
Correlation of Intraoperative 5-ALA-Induced Fluorescence Intensity and Preoperative 11C-Methionine PET Uptake in Glioma Surgery

 , ,
, ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. MET-PET Scan
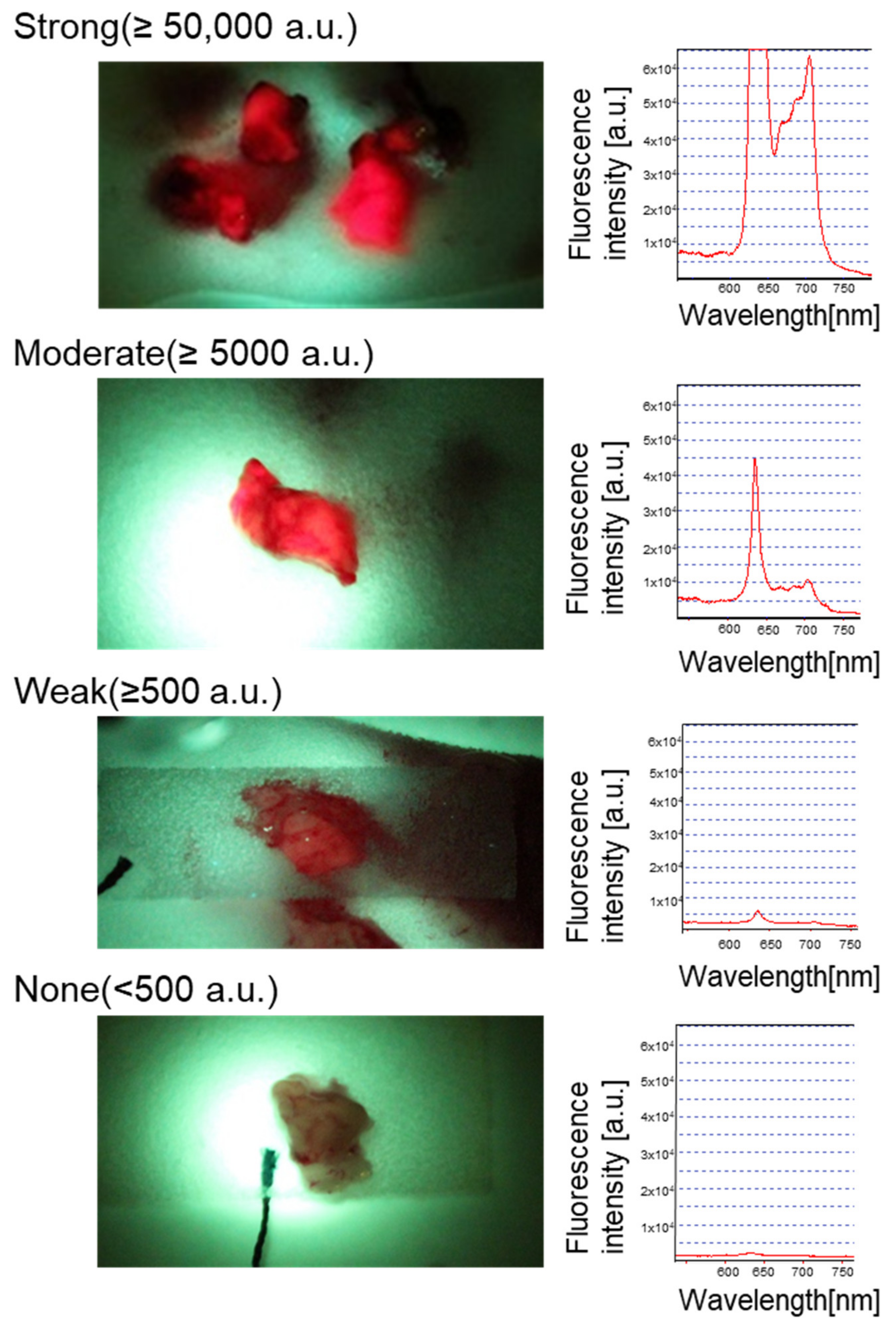
2.3. Tissue Sampling and Fluorescence Measurement
2.4. Histopathological Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in adults: A society for neuro-oncology (sno) and European society of neuro-oncology (eano) consensus review on current management and future directions. Neuro-Oncology 2020, 22, 1073–1113. [Google Scholar] [CrossRef] [PubMed]
- Domino, J.S.; Ormond, D.R.; Germano, I.M.; Sami, M.; Ryken, T.C.; Olson, J.J. Cytoreductive surgery in the management of newly diagnosed glioblastoma in adults: A systematic review and evidence-based clinical practice guideline update. J. Neurooncol. 2020, 150, 121–142. [Google Scholar] [CrossRef] [PubMed]
- Sanai, N.; Berger, M.S. Glioma extent of resection and its impact on patient outcome. Neurosurgery 2008, 62, 753–764, discussion 264–266. [Google Scholar] [CrossRef] [Green Version]
- Belykh, E.; Martirosyan, N.L.; Yagmurlu, K.; Miller, E.J.; Eschbacher, J.M.; Izadyyazdanabadi, M.; Bardonova, L.A.; Byvaltsev, V.A.; Nakaji, P.; Preul, M.C. Intraoperative fluorescence imaging for personalized brain tumor resection: Current state and future directions. Front. Surg. 2016, 3, 55. [Google Scholar] [CrossRef] [Green Version]
- Ewelt, C.; Nemes, A.; Senner, V.; Wolfer, J.; Brokinkel, B.; Stummer, W.; Holling, M. Fluorescence in neurosurgery: Its diagnostic and therapeutic use. Review of the literature. J. Photochem. Photobiol. B 2015, 148, 302–309. [Google Scholar] [CrossRef]
- Behbahaninia, M.; Martirosyan, N.L.; Georges, J.; Udovich, J.A.; Kalani, M.Y.; Feuerstein, B.G.; Nakaji, P.; Spetzler, R.F.; Preul, M.C. Intraoperative fluorescent imaging of intracranial tumors: A review. Clin. Neurol. Neurosurg. 2013, 115, 517–528. [Google Scholar] [CrossRef]
- Kostron, H. Photodynamic diagnosis and therapy and the brain. In Photodynamic Therapy: Methods and Protocols; Gomer, C.J., Ed.; Humana Press: Totowa, NJ, USA, 2010; pp. 261–280. [Google Scholar]
- Stummer, W.; Stocker, S.; Wagner, S.; Stepp, H.; Fritsch, C.; Goetz, C.; Goetz, A.E.; Kiefmann, R.; Reulen, H.J. Intraoperative detection of malignant gliomas by 5-aminolevulinic acid-induced porphyrin fluorescence. Neurosurgery 1998, 42, 518–525, discussion 25–26. [Google Scholar]
- Zhao, S.; Wu, J.; Wang, C.; Liu, H.; Dong, X.; Shi, C.; Shi, C.; Liu, Y.; Teng, L.; Han, D.; et al. Intraoperative fluorescence-guided resection of high-grade malignant gliomas using 5-aminolevulinic acid-induced porphyrins: A systematic review and meta-analysis of prospective studies. PLoS ONE 2013, 8, e63682. [Google Scholar] [CrossRef]
- Valdes, P.A.; Bekelis, K.; Harris, B.T.; Wilson, B.C.; Leblond, F.; Kim, A.; Simmons, N.E.; Erkmen, K.; Paulsen, K.D.; Roberts, D.W. 5-aminolevulinic acid-induced protoporphyrin ix fluorescence in meningioma: Qualitative and quantitative measurements in vivo. Neurosurgery 2014, 10 (Suppl. S1), 74–82; discussion 82–83. [Google Scholar] [CrossRef] [Green Version]
- Kiesel, B.; Millesi, M.; Woehrer, A.; Furtner, J.; Bavand, A.; Roetzer, T.; Mischkulnig, M.; Wolfsberger, S.; Preusser, M.; Knosp, E.; et al. 5-ala-induced fluorescence as a marker for diagnostic tissue in stereotactic biopsies of intracranial lymphomas: Experience in 41 patients. Neurosurg. Focus 2018, 44, E7. [Google Scholar] [CrossRef] [Green Version]
- Kelty, C.J.; Brown, N.J.; Reed, M.W.; Ackroyd, R. The use of 5-aminolaevulinic acid as a photosensitiser in photodynamic therapy and photodiagnosis. Photochem. Photobiol. Sci. 2002, 1, 158–168. [Google Scholar] [CrossRef]
- Stummer, W.; Stocker, S.; Novotny, A.; Heimann, A.; Sauer, O.; Kempski, O.; Plesnila, N.; Wietzorrek, J.; Reulen, H.J. In vitro and in vivo porphyrin accumulation by c6 glioma cells after exposure to 5-aminolevulinic acid. J. Photochem. Photobiol. B Biol. 1998, 45, 160–169. [Google Scholar] [CrossRef]
- Ma, R.; Watts, C. Selective 5-aminolevulinic acid-induced protoporphyrin ix fluorescence in gliomas. Acta Neurochir. 2016, 158, 1935–1941. [Google Scholar] [CrossRef]
- Kobuchi, H.; Moriya, K.; Ogino, T.; Fujita, H.; Inoue, K.; Shuin, T.; Yasuda, T.; Utsumi, K.; Utsumi, T. Mitochondrial localization of abc transporter abcg2 and its function in 5-nolevulinic acid-mediated protoporphyrin ix accumulation. PLoS ONE 2012, 7, e50082. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, T.; Kajimoto, Y.; Inoue, Y.; Ikegami, Y.; Kuroiwa, T. Critical role of abcg2 in ala-photodynamic diagnosis and therapy of human brain tumor. Adv. Cancer Res. 2015, 125, 197–216. [Google Scholar] [CrossRef]
- Ennis, S.R.; Novotny, A.; Xiang, J.; Shakui, P.; Masada, T.; Stummer, W.; Smith, D.E.; Keep, R.F. Transport of 5-aminolevulinic acid between blood and brain. Brain Res. 2003, 959, 226–234. [Google Scholar] [CrossRef]
- Valdes, P.A.; Kim, A.; Brantsch, M.; Niu, C.; Moses, Z.B.; Tosteson, T.D.; Wilson, B.C.; Paulsen, K.D.; Roberts, D.W.; Harris, T.B. Delta-aminolevulinic acid-induced protoporphyrin ix concentration correlates with histopathologic markers of malignancy in human gliomas: The need for quantitative fluorescence-guided resection to identify regions of increasing malignancy. Neuro-Oncology 2011, 13, 846–856. [Google Scholar] [CrossRef] [Green Version]
- Coburger, J.; Scheuerle, A.; Pala, A.; Thal, D.; Wirtz, C.R.; König, R. Histopathological insights on imaging results of intraoperative magnetic resonance imaging, 5-aminolevulinic acid, and intraoperative ultrasound in glioblastoma surgery. Neurosurgery 2017, 81, 165–174. [Google Scholar] [CrossRef]
- Ando, T.; Kobayashi, E.; Liao, H.; Maruyama, T.; Muragaki, Y.; Iseki, H.; Kubo, O.; Sakuma, I. Precise comparison of protoporphyrin ix fluorescence spectra with pathological results for brain tumor tissue identification. Brain Tumor Pathol. 2011, 28, 43–51. [Google Scholar] [CrossRef]
- Stummer, W.; Tonn, J.C.; Goetz, C.; Ullrich, W.; Stepp, H.; Bink, A.; Pietsch, T.; Pichlmeier, U. 5-aminolevulinic acid-derived tumor fluorescence: The diagnostic accuracy of visible fluorescence qualities as corroborated by spectrometry and histology and postoperative imaging. Neurosurgery 2014, 74, 310–319, discussion 19–20. [Google Scholar] [CrossRef] [Green Version]
- Ferraro, N.; Barbarite, E.; Albert, T.R.; Berchmans, E.; Shah, A.H.; Bregy, A.; Ivan, M.E.; Brown, T.; Komotar, R.J. The role of 5-aminolevulinic acid in brain tumor surgery: A systematic review. Neurosurg. Rev. 2016, 39, 545–555. [Google Scholar] [CrossRef]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.J. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomised controlled multicentre phase iii trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Eatz, T.A.; Eichberg, D.G.; Lu, V.M.; Di, L.; Komotar, R.J.; Ivan, M.E. Intraoperative 5-ala fluorescence-guided resection of high-grade glioma leads to greater extent of resection with better outcomes: A systematic review. J. Neurooncol. 2022, 156, 233–256. [Google Scholar] [CrossRef]
- Pala, A.; Reske, S.N.; Eberhardt, N.; Scheuerle, A.; Konig, R.; Schmitz, B.; Beer, A.J.; Wirtz, C.R.; Coburger, J. Diagnostic accuracy of intraoperative perfusion-weighted mri and 5-aminolevulinic acid in relation to contrast-enhanced intraoperative mri and (11)c-methionine positron emission tomography in resection of glioblastoma: A prospective study. Neurosurg. Rev. 2019, 42, 471–479. [Google Scholar] [CrossRef]
- Nariai, T.; Tanaka, Y.; Wakimoto, H.; Aoyagi, M.; Tamaki, M.; Ishiwata, K.; Senda, M.; Ishii, K.; Hirakawa, K.; Ohno, K. Usefulness of l-[methyl-11c] methionine-positron emission tomography as a biological monitoring tool in the treatment of glioma. J. Neurosurg. 2005, 103, 498–507. [Google Scholar] [CrossRef]
- Smith, Q.R.; Takasato, Y. Kinetics of amino acid transport at the blood-brain barrier studied using an in situ brain perfusion technique. Ann. N. Y. Acad. Sci. 1986, 481, 186–201. [Google Scholar] [CrossRef]
- Jager, P.L.; Vaalburg, W.; Pruim, J.; de Vries, E.G.; Langen, K.J.; Piers, D.A. Radiolabeled amino acids: Basic aspects and clinical applications in oncology. J. Nucl. Med. 2001, 42, 432–445. [Google Scholar]
- Nojiri, T.; Nariai, T.; Aoyagi, M.; Senda, M.; Ishii, K.; Ishiwata, K.; Ohno, K. Contributions of biological tumor parameters to the incorporation rate of l-[methyl-11c] methionine into astrocytomas and oligodendrogliomas. J. Neurooncol. 2008, 93, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Miwa, K.; Shinoda, J.; Yano, H.; Okumura, A.; Iwama, T.; Nakashima, T.; Sakai, N. Discrepancy between lesion distributions on methionine pet and mr images in patients with glioblastoma multiforme: Insight from a pet and mr fusion image study. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1457–1462. [Google Scholar] [CrossRef] [Green Version]
- Palanichamy, K.; Chakravarti, A. Diagnostic and prognostic significance of methionine uptake and methionine positron emission tomography imaging in gliomas. Front. Oncol. 2017, 7, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, S.; Inaji, M.; Nariai, T.; Kobayashi, D.; Sanjo, N.; Yokota, T.; Ishii, K.; Taketoshi, M. Usefulness of [(11)c] methionine pet in the differentiation of tumefactive multiple sclerosis from high grade astrocytoma. Neurol. Med. Chir. 2019, 59, 176–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, Y.; Nariai, T.; Momose, T.; Aoyagi, M.; Maehara, T.; Tomori, T.; Yoshino, Y.; Nagaoka, T.; Ishiwata, K.; Ishii, K.; et al. Glioma surgery using a multimodal navigation system with integrated metabolic images. J. Neurosurg. 2009, 110, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Nitta, M.; Komori, T.; Maruyama, T.; Yasuda, T.; Fujii, Y.; Masamune, K.; Kawamata, T.; Maehara, T.; Muragaki, Y. Intraoperative photodynamic diagnosis using talaporfin sodium simultaneously applied for photodynamic therapy against malignant glioma: A prospective clinical study. Front. Neurol. 2018, 9, 24. [Google Scholar] [CrossRef] [Green Version]
- Ericson, M.B.; Grapengiesser, S.; Gudmundson, F.; Wennberg, A.M.; Larko, O.; Moan, J.; Rosen, A. A spectroscopic study of the photobleaching of protoporphyrin ix in solution. Lasers Med. Sci. 2003, 18, 56–62. [Google Scholar] [CrossRef]
- Johnson, K.O.; Hsiao, S.S.; Yoshioka, T. Review: Neural coding and the basic law of psychophysics. Neuroscientist 2002, 8, 111–121. [Google Scholar] [CrossRef]
- Arita, H.; Kinoshita, M.; Kagawa, N.; Fujimoto, Y.; Kishima, H.; Hashimoto, N.; Yoshimine, T. (1)(1)c-methionine uptake and intraoperative 5-aminolevulinic acid-induced fluorescence as separate index markers of cell density in glioma: A stereotactic image-histological analysis. Cancer 2012, 118, 1619–1627. [Google Scholar] [CrossRef]
- Lau, D.; Hervey-Jumper, S.L.; Chang, S.; Molinaro, A.M.; McDermott, M.W.; Phillips, J.J.; Berger, M.S. A prospective phase ii clinical trial of 5-aminolevulinic acid to assess the correlation of intraoperative fluorescence intensity and degree of histologic cellularity during resection of high-grade gliomas. J. Neurosurg. 2016, 124, 1300–1309. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.; Shinoda, J.; Oka, N.; Miwa, K.; Nakayama, N.; Yano, H.; Maruyama, T.; Muragaki, Y.; Iwama, T. Analysis of 11c-methionine uptake in low-grade gliomas and correlation with proliferative activity. AJNR Am. J. Neuroradiol. 2008, 29, 1867–1871. [Google Scholar] [CrossRef] [Green Version]
- Goryaynov, S.A.; Widhalm, G.; Goldberg, M.F.; Chelushkin, D.; Spallone, A.; Chernyshov, K.A.; Ryzhova, M.; Pavlova, G.; Revischin, A.; Shishkina, L.; et al. The role of 5-ala in low-grade gliomas and the influence of antiepileptic drugs on intraoperative fluorescence. Front. Oncol. 2019, 9, 423. [Google Scholar] [CrossRef] [Green Version]
- Hefti, M.; Albert, I.; Luginbuehl, V. Phenytoin reduces 5-aminolevulinic acid-induced protoporphyrin ix accumulation in malignant glioma cells. J. Neurooncol. 2012, 108, 443–450. [Google Scholar] [CrossRef]
- Lawrence, J.E.; Steele, C.J.; Rovin, R.A.; Belton, R.J., Jr.; Winn, R.J. Dexamethasone alone and in combination with desipramine, phenytoin, valproic acid or levetiracetam interferes with 5-ala-mediated ppix production and cellular retention in glioblastoma cells. J. Neurooncol. 2016, 127, 15–21. [Google Scholar] [CrossRef]
- Okubo, S.; Zhen, H.N.; Kawai, N.; Nishiyama, Y.; Haba, R.; Tamiya, T. Correlation of l-methyl-11c-methionine (met) uptake with l-type amino acid transporter 1 in human gliomas. J. Neurooncol. 2010, 99, 217–225. [Google Scholar] [CrossRef]
- McNicholas, K.; MacGregor, M.N.; Gleadle, J.M. In order for the light to shine so brightly, the darkness must be present-why do cancers fluoresce with 5-aminolaevulinic acid? Br. J. Cancer 2019, 121, 631–639. [Google Scholar] [CrossRef]
- Tran, T.T.; Mu, A.; Adachi, Y.; Adachi, Y.; Taketani, S. Neurotransmitter transporter family including slc6a6 and slc6a13 contributes to the 5-aminolevulinic acid (ala)-induced accumulation of protoporphyrin ix and photodamage, through uptake of ala by cancerous cells. Photochem. Photobiol. 2014, 90, 1136–1143. [Google Scholar] [CrossRef]
- Hagiya, Y.; Fukuhara, H.; Matsumoto, K.; Endo, Y.; Nakajima, M.; Tanaka, T.; Okura, I.; Kurabayashi, A.; Furihata, M.; Inoue, K.; et al. Expression levels of pept1 and abcg2 play key roles in 5-aminolevulinic acid (ala)-induced tumor-specific protoporphyrin ix (ppix) accumulation in bladder cancer. Photodiagn. Photodyn. Ther. 2013, 10, 288–295. [Google Scholar] [CrossRef]
- Hagiya, Y.; Endo, Y.; Yonemura, Y.; Takahashi, K.; Ishizuka, M.; Abe, F.; Tanaka, T.; Okura, I.; Nakajima, M.; Ishikawa, T.; et al. Pivotal roles of peptide transporter pept1 and atp-binding cassette (abc) transporter abcg2 in 5-aminolevulinic acid (ala)-based photocytotoxicity of gastric cancer cells in vitro. Photodiagn. Photodyn. Ther. 2012, 9, 204–214. [Google Scholar] [CrossRef]
- Mitamura, K.; Yamamoto, Y.; Norikane, T.; Hatakeyama, T.; Okada, M.; Nishiyama, Y. Correlation of (18)f-fdg and (11)c-methionine uptake on pet/ct with ki-67 immunohistochemistry in newly diagnosed intracranial meningiomas. Ann. Nucl. Med. 2018, 32, 627–633. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Age (Years) | Sex | Localization | Histology | WHO Grade | Tumor Status | IDH-1 | Ki67 | Gd Enhancement | AED | Fluorescence Intesnsity | Met SUV | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T/N | Tumor | Normal | ||||||||||||
| 1 | 54 | M | Parietal | GBM | IV | Recurrent | Wild type | 23.5 | Ring/Solid | LEV | Strong | 2.83 | 5.72 | 2.02 |
| 2 | 78 | F | Temporal | GBM | IV | New | Wild type | 18.9 | Ring/Solid | None | Strong | 3.82 | 4.96 | 1.3 |
| 3 | 59 | M | Temporal | GBM | IV | New | Wild type | 27.4 | Ring/Solid | LEV | Strong | 4.78 | 6.84 | 1.43 |
| 4 | 67 | F | Temporal | GBM | IV | New | Wild type | 43.4 | Ring/Solid | LEV | Strong | 4.66 | 8.44 | 1.81 |
| 5 | 78 | M | Frontal | GBM | IV | New | Wild type | 82.8 | Ring/Solid | LEV | Strong | 3.05 | 4.48 | 1.47 |
| 6 | 37 | F | Frontal | GBM | IV | Recurrent | Mutant | 35.4 | Ring/Solid | LEV | Strong | 2.51 | 6.7 | 2.67 |
| 7 | 65 | M | Temporal | GBM | IV | New | Wild type | 18.9 | Ring/Solid | LEV | Strong | 3.65 | 4.02 | 1.1 |
| 8 | 67 | F | Temporal | GBM | IV | Recurrent | Wild type | 43.8 | Ring/Solid | None | Strong | 1.51 | 2.71 | 1.8 |
| 9 | 53 | M | Temporal | GBM | IV | New | Wild type | 30.9 | Ring/Solid | LEV | Strong | 2.95 | 4.04 | 1.37 |
| 10 | 72 | F | Frontal | GBM | IV | New | Wild type | 24.2 | Ring/Solid | NA | Strong | 4 | 8.15 | 2.04 |
| 11 | 38 | F | Frontal | GBM | IV | Recurrent | Mutant | 48 | Ring/Solid | LEV | Strong | 4.04 | 9.65 | 2.39 |
| 12 | 70 | M | Temporal | GBM | IV | New | Wild type | 16.9 | Ring/Solid | LEV | Strong | 4.91 | 7.42 | 1.51 |
| 13 | 26 | M | Parietal | GBM | IV | Recurrent | Unknown | NA | Ring/Solid | None | Strong | 2.8 | 4.79 | 1.71 |
| 14 | 72 | F | Parietal | GBM | IV | New | Wild type | 39.5 | None/Slight | None | Strong | 1.6 | 3.27 | 2.04 |
| 15 | 77 | M | Frontal | GBM | IV | New | Wild type | 23.6 | Ring/Solid | Others | Strong | 3.82 | 5.46 | 1.43 |
| 16 | 81 | F | Frontal | GBM | IV | New | Wild type | 32.5 | Ring/Solid | LEV | Strong | 2.75 | 5.67 | 2.06 |
| 17 | 69 | M | Frontal | GBM | IV | New | Wild type | 45 | Ring/Solid | LEV | Strong | 3.66 | 8.09 | 2.21 |
| 18 | 46 | M | Temporal | GBM | IV | New | Wild type | 28.6 | Ring/Solid | LEV | Strong | 3.84 | 6.45 | 1.68 |
| 19 | 52 | F | Temporal | AA | III | New | Mutant | 9.8 | None/Slight | None | Weak | 1.93 | 3.24 | 1.68 |
| 20 | 54 | M | Parietal | AA | III | Recurrent | Mutant | 4.7 | None/Slight | LEV | Weak | 2.22 | 1.71 | 0.77 |
| 21 | 23 | M | Temporal | AA | III | New | Wild type | 16.2 | None/Slight | LEV | None | 1.82 | 2.35 | 1.29 |
| 22 | 44 | F | Frontal | AA | III | New | Mutant | 14 | None/Slight | LEV | None | 2.57 | 4.65 | 1.81 |
| 23 | 23 | F | Frontal | AA | III | New | Wild type | 8.4 | None/Slight | LEV | Weak | 2.01 | 2.87 | 1.43 |
| 24 | 40 | F | Frontal | AA | III | New | Wild type | 18.5 | Ring/Solid | LEV | Moderate | 3.77 | 7.43 | 1.97 |
| 25 | 58 | M | Frontal | AA | III | New | Mutant | 5.2 | None/Slight | LEV | Strong | 1.87 | 3.99 | 2.13 |
| 26 | 33 | M | Insula | AA | III | Recurrent | Mutant | 21.3 | None/Slight | LEV | Strong | 2.84 | 5.4 | 1.9 |
| 27 | 33 | M | Insula | AA | III | Recurrent | Mutant | 15.2 | None/Slight | LEV | Strong | 3.04 | 7.23 | 2.38 |
| 28 | 43 | M | Frontal | AA | III | New | Mutant | 12.9 | None/Slight | LEV | Strong | 2.32 | 3.78 | 1.63 |
| 29 | 31 | M | Insula | DA | II | New | Mutant | 3.3 | None/Slight | LEV | None | 2.07 | 3.72 | 1.8 |
| 30 | 77 | F | Temporal | DA | II | New | Wild type | 1 | None/Slight | None | Moderate | 2.19 | 3.96 | 1.81 |
| 31 | 37 | F | Insula | DA | II | Recurrent | Mutant | 5.8 | None/Slight | LEV | Moderate | 1.52 | 2.47 | 1.63 |
| 32 | 42 | M | Temporal | DA | II | New | Mutant | 5.1 | None/Slight | LEV | None | 2.02 | 4.96 | 2.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, K.; Tamura, K.; Hara, S.; Inaji, M.; Tanaka, Y.; Kobayashi, D.; Sugawara, T.; Wakimoto, H.; Nariai, T.; Ishii, K.; et al. Correlation of Intraoperative 5-ALA-Induced Fluorescence Intensity and Preoperative 11C-Methionine PET Uptake in Glioma Surgery. Cancers 2022, 14, 1449. https://doi.org/10.3390/cancers14061449
Shimizu K, Tamura K, Hara S, Inaji M, Tanaka Y, Kobayashi D, Sugawara T, Wakimoto H, Nariai T, Ishii K, et al. Correlation of Intraoperative 5-ALA-Induced Fluorescence Intensity and Preoperative 11C-Methionine PET Uptake in Glioma Surgery. Cancers. 2022; 14(6):1449. https://doi.org/10.3390/cancers14061449
Chicago/Turabian StyleShimizu, Kazuhide, Kaoru Tamura, Shoko Hara, Motoki Inaji, Yoji Tanaka, Daisuke Kobayashi, Takashi Sugawara, Hiroaki Wakimoto, Tadashi Nariai, Kenji Ishii, and et al. 2022. "Correlation of Intraoperative 5-ALA-Induced Fluorescence Intensity and Preoperative 11C-Methionine PET Uptake in Glioma Surgery" Cancers 14, no. 6: 1449. https://doi.org/10.3390/cancers14061449
APA StyleShimizu, K., Tamura, K., Hara, S., Inaji, M., Tanaka, Y., Kobayashi, D., Sugawara, T., Wakimoto, H., Nariai, T., Ishii, K., Sakuma, I., & Maehara, T. (2022). Correlation of Intraoperative 5-ALA-Induced Fluorescence Intensity and Preoperative 11C-Methionine PET Uptake in Glioma Surgery. Cancers, 14(6), 1449. https://doi.org/10.3390/cancers14061449