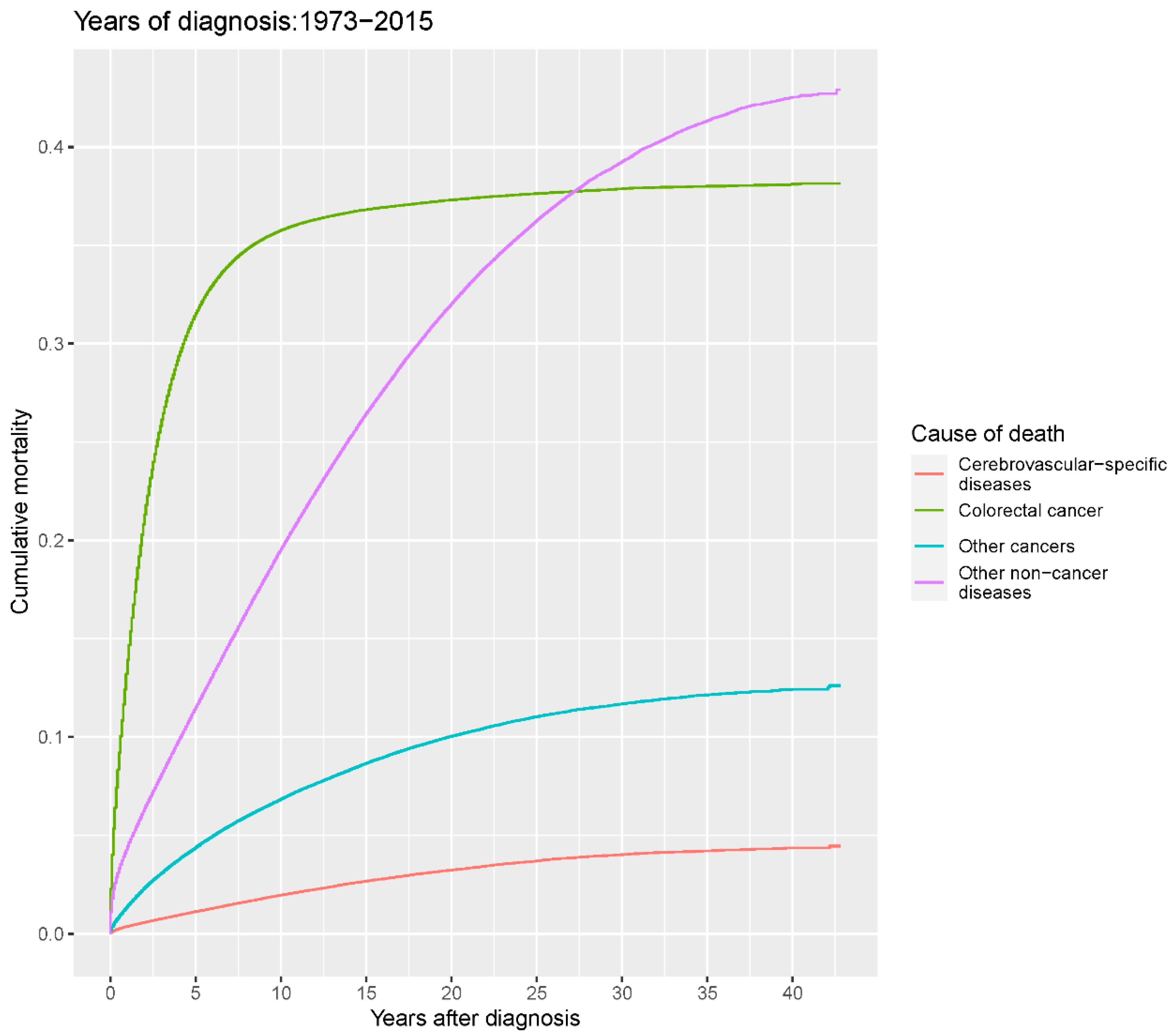
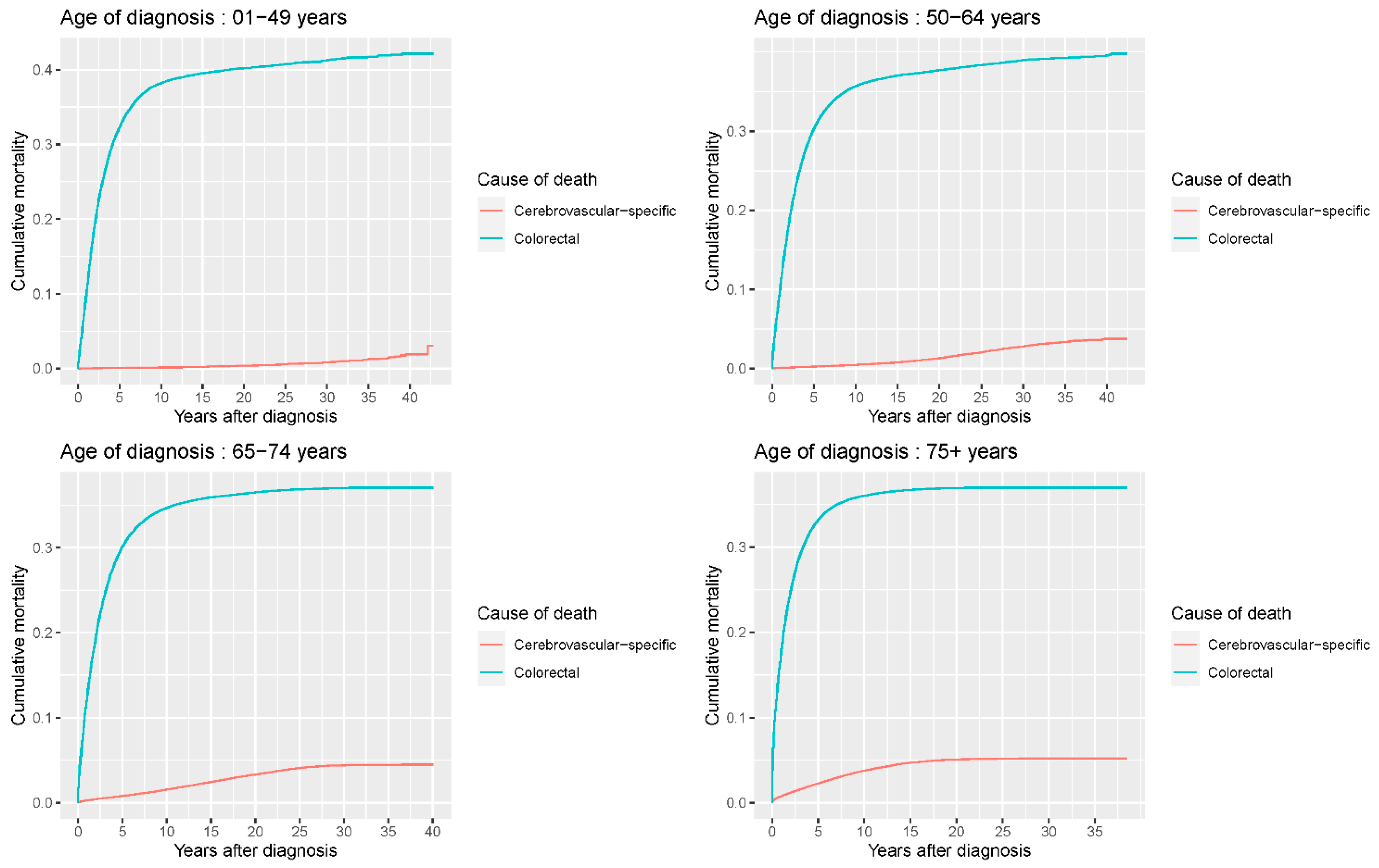
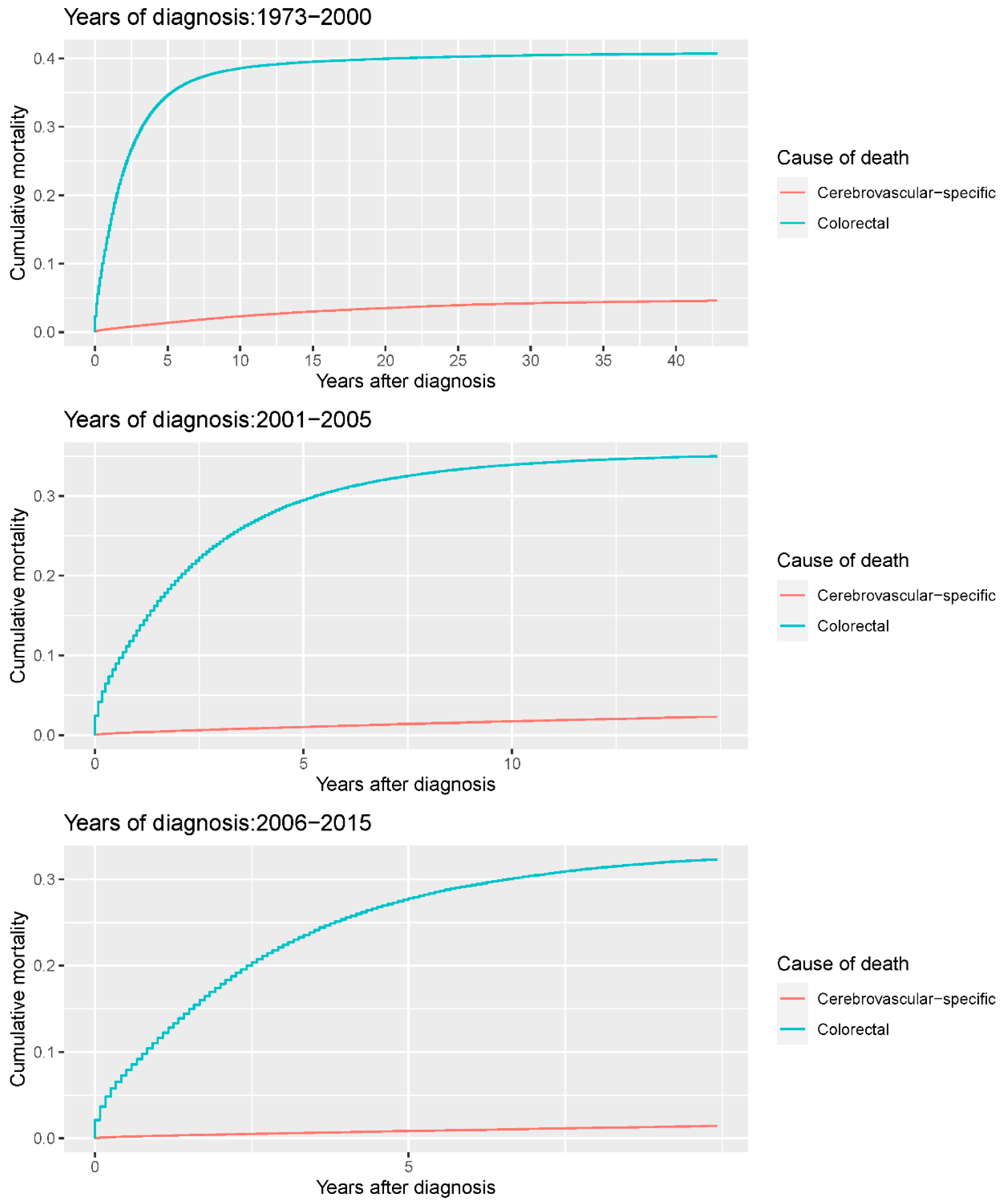
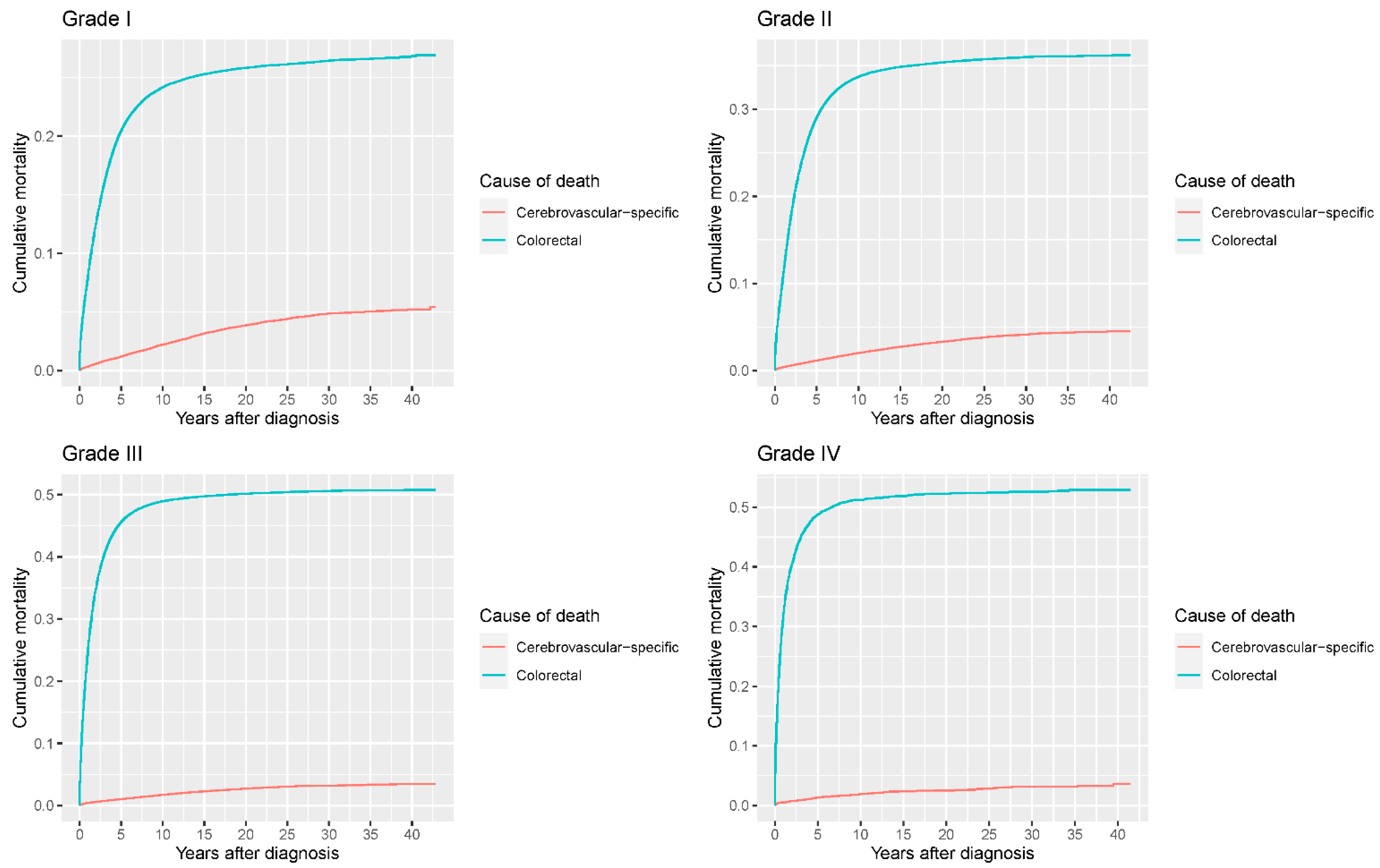
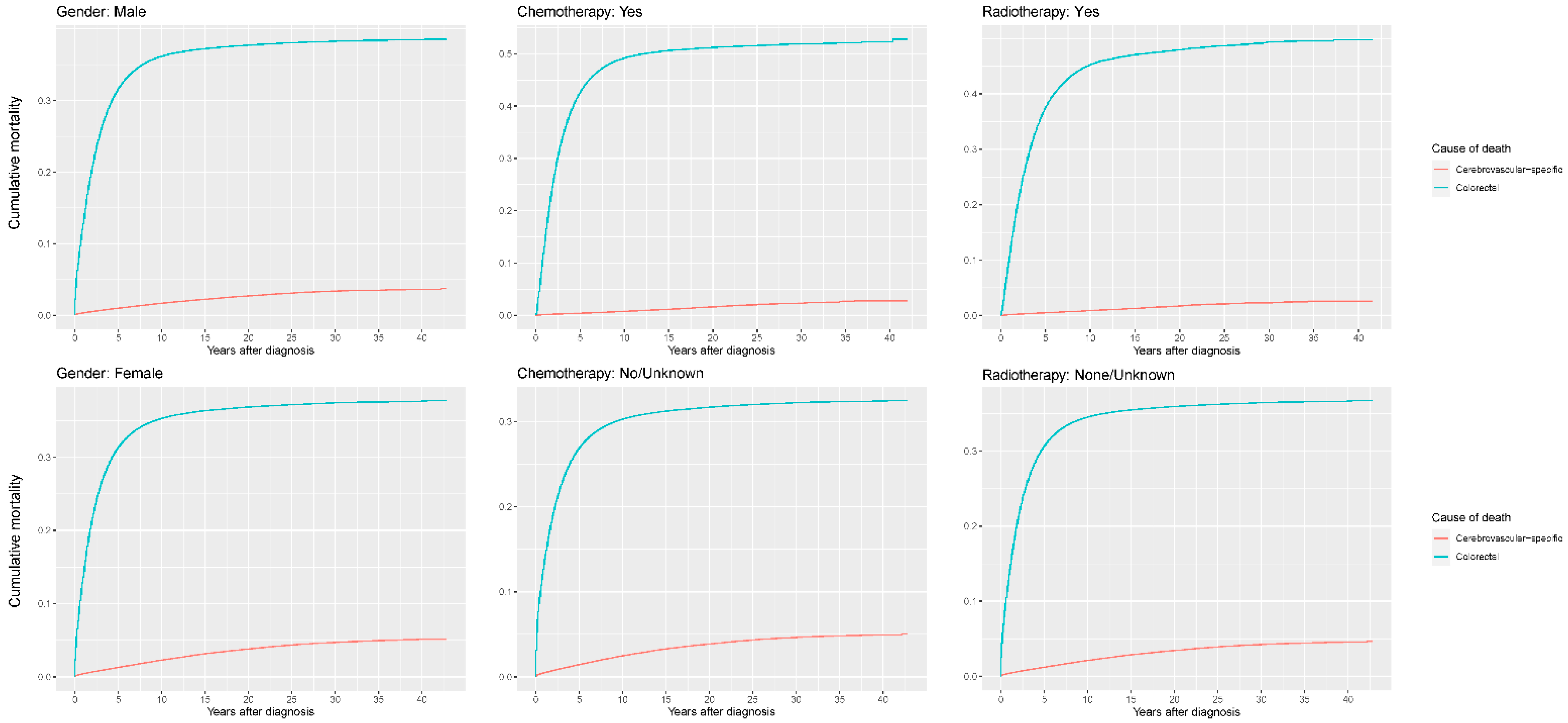
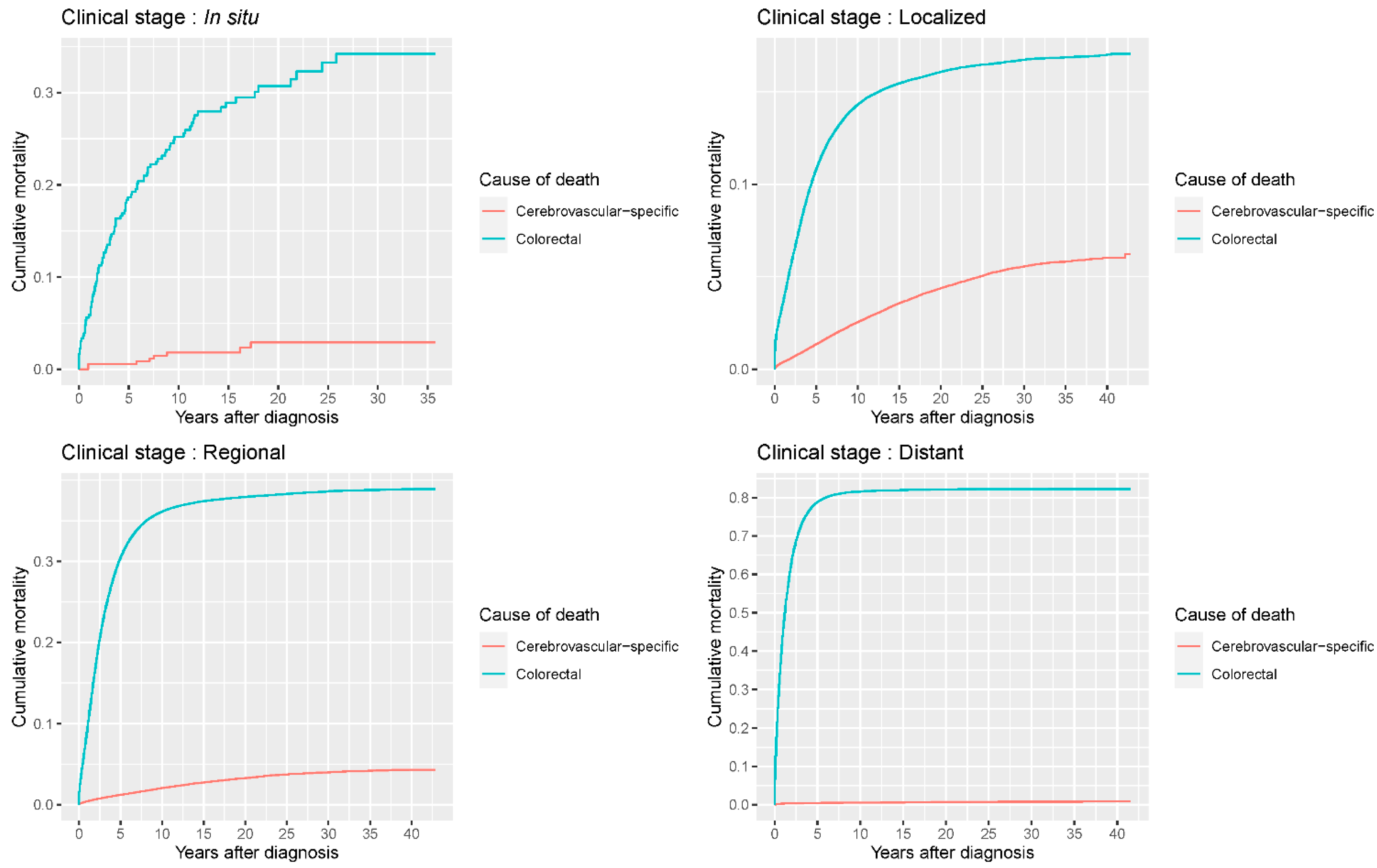
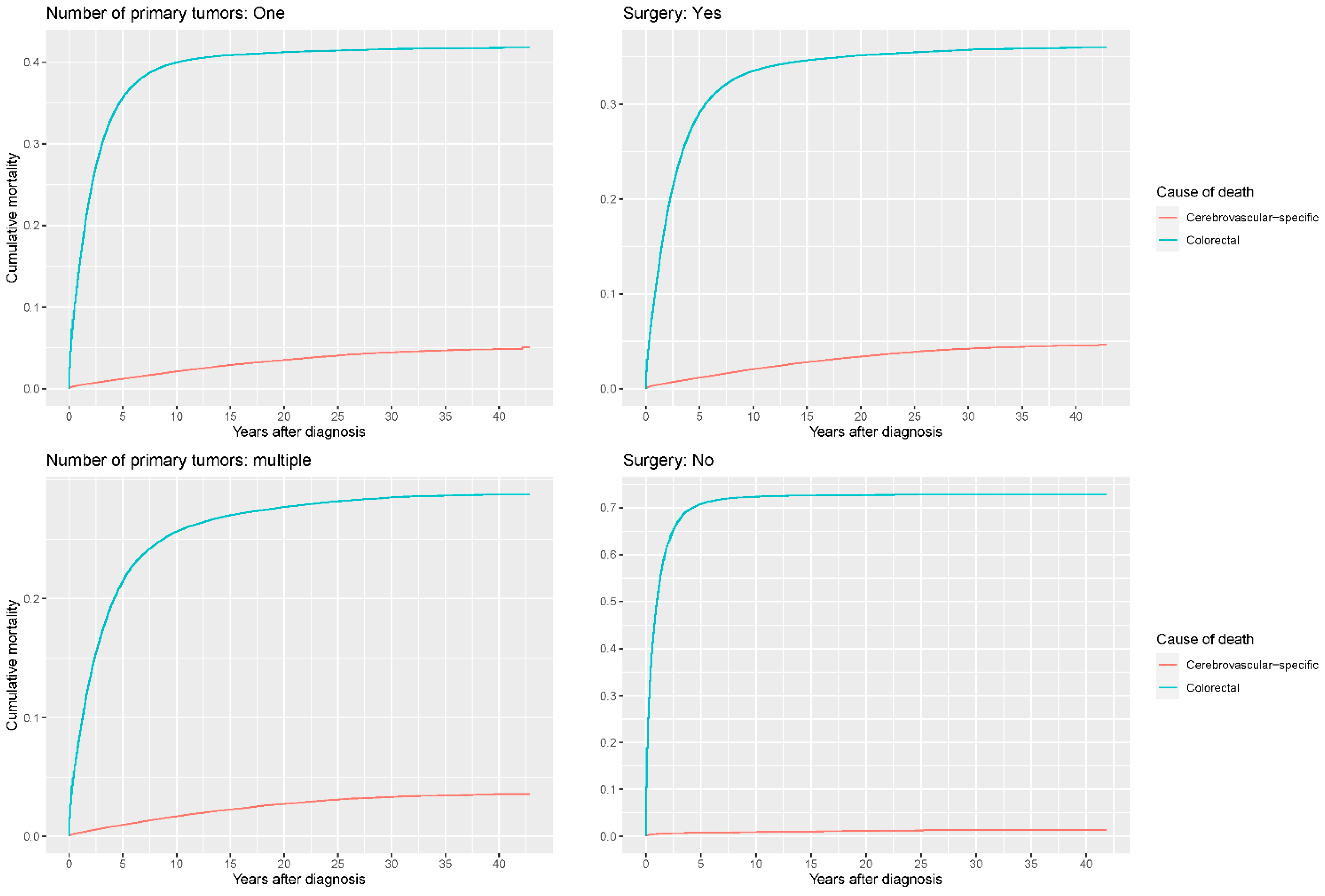
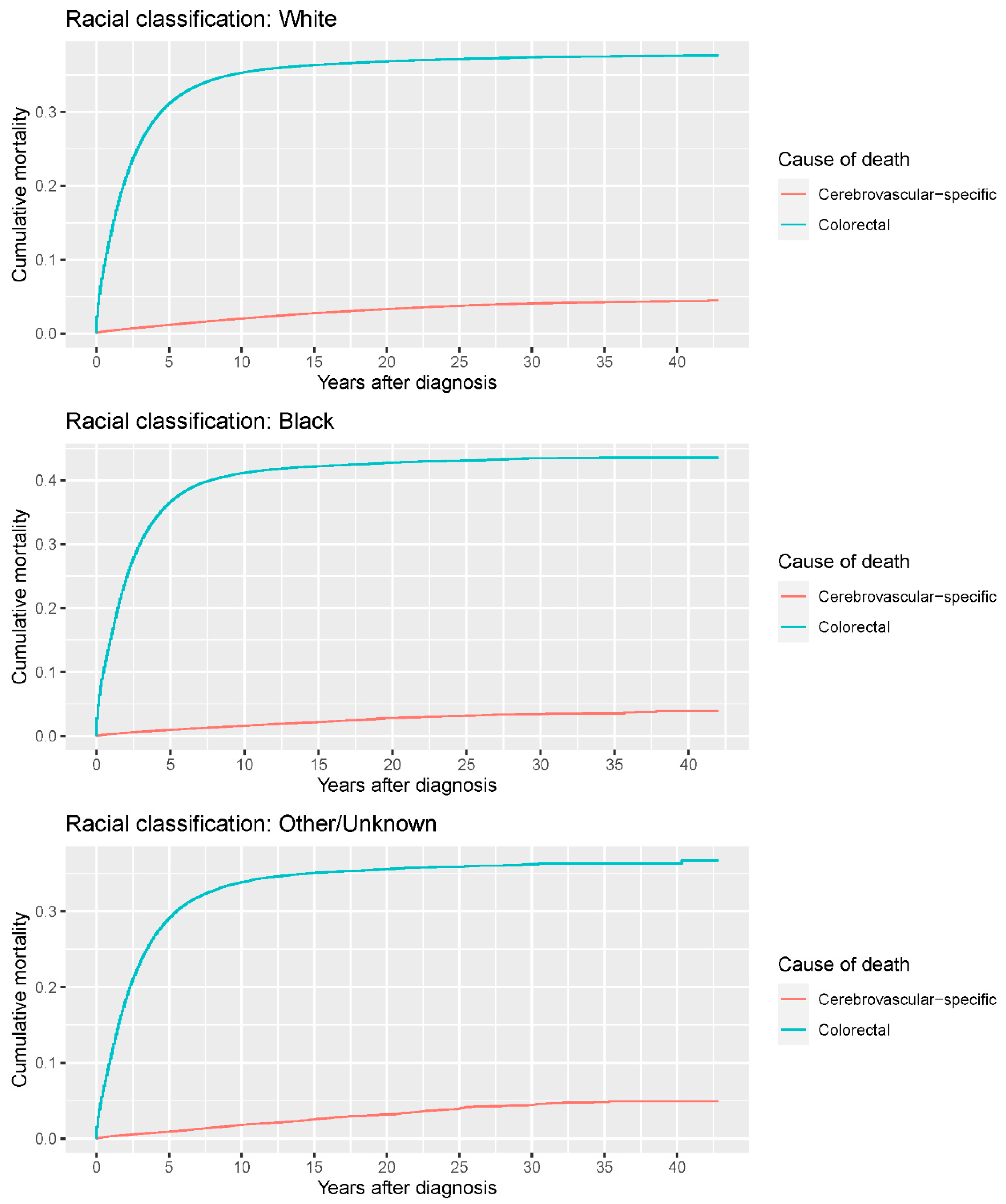
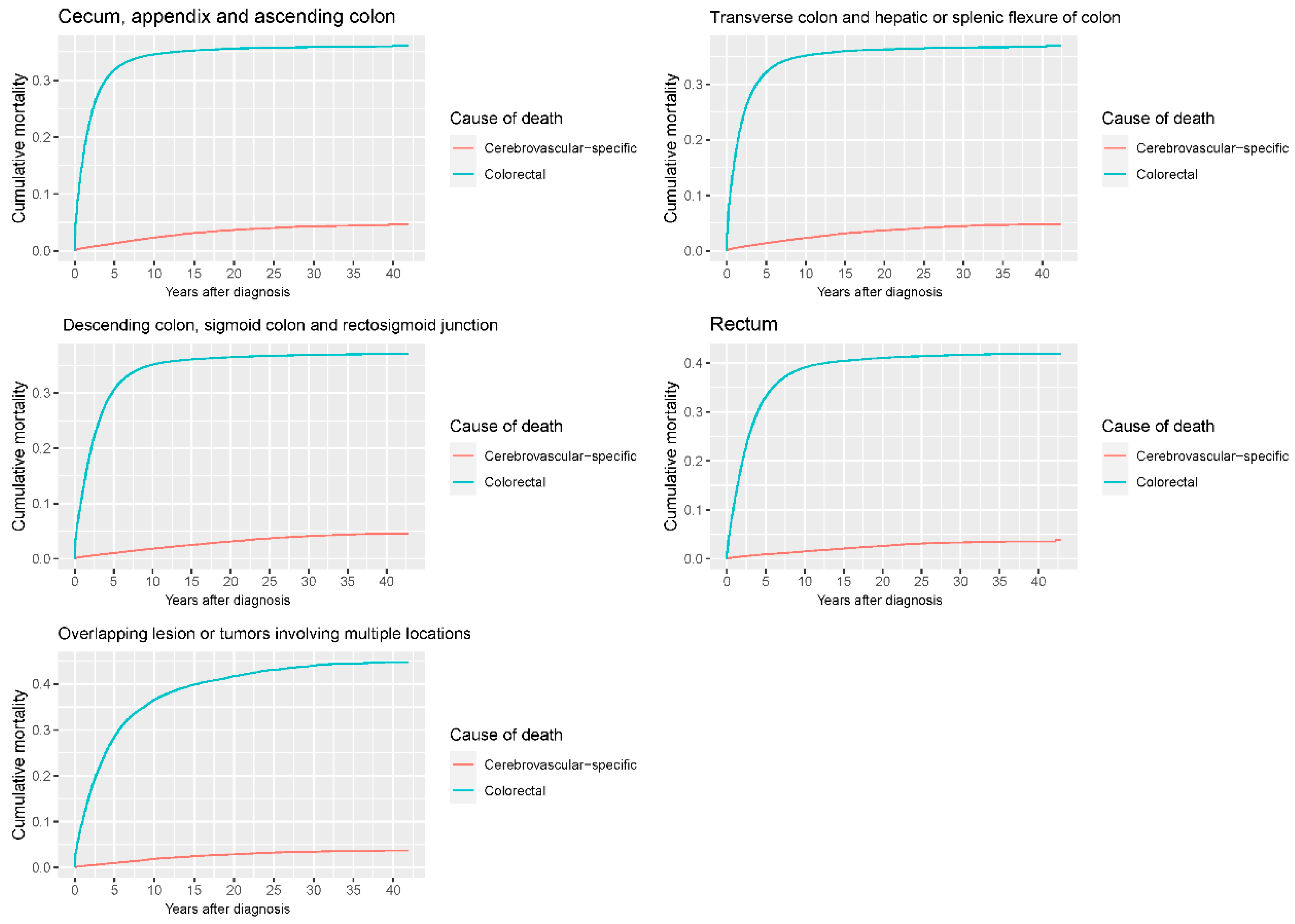
3.2. Cumulative Mortality
3.3. Conditional Standardized Mortality Ratio
3.4. Cause-Specific Hazard Ratios (HRs)
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef] [PubMed]
- Navi, B.B.; Howard, G.; Howard, V.J.; Zhao, H.; Hudd, S.E.; Elkind, M.S.V.; Iadecola, C.; DeAngelis, L.M.; Kamel, H.; Okin, P.M.; et al. New diagnosis of cancer and the risk of subsequent cerebrovascular events. Neurology 2018, 90, e2025–e2033. [Google Scholar] [CrossRef] [PubMed]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Elkind, M.S.V.; Panageas, K.; DeAngelis, L.M. Association between incident cancer and subsequent stroke. Ann. Neurol. 2015, 77, 291–300. [Google Scholar] [CrossRef]
- De Bruin, M.L.; Dorresteijn, L.D.; Van’t Veer, M.B.; Krol, A.D.G.; van der Pal, H.J.; Kappelle, A.C.; Boogerd, W.; Aleman, B.M.P.; van Leeuwen, F.E. Increased risk of stroke and transient ischemic attack in 5-year survivors of Hodgkin lymphoma. J. Natl. Cancer Inst. 2009, 101, 928–937. [Google Scholar] [CrossRef] [Green Version]
- Kadosh, E.; Snir-Alkalay, I.; Venkatachalam, A.; May, S.; Lasry, A.; Elyada, E.; Zinger, A.; Shaham, M.; Vaalani, G.; Mernberger, M.; et al. The gut microbiome switches mutant p53 from tumour-suppressive to oncogenic. Nature 2020, 586, 133–138. [Google Scholar] [CrossRef]
- Wirbel, J.; Pyl, P.T.; Kartal, E.; Zych, K.; Kashani, A.; Milanese, A.; Fleck, J.S.; Voigt, A.Y.; Palleja, A.; Ponnudurai, R.P.; et al. Meta-analysis of fecal metagenomes reveals global microbial signatures that are specific for colorectal cancer. Nat. Med. 2019, 25, 679–689. [Google Scholar] [CrossRef] [Green Version]
- Jonsson, A.L.; Backhed, F. Role of gut microbiota in atherosclerosis. Nat. Rev. Cardiol. 2017, 14, 79–87. [Google Scholar] [CrossRef]
- Tang, W.H.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef] [Green Version]
- Zaorsky, N.G.; Zhang, Y.; Tchelebi, L.T.; Mackley, H.B.; Chinchilli, V.M.; Zacharia, B.E. Stroke among cancer patients. Nat. Commun. 2019, 10, 5172. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Wang, K.; Du, P.; Yang, W.; He, Y.; Li, T.; Mei, Z. Risk of Stroke in Cancer Survivors: A Meta-analysis of Population-Based Cohort Studies. Neurology 2021, 96, e513–e526. [Google Scholar] [CrossRef] [PubMed]
- Surveillance, Epidemiology, and End Results (SEER) Program Populations (1973–2015). National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch. Available online: http://www.seer.cancer.gov/popdata (accessed on 11 June 2021).
- Centers for Disease Control and Prevention. CDC Wonder. Available online: http://wonder.cdc.gov/ (accessed on 27 June 2021).
- Weberpals, J.; Jansen, L.; Muller, O.J.; Brenner, H. Long-term heart-specific mortality among 347 476 breast cancer patients treated with radiotherapy or chemotherapy: A registry-based cohort study. Eur. Heart J. 2018, 39, 3896–3903. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Dess, R.T.; Suresh, K.; Zelefsky, M.J.; Freedland, S.J.; Mahal, B.A.; Cooperberg, M.R.; Davis, B.J.; Horwitz, E.M.; Terris, M.; Amling, C.L.; et al. Development and Validation of a Clinical Prognostic Stage Group System for Nonmetastatic Prostate Cancer Using Disease-Specific Mortality Results from the International Staging Collaboration for Cancer of the Prostate. JAMA Oncol. 2020, 6, 1912–1920. [Google Scholar] [CrossRef]
- Tapper, E.B.; Nikirk, S.; Parikh, N.D.; Zhao, L. Falls are common, morbid, and predictable in patients with cirrhosis. J. Hepatol. 2021, 75, 582–588. [Google Scholar] [CrossRef]
- Chatterjee, N.A.; Tikkanen, J.T.; Panicker, G.K.; Narula, D.; Lee, D.C.; Kentta, T.; Junttila, J.M.; Cook, N.R.; Kadish, A.; Goldberger, J.J.; et al. Simple electrocardiographic measures improve sudden arrhythmic death prediction in coronary disease. Eur. Heart J. 2020, 41, 1988–1999. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Fuchs, E.; Ricken, G.; Mlecnik, B.; Bindea, G.; Spanberger, T.; Hackl, M.; Widhalm, G.; Dieckmann, K.; Prayer, D.; et al. Density of tumor-infiltrating lymphocytes correlates with extent of brain edema and overall survival time in patients with brain metastases. Oncoimmunology 2016, 5, e1057388. [Google Scholar] [CrossRef]
- Moore, D.S.; Notz, W.I.; Flinger, M.A. The Basic Practice of Statistics, 6th ed.; W. H. Freeman and Company: New York, NY, USA, 2013. [Google Scholar]
- Vandenbroucke, J.P. A shortcut method for the calculation of the 95 percent confidence interval of the standarized mortality ratio. Am. J. Epidemiol. 1982, 115, 303–304. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. How to obtain the P value from a confidence interval. BMJ 2011, 343, d2304. [Google Scholar] [CrossRef] [Green Version]
- Zoller, B.; Ji, J.; Sundquist, J.; Sundquist, K. Risk of haemorrhagic and ischaemic stroke in patients with cancer: A nationwide follow-up study from Sweden. Eur. J. Cancer 2012, 48, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; O’riordan, K.J.; Cowan, C.S.M.; Sandhu, K.V.; Bastiaanssen, T.F.S.; Boehme, M.; Codagnone, M.G.; Cussotto, S.; Fulling, C.; Golubeva, A.V.; et al. The Microbiota-Gut-Brain Axis. Physiol. Rev. 2019, 99, 1877–2013. [Google Scholar] [CrossRef] [PubMed]
- Sikpa, D.; Whittingstall, L.; Fouquet, J.P.; Radulska, A.; Tremblay, L.; Lebel, R.; Paquette, B.; Lepage, M. Cerebrovascular inflammation promotes the formation of brain metastases. Int. J. Cancer 2020, 147, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Ridler, C. Cerebrovascular malformations: Microbiota promotes cerebral cavernous malformations. Nat. Rev. Neurol. 2017, 13, 386. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, D.M.; Rahman, A.H.; Fernandez, N.F.; Chudnovskiy, A.; Amir, E.-A.D.; Amadori, L.; Khan, N.S.; Wong, C.K.; Shamailova, R.; Hill, C.A.; et al. Single-cell immune landscape of human atherosclerotic plaques. Nat. Med. 2019, 25, 1576–1588. [Google Scholar] [CrossRef] [PubMed]
- Yeh, E.T.H.; Chang, H.M. Cancer and Clot: Between a Rock and a Hard Place. J. Am. Coll. Cardiol. 2017, 70, 939–941. [Google Scholar] [CrossRef]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Okin, P.M.; Elkind, M.S.V.; Panageas, K.S.; DeAngelis, L.M. Risk of Arterial Thromboembolism in Patients with Cancer. J. Am. Coll. Cardiol. 2017, 70, 926–938. [Google Scholar] [CrossRef]
- Young, A.; Chapman, O.; Connor, C.; Poole, C.; Rose, P.; Kakkar, A.K. Thrombosis and cancer. Nat. Rev. Clin. Oncol. 2012, 9, 437–449. [Google Scholar] [CrossRef]
- Koeth, R.A.; Wang, Z.; Levison, B.S.; Buffa, J.A.; Org, E.; Sheehy, B.T.; Britt, E.B.; Fu, X.; Wu, Y.; Li, L.; et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 2013, 19, 576–585. [Google Scholar] [CrossRef] [Green Version]
- Garrett, W.S. Cancer and the microbiota. Science 2015, 348, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.H.; Yu, J. Gut microbiota in colorectal cancer: Mechanisms of action and clinical applications. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 690–704. [Google Scholar] [CrossRef] [PubMed]
- Louis, P.; Hold, G.L.; Flint, H.J. The gut microbiota, bacterial metabolites and colorectal cancer. Nat. Rev. Microbiol. 2014, 12, 661–672. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C.; Davisson, R.L. Hypertension and cerebrovascular dysfunction. Cell Metab. 2008, 7, 476–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuladhar, A.M.; De Leeuw, F.E. Increased Risk of Cerebrovascular Events in Young Cancer Survivors: The Downside of Surviving Cancer. Circulation 2017, 135, 1211–1213. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, V.M.; Duckles, S.P. Vascular actions of estrogens: Functional implications. Pharmacol. Rev. 2008, 60, 210–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straub, R.H. The complex role of estrogens in inflammation. Endocr. Rev. 2007, 28, 521–574. [Google Scholar] [CrossRef] [Green Version]
- Wagner, C.A.; Roque, P.J.; Mileur, T.R.; Liggitt, D.; Goverman, J.M. Myelin-specific CD8+ T cells exacerbate brain inflammation in CNS autoimmunity. J. Clin. Investig. 2020, 130, 203–213. [Google Scholar] [CrossRef]
- Miggelbrink, A.M.; Jackson, J.D.; Lorrey, S.J.; Srinivasan, E.S.; Waibl-Polania, J.; Wilkinson, D.S.; Fecci, P.E. CD4 T-Cell Exhaustion: Does It Exist and What Are Its Roles in Cancer? Clin. Cancer Res. 2021, 27, 5742–5752. [Google Scholar] [CrossRef]
- Gialdini, G.; Nearing, K.; Bhave, P.D.; Bonuccelli, U.; Iadecola, C.; Healey, J.S.; Kamel, H. Perioperative atrial fibrillation and the long-term risk of ischemic stroke. JAMA 2014, 312, 616–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smilowitz, N.R.; Gupta, N.; Ramakrishna, H.; Guo, Y.; Berger, J.S.; Bangalore, S. Perioperative Major Adverse Cardiovascular and Cerebrovascular Events Associated with Noncardiac Surgery. JAMA Cardiol. 2017, 2, 181–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boral, D.; Vishnoi, M.; Liu, H.N.; Yin, W.; Sprouse, M.L.; Scamardo, A.; Hong, D.S.; Tan, T.Z.; Thiery, J.P.; Chang, J.C.; et al. Molecular characterization of breast cancer CTCs associated with brain metastasis. Nat. Commun. 2017, 8, 196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klotz, R.; Thomas, A.; Teng, T.; Han, S.M.; Iriondo, O.; Li, L.; Restrepo-Vassalli, S.; Wang, A.; Izadian, N.; Mackay, M.; et al. Circulating Tumor Cells Exhibit Metastatic Tropism and Reveal Brain Metastasis Drivers. Cancer Discov. 2020, 10, 86–103. [Google Scholar] [CrossRef] [Green Version]
- Gan, T.; Schaberg, K.B.; He, D.; Mansour, A.; Kapoor, H.; Wang, C.; Evers, B.M.; Bocklage, T.J. Association Between Obesity and Histological Tumor Budding in Patients with Nonmetastatic Colon Cancer. JAMA Netw. Open 2021, 4, e213897. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Ng, A.S.; Cai, S.; Li, Q.; Yang, L.; Kerr, D. Novel therapeutic strategies: Targeting epithelial–mesenchymal transition in colorectal cancer. Lancet Oncol. 2021, 22, e358–e368. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Number of Patients (%) |
|---|---|
| N | 563,298 |
| Age (continuous, mean ± SD) | 68.6 ± 13.1 |
| Age (years, groups) | |
| <50 | 47,947 (8.5) |
| 50–64 | 150,201 (26.7) |
| 65–74 | 158,222 (28.1) |
| 75+ | 206,928 (36.7) |
| Year of diagnosis | |
| ≤2000 | 269,323 (47.8) |
| 2001–2005 | 148,725 (26.4) |
| 2006–2015 | 145,250 (25.8) |
| Sex | |
| Female | 276,592 (49.1) |
| Male | 286,706 (50.9) |
| Race | |
| White | 469,427 (83.3) |
| Black | 53,364 (9.5) |
| Other/unknown | 40,507 (7.2) |
| Grading | |
| I | 69,849 (12.4) |
| II | 375,542 (66.7) |
| III | 109,875 (19.5) |
| Ⅳ | 8032 (1.4) |
| Stage | |
| In situ | 356 (0.1) |
| Localized | 224,781 (39.9) |
| Regional | 234,669 (41.7) |
| Distant | 103,492 (18.4) |
| Tumor site | |
| Rectum | 99,924 (17.7) |
| Rectosigmoid junction | 50,683 (9.0) |
| Overlapping lesion or tumor involving multiple locations | 26,848 (4.9) |
| Sigmoid colon | 123,198 (21.9) |
| Descending colon | 24,961 (4.4) |
| Splenic flexure of colon | 14,779 (2.6) |
| Transverse colon | 36,841 (6.5) |
| Hepatic flexure of colon | 20,629 (3.7) |
| Ascending colon | 67,767 (12.0) |
| Appendix | 3987 (0.7) |
| Cecum | 93,681 (16.6) |
| Cause of death | |
| Alive | 155,753 (27.7) |
| Colorectal cancer | 202,872 (36.0) |
| Cerebrovascular-specific diseases | 14,600 (2.6) |
| Other cancer | 46,648 (8.3) |
| Other non-cancer diseases | 143,425 (25.5) |
| Radiotherapy | |
| Yes | 65,352 (11.6) |
| No/unknown | 497,946 (88.4) |
| Chemotherapy | |
| Yes | 163,975 (29.1) |
| No/unknown | 399,323 (70.9) |
| Number of primary tumors | |
| One | 398,107 (70.7) |
| Multiple | 165,191 (29.3) |
| Surgery | |
| Yes | 530,282 (94.1) |
| No | 33,016 (5.9) |
| Duration of follow-up (years, mean ± SD) | 6.67 ± 6.48 |
| AgeGroup | cSMR Cerebrovascular-Specific | p-Value | cSMR Overall | p-Value |
|---|---|---|---|---|
| <50 | 83.14 (69.99–97.42) | <0.0001 | 371.66 (366.75–376.62) | <0.0001 |
| 50–54 | 21.76 (18.81–24.92) | <0.0001 | 97.64 (96.23–99.06) | <0.0001 |
| 55–59 | 26.54 (24.20–29.00) | <0.0001 | 76.96 (76.04–77.88) | <0.0001 |
| 60–64 | 24.56 (22.96–26.22) | <0.0001 | 58.68 (58.09–59.27) | <0.0001 |
| 65–69 | 20.92 (19.88–21.99) | <0.0001 | 43.20 (42.82–43.57) | <0.0001 |
| 70–74 | 16.37 (15.72–17.04) | <0.0001 | 30.66 (30.41–30.90) | <0.0001 |
| 75–79 | 10.64 (10.26–11.03) | <0.0001 | 20.80 (20.64–20.96) | <0.0001 |
| 80–84 | 6.91 (6.66–7.17) | <0.0001 | 13.58 (13.47–13.69) | <0.0001 |
| Factors | Number of Patients | Cause-Specific Hazards Ratios | |
|---|---|---|---|
| Cerebrovascular | p-Value | ||
| Age at diagnosis (years) | |||
| <50 | 47,947 | 1.000 (ref.) | |
| 50–64 | 150,201 | 3.098 (2.617–3.667) | <0.0001 |
| 65–74 | 158,222 | 6.666 (5.654–7.859) | <0.0001 |
| ≥75 | 206,928 | 10.951 (9.299–12.897) | <0.0001 |
| Sex | |||
| Male | 286,706 | 1.000 (ref.) | |
| Female | 276,592 | 1.223 (1.183–1.264) | <0.0001 |
| Surgery | |||
| No | 33,016 | 1.000(ref.) | |
| Yes | 530,282 | 1.558 (1.385–1.754) | <0.0001 |
| Radiotherapy | |||
| No/unknown | 497,946 | 1.000 (ref.) | |
| Yes | 65,352 | 0.849 (0.783–0.921) | <0.0001 |
| Chemotherapy | |||
| No/unknown | 399,323 | 1.000 (ref.) | |
| Yes | 163,975 | 0.653 (0.616–0.691) | <0.0001 |
| Year of diagnosis | |||
| ≤2000 | 269,323 | 1.000 (ref.) | |
| 2001–2005 | 148,725 | 0.610 (0.586–0.636) | <0.0001 |
| 2006–2015 | 145,250 | 0.451 (0.428–0.475) | <0.0001 |
| Number of primary tumors | |||
| One | 398,107 | 1.000 (ref.) | |
| Multiple | 165,191 | 0.685 (0.659–0.712) | <0.0001 |
| Stage | |||
| In situ | 356 | 1.000 (ref.) | |
| Localized | 224,781 | 1.361 (0.682–2.715) | 0.3800 |
| Regional | 234,669 | 1.120 (0.561–2.236) | 0.7500 |
| Distant | 103,492 | 0.298 (0.149–0.598) | 0.0006 |
| Grading | |||
| I | 69,849 | 1.000 (ref.) | |
| II | 375,542 | 0.953 (0.910–0.998) | 0.0410 |
| III | 109,875 | 0.892 (0.840–0.946) | 0.0002 |
| IV | 8032 | 1.023 (0.875–1.196) | 0.7800 |
| Race | |||
| White | 469,427 | 1.000 (ref.) | |
| Black | 53,364 | 1.019 (0.958–1.085) | 0.5500 |
| Other/Unknown | 40,507 | 1.110 (1.039–1.186) | 0.0019 |
| Tumor site | |||
| Cecum, appendix and ascending colon | 165,435 | 1.000 (ref.) | |
| Transverse colon and hepatic or splenic flexure of colon | 72,249 | 1.061 (1.008–1.116) | 0.0240 |
| Descending colon, sigmoid colon and rectosigmoid junction | 198,842 | 0.968 (0.930–1.008) | 0.1200 |
| Rectum | 99,924 | 0.900 (0.851–0.952) | 0.0002 |
| Overlapping lesion or tumors involving multiple locations | 26,848 | 1.057 (0.972–1.149) | 0.1900 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, Z.-H.; Tang, M.; Chen, Y.-L.; Zhang, T.-L.; Li, J.; Lv, G.-H.; Yan, Y.-G.; Ouyang, Z.-H.; Huang, W.; Zou, M.-X. Incidence and Risk Factors for Cerebrovascular-Specific Mortality in Patients with Colorectal Cancer: A Registry-Based Cohort Study Involving 563,298 Patients. Cancers 2022, 14, 2053. https://doi.org/10.3390/cancers14092053
Dai Z-H, Tang M, Chen Y-L, Zhang T-L, Li J, Lv G-H, Yan Y-G, Ouyang Z-H, Huang W, Zou M-X. Incidence and Risk Factors for Cerebrovascular-Specific Mortality in Patients with Colorectal Cancer: A Registry-Based Cohort Study Involving 563,298 Patients. Cancers. 2022; 14(9):2053. https://doi.org/10.3390/cancers14092053
Chicago/Turabian StyleDai, Zhi-Hui, Ming Tang, Yun-Liang Chen, Tao-Lan Zhang, Jing Li, Guo-Hua Lv, Yi-Guo Yan, Zhi-Hua Ouyang, Wei Huang, and Ming-Xiang Zou. 2022. "Incidence and Risk Factors for Cerebrovascular-Specific Mortality in Patients with Colorectal Cancer: A Registry-Based Cohort Study Involving 563,298 Patients" Cancers 14, no. 9: 2053. https://doi.org/10.3390/cancers14092053
APA StyleDai, Z.-H., Tang, M., Chen, Y.-L., Zhang, T.-L., Li, J., Lv, G.-H., Yan, Y.-G., Ouyang, Z.-H., Huang, W., & Zou, M.-X. (2022). Incidence and Risk Factors for Cerebrovascular-Specific Mortality in Patients with Colorectal Cancer: A Registry-Based Cohort Study Involving 563,298 Patients. Cancers, 14(9), 2053. https://doi.org/10.3390/cancers14092053