
Tumor-Infiltrating Lymphocytes in Head and Neck Cancer: Ready for Prime Time?

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Accumulated Evidence on TILs as a Prognosticator: Where Are We Currently?
3. Clinical Scenarios of TILs in HNSCC
3.1. TILs as Indicator for Selection of HNSCC Patients for Immunotherapeutic Approaches
3.2. The Role of TILs in the Elucidation of De-Escalation Therapies in HNSCC
4. Automated Analysis of TILs
5. Morphological Pitfalls in the Assessment of TILs in HNSCC
- (1).
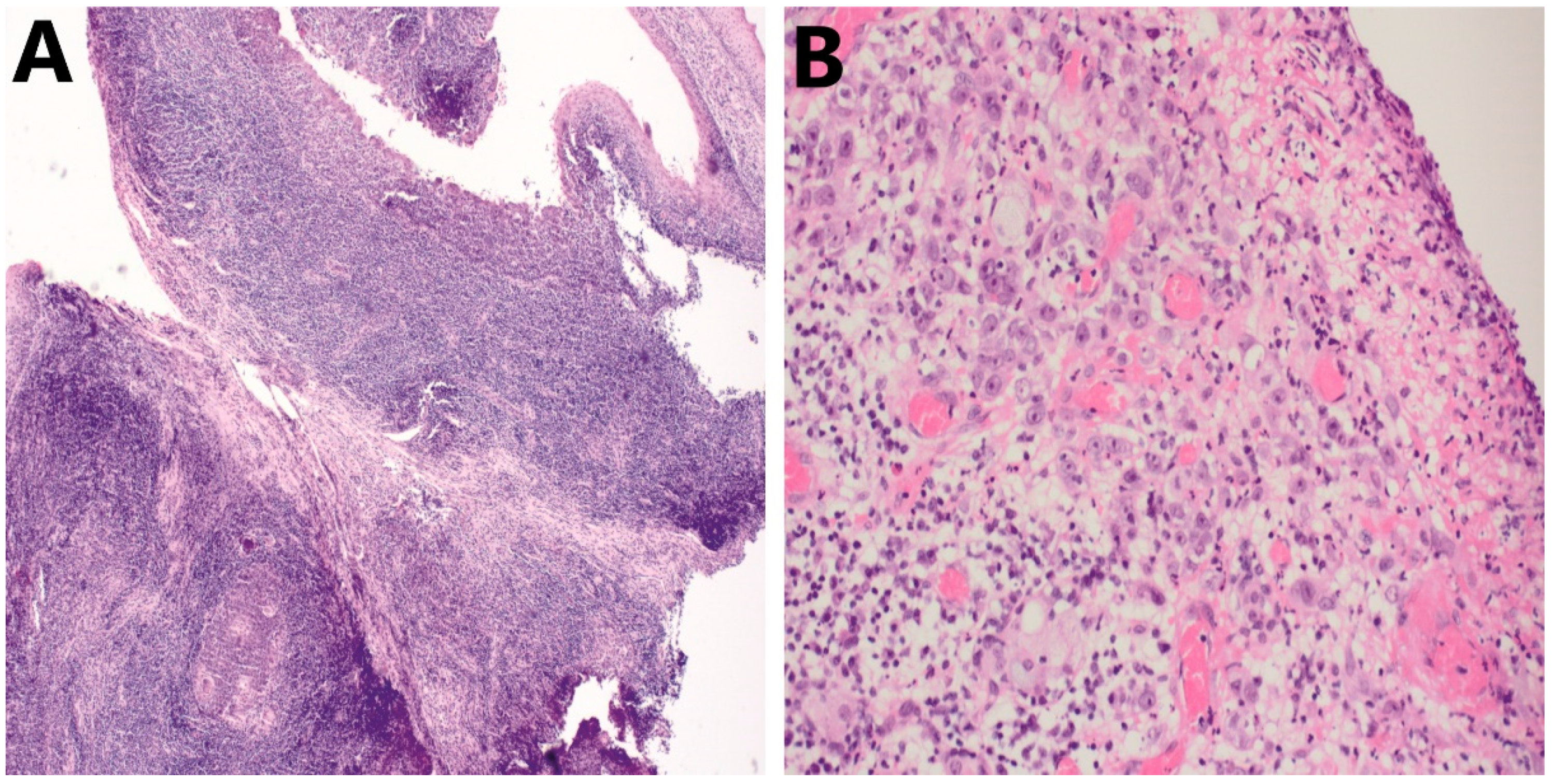
- Differentiating TILs from a pre-existing immune infiltrate and other immune cells. First, this can be attributed due to the presence of pre-existing lymphoid tissue (Figure 3A), not only in the oropharyngeal/tonsillar region but in all (sub)sites of the head and neck region. Therefore, distinguishing tumor-attracted from pre-existing mononuclear cells may be challenging. Second, regions with ulcerations (Figure 3B) or erosions are seeded with infiltrating immune cells that are predominantly polymorphonuclear cells, which can also hamper the correct assessment of TILs in the TME. Evidently, these should be excluded from evaluation.
- (2).
- Inadequate tumor material for evaluation. In HNSCC, available tissue specimens typically comprise diagnostic biopsies. However, these are often characterized by insufficient amounts of stroma, disabling the correct quantification of stromal lymphocytes in this compartment. Ideally, whole-tumor resected specimens are the ‘golden standard’ to perform quantification of TILs but are mostly unavailable for patients diagnosed with recurrent and unresectable or metastasized HNSCC. In addition, long time intervals may exist between the initial biopsy or resection and the decision to commence palliative treatment. The temporal variance that has occurred in the TME will ultimately have an effect on the use of TILs as a predictive biomarker in this setting.
6. Why Is the Assessment of TILs Not Yet Used in the Daily Practice of HNSCC Pathology Reporting?
7. Future Considerations for the Inclusion of TILs in Daily Clinico-Pathological Practice
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thompson-Harvey, A.; Yetukuri, M.; Hansen, A.R.; Simpson, M.C.; Adjei Boakye, E.; Varvares, M.A.; Osazuwa-Peters, N. Rising incidence of late-stage head and neck cancer in the United States. Cancer 2020, 126, 1090–1101. [Google Scholar] [CrossRef] [PubMed]
- Meccariello, G.; Maniaci, A.; Bianchi, G.; Cammaroto, G.; Iannella, G.; Catalano, A.; Sgarzani, R.; De Vito, A.; Capaccio, P.; Pelucchi, S.; et al. Neck dissection and trans oral robotic surgery for oropharyngeal squamous cell carcinoma. Auris Nasus Larynx 2022, 49, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Pisani, P.; Airoldi, M.; Allais, A.; Aluffi Valletti, P.; Battista, M.; Benazzo, M.; Briatore, R.; Cacciola, S.; Cocuzza, S.; Colombo, A.; et al. Metastatic disease in head & neck oncology. Acta Otorhinolaryngol Ital. 2020, 40, S1–S86. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and Neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef]
- Gavrielatou, N.; Doumas, S.; Economopoulou, P.; Foukas, P.G.; Psyrri, A. Biomarkers for immunotherapy response in head and neck cancer. Cancer Treat. Rev. 2020, 84, 101977. [Google Scholar] [CrossRef]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non-Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv. Anat. Pathol. 2017, 24, 311–335. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Almangush, A.; Ruuskanen, M.; Hagstrom, J.; Hirvikoski, P.; Tommola, S.; Kosma, V.M.; Nieminen, P.; Makitie, A.; Leivo, I. Tumor-infiltrating lymphocytes associate with outcome in nonendemic nasopharyngeal carcinoma: A multicenter study. Hum. Pathol. 2018, 81, 211–219. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Q.; Chen, Y.P.; Zhang, Y.; Jiang, W.; Liu, N.; Yun, J.P.; Sun, Y.; He, Q.M.; Tang, X.R.; Wen, X.; et al. Prognostic significance of tumor-infiltrating lymphocytes in non-disseminated nasopharyngeal carcinoma: A large-scale cohort study. Int. J. Cancer 2018, 142, 2558–2566. [Google Scholar] [CrossRef]
- Heikkinen, I.; Bello, I.O.; Wahab, A.; Hagstrom, J.; Haglund, C.; Coletta, R.D.; Nieminen, P.; Makitie, A.A.; Salo, T.; Leivo, I.; et al. Assessment of Tumor-infiltrating Lymphocytes Predicts the Behavior of Early-stage Oral Tongue Cancer. Am. J. Surg. Pathol. 2019, 43, 1392–1396. [Google Scholar] [CrossRef] [PubMed]
- De Keukeleire, S.J.; Vermassen, T.; De Meulenaere, A.; Deron, P.; Huvenne, W.; Duprez, F.; Creytens, D.; Van Dorpe, J.; Rottey, S.; Ferdinande, L. Tumour infiltrating lymphocytes in oropharyngeal carcinoma: Prognostic value and evaluation of a standardised method. Pathology 2021, 53, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.J.; Thirdborough, S.M.; Mellows, T.; Riley, C.; Harris, S.; Suchak, K.; Webb, A.; Hampton, C.; Patel, N.N.; Randall, C.J.; et al. Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer. Br. J. Cancer 2014, 110, 489–500. [Google Scholar] [CrossRef] [Green Version]
- Ruangritchankul, K.; Sandison, A.; Warburton, F.; Guerrero-Urbano, T.; Reis Ferreira, M.; Lei, M.; Thavaraj, S. Clinical evaluation of tumour-infiltrating lymphocytes as a prognostic factor in patients with human papillomavirus-associated oropharyngeal squamous cell carcinoma. Histopathology 2019, 75, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Faraji, F.; Fung, N.; Zaidi, M.; Gourin, C.C.; Eisele, D.W.; Rooper, L.M.; Fakhry, C. Tumor-infiltrating lymphocyte quantification stratifies early-stage human papillomavirus oropharynx cancer prognosis. Laryngoscope 2019, 130, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Wang, C.; Yuan, X.; Feng, Z.; Han, Z. Prognostic Value of Tumor-Infiltrating Lymphocytes for Patients With Head and Neck Squamous Cell Carcinoma. Transl. Oncol. 2017, 10, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wang, S.; Song, X.; Zeng, W.; Wang, S.; Chen, F.; Ding, H. The prognostic value of systemic and local inflammation in patients with laryngeal squamous cell carcinoma. Onco Targets Ther. 2016, 9, 7177–7185. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Tang, D.; Heng, Y.; Zhu, X.K.; Zhou, L.; Tao, L.; Lu, L.M. Prognostic Impact of Tumor-Infiltrating Lymphocytes in Laryngeal Squamous Cell Carcinoma Patients. Laryngoscope 2021, 131, E1249–E1255. [Google Scholar] [CrossRef]
- Wang, J.; Tian, S.; Sun, J.; Zhang, J.; Lin, L.; Hu, C. The presence of tumour-infiltrating lymphocytes (TILs) and the ratios between different subsets serve as prognostic factors in advanced hypopharyngeal squamous cell carcinoma. BMC Cancer 2020, 20, 731. [Google Scholar] [CrossRef]
- Huang, Y.; Lin, C.; Kao, H.K.; Hung, S.Y.; Ko, H.J.; Huang, Y.C.; Chang, Y.L.; Chang, K.P. Digital Image Analysis of CD8+ and CD3+ Tumor-Infiltrating Lymphocytes in Tongue Squamous Cell Carcinoma. Cancer Manag. Res. 2020, 12, 8275–8285. [Google Scholar] [CrossRef]
- Caruntu, A.; Moraru, L.; Lupu, M.; Vasilescu, F.; Dumitrescu, M.; Cioplea, M.; Popp, C.; Dragusin, A.; Caruntu, C.; Zurac, S. Prognostic Potential of Tumor-Infiltrating Immune Cells in Resectable Oral Squamous Cell Carcinoma. Cancers 2021, 13, 2268. [Google Scholar] [CrossRef]
- De Meulenaere, A.; Vermassen, T.; Aspeslagh, S.; Deron, P.; Duprez, F.; Laukens, D.; Van Dorpe, J.; Ferdinande, L.; Rottey, S. Tumor PD-L1 status and CD8(+) tumor-infiltrating T cells: Markers of improved prognosis in oropharyngeal cancer. Oncotarget 2017, 8, 80443–80452. [Google Scholar] [CrossRef] [Green Version]
- De Meulenaere, A.; Vermassen, T.; Aspeslagh, S.; Zwaenepoel, K.; Deron, P.; Duprez, F.; Rottey, S.; Ferdinande, L. Prognostic markers in oropharyngeal squamous cell carcinoma: Focus on CD70 and tumour infiltrating lymphocytes. Pathology 2017, 49, 397–404. [Google Scholar] [CrossRef]
- Taghavi, N.; Bagheri, S.; Akbarzadeh, A. Prognostic implication of CD57, CD16, and TGF-beta expression in oral squamous cell carcinoma. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2016, 45, 58–62. [Google Scholar] [CrossRef]
- Hori, Y.; Kubota, A.; Yokose, T.; Furukawa, M.; Matsushita, T.; Katsumata, N.; Oridate, N. Prognostic Role of Tumor-Infiltrating Lymphocytes and Tumor Budding in Early Oral Tongue Carcinoma. Laryngoscope 2021, 131, 2512–2518. [Google Scholar] [CrossRef]
- de Ruiter, E.J.; Ooft, M.L.; Devriese, L.A.; Willems, S.M. The prognostic role of tumor infiltrating T-lymphocytes in squamous cell carcinoma of the head and neck: A systematic review and meta-analysis. Oncoimmunology 2017, 6, e1356148. [Google Scholar] [CrossRef] [Green Version]
- Bisheshar, S.K.; De Ruiter, E.J.; Devriese, L.A.; Willems, S.M. The prognostic role of NK cells and their ligands in squamous cell carcinoma of the head and neck: A systematic review and meta-analysis. Oncoimmunology 2020, 9, 1747345. [Google Scholar] [CrossRef] [Green Version]
- Borsetto, D.; Tomasoni, M.; Payne, K.; Polesel, J.; Deganello, A.; Bossi, P.; Tysome, J.R.; Masterson, L.; Tirelli, G.; Tofanelli, M.; et al. Prognostic Significance of CD4+ and CD8+ Tumor-Infiltrating Lymphocytes in Head and Neck Squamous Cell Carcinoma: A Meta-Analysis. Cancers 2021, 13, 781. [Google Scholar] [CrossRef]
- Yang, W.F.; Wong, M.C.M.; Thomson, P.J.; Li, K.Y.; Su, Y.X. The prognostic role of PD-L1 expression for survival in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral Oncol 2018, 86, 81–90. [Google Scholar] [CrossRef]
- Rodrigo, J.P.; Sanchez-Canteli, M.; Lopez, F.; Wolf, G.T.; Hernandez-Prera, J.C.; Williams, M.D.; Willems, S.M.; Franchi, A.; Coca-Pelaz, A.; Ferlito, A. Tumor-Infiltrating Lymphocytes in the Tumor Microenvironment of Laryngeal Squamous Cell Carcinoma: Systematic Review and Meta-Analysis. Biomedicines 2021, 9, 486. [Google Scholar] [CrossRef]
- Taube, J.M. Emerging immunologic biomarkers: Setting the (TNM-immune) stage. Clin. Cancer Res. 2014, 20, 2023–2025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almangush, A.; Bello, I.O.; Heikkinen, I.; Hagstrom, J.; Haglund, C.; Kowalski, L.P.; Coletta, R.D.; Makitie, A.A.; Salo, T.; Leivo, I. Improving Risk Stratification of Early Oral Tongue Cancer with TNM-Immune (TNM-I) Staging System. Cancers 2021, 13, 486. [Google Scholar] [CrossRef] [PubMed]
- Zandberg, D.P.; Algazi, A.P.; Jimeno, A.; Good, J.S.; Fayette, J.; Bouganim, N.; Ready, N.E.; Clement, P.M.; Even, C.; Jang, R.W.; et al. Durvalumab for recurrent or metastatic head and neck squamous cell carcinoma: Results from a single-arm, phase II study in patients with ≥25% tumour cell PD-L1 expression who have progressed on platinum-based chemotherapy. Eur. J. Cancer 2019, 107, 142–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Baste, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Masarwy, R.; Kampel, L.; Horowitz, G.; Gutfeld, O.; Muhanna, N. Neoadjuvant PD-1/PD-L1 Inhibitors for Resectable Head and Neck Cancer: A Systematic Review and Meta-analysis. JAMA Otolaryngol Head Neck Surg. 2021, 147, 871–878. [Google Scholar] [CrossRef]
- Machiels, J.P.; Tao, Y.; Burtness, B.; Tahara, M.; Licitra, L.; Rischin, D.; Waldron, J.; Simon, C.; Gregoire, V.; Harrington, K.; et al. Pembrolizumab given concomitantly with chemoradiation and as maintenance therapy for locally advanced head and neck squamous cell carcinoma: KEYNOTE-412. Future Oncol. 2020, 16, 1235–1243. [Google Scholar] [CrossRef]
- Lee, N.Y.; Ferris, R.L.; Psyrri, A.; Haddad, R.I.; Tahara, M.; Bourhis, J.; Harrington, K.; Chang, P.M.; Lin, J.C.; Razaq, M.A.; et al. Avelumab plus standard-of-care chemoradiotherapy versus chemoradiotherapy alone in patients with locally advanced squamous cell carcinoma of the head and neck: A randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. Lancet Oncol. 2021, 22, 450–462. [Google Scholar] [CrossRef]
- Luen, S.J.; Salgado, R.; Fox, S.; Savas, P.; Eng-Wong, J.; Clark, E.; Kiermaier, A.; Swain, S.M.; Baselga, J.; Michiels, S.; et al. Tumour-infiltrating lymphocytes in advanced HER2-positive breast cancer treated with pertuzumab or placebo in addition to trastuzumab and docetaxel: A retrospective analysis of the CLEOPATRA study. Lancet Oncol. 2017, 18, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Bai, R.; Lv, Z.; Xu, D.; Cui, J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomark. Res. 2020, 8, 34. [Google Scholar] [CrossRef]
- Cogdill, A.P.; Andrews, M.C.; Wargo, J.A. Hallmarks of response to immune checkpoint blockade. Br. J. Cancer 2017, 117, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forget, M.A.; Haymaker, C.; Hess, K.R.; Meng, Y.J.; Creasy, C.; Karpinets, T.; Fulbright, O.J.; Roszik, J.; Woodman, S.E.; Kim, Y.U.; et al. Prospective Analysis of Adoptive TIL Therapy in Patients with Metastatic Melanoma: Response, Impact of Anti-CTLA4, and Biomarkers to Predict Clinical Outcome. Clin. Cancer Res. 2018, 24, 4416–4428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandal, R.; Senbabaoglu, Y.; Desrichard, A.; Havel, J.J.; Dalin, M.G.; Riaz, N.; Lee, K.W.; Ganly, I.; Hakimi, A.A.; Chan, T.A.; et al. The head and neck cancer immune landscape and its immunotherapeutic implications. JCI Insight 2016, 1, e89829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, G.J.; Lizotte, P.; Cavanaugh, M.; Kuo, F.C.; Shivdasani, P.; Frieden, A.; Chau, N.G.; Schoenfeld, J.D.; Lorch, J.H.; Uppaluri, R.; et al. Frameshift events predict anti-PD-1/L1 response in head and neck cancer. JCI Insight 2018, 3, e98811. [Google Scholar] [CrossRef] [Green Version]
- Chitsike, L.; Duerksen-Hughes, P.J. Targeted Therapy as a Potential De-Escalation Strategy in Locally Advanced HPV-Associated Oropharyngeal Cancer: A Literature Review. Front. Oncol. 2021, 11, 730412. [Google Scholar] [CrossRef]
- Denaro, N.; Russi, E.G.; Merlano, M.C. Pros and Cons of the New Edition of TNM Classification of Head and Neck Squamous Cell Carcinoma. Oncology 2018, 95, 202–210. [Google Scholar] [CrossRef]
- Rosenberg, A.J.; Vokes, E.E. Optimizing Treatment De-Escalation in Head and Neck Cancer: Current and Future Perspectives. Oncologist 2021, 26, 40–48. [Google Scholar] [CrossRef]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet 2019, 393, 40–50. [Google Scholar] [CrossRef]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [Green Version]
- El Sissy, C.; Kirilovsky, A.; Zeitoun, G.; Marliot, F.; Haicheur, N.; Lagorce-Pages, C.; Galon, J.; Pages, F. Therapeutic Implications of the Immunoscore in Patients with Colorectal Cancer. Cancers 2021, 13, 1281. [Google Scholar] [CrossRef]
- Bruni, D.; Angell, H.K.; Galon, J. The immune contexture and Immunoscore in cancer prognosis and therapeutic efficacy. Nat. Rev. Cancer 2020, 20, 662–680. [Google Scholar] [CrossRef]
- Galon, J.; Mlecnik, B.; Bindea, G.; Angell, H.K.; Berger, A.; Lagorce, C.; Lugli, A.; Zlobec, I.; Hartmann, A.; Bifulco, C.; et al. Towards the introduction of the ‘Immunoscore’ in the classification of malignant tumours. J. Pathol. 2014, 232, 199–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ruiter, E.J.; de Roest, R.H.; Brakenhoff, R.H.; Leemans, C.R.; de Bree, R.; Terhaard, C.H.J.; Willems, S.M. Digital pathology-aided assessment of tumor-infiltrating T lymphocytes in advanced stage, HPV-negative head and neck tumors. Cancer Immunol. Immunother. 2020, 69, 581–591. [Google Scholar] [CrossRef] [Green Version]
- Sung, Y.E.; Kim, M.S.; Lee, Y.S. Proposal of a scoring system for predicting pathological risk based on a semiautomated analysis of whole slide images in oral squamous cell carcinoma. Head Neck 2021, 43, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Hartman, D.J.; Ahmad, F.; Ferris, R.L.; Rimm, D.L.; Pantanowitz, L. Utility of CD8 score by automated quantitative image analysis in head and neck squamous cell carcinoma. Oral Oncol 2018, 86, 278–287. [Google Scholar] [CrossRef] [PubMed]
- De Meulenaere, A.; Vermassen, T.; Creytens, D.; Aspeslagh, S.; Deron, P.; Duprez, F.; Rottey, S.; Van Dorpe, J.A.; Ferdinande, L. Importance of choice of materials and methods in PD-L1 and TIL assessment in oropharyngeal squamous cell carcinoma. Histopathology 2018, 73, 500–509. [Google Scholar] [CrossRef]
- Althammer, S.; Tan, T.H.; Spitzmuller, A.; Rognoni, L.; Wiestler, T.; Herz, T.; Widmaier, M.; Rebelatto, M.C.; Kaplon, H.; Damotte, D.; et al. Automated image analysis of NSCLC biopsies to predict response to anti-PD-L1 therapy. J. Immunother. Cancer 2019, 7, 121. [Google Scholar] [CrossRef] [Green Version]
- Acs, B.; Salgado, R.; Hartman, J. What do we still need to learn on digitally assessed biomarkers? EBioMedicine 2021, 70, 103520. [Google Scholar] [CrossRef]
- Sun, P.; He, J.; Chao, X.; Chen, K.; Xu, Y.; Huang, Q.; Yun, J.; Li, M.; Luo, R.; Kuang, J.; et al. A Computational Tumor-Infiltrating Lymphocyte Assessment Method Comparable with Visual Reporting Guidelines for Triple-Negative Breast Cancer. EBioMedicine 2021, 70, 103492. [Google Scholar] [CrossRef]
- Shaban, M.; Khurram, S.A.; Fraz, M.M.; Alsubaie, N.; Masood, I.; Mushtaq, S.; Hassan, M.; Loya, A.; Rajpoot, N.M. A Novel Digital Score for Abundance of Tumour Infiltrating Lymphocytes Predicts Disease Free Survival in Oral Squamous Cell Carcinoma. Sci. Rep. 2019, 9, 13341. [Google Scholar] [CrossRef] [Green Version]
- Badr, M.; Johrens, K.; Allgauer, M.; Boxberg, M.; Weichert, W.; Tinhofer, I.; Denkert, C.; Schirmacher, P.; Stenzinger, A.; Budczies, J. Morphomolecular analysis of the immune tumor microenvironment in human head and neck cancer. Cancer Immunol. Immunother. 2019, 68, 1443–1454. [Google Scholar] [CrossRef] [PubMed]
- Shaban, M.; Ahmed Raza, S.E.; Hassan, M.; Jamshed, A.; Mushtaq, S.; Loya, A.; Batis, N.; Brooks, J.; Nankivell, P.; Sharma, N.; et al. A digital score of tumour-associated stroma infiltrating lymphocytes predicts survival in head and neck squamous cell carcinoma. J. Pathol. 2021, 256, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Abe, N.; Matsumoto, H.; Takamatsu, R.; Tamaki, K.; Takigami, N.; Uehara, K.; Kamada, Y.; Tamaki, N.; Motonari, T.; Unesoko, M.; et al. Quantitative digital image analysis of tumor-infiltrating lymphocytes in HER2-positive breast cancer. Virchows Arch. Int. J. Pathol. 2020, 476, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.Y.; Park, H.E.; Kim, J.H.; Wen, X.; Jeong, S.; Cho, N.Y.; Gwon, H.G.; Kim, K.; Lee, H.S.; Jeong, S.Y.; et al. Whole-Slide Image Analysis Reveals Quantitative Landscape of Tumor-Immune Microenvironment in Colorectal Cancers. Clin. Cancer Res. 2020, 26, 870–881. [Google Scholar] [CrossRef]
- Acs, B.; Ahmed, F.S.; Gupta, S.; Wong, P.F.; Gartrell, R.D.; Sarin Pradhan, J.; Rizk, E.M.; Gould Rothberg, B.; Saenger, Y.M.; Rimm, D.L. An open source automated tumor infiltrating lymphocyte algorithm for prognosis in melanoma. Nat. Commun. 2019, 10, 5440. [Google Scholar] [CrossRef]
- Nederlof, I.; De Bortoli, D.; Bareche, Y.; Nguyen, B.; de Maaker, M.; Hooijer, G.K.J.; Buisseret, L.; Kok, M.; Smid, M.; Van den Eynden, G.; et al. Comprehensive evaluation of methods to assess overall and cell-specific immune infiltrates in breast cancer. Breast Cancer Res. BCR 2019, 21, 151. [Google Scholar] [CrossRef] [Green Version]
- Galon, J.; Costes, A.; Sanchez-Cabo, F.; Kirilovsky, A.; Mlecnik, B.; Lagorce-Pages, C.; Tosolini, M.; Camus, M.; Berger, A.; Wind, P.; et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 2006, 313, 1960–1964. [Google Scholar] [CrossRef] [Green Version]
- Miyakita, H.; Sadahiro, S.; Suzuki, T.; Chan, L.F.; Ogimi, T.; Okada, K.; Yamamoto, S.; Kajiwara, H. Tumor-Infiltrating Lymphocytes in Biopsy Specimens Obtained 7 Days after Starting Chemoradiotherapy for Rectal Cancer Are Predictors of the Response to Chemoradiotherapy. Oncology 2020, 98, 869–875. [Google Scholar] [CrossRef]
- Miyasaka, Y.; Yoshimoto, Y.; Murata, K.; Noda, S.E.; Ando, K.; Ebara, T.; Okonogi, N.; Kaminuma, T.; Yamada, S.; Ikota, H.; et al. Treatment outcomes of patients with adenocarcinoma of the uterine cervix after definitive radiotherapy and the prognostic impact of tumor-infiltrating CD8+ lymphocytes in pre-treatment biopsy specimens: A multi-institutional retrospective study. J. Radiat. Res. 2020, 61, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Harada, Y.; Kazama, S.; Morikawa, T.; Sonoda, H.; Ishi, H.; Emoto, S.; Murono, K.; Kaneko, M.; Sasaki, K.; Shuno, Y.; et al. Clinical significance of CD8(+) and FoxP3(+) tumor-infiltrating lymphocytes and MFG-E8 expression in lower rectal cancer with preoperative chemoradiotherapy. Mol. Clin. Oncol. 2021, 14, 87. [Google Scholar] [CrossRef]
- Takada, K.; Kashiwagi, S.; Asano, Y.; Goto, W.; Kouhashi, R.; Yabumoto, A.; Morisaki, T.; Shibutani, M.; Takashima, T.; Fujita, H.; et al. Prediction of lymph node metastasis by tumor-infiltrating lymphocytes in T1 breast cancer. BMC Cancer 2020, 20, 598. [Google Scholar] [CrossRef] [PubMed]
- Brcic, I.; Gallob, M.; Schwantzer, G.; Zrnc, T.; Weiland, T.; Thurnher, D.; Wolf, A.; Brcic, L. Concordance of tumor infiltrating lymphocytes, PD-L1 and p16 expression in small biopsies, resection and lymph node metastases of oropharyngeal squamous cell carcinoma. Oral Oncol. 2020, 106, 104719. [Google Scholar] [CrossRef] [PubMed]
- Almangush, A.; Jouhi, L.; Atula, T.; Haglund, C.; Makitie, A.A.; Hagstrom, J.; Leivo, I. Tumour-infiltrating lymphocytes in oropharyngeal cancer: A validation study according to the criteria of the International Immuno-Oncology Biomarker Working Group. Br. J. Cancer 2022. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Author (Year) | TILs Subset | No. Studies (No. Cases) | Endpoint | SCC Location | Pooled HR (95% CI), p |
|---|---|---|---|---|---|
| de Ruiter et al. [27] (2017) | CD3+ | 4 studies (904 cases) | OS | HNSCC | HR 0.64 (0.47–0.85) |
| 4 studies (735 cases) | DFS | HNSCC | HR 0.63 (0.49–0.82) | ||
| CD8+ | 9 studies (1697 cases) | OS | HNSCC | HR 0.67 (0.58–0.79) | |
| 7 studies (1053 cases) | DFS | HNSCC | HR 0.50 (0.37–0.68) | ||
| 4 studies (596 cases) | LRC | HNSCC | HR 0.82 (0.70–0.96) | ||
| CD4+ | 4 studies (775 cases) | OS | HNSCC | HR 0.76 (0.64–0.89) | |
| 3 studies (513 cases) | LRC | HNSCC | HR 0.81 (0.68–0.96) | ||
| FoxP3+ | 6 studies (977 cases) | OS | HNSCC | HR 0.80 (0.70–0.92) | |
| Yang et al. [30] (2018) | PD-L1 | 21 studies (2477 cases) | OS | HNSCC | HR 0.98 (0.71–1.37), p = 0.93 |
| 7 studies (1001 cases) | DFS | HNSCC | HR 1.07 (0.68–1.70), p = 0.76 | ||
| 4 studies (592 cases) | DSS | HNSCC | HR 0.90 (0.63–1.29), p = 0.56 | ||
| 6 studies (585 cases) | PFS | HNSCC | HR 0.71 (0.55–0.93), p = 0.01 | ||
| Bisheshar et al. [28] (2020) | CD56/CD57 | 4 studies (420 cases) | OS | HNSCC | HR 0.19 (0.11–0.35) |
| Borsetto et al. [29] (2021) | CD4+ | 3 studies (548 cases) | OS | HNSSCC | HR 0.77 (0.65–0.93) |
| CD8+ | 6 studies (1220 cases) | OS | HNSSCC | HR 0.64 (0.47–0.88) | |
| CD4+ | 3 studies (498 cases) | OS | OPSCC | HR 0.52 (0.31–0.89) | |
| CD8+ | 3 studies (326 cases) | OS | OPSCC (HPV-Neg) | HR 0.39 (0.16–0.93) | |
| CD8+ | 6 studies (661 cases) | OS | OPSCC (HPV-Pos) | HR 0.40 (0.21–0.76) | |
| CD8+ | 3 studies (250 cases) | OS | Hypopharyngeal SCC | HR 0.43 (0.30–0.63) | |
| Rodrigo et al. [31] (2021) | HE staining | 4 studies (719 cases) | OS | Laryngeal SCC | HR 0.57 (0.36–0.91), p = 0.02 |
| HE staining | 4 studies (659 cases) | DFS | Laryngeal SCC | HR 0.56 (0.34–0.94), p = 0.03 | |
| CD8+ | 5 studies (536 caess) | OS | Laryngeal SCC | HR 0.62 (0.40–0.97), p = 0.04 | |
| CD8+ | 4 studies (574 caess) | DFS | Laryngeal SCC | HR 0.73 (0.60–0.90), p = 0.002 | |
| CD3+/CD4+ | 4 studies (369 caess) | OS | Laryngeal SCC | HR 0.38 (0.16–0.9), p = 0.03 | |
| CD3+/CD4+ | 2 studies (224 caess) | DFS | Laryngeal SCC | HR 0.23 (0.10–0.53), p = 0.0005 |
| To do | How? | Current Status | Future Steps |
|---|---|---|---|
| Construct standardized methods | International working groups | IIBWG method Immunoscore | Further improvement upon external feedback |
| Registry trials | Large scale observational trials per subsite | Retrospective trials only | Nation-wide/international analysis using standardized protocols |
| Prospective validation (predictive/prognostic value) | Clinical trials (introduce TNM–Immune) | Retrospective trials only | Interventional clinical trials(de-escalation strategies) |
| Determining clinically valuable cutoff | Further dissemination and implementation of TIL quantification | Continuous variable only for more accurate statistical analysis | Introduce di-/trichotomized cutoffs (non vs. moderately vs. highly inflamed tumors) |
| Education | Symposia Congresses Workshops | Word-of-mouth marketing | Further implementationof the method |
| Quality control | Ring trials | Non-existing in HNSCC | Further implementationof the method |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almangush, A.; De Keukeleire, S.; Rottey, S.; Ferdinande, L.; Vermassen, T.; Leivo, I.; Mäkitie, A.A. Tumor-Infiltrating Lymphocytes in Head and Neck Cancer: Ready for Prime Time? Cancers 2022, 14, 1558. https://doi.org/10.3390/cancers14061558
Almangush A, De Keukeleire S, Rottey S, Ferdinande L, Vermassen T, Leivo I, Mäkitie AA. Tumor-Infiltrating Lymphocytes in Head and Neck Cancer: Ready for Prime Time? Cancers. 2022; 14(6):1558. https://doi.org/10.3390/cancers14061558
Chicago/Turabian StyleAlmangush, Alhadi, Stijn De Keukeleire, Sylvie Rottey, Liesbeth Ferdinande, Tijl Vermassen, Ilmo Leivo, and Antti A. Mäkitie. 2022. "Tumor-Infiltrating Lymphocytes in Head and Neck Cancer: Ready for Prime Time?" Cancers 14, no. 6: 1558. https://doi.org/10.3390/cancers14061558
APA StyleAlmangush, A., De Keukeleire, S., Rottey, S., Ferdinande, L., Vermassen, T., Leivo, I., & Mäkitie, A. A. (2022). Tumor-Infiltrating Lymphocytes in Head and Neck Cancer: Ready for Prime Time? Cancers, 14(6), 1558. https://doi.org/10.3390/cancers14061558