
Organ-Specific and Mixed Responses to Pembrolizumab in Patients with Unresectable or Metastatic Urothelial Carcinoma: A Multicenter Retrospective Study


 , , ,
on behalf of the Nara Urological Research and Treatment Group †add
Show full author list
, , ,
on behalf of the Nara Urological Research and Treatment Group †add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
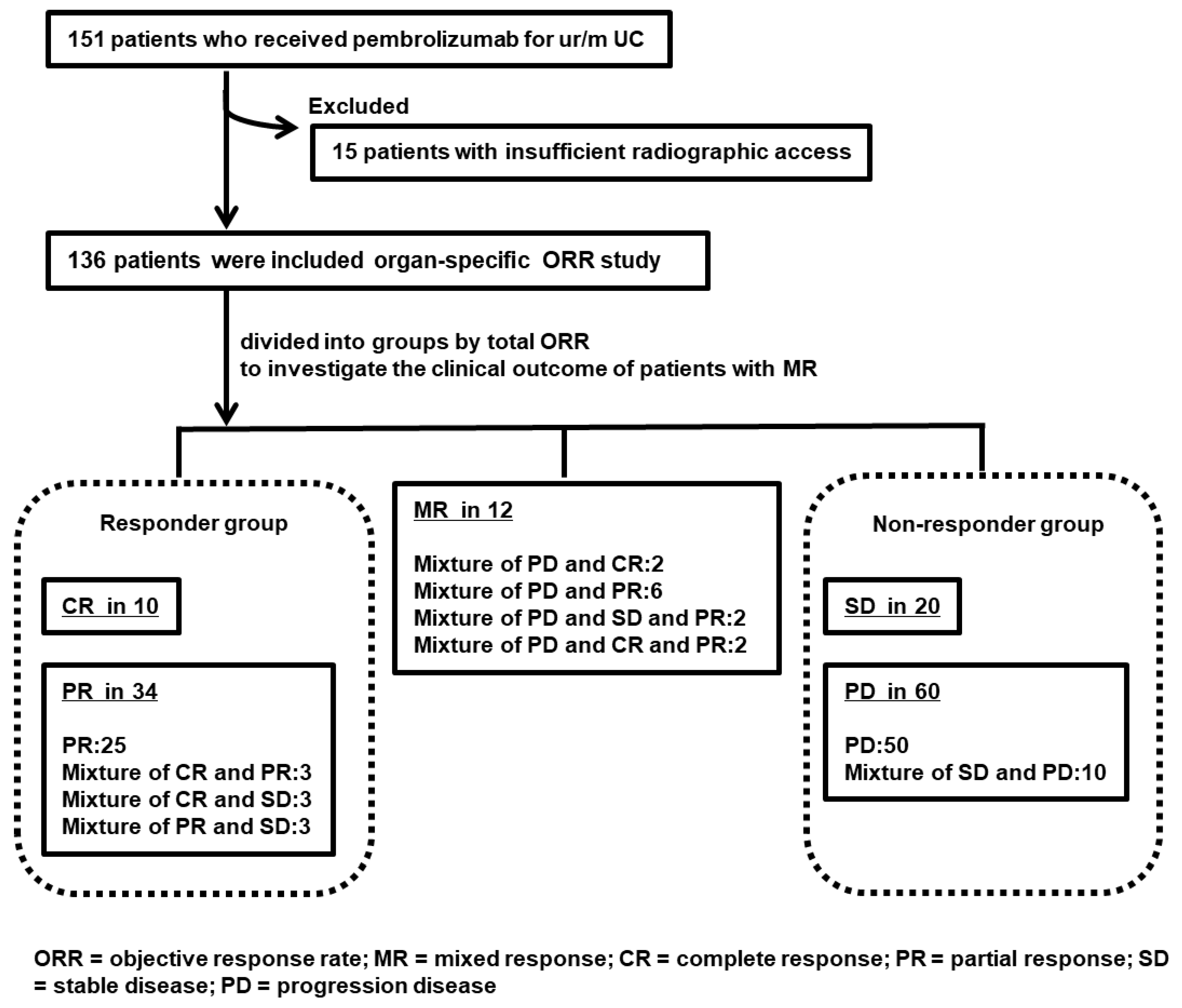
2.2. Patient Selection and Data Collection
2.3. Response Evaluation
2.4. Statistical Analysis
3. Results
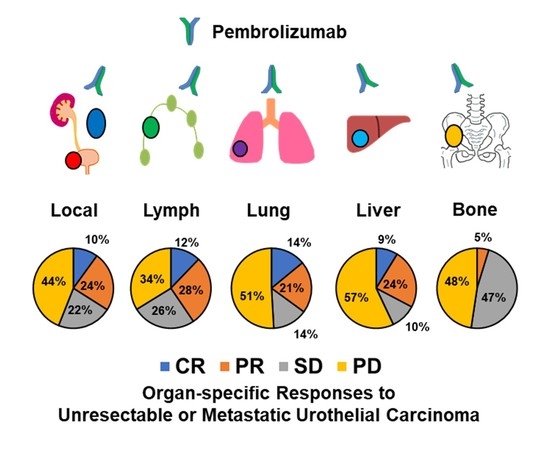
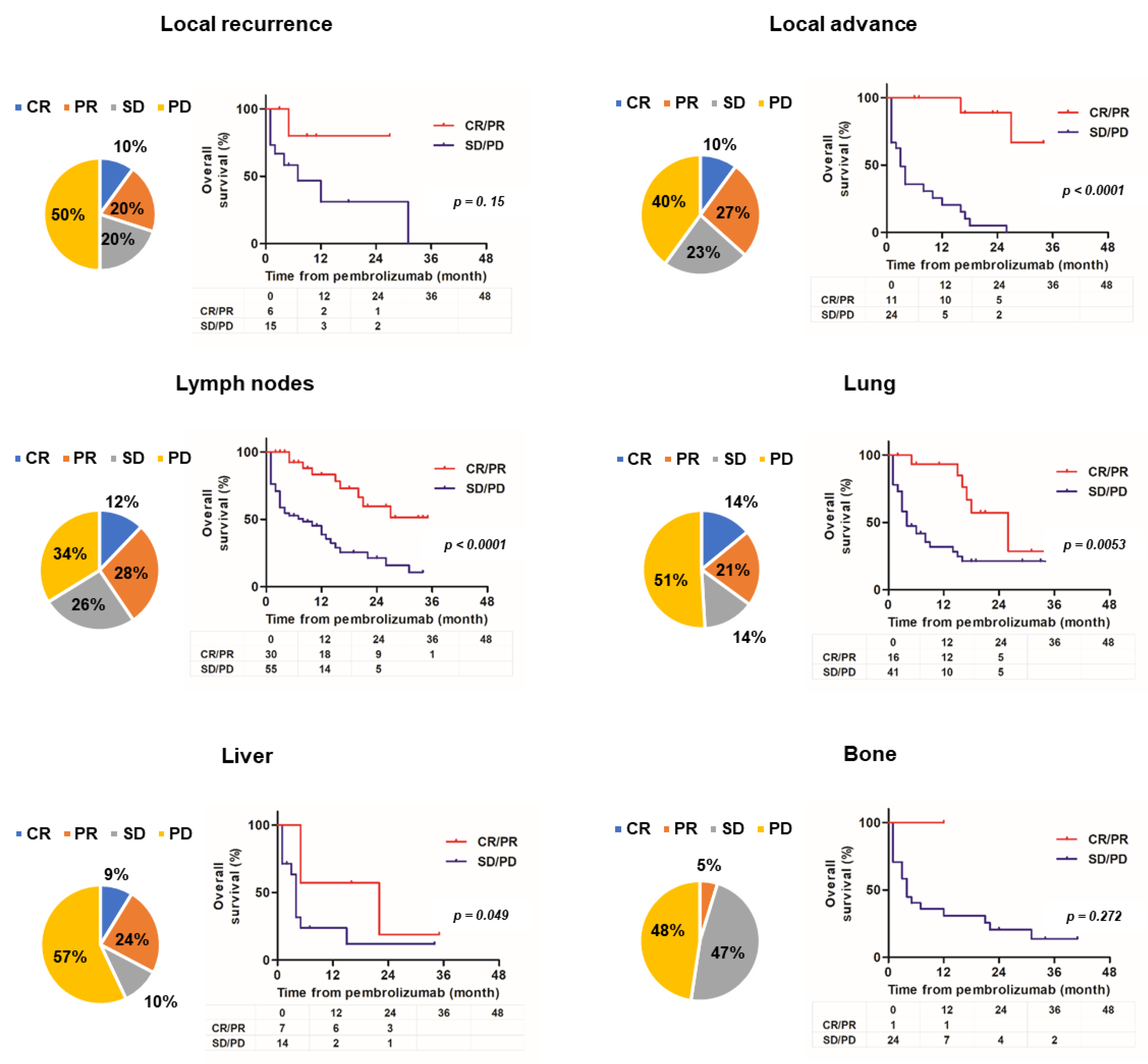
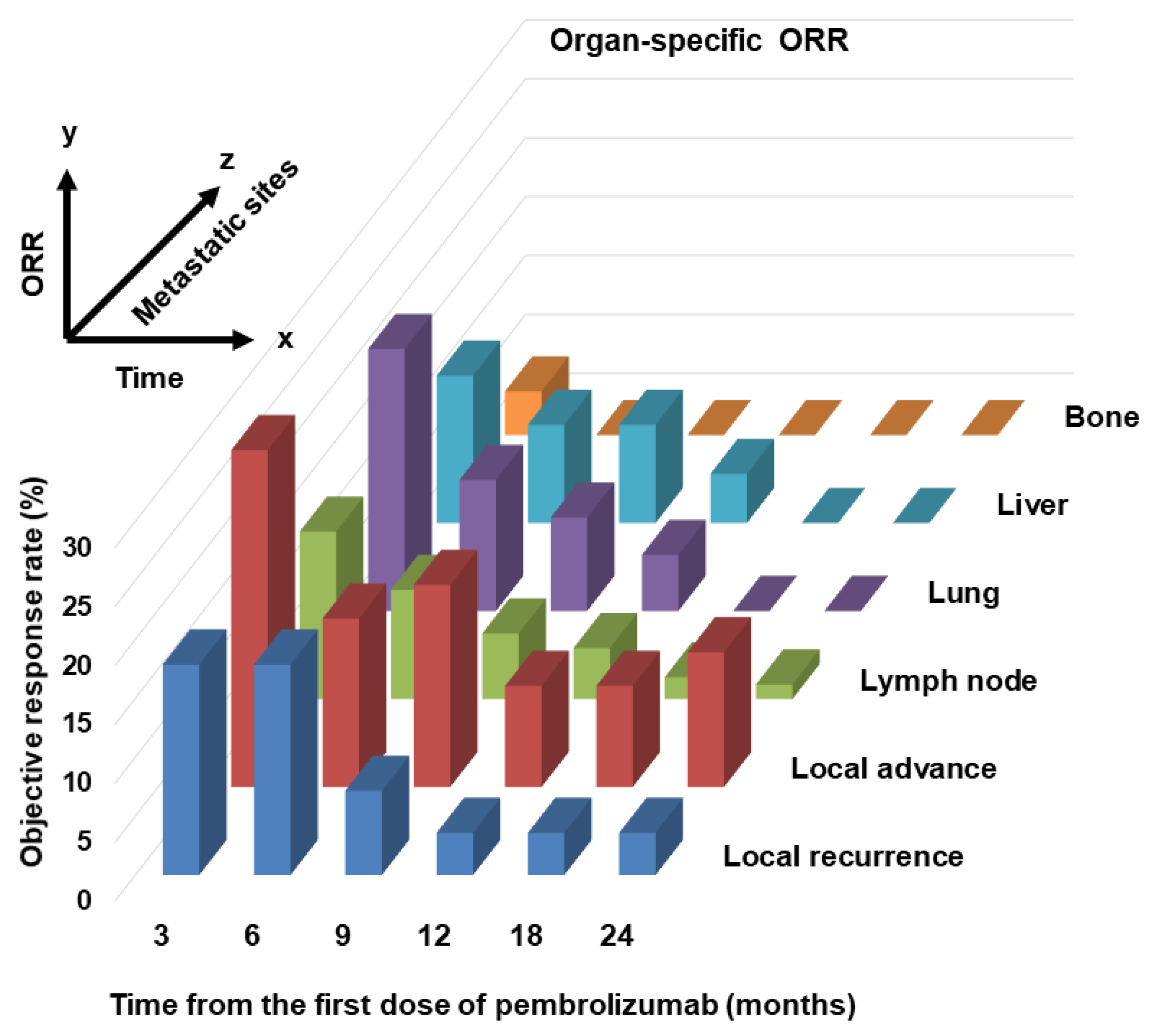
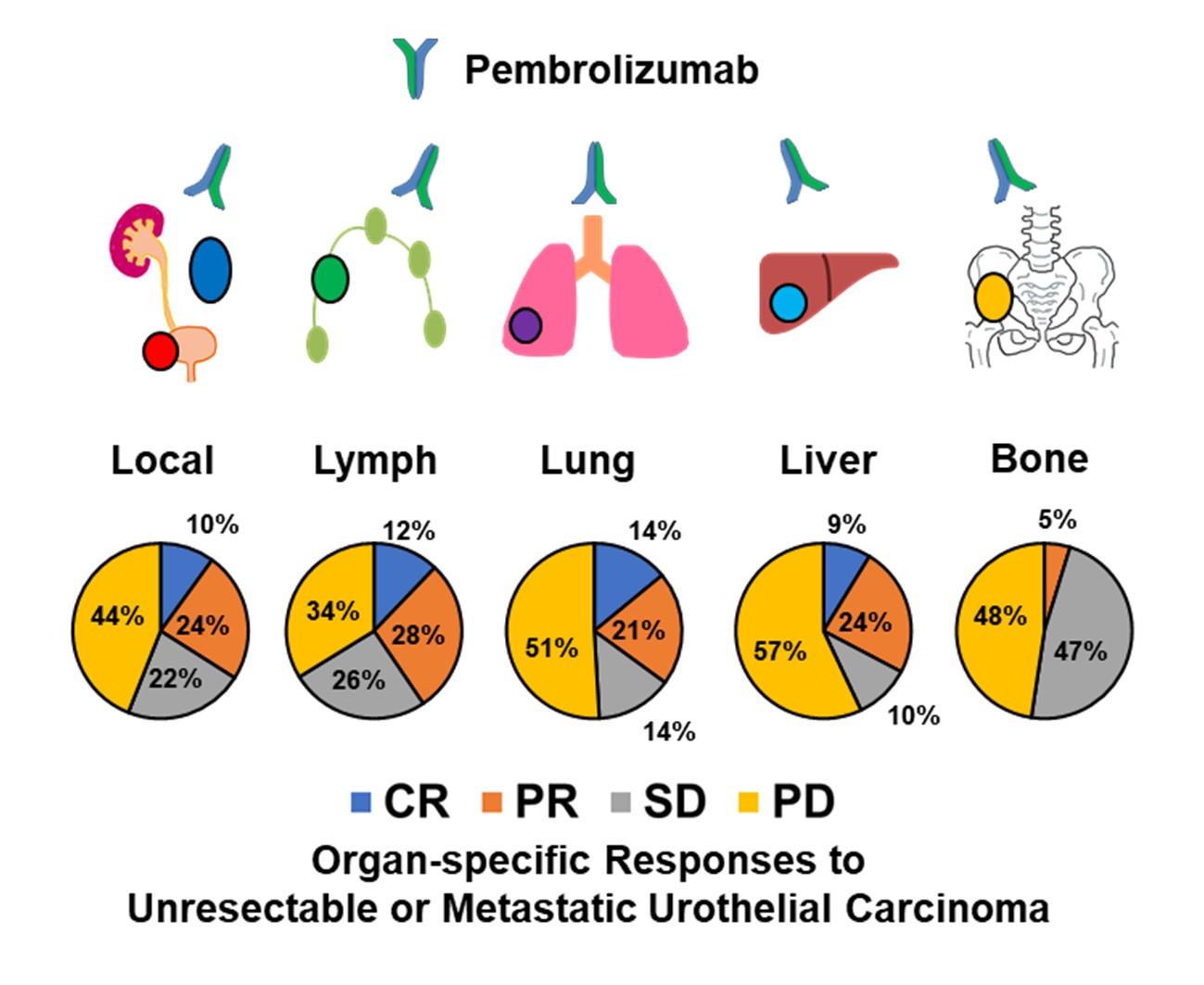
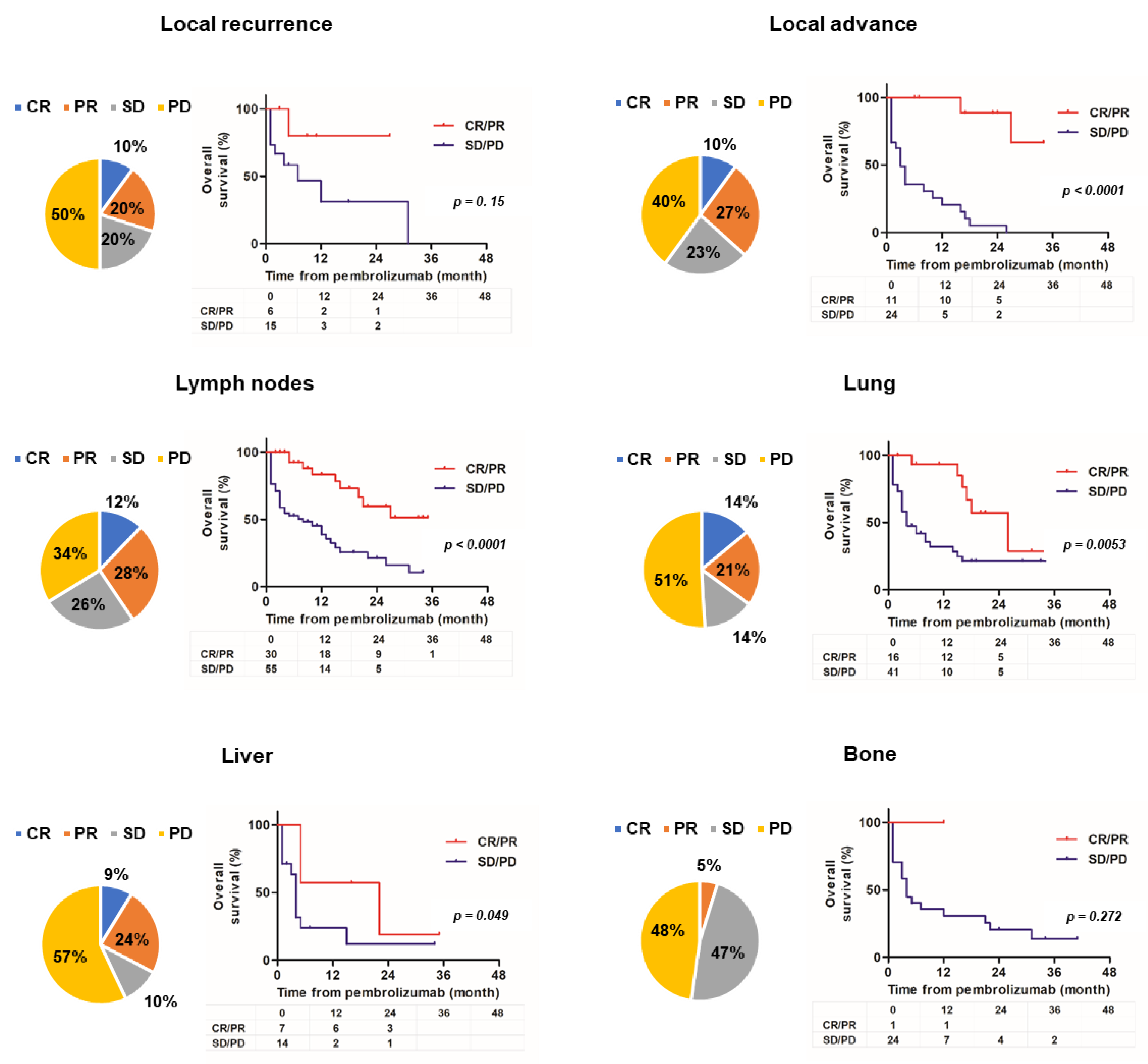
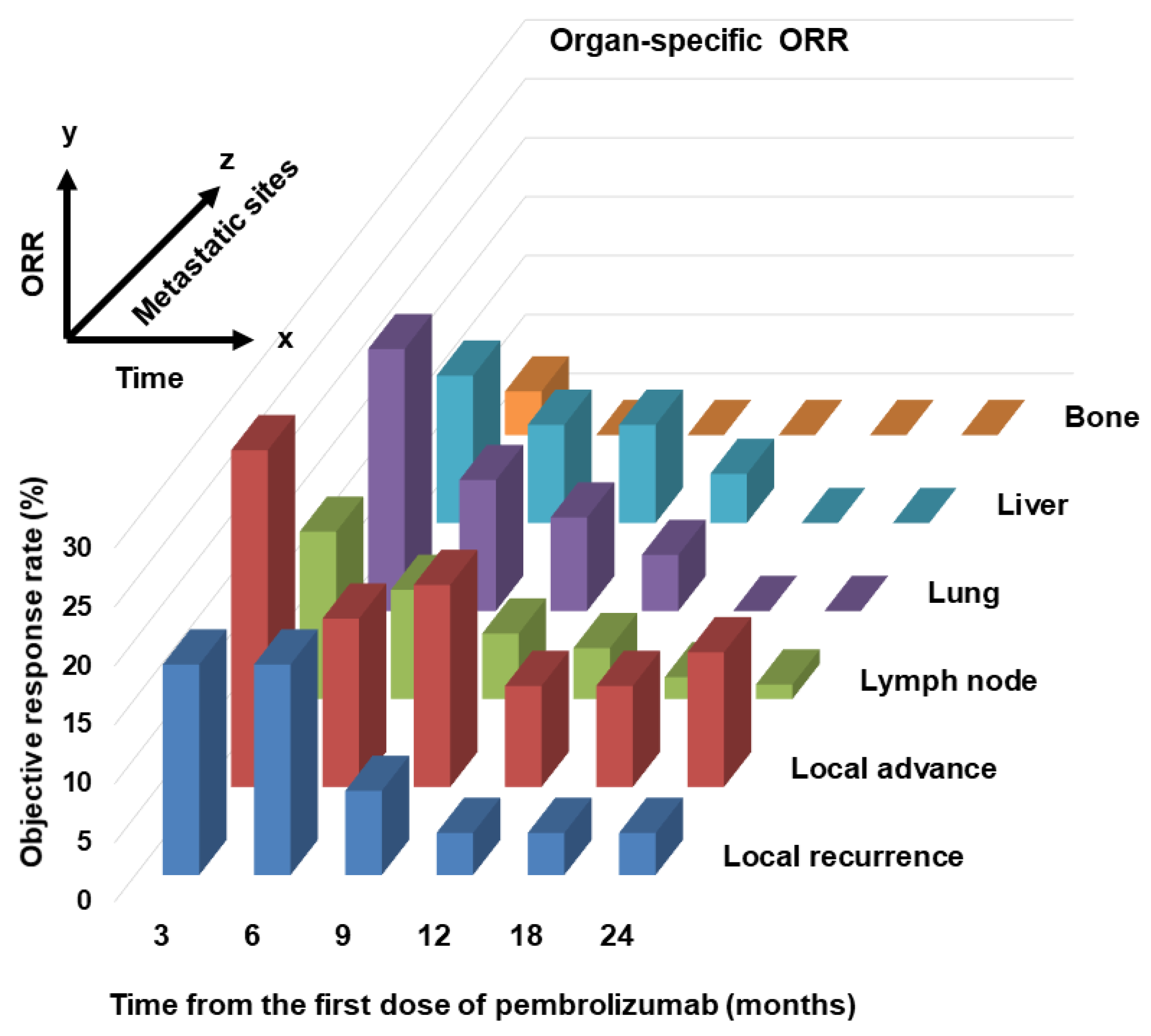
3.1. Organ-Specific ORR Results
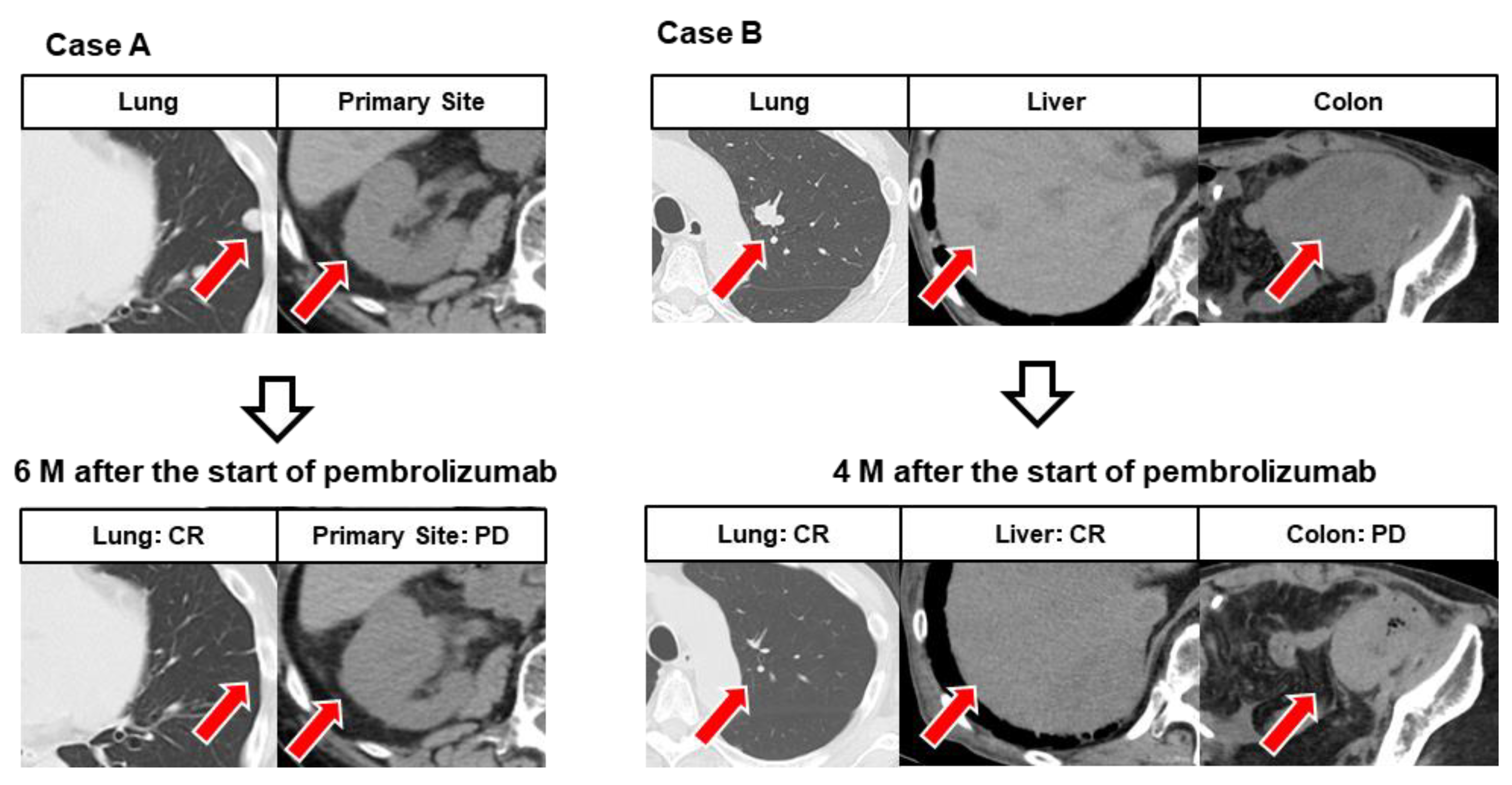
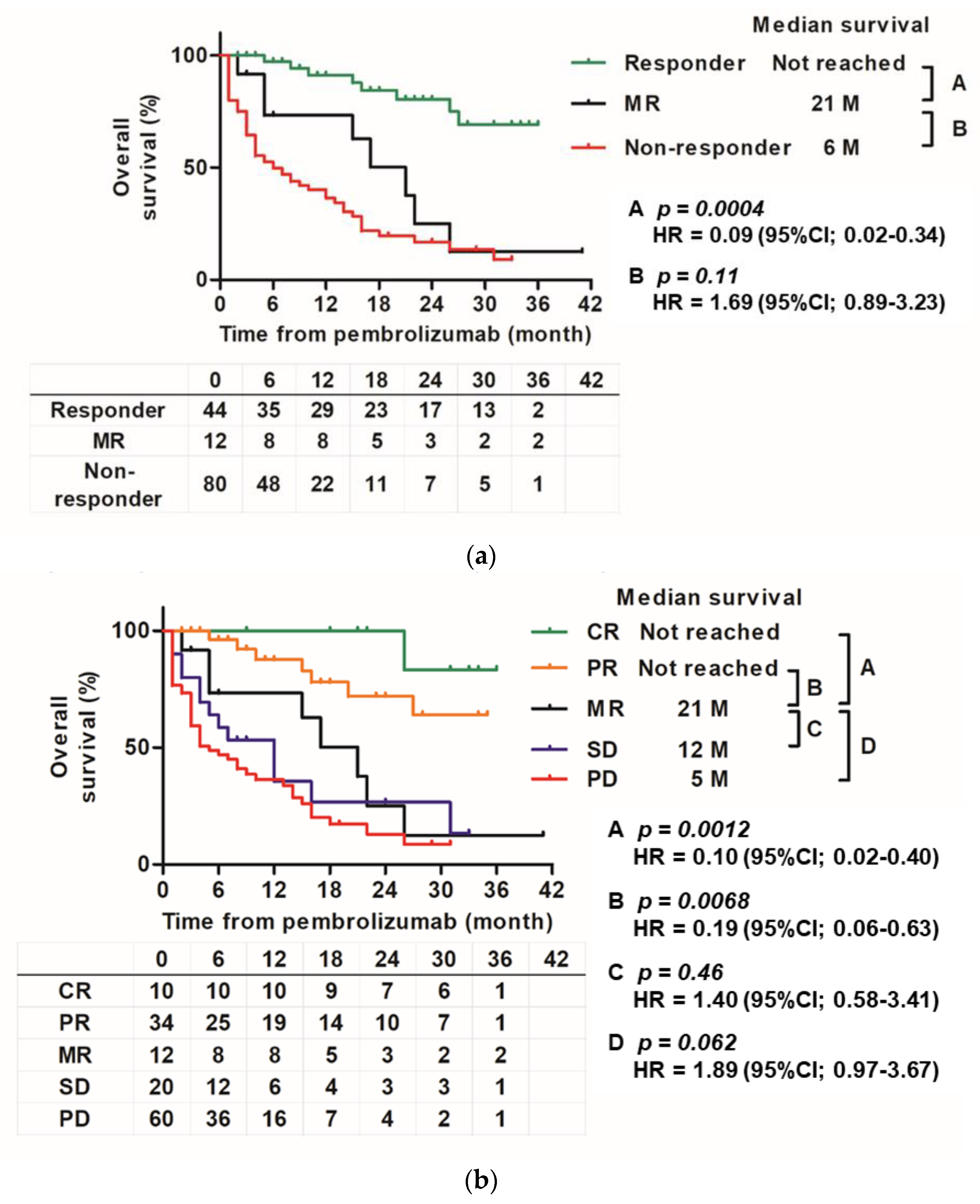
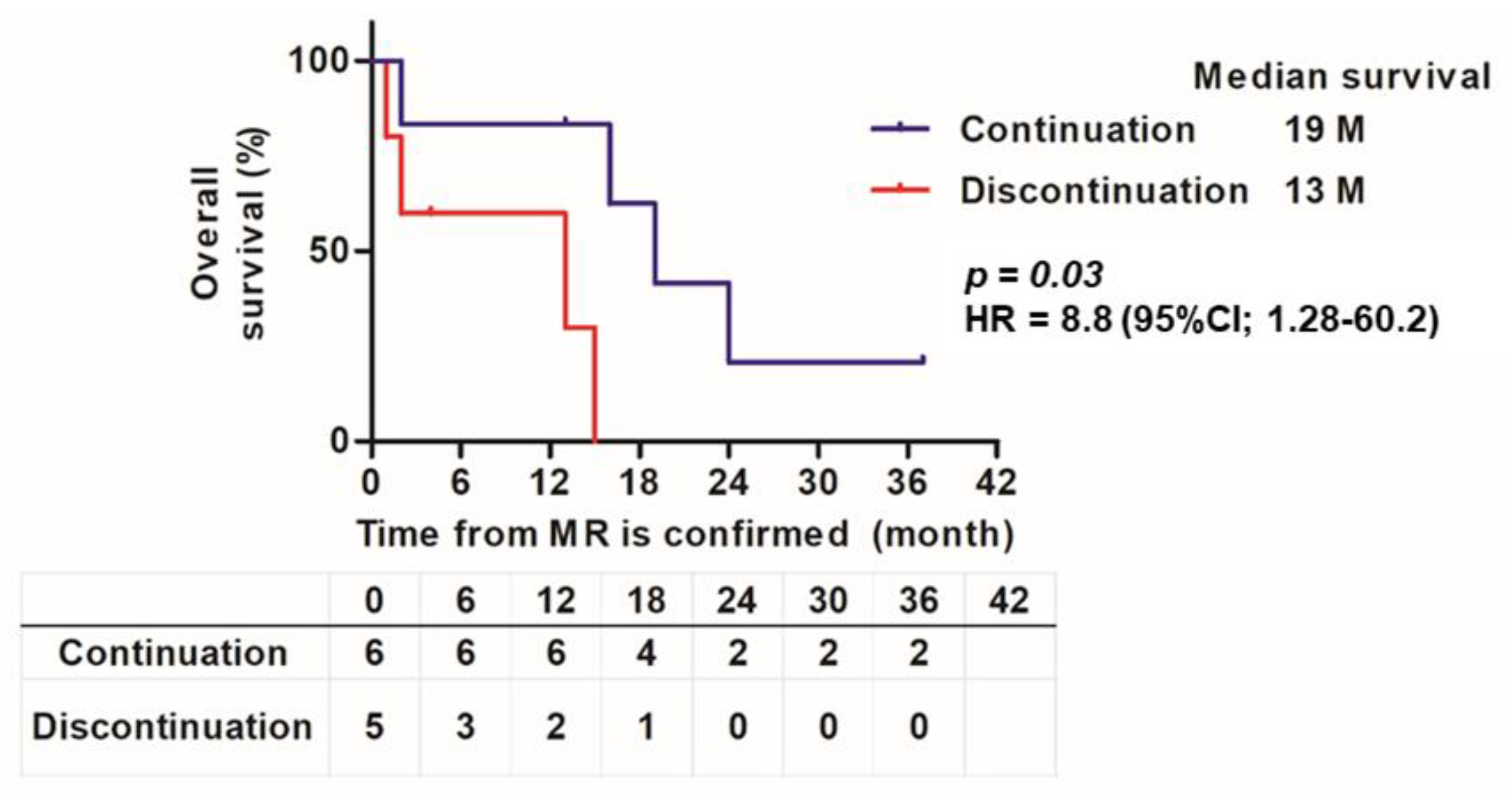
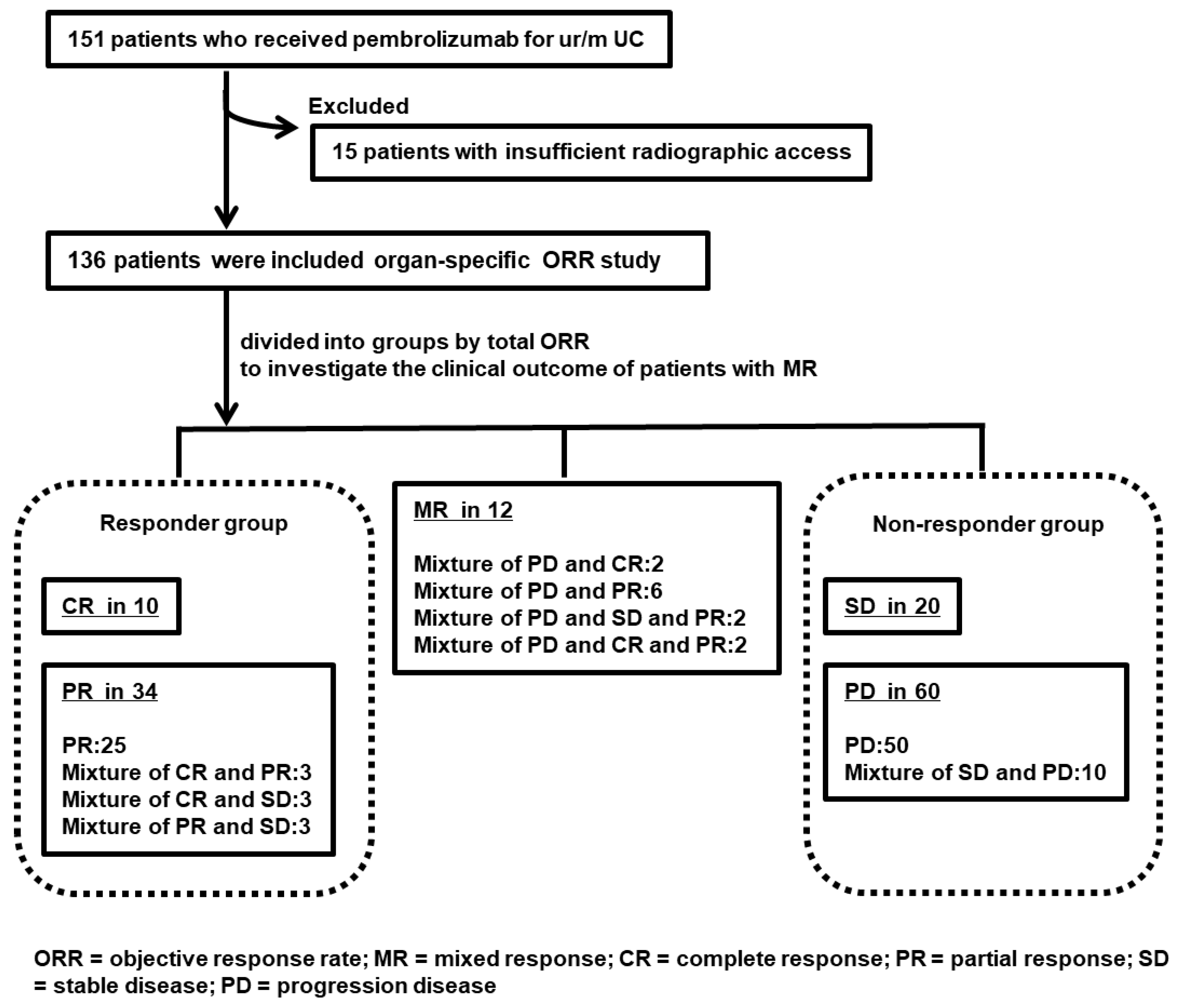
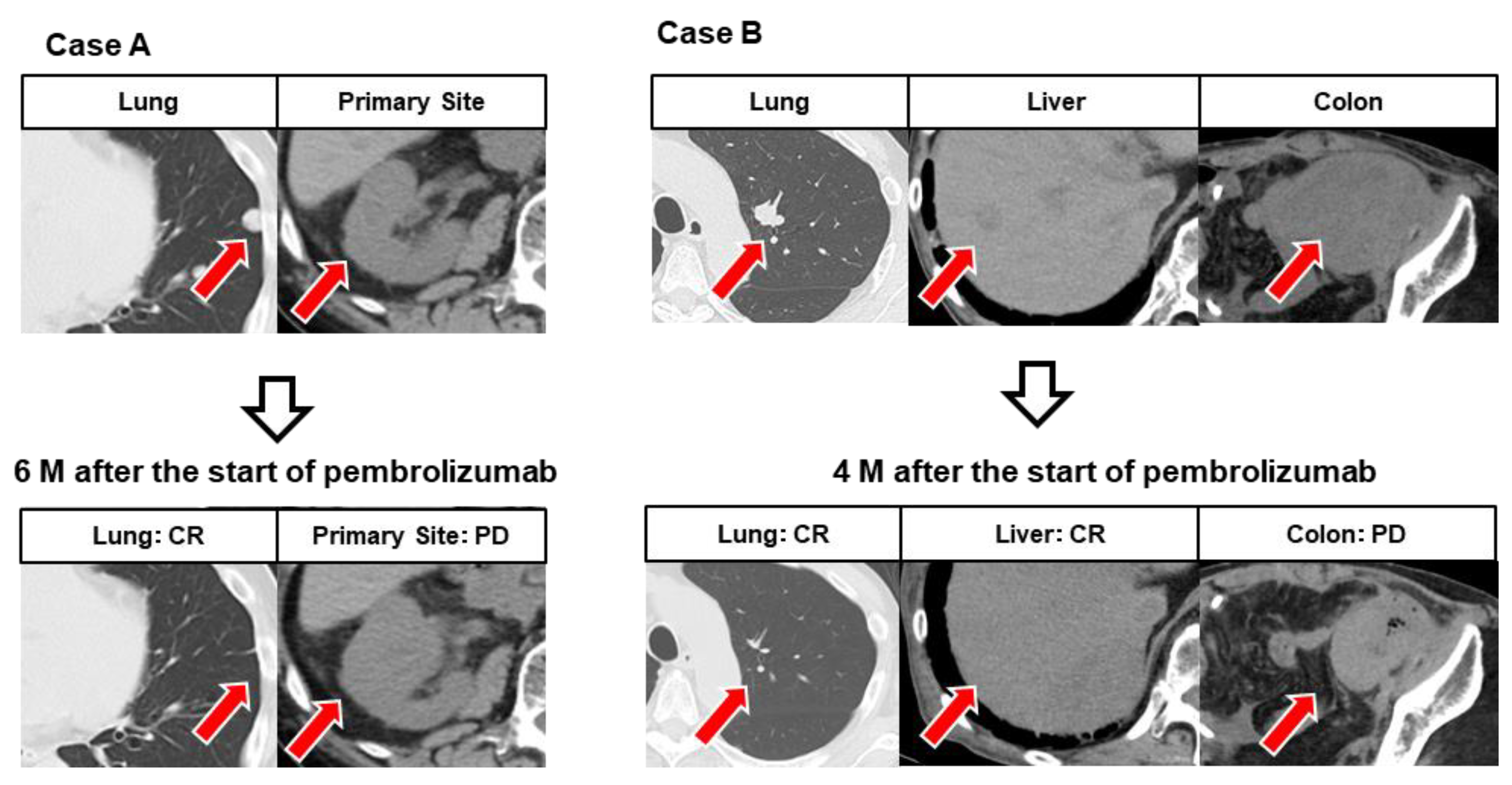
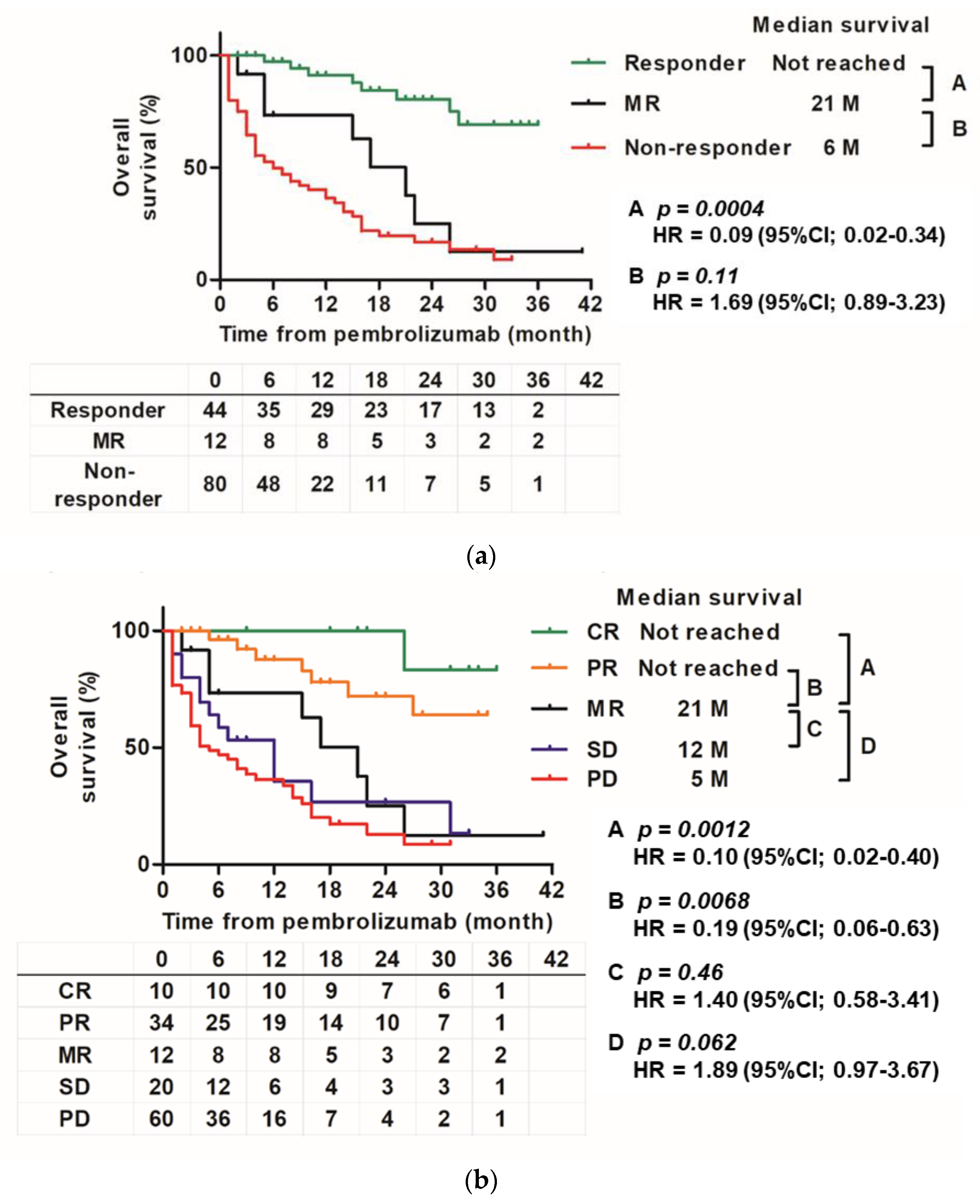
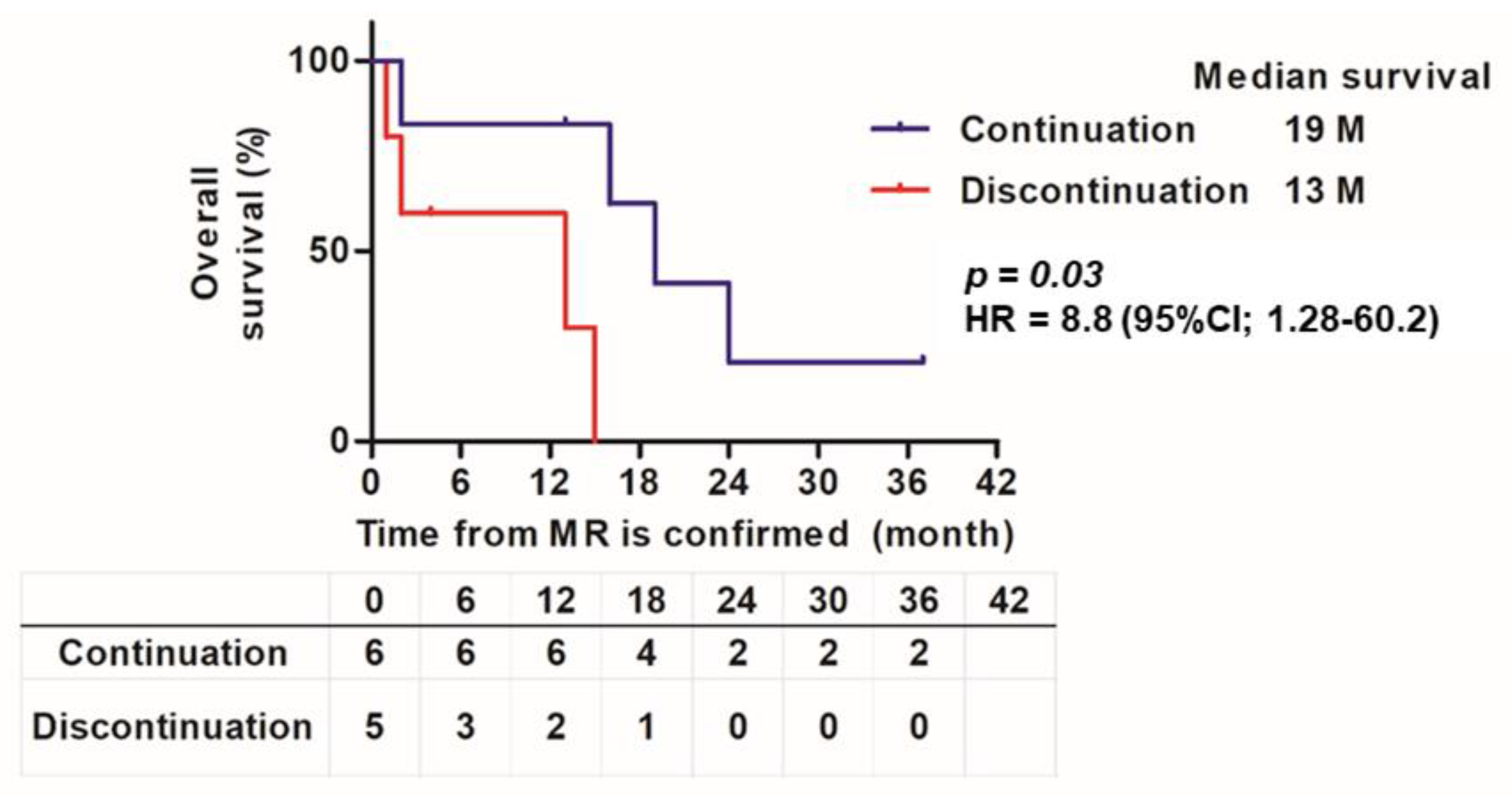
3.2. Results of Research on MR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bellmunt, J.; De Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Nishimura, N.; Shimizu, T.; Ohnishi, M.; Kuwada, M.; Itami, Y.; Inoue, T.; Ohnishi, K.; Matsumoto, Y.; Yoshida, T.; et al. Significant Improvement of Prognosis After the Advent of Immune Checkpoint Inhibitors in Patients with Advanced, Unresectable, or Metastatic Urothelial Carcinoma: A Propensity Score Matching and Inverse Probability of Treatment Weighting Analysis on Real-World Data. Cancer Manag. Res. 2022, 14, 623–635. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.M.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Tumeh, P.C.; Hellmann, M.D.; Hamid, O.; Tsai, K.K.; Loo, K.L.; Gubens, M.A.; Rosenblum, M.; Harview, C.L.; Taube, J.M.; Handley, N.; et al. Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC. Cancer Immunol. Res. 2017, 5, 417–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furubayashi, N.; Negishi, T.; Sakamoto, N.; Shimokawa, H.; Morokuma, F.; Song, Y.; Hori, Y.; Tomoda, T.; Tokuda, N.; Seki, N.; et al. Organ-Specific Tumor Response to Pembrolizumab in Advanced Urothelial Carcinoma After Platinum-Based Chemotherapy. OncoTargets Ther. 2021, 14, 1981–1988. [Google Scholar] [CrossRef]
- Schmid, S.; Diem, S.; Li, Q.; Krapf, M.; Flatz, L.; Leschka, S.; Desbiolles, L.; Klingbiel, D.; Jochum, W.; Früh, M. Organ-specific response to nivolumab in patients with non-small cell lung cancer (NSCLC). Cancer Immunol. Immunother. 2018, 67, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef] [Green Version]
- Furubayashi, N.; Negishi, T.; Sakamoto, N.; Tamura, S.; Morokuma, F.; Song, Y.; Hori, Y.; Tomoda, T.; Seki, N.; Kuroiwa, K.; et al. Clinical Outcomes of Mixed Response to Pembrolizumab in Advanced Urothelial Carcinoma After Platinum-based Chemotherapy. Vivo 2021, 35, 2869–2874. [Google Scholar] [CrossRef] [PubMed]
- Rauwerdink, D.J.W.; Molina, G.; Ms, D.T.F.; Sharova, T.; Van Der Hage, J.; Cohen, S.; Boland, G.M. Mixed Response to Immunotherapy in Patients with Metastatic Melanoma. Ann. Surg. Oncol. 2020, 27, 3488–3497. [Google Scholar] [CrossRef] [PubMed]
- Owari, T.; Miyake, M.; Nakai, Y.; Tanaka, N.; Itami, Y.; Hirao, S.; Momose, H.; Nakagawa, Y.; Iida, K.; Maesaka, F.; et al. External validation of a genitourinary cancer-specific prognostic scoring system to predict survival for patients with bone metastasis (modified B-FOM scoring model): Comparison with other scoring models in terms of accuracy. J. Bone Oncol. 2020, 26, 100344. [Google Scholar] [CrossRef] [PubMed]
- Stellato, M.; Santini, D.; Cursano, M.C.; Foderaro, S.; Tonini, G.; Procopio, G. Bone metastases from urothelial carcinoma. The dark side of the moon. J. Bone Oncol. 2021, 31, 100405. [Google Scholar] [CrossRef] [PubMed]
- Owari, T.; Miyake, M.; Nakai, Y.; Hori, S.; Tomizawa, M.; Ichikawa, K.; Shimizu, T.; Iida, K.; Samma, S.; Iemura, Y.; et al. Clinical benefit of early treatment with bone-modifying agents for preventing skeletal-related events in patients with genitourinary cancer with bone metastasis: A multi-institutional retrospective study. Int. J. Urol. 2019, 26, 630–637. [Google Scholar] [CrossRef]
- Uchimoto, T.; Komura, K.; Fukuokaya, W.; Kimura, T.; Takahashi, K.; Yano, Y.; Nishimura, K.; Nakamori, K.; Fujiwara, Y.; Matsunaga, T.; et al. Risk Classification for Overall Survival by the Neutrophil–Lymphocyte Ratio and the Number of Metastatic Sites in Patients Treated with Pembrolizumab—A Multicenter Collaborative Study in Japan. Cancers 2021, 13, 3554. [Google Scholar] [CrossRef]
- Kobayashi, T.; Ito, K.; Kojima, T.; Kato, M.; Kanda, S.; Hatakeyama, S.; Matsui, Y.; Matsushita, Y.; Naito, S.; Shiga, M.; et al. Risk stratification for the prognosis of patients with chemoresistant urothelial cancer treated with pembrolizumab. Cancer Sci. 2020, 112, 760–773. [Google Scholar] [CrossRef]
- Diem, S.; Ali, O.H.; Ackermann, C.J.; Bomze, D.; Koelzer, V.H.; Jochum, W.; Speiser, D.E.; Mertz, K.D.; Flatz, L. Tumor infiltrating lymphocytes in lymph node metastases of stage III melanoma correspond to response and survival in nine patients treated with ipilimumab at the time of stage IV disease. Cancer Immunol. Immunother. 2017, 67, 39–45. [Google Scholar] [CrossRef]
- Chan, T.; Wiltrout, R.H.; Weiss, J.M. Immunotherapeutic modulation of the suppressive liver and tumor microenvironments. Int. Immunopharmacol. 2011, 11, 879–889. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Tian, Z. The liver works as a school to educate regulatory immune cells. Cell. Mol. Immunol. 2013, 10, 292–302. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Allison, J.P. The future of immune checkpoint therapy. Science 2015, 348, 56–61. [Google Scholar] [CrossRef]
- Galon, J.; Bruni, D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat. Rev. Drug Discov. 2019, 18, 197–218. [Google Scholar] [CrossRef] [PubMed]
- Sakatani, T.; Kita, Y.; Fujimoto, M.; Sano, T.; Hamada, A.; Nakamura, K.; Takada, H.; Goto, T.; Sawada, A.; Akamatsu, S.; et al. IFN-Gamma Expression in the Tumor Microenvironment and CD8-Positive Tumor-Infiltrating Lymphocytes as Prognostic Markers in Urothelial Cancer Patients Receiving Pembrolizumab. Cancers 2022, 14, 263. [Google Scholar] [CrossRef]
- Aksoylar, H.-I.; Boussiotis, V.A. PD-1+ Treg cells: A foe in cancer immunotherapy? Nat. Immunol. 2020, 21, 1311–1312. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Togashi, Y.; Kamada, T.; Sugiyama, E.; Nishinakamura, H.; Takeuchi, Y.; Vitaly, K.; Itahashi, K.; Maeda, Y.; Matsui, S.; et al. The PD-1 expression balance between effector and regulatory T cells predicts the clinical efficacy of PD-1 blockade therapies. Nat. Immunol. 2020, 21, 1346–1358. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Kinn, J.; Zirakzadeh, A.A.; Sherif, A.; Norstedt, G.; Wikström, A.-C.; Winqvist, O. The effects of chemotherapeutic drugs on human monocyte-derived dendritic cell differentiation and antigen presentation. Clin. Exp. Immunol. 2012, 172, 490–499. [Google Scholar] [CrossRef]
- Krantz, D.; Hartana, C.A.; Winerdal, M.E.; Johansson, M.; Alamdari, F.; Jakubczyk, T.; Huge, Y.; Aljabery, F.; Palmqvist, K.; Zirakzadeh, A.A.; et al. Neoadjuvant Chemotherapy Reinforces Antitumour T cell Response in Urothelial Urinary Bladder Cancer. Eur. Urol. 2018, 74, 688–692. [Google Scholar] [CrossRef] [Green Version]
- Fournel, L.; Wu, Z.; Stadler, N.; Damotte, D.; Lococo, F.; Boulle, G.; Ségal-Bendirdjian, E.; Bobbio, A.; Icard, P.; Trédaniel, J.; et al. Cisplatin increases PD-L1 expression and optimizes immune check-point blockade in non-small cell lung cancer. Cancer Lett. 2019, 464, 5–14. [Google Scholar] [CrossRef]
- Miyake, M.; Shimizu, T.; Nishimura, N.; Kiba, K.; Maesaka, F.; Oda, Y.; Tachibana, A.; Tomizawa, M.; Ohmori, C.; Matsumura, Y.; et al. Response to Pembrolizumab After Dose-Reduced Cisplatin Plus Gemcitabine Chemotherapy Is Inferior to That After Carboplatin Plus Gemcitabine Chemotherapy in Cisplatin-Unfit Patients With Advanced Urothelial Carcinoma. Clin. Genitourin. Cancer, 2021; in press. [Google Scholar] [CrossRef]
- Powles, T.; Rosenberg, J.E.; Sonpavde, G.P.; Loriot, Y.; Durán, I.; Lee, J.-L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Wu, C.; et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 1125–1135. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbé, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Response to Pembrolizumab | p Value | |||
|---|---|---|---|---|---|---|
| Responder Group CR/PR | MR | Non-Responder Group SD/PD | ||||
| Total | 136 (100%) | 44 (32%) | 12 (9%) | 80 (59%) | ||
| Age | Median, (range) | 73 (49–87) | 74 (54–85) | 68 (52–82) | 72 (49–87) | 0.09 |
| Sex | Male | 100 (74%) | 31 (70%) | 9 (75%) | 60 (75%) | 0.16 |
| ECOG–PS | 0–1 2≤ | 118 (867%) 18 (13%) | 42 (95%) 2 (5%) | 10 (83%) 2 (17%) | 66 (83%) 14 (17%) | 0.32 |
| Hemoglobin | ≥10 g/dL <10 g/dL | 91 (67%) 42 (31%) | 28 (64%) 16 (36%) | 7 (58%) 5 (42%) | 58 (73%) 22 (27%) | 0.15 |
| eGFR (mL/min/1.73 m2) | ≥45 <45 | 73 (54%) 58 (43%) | 24 (55%) 20 (45%) | 7 (58%) 5 (42%) | 46 (58%) 34 (42%) | 0.10 |
| Primary site | BC UTUC | 71 (52%) 65 (48%) | 18 (41%) 26 (59%) | 8 (67%) 4 (33%) | 45 (56%) 35 (44%) | 0.10 |
| Variant histology | n (%) | 13 (10%) | 4 (9%) | 0 (0%) | 9 (11%) | 0.56 |
| Number of prior chemotherapies | 1 2≤ | 113 (83%) 23 (17%) | 34 (77%) 10 (23%) | 8 (67%) 4 (33%) | 71 (89%) 9 (11%) | 0.18 |
| Interval since last chemotherapy | <3 months ≥3 months | 85 (63%) 51 (37%) | 23 (52%) 21 (48%) | 8 (67%) 4 (33%) | 55 (69%) 25 (31%) | 0.10 |
| Evaluable lesion | ||||||
| Local recurrence | n (%) | 24 (18%) | 8 (18%) | 3 (25%) | 15 (19%) | 0.28 |
| Local advance | n (%) | 35 (26%) | 12 (27%) | 1 (8%) | 20 (25%) | 0.16 |
| Lymph nodes | n (%) | 85 (63%) | 32 (73%) | 8 (67%) | 46 (58%) | 0.10 |
| Lung | n (%) | 57 (42%) | 13 (30%) | 9 (75%) | 37 (46%) | 0.17 |
| Liver | n (%) | 22 (16%) | 5 (11%) | 3 (25%) | 14 (18%) | 0.28 |
| Bone | n (%) | 25 (18%) | 3 (7%) | 3 (25%) | 18 (23%) | 0.32 |
| Brain | n (%) | 2 (2%) | 0 (0%) | 2 (17%) | 0 (0%) | 0.98 |
| Pleura | n (%) | 5 (4%) | 2 (5%) | 2 (17%) | 2 (3%) | 0.85 |
| Peritoneal | n (%) | 11 (8%) | 1 (2%) | 2 (17%) | 9 (11%) | 0.65 |
| Others | n (%) | 12 (9%) | 2 (5%) | 3 (25%) | 7 (9%) | 0.65 |
| Follow-Up (month) | Median, (range) | 8 (1–41) | 18 (2–36) | 15 (2–41) | 5 (1–33) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, T.; Miyake, M.; Nishimura, N.; Inoue, K.; Fujii, K.; Iemura, Y.; Ichikawa, K.; Omori, C.; Tomizawa, M.; Maesaka, F.; et al. Organ-Specific and Mixed Responses to Pembrolizumab in Patients with Unresectable or Metastatic Urothelial Carcinoma: A Multicenter Retrospective Study. Cancers 2022, 14, 1735. https://doi.org/10.3390/cancers14071735
Shimizu T, Miyake M, Nishimura N, Inoue K, Fujii K, Iemura Y, Ichikawa K, Omori C, Tomizawa M, Maesaka F, et al. Organ-Specific and Mixed Responses to Pembrolizumab in Patients with Unresectable or Metastatic Urothelial Carcinoma: A Multicenter Retrospective Study. Cancers. 2022; 14(7):1735. https://doi.org/10.3390/cancers14071735
Chicago/Turabian StyleShimizu, Takuto, Makito Miyake, Nobutaka Nishimura, Kuniaki Inoue, Koyo Fujii, Yusuke Iemura, Kazuki Ichikawa, Chihiro Omori, Mitsuru Tomizawa, Fumisato Maesaka, and et al. 2022. "Organ-Specific and Mixed Responses to Pembrolizumab in Patients with Unresectable or Metastatic Urothelial Carcinoma: A Multicenter Retrospective Study" Cancers 14, no. 7: 1735. https://doi.org/10.3390/cancers14071735
APA StyleShimizu, T., Miyake, M., Nishimura, N., Inoue, K., Fujii, K., Iemura, Y., Ichikawa, K., Omori, C., Tomizawa, M., Maesaka, F., Oda, Y., Miyamoto, T., Sakamoto, K., Kiba, K., Tanaka, M., Oyama, N., Okajima, E., Fujimoto, K., Hori, S., ... Fujimoto, K., on behalf of the Nara Urological Research and Treatment Group †. (2022). Organ-Specific and Mixed Responses to Pembrolizumab in Patients with Unresectable or Metastatic Urothelial Carcinoma: A Multicenter Retrospective Study. Cancers, 14(7), 1735. https://doi.org/10.3390/cancers14071735