
Predictors of Recurrence in Patients with Papillary Thyroid Carcinoma: Does Male Sex Matter?


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcome Measures
2.3. Subgroup Analyses
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics and Tumor Characteristics
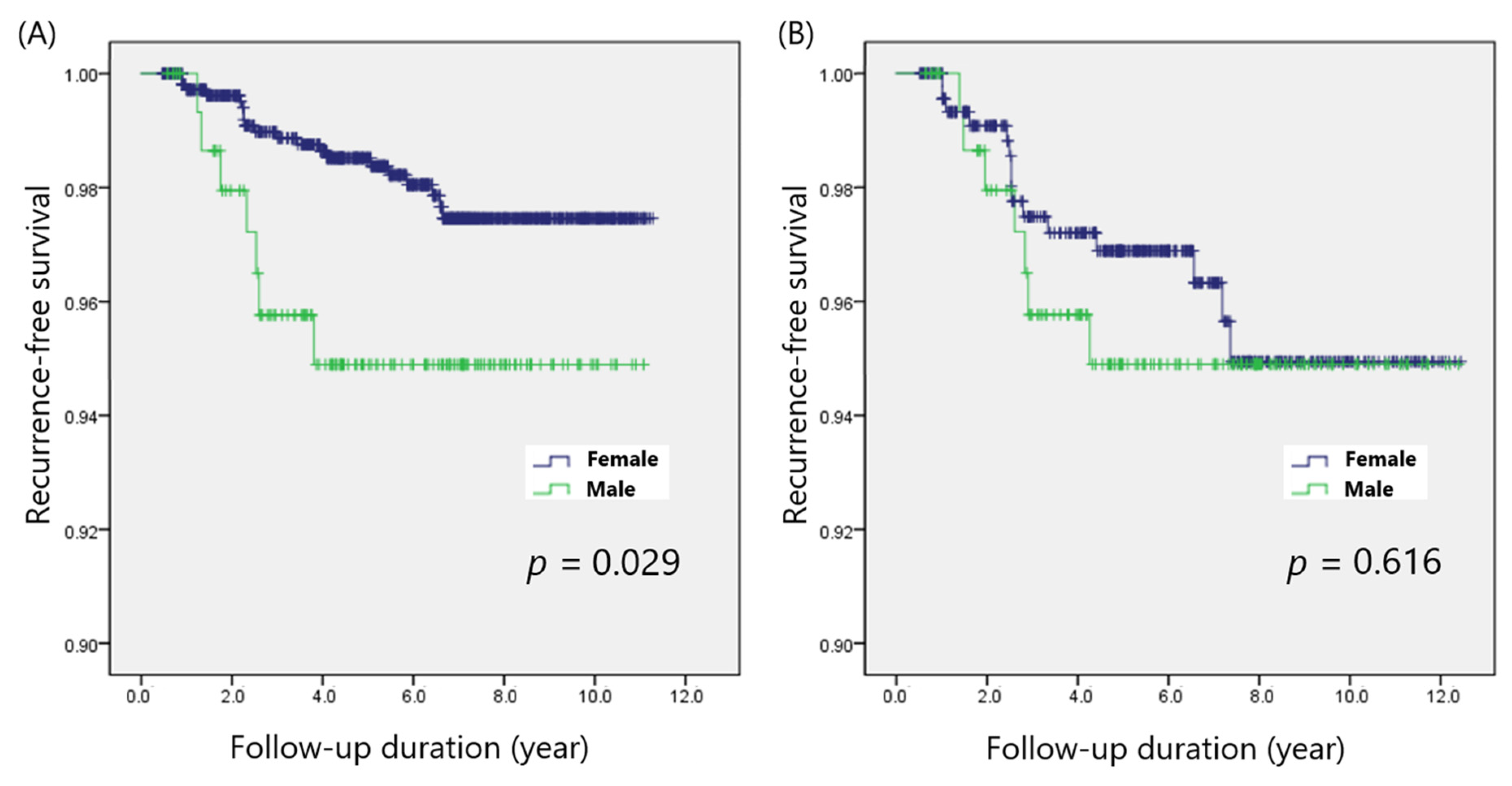
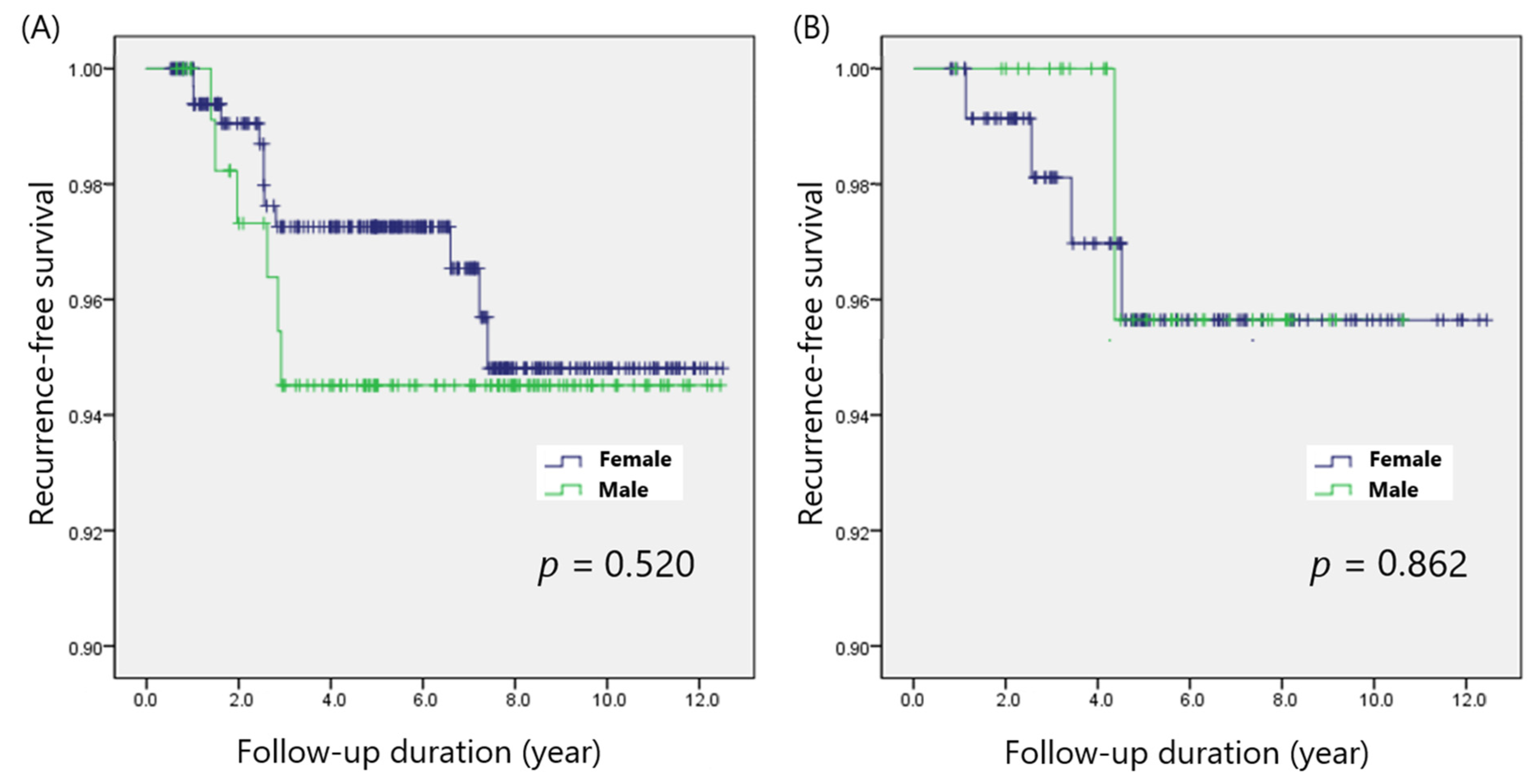
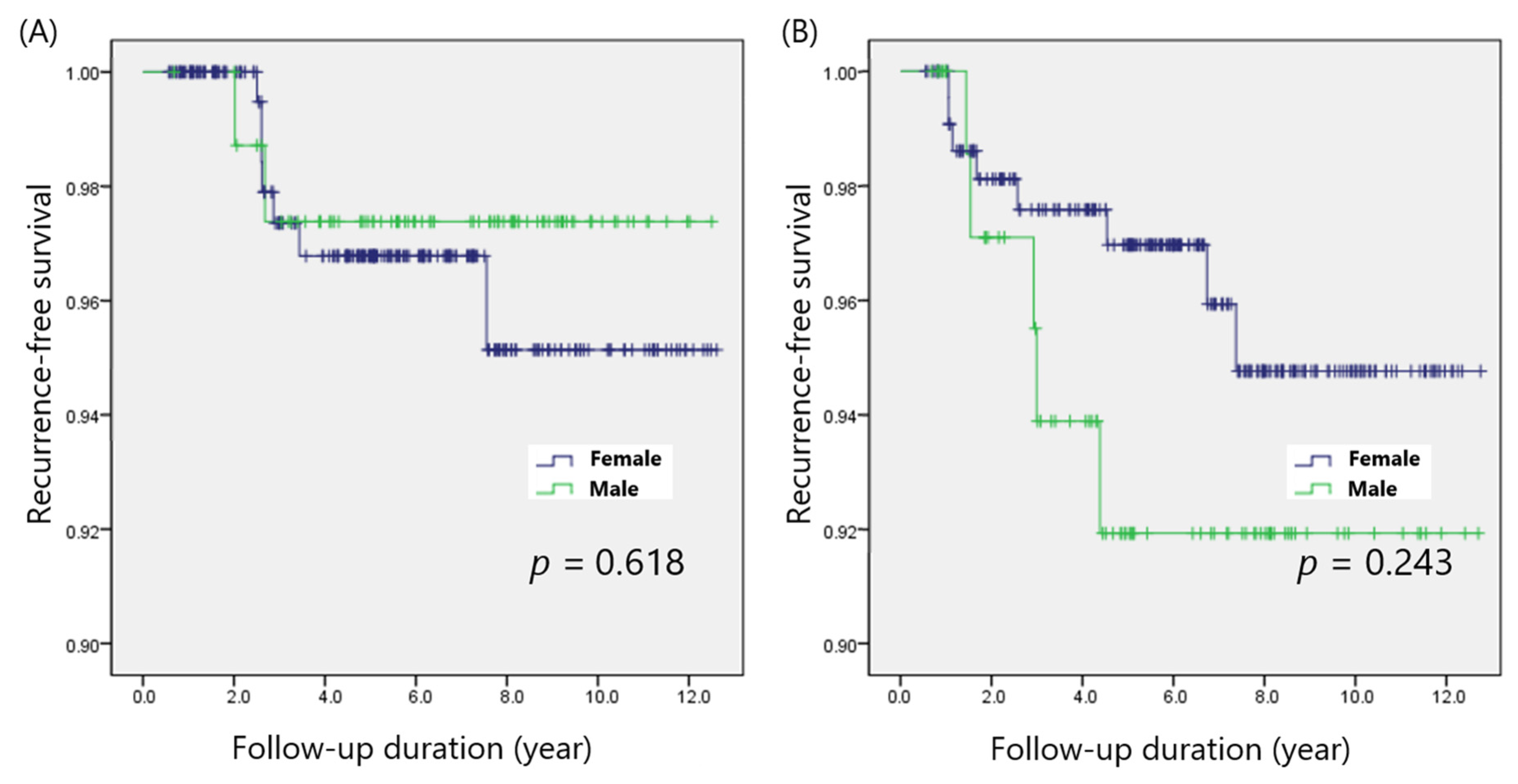
3.2. Comparison of Disease-Free Survival in the Matched Cohorts
3.3. Predictors of Poor DFS in Patients with PTC
3.4. Subgroup Analysis of the Impact of Patient Sex with Adjustments for Possible Confounders
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Won, Y.J.; Lee, J.J.; Jung, K.W.; Kong, H.J.; Im, J.S.; Seo, H.G.; Community of Population-Based Regional Cancer Registries. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2018. Cancer Res. Treat. 2021, 53, 301–315. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.Y.; Choi, H.S.; Park, Y.J.; Lim, J.A.; Ahn, H.Y.; Lee, E.K.; Kim, K.W.; Yi, K.H.; Chung, J.-K.; Youn, Y.-K.; et al. Changes in the clinicopathological characteristics and outcomes of thyroid cancer in korea over the past four decades. Thyroid 2013, 23, 797–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlumberger, M.; Leboulleux, S. Current practice in patients with differentiated thyroid cancer. Nat. Rev. Endocrinol. 2021, 17, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kwon, H.; Moon, B.I. Association of Multifocality With Prognosis of Papillary Thyroid Carcinoma: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 847–854. [Google Scholar] [CrossRef]
- Li, X.; Kwon, H. The Impact of BRAF Mutation on the Recurrence of Papillary Thyroid Carcinoma: A Meta-Analysis. Cancers 2020, 12, 2056. [Google Scholar] [CrossRef]
- Kwon, H.; Moon, B.I. Prognosis of papillary thyroid cancer in patients with Graves’ disease: A propensity score-matched analysis. World J. Surg. Oncol. 2020, 18, 266. [Google Scholar] [CrossRef]
- Shobab, L.; Burman, K.D.; Wartofsky, L. Sex Differences in Differentiated Thyroid Cancer. Thyroid 2022, 32, 224–235. [Google Scholar] [CrossRef]
- Rahbari, R.; Zhang, L.; Kebebew, E. Thyroid cancer gender disparity. Future Oncol. 2010, 6, 1771–1779. [Google Scholar] [CrossRef] [Green Version]
- Zahedi, A.; Bondaz, L.; Rajaraman, M.; Leslie, W.D.; Jefford, C.; Young, J.E.; Pathak, K.A.; Bureau, Y.; Rachinsky, I.; Badreddine, M.; et al. Risk for Thyroid Cancer Recurrence Is Higher in Men Than in Women Independent of Disease Stage at Presentation. Thyroid 2020, 30, 871–877. [Google Scholar] [CrossRef]
- Kim, M.J.; Lee, S.G.; Kim, K.; Lee, C.R.; Kang, S.W.; Lee, J.; Nam, K.-H.; Chung, W.Y.; Jeong, J.J. Current trends in the features of male thyroid cancer: Retrospective evaluation of their prognostic value. Medicine 2019, 98, e15559. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Chen, T.; Zeng, W.; Wang, S.; Xiong, Y.; Liu, Z.; Huang, T. Reevaluating the prognostic significance of male gender for papillary thyroid carcinoma and microcarcinoma: A SEER database analysis. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guo, K.; Wang, Z.Y. Risk factors influencing the recurrence of papillary thyroid carcinoma: A systematic review and meta-analysis. Int. J. Clin. Exp. Pathol. 2014, 7, 5393–5403. [Google Scholar] [PubMed]
- Kim, S.K.; Woo, J.W.; Lee, J.H.; Park, I.; Choe, J.H.; Kim, J.H.; Kim, J.S. Prophylactic Central Neck Dissection Might Not Be Necessary in Papillary Thyroid Carcinoma: Analysis of 11,569 Cases from a Single Institution. J. Am. Coll. Surg. 2016, 222, 853–864. [Google Scholar] [CrossRef]
- Jiang, L.H.; Yin, K.X.; Wen, Q.L.; Chen, C.; Ge, M.H.; Tan, Z. Predictive Risk-scoring Model For Central Lymph Node Metastasis and Predictors of Recurrence in Papillary Thyroid Carcinoma. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Kim, K.; Lim, D.J.; Bae, J.S.; Kim, J.S. Male sex is not an independent risk factor for recurrence of differentiated thyroid cancer: A propensity score-matching study. Sci. Rep. 2021, 11, 14908. [Google Scholar] [CrossRef]
- Zhu, J.; Huang, R.; Yu, P.; Ren, H.; Su, X. Male Gender Is Associated with Lymph Node Metastasis but Not with Recurrence in Papillary Thyroid Carcinoma. Int. J. Endocrinol. 2022, 2022, 3534783. [Google Scholar] [CrossRef]
- Hei, H.; Zhou, B.; Gong, W.; Zheng, C.; Qin, J. Male patients with papillary thyroid cancer have a higher risk of extranodal extension. Int. J. Clin. Oncol. 2022, 27, 648–654. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Gajowiec, A.; Chromik, A.; Furga, K.; Skuza, A.; Gąsior-Perczak, D.; Walczyk, A.; Pałyga, I.; Trybek, T.; Mikina, E.; Szymonek, M.; et al. Is Male Sex A Prognostic Factor in Papillary Thyroid Cancer? J. Clin. Med. 2021, 10, 2438. [Google Scholar] [CrossRef]
- Ding, J.; Wu, W.; Fang, J.; Zhao, J.; Jiang, L. Male sex is associated with aggressive behaviour and poor prognosis in Chinese papillary thyroid carcinoma. Sci. Rep. 2020, 10, 1–8. [Google Scholar]
- Sapuppo, G.; Tavarelli, M.; Belfiore, A.; Vigneri, R.; Pellegriti, G. Time to Separate Persistent From Recurrent Differentiated Thyroid Cancer: Different Conditions With Different Outcomes. J. Clin. Endocrinol. Metab. 2019, 104, 258–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Lee, Y.M.; Sung, T.Y.; Yoon, J.H.; Song, D.E.; Kim, T.Y.; Baek, J.H.; Ryu, J.S.; Chung, K.W.; Hong, S.J. Is Male Gender a Prognostic Factor for Papillary Thyroid Microcarcinoma? Ann. Surg. Oncol. 2017, 24, 1958–1964. [Google Scholar] [CrossRef]
- Jonklaas, J.; Nogueras-Gonzalez, G.; Munsell, M.; Litofsky, D.; Ain, K.B.; Bigos, S.T.; Brierley, J.D.; Cooper, D.S.; Haugen, B.R.; Ladenson, P.W.; et al. The impact of age and gender on papillary thyroid cancer survival. J. Clin. Endocrinol. Metab. 2012, 97, E878–E887. [Google Scholar] [CrossRef] [PubMed]
- Oyer, S.L.; Smith, V.A.; Lentsch, E.J. Sex is not an independent risk factor for survival in differentiated thyroid cancer. Laryngoscope 2013, 123, 2913–2919. [Google Scholar] [CrossRef]
- Woo, J.; Kim, H.; Kwon, H. Impact of Multifocality on the Recurrence of Papillary Thyroid Carcinoma. J. Clin. Med. 2021, 10, 5144. [Google Scholar] [CrossRef]
- Kim, Y.; Roh, J.L.; Song, D.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Predictors of recurrence after total thyroidectomy plus neck dissection and radioactive iodine ablation for high-risk papillary thyroid carcinoma. J. Surg. Oncol. 2020, 122, 906–913. [Google Scholar] [CrossRef]
- Taboni, S.; Paderno, A.; Giordano, D.; Albano, D.; Piana, S.; Zanetti, E.; Bertagna, F.; Grammatica, A.; Ghidini, A.; Cappelli, C.; et al. Differentiated Thyroid Cancer: The Role of ATA Nodal Risk Factors in N1b Patients. Laryngoscope 2021, 131, E1029–E1034. [Google Scholar] [CrossRef]
- Nilubol, N.; Zhang, L.; Kebebew, E. Multivariate analysis of the relationship between male sex, disease-specific survival, and features of tumor aggressiveness in thyroid cancer of follicular cell origin. Thyroid 2013, 23, 695–702. [Google Scholar] [CrossRef]
- Wang, F.; Zhao, S.; Shen, X.; Zhu, G.; Liu, R.; Viola, D.; Elisei, R.; Puxeddu, E.; Fugazzola, L.; Colombo, C.; et al. BRAF V600E confers male sex disease-specific mortality risk in patients with papillary thyroid cancer. J. Clin. Oncol. 2018, 36, 2787–2795. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Male (n = 157) | Female (n = 1095) | p-Value |
|---|---|---|---|
| Age (years) | 46.7 ± 11.2 | 47.6 ± 11.3 | 0.322 |
| Pathologic characteristics | |||
| Tumor size (cm) | 1.3 ± 0.9 | 1.0 ± 0.6 | <0.001 |
| Extrathyroidal extension | 0.018 | ||
| No | 56 (35.7%) | 425 (38.8%) | |
| Microscopic | 98 (62.4%) | 667 (60.9%) | |
| Gross | 3 (1.9%) | 3 (0.3%) | |
| Multifocality | 64 (40.8%) | 428 (39.1%) | 0.687 |
| LN metastasis | 0.001 | ||
| N0 | 73 (46.5%) | 650 (59.4%) | |
| N1a | 58 (36.9%) | 350 (32.0%) | |
| N1b | 26 (16.6%) | 95 (8.7%) | |
| Margin involvement | 5 (3.2%) | 38 (3.5%) | 0.854 |
| Coexisting HT | 21 (13.4%) | 332 (30.3%) | <0.001 |
| Postoperative management | |||
| 131I remnant ablation | 77 (49.0%) | 466 (42.6%) | 0.125 |
| 131I dose (mCi) | 144.1 ± 33.1 | 132.5 ± 35.4 | 0.006 |
| Follow-up period (years) | 6.2 ± 3.0 | 6.6 ± 3.2 | 0.078 |
| Recurrence | 7 (4.5%) | 20 (1.8%) | 0.034 |
| Characteristics | Male (n = 157) | Female (n = 471) | p-Value |
|---|---|---|---|
| Age (years) | 46.7 ± 11.2 | 47.6 ± 12.0 | 0.397 |
| Pathologic characteristics | |||
| Tumor size (cm) | 1.3 ± 0.9 | 1.2 ± 0.8 | 0.258 |
| Extrathyroidal extension | 0.134 | ||
| No | 56 (35.7%) | 153 (32.5%) | |
| Microscopic | 98 (62.4%) | 316 (67.1%) | |
| Gross | 3 (1.9%) | 2 (0.4%) | |
| Multifocality | 64 (40.8%) | 197 (41.8%) | 0.815 |
| LN metastasis | 0.503 | ||
| N0 | 73 (46.5%) | 200 (42.5%) | |
| N1a | 58 (36.9%) | 199 (42.3%) | |
| N1b | 26 (16.6%) | 72 (15.3%) | |
| Margin involvement | 5 (3.2%) | 22 (4.7%) | 0.427 |
| Coexisting HT | 21 (13.4%) | 58 (12.3%) | 0.728 |
| Postoperative management | |||
| 131I remnant ablation | 77 (49.0%) | 263 (55.8%) | 0.139 |
| 131I dose (mCi) | 144.1 ± 33.1 | 135.4 ± 35.0 | 0.054 |
| Follow-up period (years) | 6.2 ± 3.0 | 5.6 ± 3.1 | 0.037 |
| Recurrence | 7 (4.5%) | 15 (3.2%) | 0.452 |
| Characteristics | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (years) | 0.987 (0.952–1.023) | 0.470 | ||
| Male sex | 2.526 (1.068–5.976) | 0.035 | 1.982 (0.831–4.726) | 0.123 |
| Tumor size (cm) | 1.841 (1.319–2.567) | <0.001 | 1.504 (0.995–2.275) | 0.053 |
| Extrathyroidal extension | ||||
| Microscopic | 2.894 (1.096–7.644) | 0.032 | 1.858 (0.682–5.060) | 0.226 |
| Gross | <0.01 (0.0–infinite) | 0.985 | 0.000 (0.0–infinite) | 0.979 |
| Multifocality | 2.390 (1.109–5.151) | 0.026 | 2.105 (0.972-4.558) | 0.059 |
| LN metastasis | ||||
| N1a | 2.166 (0.855–5.490) | 0.103 | 1.642 (0.640–4.213) | 0.302 |
| N1b | 7.938 (3.061–20.57) | <0.001 | 4.204 (1.483–11.92) | 0.007 |
| Margin involvement | 2.860 (0.677–12.08) | 0.153 | 2.062 (0.475–8.953) | 0.334 |
| Hashimoto thyroiditis | 0.602 (0.228–1.589) | 0.305 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Kwon, H.; Moon, B.-I. Predictors of Recurrence in Patients with Papillary Thyroid Carcinoma: Does Male Sex Matter? Cancers 2022, 14, 1896. https://doi.org/10.3390/cancers14081896
Kim H, Kwon H, Moon B-I. Predictors of Recurrence in Patients with Papillary Thyroid Carcinoma: Does Male Sex Matter? Cancers. 2022; 14(8):1896. https://doi.org/10.3390/cancers14081896
Chicago/Turabian StyleKim, Hyeji, Hyungju Kwon, and Byung-In Moon. 2022. "Predictors of Recurrence in Patients with Papillary Thyroid Carcinoma: Does Male Sex Matter?" Cancers 14, no. 8: 1896. https://doi.org/10.3390/cancers14081896
APA StyleKim, H., Kwon, H., & Moon, B.-I. (2022). Predictors of Recurrence in Patients with Papillary Thyroid Carcinoma: Does Male Sex Matter? Cancers, 14(8), 1896. https://doi.org/10.3390/cancers14081896