
Associations between Pre-Diagnostic Physical Activity with Breast Cancer Characteristics and Survival

 , , , , ,
, , , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
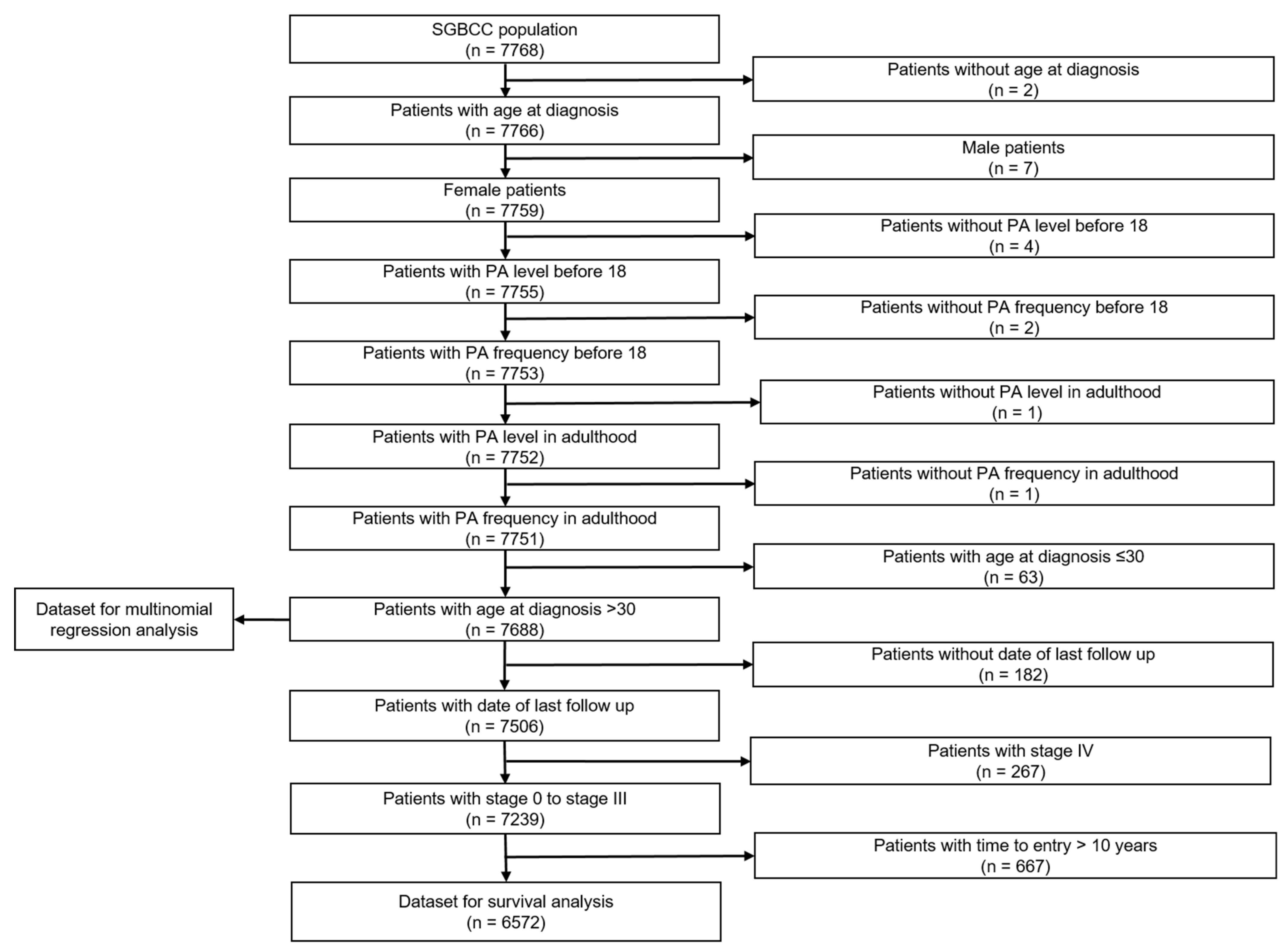
2.1. Study Population
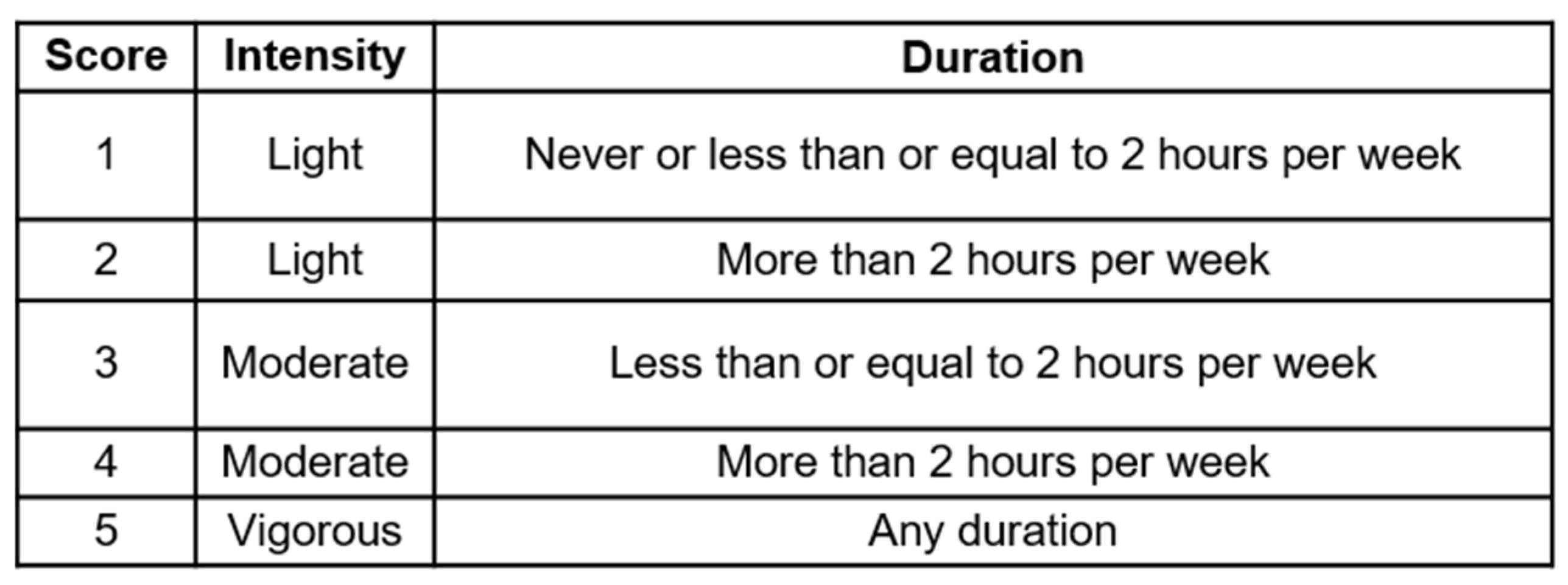
2.2. Assessment of PA
2.3. Demographics and Breast Cancer Risk Factor Data
2.4. Clinical Data
2.5. Passive Follow-Up
2.6. Exclusions
2.7. Statistical Analysis
3. Results
3.1. Pre-Diagnostic PA and Disease Characteristics
3.2. Pre-Diagnostic PA and Survival
3.3. Subset Analysis by Menopausal Status
3.4. Subset Analysis by PA Intensity and Duration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | breast cancer |
| BMI | body mass index, kg/m2 |
| CI | confidence interval |
| ER | estrogen receptor |
| HER2 | human epidermal growth factor receptor 2 |
| HR | hazard ratio |
| OR | odds ratio |
| PA | physical activity |
| PR | progesterone receptor |
| SD | standard deviation |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, S.S.; Thygesen, L.C.; Tolstrup, J.S.; Gronbaek, M. Modifiable risk factors and survival in women diagnosed with primary breast cancer: Results from a prospective cohort study. Eur. J. Cancer Prev. 2010, 19, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Killelea, B.K.; Gallagher, E.J.; Feldman, S.M.; Port, E.; King, T.; Boolbol, S.K.; Franco, R.; Fei, K.; Le Roith, D.; Bickell, N.A. The effect of modifiable risk factors on breast cancer aggressiveness among black and white women. Am. J. Surg. 2019, 218, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Pizot, C.; Boniol, M.; Mullie, P.; Koechlin, A.; Boniol, M.; Boyle, P.; Autier, P. Physical activity, hormone replacement therapy and breast cancer risk: A meta-analysis of prospective studies. Eur. J. Cancer 2016, 52, 138–154. [Google Scholar] [CrossRef] [Green Version]
- Spei, M.E.; Samoli, E.; Bravi, F.; La Vecchia, C.; Bamia, C.; Benetou, V. Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast 2019, 44, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Holmes, M.D.; Chen, W.Y.; Feskanich, D.; Kroenke, C.H.; Colditz, G.A. Physical activity and survival after breast cancer diagnosis. JAMA 2005, 293, 2479–2486. [Google Scholar] [CrossRef] [Green Version]
- Carmichael, A.R.; Daley, A.J.; Rea, D.W.; Bowden, S.J. Physical activity and breast cancer outcome: A brief review of evidence, current practice and future direction. Eur. J. Surg. Oncol. 2010, 36, 1139–1148. [Google Scholar] [CrossRef] [Green Version]
- Cleveland, R.J.; Eng, S.M.; Stevens, J.; Bradshaw, P.T.; Teitelbaum, S.L.; Neugut, A.I.; Gammon, M.D. Influence of prediagnostic recreational physical activity on survival from breast cancer. Eur. J. Cancer Prev. 2012, 21, 46–54. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Research Foundation/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective; World Cancer Research Fund and American Institute for Cancer Research: Washington, DC, USA, 2018; Available online: Dietandcancerreport.org (accessed on 7 February 2022).
- Li, T.; Wei, S.; Shi, Y.; Pang, S.; Qin, Q.; Yin, J.; Deng, Y.; Chen, Q.; Wei, S.; Nie, S.; et al. The dose-response effect of physical activity on cancer mortality: Findings from 71 prospective cohort studies. Br. J. Sports Med. 2016, 50, 339–345. [Google Scholar] [CrossRef]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef]
- Friedenreich, C.M. The role of physical activity in breast cancer etiology. Semin. Oncol. 2010, 37, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Ho, P.J.; Yeoh, Y.S.; Miao, H.; Lim, S.H.; Tan, E.Y.; Tan, B.K.T.; Tan, V.K.M.; Tan, S.M.; Yong, W.S.; Wong, F.Y.; et al. Cohort profile: The Singapore Breast Cancer Cohort (SGBCC), a multi-center breast cancer cohort for evaluation of phenotypic risk factors and genetic markers. PLoS ONE 2021, 16, e0250102. [Google Scholar] [CrossRef] [PubMed]
- Gabrielson, M.; Eriksson, M.; Hammarstrom, M.; Borgquist, S.; Leifland, K.; Czene, K.; Hall, P. Cohort Profile: The Karolinska Mammography Project for Risk Prediction of Breast Cancer (KARMA). Int. J. Epidemiol. 2017, 46, 1740–1741. [Google Scholar] [CrossRef] [PubMed]
- Keshtkar, A.A.; Semnani, S.; Pourshams, A.; Khademi, H.; Roshandel, G.; Boffetta, P.; Malekzadeh, R. Pictogram use was validated for estimating individual’s body mass index. J. Clin. Epidemiol. 2010, 63, 655–659. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Sorensen, T.; Schulsinger, F. Use of the Danish Adoption Register for the study of obesity and thinness. Res. Publ. Assoc. Res. Nerv. Ment. Dis. 1983, 60, 115–120. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Wood, W.C.; Coates, A.S.; Gelber, R.D.; Thurlimann, B.; Senn, H.J. Strategies for subtypes—Dealing with the diversity of breast cancer: Highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann. Oncol. 2011, 22, 1736–1747. [Google Scholar] [CrossRef]
- Patel, A.V.; Hildebrand, J.S.; Campbell, P.T.; Teras, L.R.; Craft, L.L.; McCullough, M.L.; Gapstur, S.M. Leisure-Time Spent Sitting and Site-Specific Cancer Incidence in a Large U.S. Cohort. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1350–1359. [Google Scholar] [CrossRef] [Green Version]
- Huerta, J.M.; Molina, A.J.; Chirlaque, M.D.; Yepes, P.; Moratalla-Navarro, F.; Moreno, V.; Amiano, P.; Guevara, M.; Moreno-Iribas, C.; Llorca, J.; et al. Domain-specific patterns of physical activity and risk of breast cancer sub-types in the MCC-Spain study. Breast Cancer Res. Treat. 2019, 177, 749–760. [Google Scholar] [CrossRef]
- Shi, J.; Kobayashi, L.C.; Grundy, A.; Richardson, H.; SenGupta, S.K.; Lohrisch, C.A.; Spinelli, J.J.; Aronson, K.J. Lifetime moderate-to-vigorous physical activity and ER/PR/HER-defined post-menopausal breast cancer risk. Breast Cancer Res. Treat. 2017, 165, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Steindorf, K.; Mutschelknauss, E.; Slanger, T.; Kropp, S.; Obi, N.; Flesch-Janys, D.; Chang-Claude, J. Physical activity and postmenopausal breast cancer: Effect modification by breast cancer subtypes and effective periods in life. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3402–3410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, S.W.; Tabar, L.; Yen, A.M.; Dean, P.B.; Smith, R.A.; Jonsson, H.; Tornberg, S.; Chen, S.L.; Chiu, S.Y.; Fann, J.C.; et al. Mammography screening reduces rates of advanced and fatal breast cancers: Results in 549,091 women. Cancer 2020, 126, 2971–2979. [Google Scholar] [CrossRef] [PubMed]
- Webb, M.L.; Cady, B.; Michaelson, J.S.; Bush, D.M.; Calvillo, K.Z.; Kopans, D.B.; Smith, B.L. A failure analysis of invasive breast cancer: Most deaths from disease occur in women not regularly screened. Cancer 2014, 120, 2839–2846. [Google Scholar] [CrossRef] [PubMed]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies. Acta Oncol. 2015, 54, 635–654. [Google Scholar] [CrossRef] [PubMed]
- Si, S.; Boyle, T.; Heyworth, J.; Glass, D.C.; Saunders, C.; Fritschi, L. Lifetime physical activity and risk of breast cancer in pre-and post-menopausal women. Breast Cancer Res. Treat. 2015, 152, 449–462. [Google Scholar] [CrossRef] [Green Version]
- Chollet-Hinton, L.; Anders, C.K.; Tse, C.K.; Bell, M.B.; Yang, Y.C.; Carey, L.A.; Olshan, A.F.; Troester, M.A. Breast cancer biologic and etiologic heterogeneity by young age and menopausal status in the Carolina Breast Cancer Study: A case-control study. Breast Cancer Res. 2016, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- de Boer, M.C.; Worner, E.A.; Verlaan, D.; van Leeuwen, P.A.M. The Mechanisms and Effects of Physical Activity on Breast Cancer. Clin. Breast Cancer 2017, 17, 272–278. [Google Scholar] [CrossRef]
- Winzer, B.M.; Whiteman, D.C.; Reeves, M.M.; Paratz, J.D. Physical activity and cancer prevention: A systematic review of clinical trials. Cancer Causes Control 2011, 22, 811–826. [Google Scholar] [CrossRef]
- Orlandella, F.M.; De Stefano, A.E.; Iervolino, P.L.C.; Buono, P.; Soricelli, A.; Salvatore, G. Dissecting the molecular pathways involved in the effects of physical activity on breast cancers cells: A narrative review. Life Sci. 2021, 265, 118790. [Google Scholar] [CrossRef]
- Picon-Ruiz, M.; Morata-Tarifa, C.; Valle-Goffin, J.J.; Friedman, E.R.; Slingerland, J.M. Obesity and adverse breast cancer risk and outcome: Mechanistic insights and strategies for intervention. CA Cancer J. Clin. 2017, 67, 378–397. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Shaw, E.; Neilson, H.K.; Brenner, D.R. Epidemiology and biology of physical activity and cancer recurrence. J. Mol. Med. 2017, 95, 1029–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannioto, R.A.; Dighe, S.; Mahoney, M.C.; Moysich, K.B.; Sen, A.; Hulme, K.; McCann, S.E.; Ambrosone, C.B. Habitual recreational physical activity is associated with significantly improved survival in cancer patients: Evidence from the Roswell Park Data Bank and BioRepository. Cancer Causes Control 2019, 30, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.M.; Al-Homaidh, A. Physical activity and survival after breast cancer diagnosis: Meta-analysis of published studies. Med. Oncol. 2011, 28, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Beasley, J.M.; Kwan, M.L.; Chen, W.Y.; Weltzien, E.K.; Kroenke, C.H.; Lu, W.; Nechuta, S.J.; Cadmus-Bertram, L.; Patterson, R.E.; Sternfeld, B.; et al. Meeting the physical activity guidelines and survival after breast cancer: Findings from the after breast cancer pooling project. Breast Cancer Res. Treat. 2012, 131, 637–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Physical Activity Guidelines Advisory Committee 2018. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; Department of Health & Human Services: Washington, DC, USA, 2018. Available online: https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 7 February 2022).
- Costa, E.C.; Hay, J.L.; Kehler, D.S.; Boreskie, K.F.; Arora, R.C.; Umpierre, D.; Szwajcer, A.; Duhamel, T.A. Effects of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training On Blood Pressure in Adults with Pre- to Established Hypertension: A Systematic Review and Meta-Analysis of Randomized Trials. Sports Med. 2018, 48, 2127–2142. [Google Scholar] [CrossRef]
- Sultana, R.N.; Sabag, A.; Keating, S.E.; Johnson, N.A. The Effect of Low-Volume High-Intensity Interval Training on Body Composition and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1687–1721. [Google Scholar] [CrossRef]
- Emmanuel, S. Quality assurance in medicine: Research and evaluation activities towards quality control in Singapore. Ann. Acad. Med. Singap. 1993, 22, 129–133. [Google Scholar]
- Helmerhorst, H.J.; Brage, S.; Warren, J.; Besson, H.; Ekelund, U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–55. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Pre-Diagnostic PA Score | |||||||
|---|---|---|---|---|---|---|---|
| Characteristic | Total, n = 7688 | 1 (Light, <2 h), n = 646 | 2 (Light, >2 h), n = 4874 | 3 (Moderate, <2 h), n = 568 | 4 (Moderate, >2 h), n = 801 | 5 (Vigorous), n = 799 | p-Value |
| (a) Sociodemographic, medical history, and breast cancer risk factors | |||||||
| Recruitment site a, n (%) | <0.001 | ||||||
| NUH | 2183 (28.4) | 65 (10.1) | 1586 (32.5) | 64 (11.3) | 295 (36.8) | 173 (21.7) | |
| CGH | 587 (7.6) | 250 (38.7) | 134 (2.7) | 95 (16.7) | 28 (3.5) | 80 (10.0) | |
| KKH | 1949 (25.4) | 153 (23.7) | 1229 (25.2) | 154 (27.1) | 68 (8.5) | 345 (43.2) | |
| SGHNCC | 1544 (20.1) | 45 (7.0) | 1028 (21.1) | 78 (13.7) | 278 (34.7) | 115 (14.4) | |
| TTSH | 1425 (18.5) | 133 (20.6) | 897 (18.4) | 177 (31.2) | 132 (16.5) | 86 (10.8) | |
| Age at diagnosis (years, IQR b) | <0.001 | ||||||
| Age at diagnosis (years, IQR) | 53.5 (46.5–61.1) | 52.0 (45.1–58.8) | 55.3 (47.8–62.7) | 49.9 (44.2–56.6) | 52.1 (45.5–60.4) | 49.1 (43.2–55.2) | |
| Ethnicity, n (%) | <0.001 | ||||||
| Chinese | 6089 (79.2) | 554 (85.8) | 3882 (79.6) | 445 (78.3) | 618 (77.2) | 590 (73.8) | |
| Malay | 913 (11.9) | 57 (8.8) | 565 (11.6) | 69 (12.1) | 100 (12.5) | 122 (15.3) | |
| Indian | 439 (5.7) | 16 (2.5) | 293 (6.0) | 33 (5.8) | 53 (6.6) | 44 (5.5) | |
| Other | 247 (3.2) | 19 (2.9) | 134 (2.7) | 21 (3.7) | 30 (3.7) | 43 (5.4) | |
| Body size one year prior to diagnosis, n (%) | 0.048 | ||||||
| Below average | 3641 (47.4) | 310 (48.0) | 2264 (46.5) | 293 (51.6) | 398 (49.7) | 376 (47.1) | |
| Average | 2102 (27.3) | 186 (28.8) | 1337 (27.4) | 148 (26.1) | 227 (28.3) | 204 (25.5) | |
| Above average | 1930 (25.1) | 148 (22.9) | 1265 (26.0) | 125 (22.0) | 175 (21.8) | 217 (27.2) | |
| Missing | 15 (0.2) | 2 (0.3) | 8 (0.2) | 2 (0.4) | 1 (0.1) | 2 (0.3) | |
| Menopausal status at diagnosis, n (%) | <0.001 | ||||||
| Pre-menopausal | 3671 (47.7) | 347 (53.7) | 2032 (41.7) | 351 (61.8) | 413 (51.6) | 528 (66.1) | |
| Post- menopausal | 4017 (52.3) | 299 (46.3) | 2842 (58.3) | 217 (38.2) | 388 (48.4) | 271 (33.9) | |
| Follow-up duration (years, IQR) | <0.001 | ||||||
| Follow-up duration (years, IQR) | 5.4 (3.0–9.0) | 6.4 (3.7–10.2) | 5.1 (2.9–8.6) | 6.6 (4.0–10.2) | 5.7 (2.8–9.6) | 4.8 (2.8–8.3) | |
| (b) Disease characteristics | |||||||
| Tumour behaviour, n (%) | 0.008 | ||||||
| Non-invasive | 1097 (14.3) | 80 (12.4) | 672 (13.8) | 80 (14.1) | 121 (15.1) | 144 (18.0) | |
| Invasive | 6236 (81.1) | 546 (84.5) | 3963 (81.3) | 472 (83.1) | 644 (80.4) | 611 (76.5) | |
| Missing | 355 (4.6) | 20 (3.1) | 239 (4.9) | 16 (2.8) | 36 (4.5) | 44 (5.5) | |
| Stage, n (%) | 0.01 | ||||||
| 0 | 1097 (14.3) | 80 (12.4) | 672 (13.8) | 80 (14.1) | 121 (15.1) | 144 (18.0) | |
| I | 2161 (28.1) | 209 (32.4) | 1337 (27.4) | 170 (29.9) | 226 (28.2) | 219 (27.4) | |
| II | 2658 (34.6) | 230 (35.6) | 1705 (35.0) | 205 (36.1) | 272 (34.0) | 246 (30.8) | |
| III | 1150 (15.0) | 99 (15.3) | 739 (15.2) | 76 (13.4) | 116 (14.5) | 120 (15.0) | |
| IV # | 267 (3.5) | 8 (1.2) | 182 (3.7) | 21 (3.7) | 30 (3.7) | 26 (3.3) | |
| Missing | 355 (4.6) | 20 (3.1) | 239 (4.9) | 16 (2.8) | 36 (4.5) | 44 (5.5) | |
| Grade, n (%) | 0.149 | ||||||
| Well differentiated | 1159 (15.1) | 94 (14.6) | 712 (14.6) | 96 (16.9) | 141 (17.6) | 116 (14.5) | |
| Moderately differentiated | 2766 (36.0) | 253 (39.2) | 1752 (35.9) | 223 (39.3) | 275 (34.3) | 263 (32.9) | |
| Poorly differentiated | 2834 (36.9) | 232 (35.9) | 1835 (37.6) | 189 (33.3) | 302 (37.7) | 276 (34.5) | |
| Missing | 929 (12.1) | 67 (10.4) | 575 (11.8) | 60 (10.6) | 83 (10.4) | 144 (18.0) | |
| Nodal status, n (%) | 0.777 | ||||||
| Negative | 4714 (61.3) | 403 (62.4) | 2953 (60.6) | 367 (64.6) | 492 (61.4) | 499 (62.5) | |
| Positive | 2556 (33.2) | 217 (33.6) | 1637 (33.6) | 186 (32.7) | 251 (31.3) | 265 (33.2) | |
| Missing | 418 (5.4) | 26 (4.0) | 284 (5.8) | 15 (2.6) | 58 (7.2) | 35 (4.4) | |
| Tumour size (cm), n (%) | 0.005 | ||||||
| ≤2 | 3998 (52.0) | 356 (55.1) | 2462 (50.5) | 325 (57.2) | 419 (52.3) | 436 (54.6) | |
| >2–5 | 2516 (32.7) | 212 (32.8) | 1623 (33.3) | 177 (31.2) | 261 (32.6) | 243 (30.4) | |
| >5 | 399 (5.2) | 35 (5.4) | 255 (5.2) | 29 (5.1) | 40 (5.0) | 40 (5.0) | |
| Other/missing | 775 (10.1) | 43 (6.7) | 534 (11.0) | 37 (6.5) | 81 (10.1) | 80 (10.0) | |
| Estrogen receptor status, n (%) | 0.469 | ||||||
| Positive | 4957 (64.5) | 430 (66.6) | 3108 (63.8) | 370 (65.1) | 542 (67.7) | 507 (63.5) | |
| Negative | 1536 (20.0) | 132 (20.4) | 1001 (20.5) | 107 (18.8) | 153 (19.1) | 143 (17.9) | |
| Missing | 1195 (15.5) | 84 (13.0) | 765 (15.7) | 91 (16.0) | 106 (13.2) | 149 (18.6) | |
| Progesterone receptor status, n (%) | 0.067 | ||||||
| Positive | 4368 (56.8) | 365 (56.5) | 2756 (56.5) | 308 (54.2) | 489 (61.0) | 450 (56.3) | |
| Negative | 2067 (26.9) | 193 (29.9) | 1317 (27.0) | 168 (29.6) | 200 (25.0) | 189 (23.7) | |
| Missing | 1253 (16.3) | 88 (13.6) | 801 (16.4) | 92 (16.2) | 112 (14.0) | 160 (20.0) | |
| HER2 status, n (%) | 0.006 | ||||||
| Positive | 1490 (19.4) | 169 (26.2) | 929 (19.1) | 103 (18.1) | 158 (19.7) | 131 (16.4) | |
| Negative | 3762 (48.9) | 310 (48.0) | 2380 (48.8) | 281 (49.5) | 400 (49.9) | 391 (48.9) | |
| Missing | 2436 (31.7) | 167 (25.9) | 1565 (32.1) | 184 (32.4) | 243 (30.3) | 277 (34.7) | |
| Subtype, n (%) | 0.014 | ||||||
| Luminal A | 2294 (29.8) | 206 (31.9) | 1446 (29.7) | 178 (31.3) | 240 (30.0) | 224 (28.0) | |
| Luminal B | 1018 (13.2) | 76 (11.8) | 654 (13.4) | 69 (12.1) | 125 (15.6) | 94 (11.8) | |
| Luminal HER2-like | 618 (8.0) | 73 (11.3) | 374 (7.7) | 38 (6.7) | 75 (9.4) | 58 (7.3) | |
| HER2 overexpressed | 545 (7.1) | 70 (10.8) | 334 (6.9) | 45 (7.9) | 49 (6.1) | 47 (5.9) | |
| Triple negative | 552 (7.2) | 40 (6.2) | 364 (7.5) | 41 (7.2) | 49 (6.1) | 58 (7.3) | |
| Missing | 2661 (34.6) | 181 (28.0) | 1702 (34.9) | 197 (34.7) | 263 (32.8) | 318 (39.8) | |
| Pre-Diagnostic PA Score | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (Light, <2 h) | 2 (Light, >2 h) | 3 (Moderate, <2 h) | 4 (Moderate, >2 h) | 5 (Vigorous) | Continuous PA Score | ||||||||||||
| N | OR (95% CI) | p | N | N | OR (95% CI) | p | N | OR (95% CI) | p | N | OR (95% CI) | p | N | OR (95% CI) | p | ||
| Tumour behaviour | |||||||||||||||||
| Non-invasive | 80 | 672 | 1.00 (Reference) | 80 | 121 | 144 | 1097 | 1.00 (Reference) | |||||||||
| Invasive | 546 | 1.12 (0.86 to 1.47) | 0.394 | 3963 | 472 | 1.02 (0.79 to 1.32) | 0.867 | 644 | 0.93 (0.75 to 1.15) | 0.512 | 611 | 0.71 (0.58 to 0.87) | 0.001 | 6236 | 0.91 (0.86 to 0.97) | 0.001 | |
| Missing | 20 | 239 | 16 | 36 | 44 | 355 | |||||||||||
| Other disease characteristics of patients with invasive cancer (n = 6236) | |||||||||||||||||
| Stage | |||||||||||||||||
| I | 209 | 1337 | 1.00 (Reference) | 170 | 226 | 219 | 2161 | 1.00 (Reference) | |||||||||
| II | 230 | 0.83 (0.66 to 1.04) | 0.098 | 1705 | 205 | 0.91 (0.73 to 1.14) | 0.407 | 272 | 1.03 (0.85 to 1.25) | 0.785 | 246 | 0.80 (0.65 to 0.98) | 0.028 | 2658 | 0.98 (0.93 to 1.03) | 0.352 | |
| III | 99 | 0.87 (0.65 to 1.15) | 0.332 | 739 | 76 | 0.81 (0.60 to 1.09) | 0.171 | 116 | 1.01 (0.79 to 1.30) | 0.914 | 120 | 0.97 (0.75 to 1.24) | 0.79 | 1150 | 1.00 (0.94 to 1.07) | 0.897 | |
| IV | 8 | 0.42 (0.20 to 0.89) | 0.023 | 182 | 21 | 1.07 (0.65 to 1.76) | 0.795 | 30 | 1.05 (0.69 to 1.59) | 0.83 | 26 | 1.00 (0.64 to 1.57) | 0.998 | 267 | 1.07 (0.95 to 1.20) | 0.291 | |
| Grade | |||||||||||||||||
| Well differentiated | 79 | 570 | 1.00 (Reference) | 80 | 105 | 94 | 928 | 1.00 (Reference) | |||||||||
| Moderately differentiated | 223 | 1.00 (0.75 to 1.35) | 0.982 | 1507 | 193 | 0.88 (0.66 to 1.17) | 0.382 | 230 | 0.82 (0.63 to 1.05) | 0.118 | 228 | 0.89 (0.68 to 1.16) | 0.375 | 2381 | 0.95 (0.88 to 1.01) | 0.117 | |
| Poorly differentiated | 213 | 0.83 (0.61 to 1.12) | 0.216 | 1619 | 171 | 0.69 (0.52 to 0.93) | 0.014 | 259 | 0.84 (0.66 to 1.08) | 0.176 | 242 | 0.81 (0.62 to 1.05) | 0.112 | 2504 | 0.94 (0.88 to 1.01) | 0.096 | |
| Missing | 31 | 267 | 28 | 50 | 47 | 423 | |||||||||||
| Nodal status | |||||||||||||||||
| Negative | 323 | 2252 | 1.00 (Reference) | 283 | 376 | 342 | 3576 | 1.00 (Reference) | |||||||||
| Positive | 217 | 0.92 (0.75 to 1.13) | 0.435 | 1634 | 184 | 0.85 (0.69 to 1.04) | 0.122 | 250 | 0.97 (0.82 to 1.16) | 0.752 | 264 | 1.00 (0.84 to 1.20) | 0.969 | 2549 | 1.00 (0.95 to 1.05) | 0.99 | |
| Missing | 6 | 77 | 5 | 18 | 5 | 111 | |||||||||||
| Tumour size (cm) | |||||||||||||||||
| ≤2 | 276 | 1794 | 1.00 (Reference) | 243 | 300 | 292 | 2905 | 1.00 (Reference) | |||||||||
| >2–5 | 212 | 0.87 (0.71 to 1.08) | 0.199 | 1613 | 176 | 0.82 (0.66 to 1.01) | 0.066 | 260 | 1.04 (0.87 to 1.25) | 0.666 | 243 | 0.90 (0.74 to 1.09) | 0.281 | 2504 | 0.99 (0.94 to 1.04) | 0.757 | |
| >5 | 34 | 0.80 (0.52 to 1.22) | 0.298 | 251 | 28 | 0.77 (0.50 to 1.18) | 0.23 | 39 | 0.91 (0.63 to 1.31) | 0.613 | 39 | 0.88 (0.61 to 1.27) | 0.495 | 391 | 0.98 (0.89 to 1.08) | 0.645 | |
| Other/missing | 24 | 305 | 25 | 45 | 37 | 436 | |||||||||||
| Estrogen receptor status | |||||||||||||||||
| Positive | 379 | 2722 | 1.00 (Reference) | 322 | 469 | 416 | 4308 | 1.00 (Reference) | |||||||||
| Negative | 122 | 0.92 (0.72 to 1.17) | 0.473 | 884 | 98 | 0.88 (0.69 to 1.13) | 0.323 | 130 | 0.81 (0.66 to 1.01) | 0.057 | 114 | 0.83 (0.66 to 1.05) | 0.115 | 1348 | 0.94 (0.89 to 1.00) | 0.049 | |
| Missing | 45 | 357 | 52 | 45 | 81 | 580 | |||||||||||
| Progesterone receptor status | |||||||||||||||||
| Positive | 322 | 2434 | 1.00 (Reference) | 268 | 429 | 371 | 3824 | 1.00 (Reference) | |||||||||
| Negative | 177 | 1.02 (0.82 to 1.26) | 0.883 | 1156 | 151 | 1.06 (0.85 to 1.32) | 0.599 | 167 | 0.82 (0.67 to 0.99) | 0.041 | 156 | 0.88 (0.71 to 1.08) | 0.207 | 1807 | 0.95 (0.90 to 1.00) | 0.051 | |
| Missing | 47 | 373 | 53 | 48 | 84 | 605 | |||||||||||
| HER2 status | |||||||||||||||||
| Positive | 154 | 875 | 1.00 (Reference) | 95 | 145 | 114 | 1383 | 1.00 (Reference) | |||||||||
| Negative | 289 | 0.82 (0.65 to 1.03) | 0.093 | 2247 | 270 | 1.24 (0.96 to 1.60) | 0.098 | 382 | 1.09 (0.88 to 1.34) | 0.419 | 353 | 1.29 (1.02 to 1.62) | 0.033 | 3541 | 1.10 (1.03 to 1.16) | 0.002 | |
| Missing | 103 | 841 | 107 | 117 | 144 | 1312 | |||||||||||
| Subtype | |||||||||||||||||
| Luminal A | 190 | 1375 | 1.00 (Reference) | 174 | 232 | 213 | 2184 | 1.00 (Reference) | |||||||||
| Luminal B | 76 | 0.81 (0.59 to 1.10) | 0.18 | 635 | 65 | 0.80 (0.58 to 1.09) | 0.149 | 120 | 1.10 (0.86 to 1.40) | 0.457 | 89 | 0.84 (0.64 to 1.11) | 0.223 | 985 | 0.99 (0.93 to 1.07) | 0.861 | |
| Luminal HER2-like | 66 | 1.10 (0.78 to 1.55) | 0.587 | 356 | 36 | 0.69 (0.46 to 1.01) | 0.059 | 71 | 1.05 (0.78 to 1.41) | 0.729 | 53 | 0.85 (0.61 to 1.19) | 0.347 | 582 | 0.95 (0.88 to 1.04) | 0.265 | |
| HER2 overexpressed | 63 | 1.13 (0.80 to 1.61) | 0.492 | 307 | 40 | 0.84 (0.58 to 1.23) | 0.374 | 43 | 0.80 (0.56 to 1.14) | 0.222 | 38 | 0.73 (0.50 to 1.06) | 0.101 | 491 | 0.89 (0.81 to 0.98) | 0.018 | |
| Triple negative | 39 | 0.66 (0.44 to 0.99) | 0.046 | 342 | 40 | 0.79 (0.54 to 1.16) | 0.235 | 45 | 0.75 (0.53 to 1.06) | 0.109 | 51 | 0.89 (0.63 to 1.24) | 0.487 | 517 | 0.98 (0.89 to 1.07) | 0.586 | |
| Missing | 112 | 948 | 117 | 133 | 167 | 1477 | |||||||||||
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| (a) Overall survival | ||||
| Pre-diagnostic PA (continuous) | ||||
| 0.93 (0.85 to 1.02) | 0.112 | 0.98 (0.89 to 1.08) | 0.647 | |
| Age at diagnosis | ||||
| 1.03 (1.02 to 1.04) | <0.001 | 1.03 (1.02 to 1.04) | <0.001 | |
| Recruitment site a | ||||
| NUH | 1.00 (Reference) | 1.00 (Reference) | ||
| CGH | 0.64 (0.35 to 1.17) | 0.146 | 0.63 (0.34 to 1.16) | 0.14 |
| KKH | 0.59 (0.46 to 0.76) | <0.001 | 0.62 (0.48 to 0.80) | <0.001 |
| SGHNCC | 1.42 (1.04 to 1.95) | 0.028 | 1.40 (1.03 to 1.92) | 0.034 |
| TTSH | 0.98 (0.75 to 1.29) | 0.893 | 0.91 (0.69 to 1.20) | 0.513 |
| (b) Breast cancer specific survival | ||||
| Pre-diagnostic PA (continuous) | ||||
| 0.93 (0.83 to 1.05) | 0.247 | 0.96 (0.84 to 1.09) | 0.495 | |
| Age at diagnosis | ||||
| 1.02 (1.00 to 1.03) | 0.012 | 1.01 (1.00 to 1.03) | 0.035 | |
| Recruitment site | ||||
| NUH | 1.00 (Reference) | 1.00 (Reference) | ||
| CGH | 0.00 (0.00 to Inf) | 0.992 | 0.00 (0.00 to Inf) | 0.992 |
| KKH | 0.57 (0.42 to 0.77) | <0.001 | 0.58 (0.43 to 0.79) | <0.001 |
| SGHNCC | 0.00 (0.00 to Inf) | 0.988 | 0.00 (0.00 to Inf) | 0.988 |
| TTSH | 0.95 (0.69 to 1.32) | 0.777 | 0.92 (0.66 to 1.27) | 0.604 |
| Pre-Diagnostic PA Score | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (Light, <2 h) | 2 (Light, >2 h) | 3 (Moderate, <2 h) | 4 (Moderate, >2 h) | 5 (Vigorous) | Continuous PA score | ||||||||||||
| N | OR (95% CI) | p | N | N | OR (95% CI) | p | N | OR (95% CI) | p | N | OR (95% CI) | p | N | OR (95% CI) | p | ||
| (a) Pre-menopausal breast cancer (n = 3671) | |||||||||||||||||
| Tumour behaviour | |||||||||||||||||
| Non-invasive | 49 | 314 | 1.00 (Reference) | 52 | 58 | 98 | 571 | 1.00 (Reference) | |||||||||
| Invasive | 285 | 0.98 (0.69 to 1.39) | 0.924 | 1612 | 288 | 1.01 (0.73 to 1.41) | 0.944 | 334 | 1.14 (0.83 to 1.55) | 0.42 | 403 | 0.73 (0.56 to 0.94) | 0.016 | 2922 | 0.94 (0.87 to 1.01) | 0.11 | |
| Missing | 13 | 106 | 11 | 21 | 27 | 178 | |||||||||||
| Other disease characteristics of patients with invasive cancer (n = 2922) | |||||||||||||||||
| Stage | |||||||||||||||||
| I | 123 | 567 | 1.00 (Reference) | 102 | 112 | 143 | 1047 | 1.00 (Reference) | |||||||||
| II | 111 | 0.68 (0.50 to 0.92) | 0.014 | 739 | 129 | 0.97 (0.72 to 1.30) | 0.846 | 151 | 1.09 (0.83 to 1.43) | 0.533 | 171 | 0.86 (0.67 to 1.11) | 0.255 | 1301 | 1.02 (0.95 to 1.09) | 0.628 | |
| III | 46 | 0.84 (0.56 to 1.26) | 0.397 | 255 | 41 | 0.88 (0.59 to 1.33) | 0.551 | 60 | 1.24 (0.87 to 1.77) | 0.229 | 74 | 1.08 (0.78 to 1.50) | 0.634 | 476 | 1.06 (0.97 to 1.16) | 0.197 | |
| IV | 5 | 0.70 (0.26 to 1.90) | 0.488 | 51 | 16 | 2.09 (1.11 to 3.94) | 0.023 | 11 | 1.08 (0.54 to 2.17) | 0.82 | 15 | 1.29 (0.69 to 2.39) | 0.425 | 98 | 1.12 (0.95 to 1.33) | 0.189 | |
| Grade | |||||||||||||||||
| Well differentiated | 47 | 252 | 1.00 (Reference) | 45 | 51 | 63 | 458 | 1.00 (Reference) | |||||||||
| Moderately differentiated | 114 | 0.99 (0.67 to 1.48) | 0.968 | 615 | 118 | 1.09 (0.74 to 1.61) | 0.648 | 117 | 0.92 (0.64 to 1.32) | 0.634 | 150 | 0.94 (0.67 to 1.31) | 0.716 | 1114 | 0.98 (0.89 to 1.07) | 0.676 | |
| Poorly differentiated | 105 | 0.78 (0.52 to 1.16) | 0.22 | 634 | 103 | 0.87 (0.59 to 1.29) | 0.482 | 136 | 1.05 (0.73 to 1.50) | 0.803 | 159 | 0.90 (0.64 to 1.25) | 0.528 | 1137 | 1.00 (0.92 to 1.10) | 0.938 | |
| Missing | 19 | 111 | 22 | 30 | 31 | 213 | |||||||||||
| Nodal status | |||||||||||||||||
| Negative | 179 | 946 | 1.00 (Reference) | 170 | 195 | 223 | 1713 | 1.00 (Reference) | |||||||||
| Positive | 104 | 0.84 (0.63 to 1.11) | 0.222 | 641 | 114 | 0.94 (0.72 to 1.22) | 0.627 | 131 | 1.04 (0.81 to 1.34) | 0.743 | 177 | 1.09 (0.87 to 1.37) | 0.469 | 1167 | 1.04 (0.98 to 1.11) | 0.212 | |
| Missing | 2 | 25 | 4 | 8 | 3 | 42 | |||||||||||
| Tumour size | |||||||||||||||||
| ≤2 cm | 162 | 763 | 1.00 (Reference) | 146 | 151 | 194 | 1416 | 1.00 (Reference) | |||||||||
| >2–5 cm | 97 | 0.72 (0.54 to 0.97) | 0.033 | 649 | 107 | 0.89 (0.67 to 1.18) | 0.426 | 135 | 1.10 (0.85 to 1.43) | 0.477 | 165 | 0.96 (0.76 to 1.22) | 0.755 | 1153 | 1.03 (0.97 to 1.10) | 0.33 | |
| >5 cm | 21 | 0.85 (0.49 to 1.49) | 0.577 | 109 | 18 | 0.85 (0.49 to 1.48) | 0.558 | 23 | 1.04 (0.63 to 1.70) | 0.886 | 21 | 0.74 (0.44 to 1.22) | 0.235 | 192 | 0.95 (0.84 to 1.09) | 0.477 | |
| Other/missing | 5 | 91 | 17 | 25 | 23 | 161 | |||||||||||
| Estrogen receptor status | |||||||||||||||||
| Positive | 197 | 1092 | 1.00 (Reference) | 207 | 239 | 266 | 2001 | 1.00 (Reference) | |||||||||
| Negative | 62 | 0.88 (0.63 to 1.24) | 0.477 | 344 | 47 | 0.70 (0.49 to 0.99) | 0.046 | 68 | 0.86 (0.64 to 1.17) | 0.337 | 75 | 0.91 (0.68 to 1.21) | 0.502 | 596 | 0.97 (0.89 to 1.04) | 0.387 | |
| Missing | 26 | 176 | 34 | 27 | 62 | 325 | |||||||||||
| Progesterone receptor status | |||||||||||||||||
| Positive | 179 | 1012 | 1.00 (Reference) | 176 | 231 | 250 | 1848 | 1.00 (Reference) | |||||||||
| Negative | 80 | 0.85 (0.62 to 1.16) | 0.305 | 419 | 77 | 0.90 (0.67 to 1.22) | 0.507 | 76 | 0.80 (0.60 to 1.07) | 0.137 | 89 | 0.80 (0.61 to 1.06) | 0.119 | 741 | 0.95 (0.88 to 1.02) | 0.137 | |
| Missing | 26 | 181 | 35 | 27 | 64 | 333 | |||||||||||
| HER2 status | |||||||||||||||||
| Positive | 78 | 328 | 1.00 (Reference) | 59 | 66 | 71 | 602 | 1.00 (Reference) | |||||||||
| Negative | 144 | 0.81 (0.58 to 1.13) | 0.206 | 855 | 155 | 1.11 (0.80 to 1.56) | 0.531 | 200 | 1.21 (0.89 to 1.65) | 0.225 | 226 | 1.29 (0.95 to 1.75) | 0.098 | 1580 | 1.11 (1.02 to 1.20) | 0.01 | |
| Missing | 63 | 429 | 74 | 68 | 106 | 740 | |||||||||||
| Subtype | |||||||||||||||||
| Luminal A | 94 | 542 | 1.00 (Reference) | 103 | 116 | 137 | 992 | 1.00 (Reference) | |||||||||
| Luminal B | 37 | 0.89 (0.57 to 1.39) | 0.598 | 219 | 40 | 0.94 (0.62 to 1.41) | 0.754 | 64 | 1.33 (0.94 to 1.89) | 0.104 | 49 | 0.83 (0.57 to 1.20) | 0.329 | 409 | 1.01 (0.92 to 1.11) | 0.871 | |
| Luminal HER2-like | 39 | 1.36 (0.86 to 2.15) | 0.189 | 149 | 27 | 0.89 (0.55 to 1.44) | 0.638 | 34 | 0.99 (0.64 to 1.52) | 0.95 | 41 | 1.01 (0.67 to 1.50) | 0.979 | 290 | 0.96 (0.86 to 1.08) | 0.507 | |
| HER2 overexpressed | 29 | 1.09 (0.65 to 1.83) | 0.753 | 102 | 21 | 0.88 (0.52 to 1.51) | 0.654 | 21 | 0.95 (0.57 to 1.59) | 0.846 | 20 | 0.71 (0.42 to 1.21) | 0.206 | 193 | 0.91 (0.80 to 1.04) | 0.176 | |
| Triple negative | 20 | 0.67 (0.38 to 1.18) | 0.162 | 134 | 14 | 0.50 (0.27 to 0.91) | 0.024 | 22 | 0.76 (0.46 to 1.25) | 0.285 | 35 | 0.95 (0.62 to 1.45) | 0.803 | 225 | 0.99 (0.88 to 1.11) | 0.849 | |
| Missing | 66 | 466 | 83 | 77 | 121 | 813 | |||||||||||
| (b) Post-menopausal breast cancer (n = 4017) | |||||||||||||||||
| Tumour behaviour | |||||||||||||||||
| Non-invasive | 31 | 358 | 1.00 (Reference) | 28 | 63 | 46 | 526 | 1.00 (Reference) | |||||||||
| Invasive | 261 | 1.38 (0.90 to 2.11) | 0.139 | 2351 | 184 | 1.07 (0.70 to 1.63) | 0.762 | 310 | 0.76 (0.56 to 1.02) | 0.068 | 208 | 0.71 (0.50 to 1.00) | 0.05 | 3314 | 0.87 (0.80 to 0.96) | 0.003 | |
| Missing | 7 | 133 | 5 | 15 | 17 | 177 | |||||||||||
| Other disease characteristics of patients with invasive cancer (n = 3314) | |||||||||||||||||
| Stage | |||||||||||||||||
| I | 86 | 770 | 1.00 (Reference) | 68 | 114 | 76 | 1114 | 1.00 (Reference) | |||||||||
| II | 119 | 1.05 (0.76 to 1.47) | 0.753 | 966 | 76 | 0.84 (0.59 to 1.20) | 0.331 | 121 | 0.96 (0.73 to 1.27) | 0.79 | 75 | 0.71 (0.50 to 1.00) | 0.048 | 1357 | 0.92 (0.85 to 1.00) | 0.06 | |
| III | 53 | 0.91 (0.61 to 1.38) | 0.662 | 484 | 35 | 0.76 (0.49 to 1.18) | 0.215 | 56 | 0.86 (0.61 to 1.21) | 0.387 | 46 | 0.85 (0.57 to 1.26) | 0.413 | 674 | 0.95 (0.86 to 1.05) | 0.286 | |
| IV | 3 | 0.24 (0.07 to 0.82) | 0.022 | 131 | 5 | 0.41 (0.16 to 1.07) | 0.069 | 19 | 1.04 (0.61 to 1.77) | 0.879 | 11 | 0.82 (0.42 to 1.60) | 0.555 | 169 | 1.02 (0.86 to 1.20) | 0.822 | |
| Grade | |||||||||||||||||
| Well differentiated | 32 | 318 | 1.00 (Reference) | 35 | 54 | 31 | 470 | 1.00 (Reference) | |||||||||
| Moderately differentiated | 109 | 1.03 (0.65 to 1.62) | 0.906 | 892 | 75 | 0.69 (0.45 to 1.07) | 0.094 | 113 | 0.73 (0.52 to 1.05) | 0.086 | 78 | 0.85 (0.55 to 1.32) | 0.475 | 1267 | 0.91 (0.81 to 1.01) | 0.069 | |
| Poorly differentiated | 108 | 0.88 (0.56 to 1.40) | 0.599 | 985 | 68 | 0.54 (0.35 to 0.85) | 0.007 | 123 | 0.70 (0.50 to 1.00) | 0.05 | 83 | 0.73 (0.47 to 1.13) | 0.156 | 1367 | 0.88 (0.79 to 0.98) | 0.018 | |
| Missing | 12 | 156 | 6 | 20 | 16 | 210 | |||||||||||
| Nodal status | |||||||||||||||||
| Negative | 144 | 1306 | 1.00 (Reference) | 113 | 181 | 119 | 1863 | 1.00 (Reference) | |||||||||
| Positive | 113 | 1.01 (0.75 to 1.36) | 0.938 | 993 | 70 | 0.75 (0.55 to 1.04) | 0.086 | 119 | 0.92 (0.72 to 1.18) | 0.508 | 87 | 0.88 (0.66 to 1.19) | 0.415 | 1382 | 0.95 (0.89 to 1.03) | 0.195 | |
| Missing | 4 | 52 | 1 | 10 | 2 | 69 | |||||||||||
| Tumour size (cm) | |||||||||||||||||
| ≤2 | 114 | 1031 | 1.00 (Reference) | 97 | 149 | 98 | 1489 | 1.00 (Reference) | |||||||||
| >2–5 | 115 | 1.05 (0.77 to 1.44) | 0.735 | 964 | 69 | 0.73 (0.53 to 1.02) | 0.069 | 125 | 0.99 (0.76 to 1.28) | 0.926 | 78 | 0.80 (0.58 to 1.10) | 0.165 | 1351 | 0.94 (0.87 to 1.02) | 0.124 | |
| >5 | 13 | 0.66 (0.34 to 1.31) | 0.238 | 142 | 10 | 0.62 (0.31 to 1.25) | 0.182 | 16 | 0.78 (0.45 to 1.36) | 0.384 | 18 | 1.17 (0.67 to 2.03) | 0.575 | 199 | 1.02 (0.88 to 1.18) | 0.794 | |
| Other/missing | 19 | 214 | 8 | 20 | 14 | 275 | |||||||||||
| Estrogen receptor status | |||||||||||||||||
| Positive | 182 | 1630 | 1.00 (Reference) | 115 | 230 | 150 | 2307 | 1.00 (Reference) | |||||||||
| Negative | 60 | 0.96 (0.68 to 1.36) | 0.805 | 540 | 51 | 1.23 (0.86 to 1.77) | 0.248 | 62 | 0.78 (0.58 to 1.05) | 0.103 | 39 | 0.76 (0.52 to 1.10) | 0.14 | 752 | 0.93 (0.85 to 1.01) | 0.099 | |
| Missing | 19 | 181 | 18 | 18 | 19 | 255 | |||||||||||
| Progesterone receptor status | |||||||||||||||||
| Positive | 143 | 1422 | 1.00 (Reference) | 92 | 198 | 121 | 1976 | 1.00 (Reference) | |||||||||
| Negative | 97 | 1.21 (0.88 to 1.64) | 0.239 | 737 | 74 | 1.34 (0.96 to 1.86) | 0.087 | 91 | 0.85 (0.65 to 1.11) | 0.23 | 67 | 1.00 (0.72 to 1.37) | 0.982 | 1066 | 0.97 (0.89 to 1.05) | 0.391 | |
| Missing | 21 | 192 | 18 | 21 | 20 | 272 | |||||||||||
| HER2 status | |||||||||||||||||
| Positive | 76 | 547 | 1.00 (Reference) | 36 | 79 | 43 | 781 | 1.00 (Reference) | |||||||||
| Negative | 145 | 0.84 (0.60 to 1.18) | 0.309 | 1392 | 115 | 1.42 (0.95 to 2.12) | 0.084 | 182 | 0.97 (0.73 to 1.29) | 0.825 | 127 | 1.26 (0.87 to 1.82) | 0.217 | 1961 | 1.07 (0.98 to 1.17) | 0.128 | |
| Missing | 40 | 412 | 33 | 49 | 38 | 572 | |||||||||||
| Subtype | |||||||||||||||||
| Luminal A | 96 | 833 | 1.00 (Reference) | 71 | 116 | 76 | 1192 | 1.00 (Reference) | |||||||||
| Luminal B | 39 | 0.73 (0.47 to 1.14) | 0.168 | 416 | 25 | 0.67 (0.41 to 1.09) | 0.109 | 56 | 0.95 (0.67 to 1.34) | 0.768 | 40 | 0.91 (0.61 to 1.38) | 0.67 | 576 | 0.99 (0.90 to 1.10) | 0.869 | |
| Luminal HER2-like | 27 | 0.77 (0.45 to 1.33) | 0.354 | 207 | 9 | 0.41 (0.20 to 0.86) | 0.018 | 37 | 1.13 (0.76 to 1.70) | 0.541 | 12 | 0.57 (0.30 to 1.09) | 0.088 | 292 | 0.94 (0.82 to 1.08) | 0.366 | |
| HER2 overexpressed | 34 | 1.16 (0.72 to 1.88) | 0.542 | 205 | 19 | 0.84 (0.49 to 1.46) | 0.54 | 22 | 0.73 (0.45 to 1.19) | 0.203 | 18 | 0.80 (0.46 to 1.39) | 0.434 | 298 | 0.89 (0.78 to 1.02) | 0.093 | |
| Triple negative | 19 | 0.64 (0.36 to 1.14) | 0.131 | 208 | 26 | 1.22 (0.74 to 2.00) | 0.442 | 23 | 0.77 (0.48 to 1.24) | 0.285 | 16 | 0.78 (0.44 to 1.37) | 0.383 | 292 | 0.97 (0.85 to 1.11) | 0.706 | |
| Missing | 46 | 482 | 34 | 56 | 46 | 664 | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, Z.L.; Lim, G.H.; Ho, P.J.; Khng, A.J.; Yeoh, Y.S.; Ong, A.T.W.; Tan, B.K.T.; Tan, E.Y.; Tan, S.-M.; Tan, V.K.-M.; et al. Associations between Pre-Diagnostic Physical Activity with Breast Cancer Characteristics and Survival. Cancers 2022, 14, 1756. https://doi.org/10.3390/cancers14071756
Lim ZL, Lim GH, Ho PJ, Khng AJ, Yeoh YS, Ong ATW, Tan BKT, Tan EY, Tan S-M, Tan VK-M, et al. Associations between Pre-Diagnostic Physical Activity with Breast Cancer Characteristics and Survival. Cancers. 2022; 14(7):1756. https://doi.org/10.3390/cancers14071756
Chicago/Turabian StyleLim, Zi Lin, Geok Hoon Lim, Peh Joo Ho, Alexis Jiaying Khng, Yen Shing Yeoh, Amanda Tse Woon Ong, Benita Kiat Tee Tan, Ern Yu Tan, Su-Ming Tan, Veronique Kiak-Mien Tan, and et al. 2022. "Associations between Pre-Diagnostic Physical Activity with Breast Cancer Characteristics and Survival" Cancers 14, no. 7: 1756. https://doi.org/10.3390/cancers14071756
APA StyleLim, Z. L., Lim, G. H., Ho, P. J., Khng, A. J., Yeoh, Y. S., Ong, A. T. W., Tan, B. K. T., Tan, E. Y., Tan, S.-M., Tan, V. K.-M., Li, J., & Hartman, M. (2022). Associations between Pre-Diagnostic Physical Activity with Breast Cancer Characteristics and Survival. Cancers, 14(7), 1756. https://doi.org/10.3390/cancers14071756