
Machine Learning Applications for Differentiation of Glioma from Brain Metastasis—A Systematic Review

 ,
,  , , , ,
, , , ,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Database Search
2.2. Data Extraction and Aggregation
2.3. Descriptive Statistics and Performance Evaluation Metrics
2.4. Assessment of Quality of Reporting
2.5. Statistical Analysis
3. Results
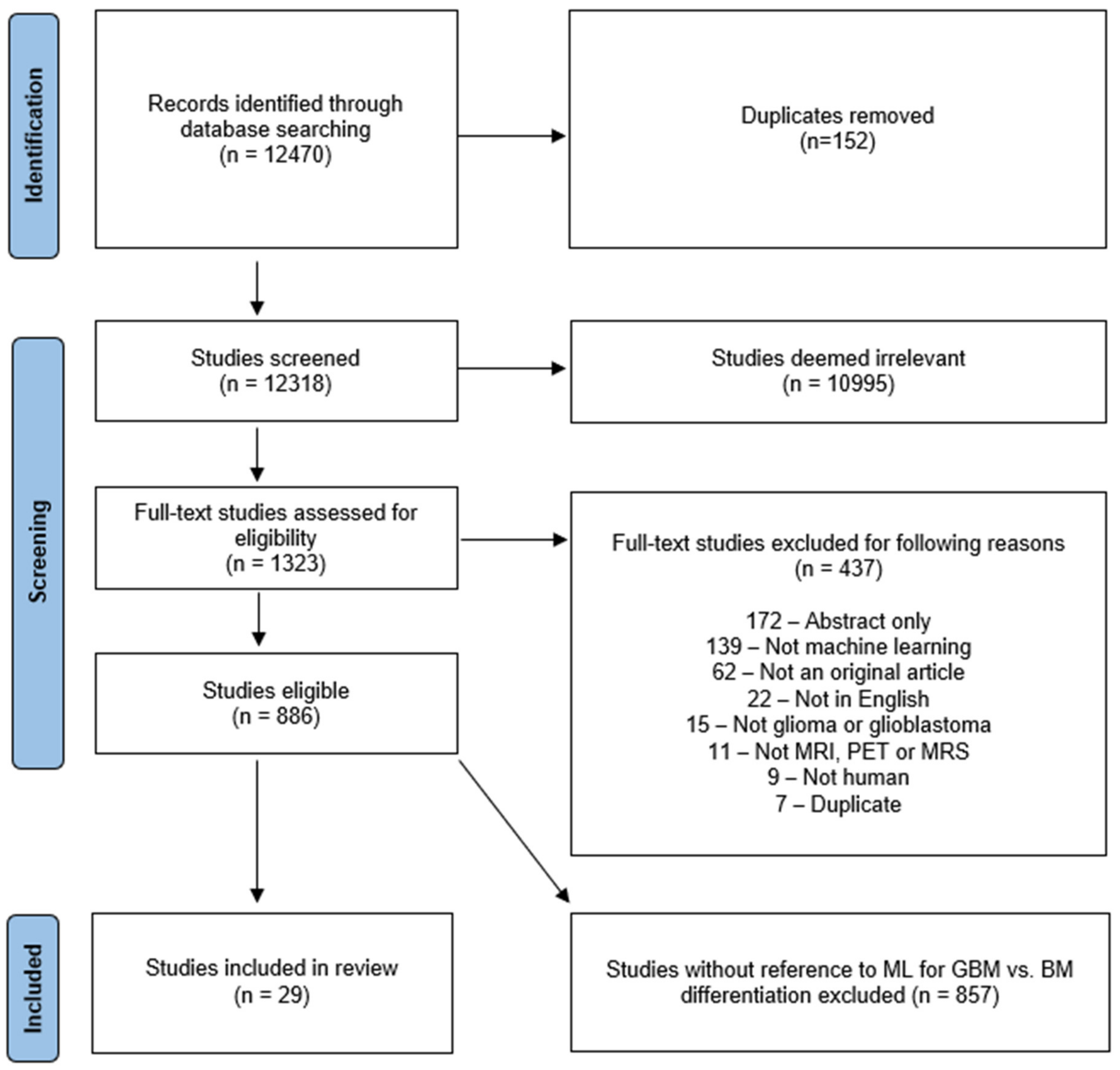
3.1. Study Selection
3.2. Study Characteristics
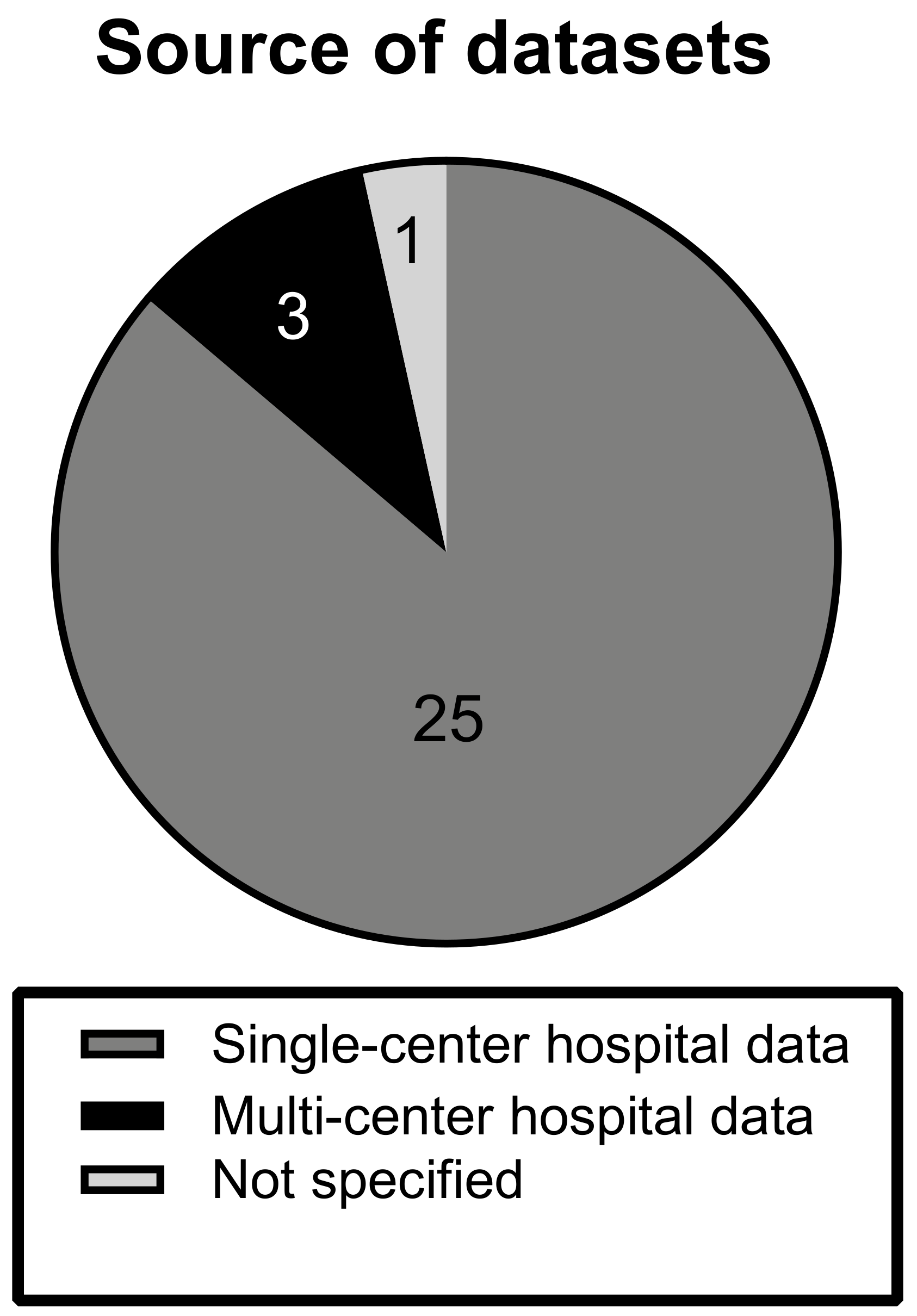
3.2.1. Datasets
3.2.2. Dataset Composition
3.2.3. Imaging Modalities and Features
3.2.4. Algorithms
3.2.5. Model Validation
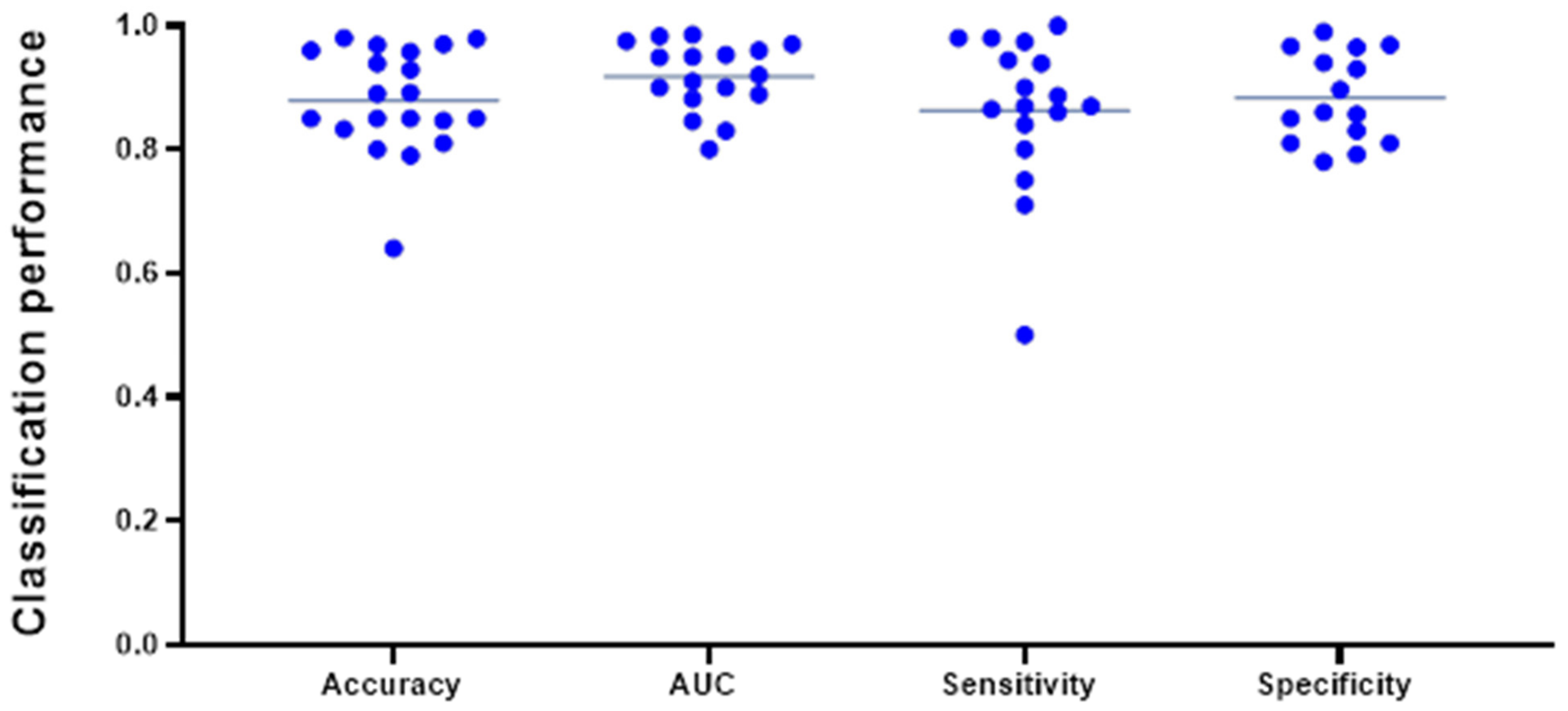
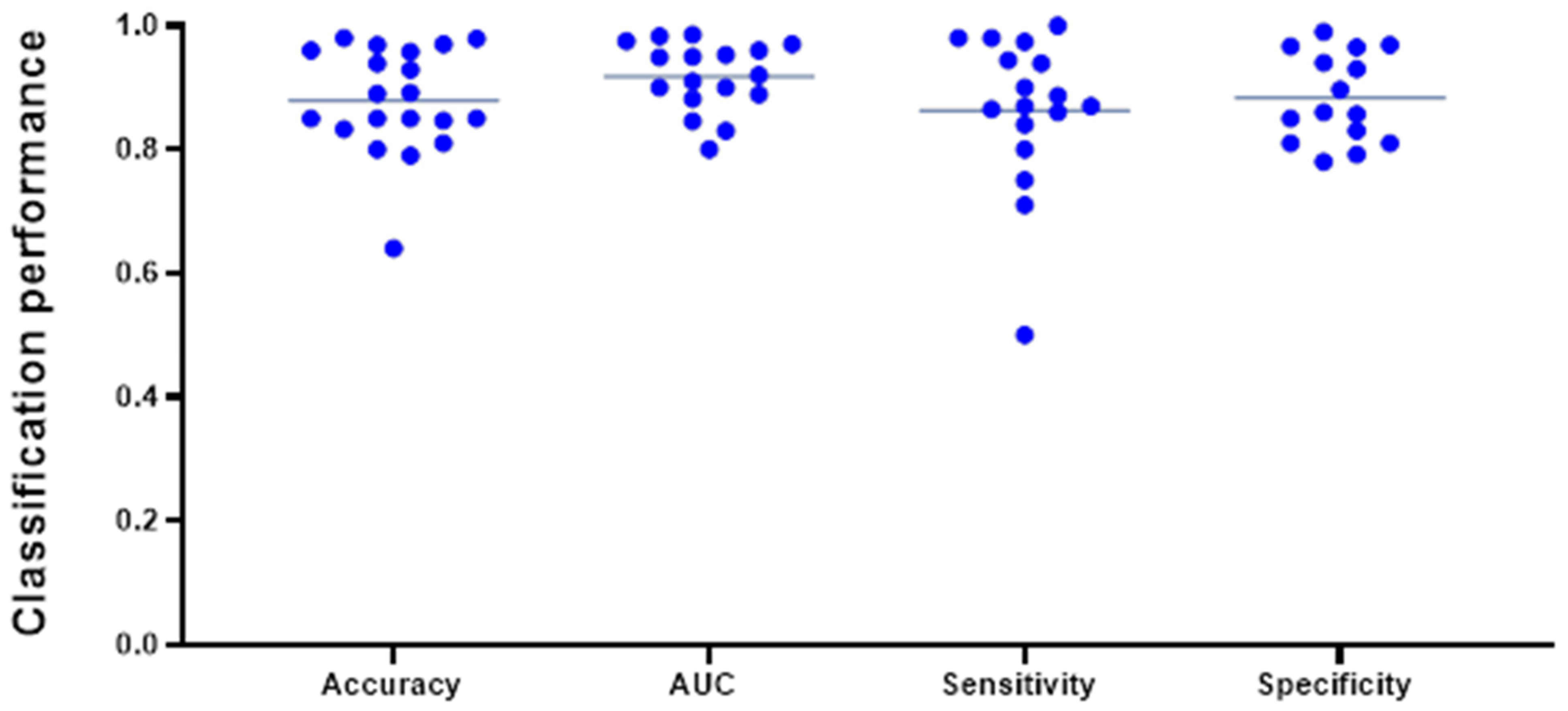
3.2.6. Classification Performance
3.3. Meta-Analysis
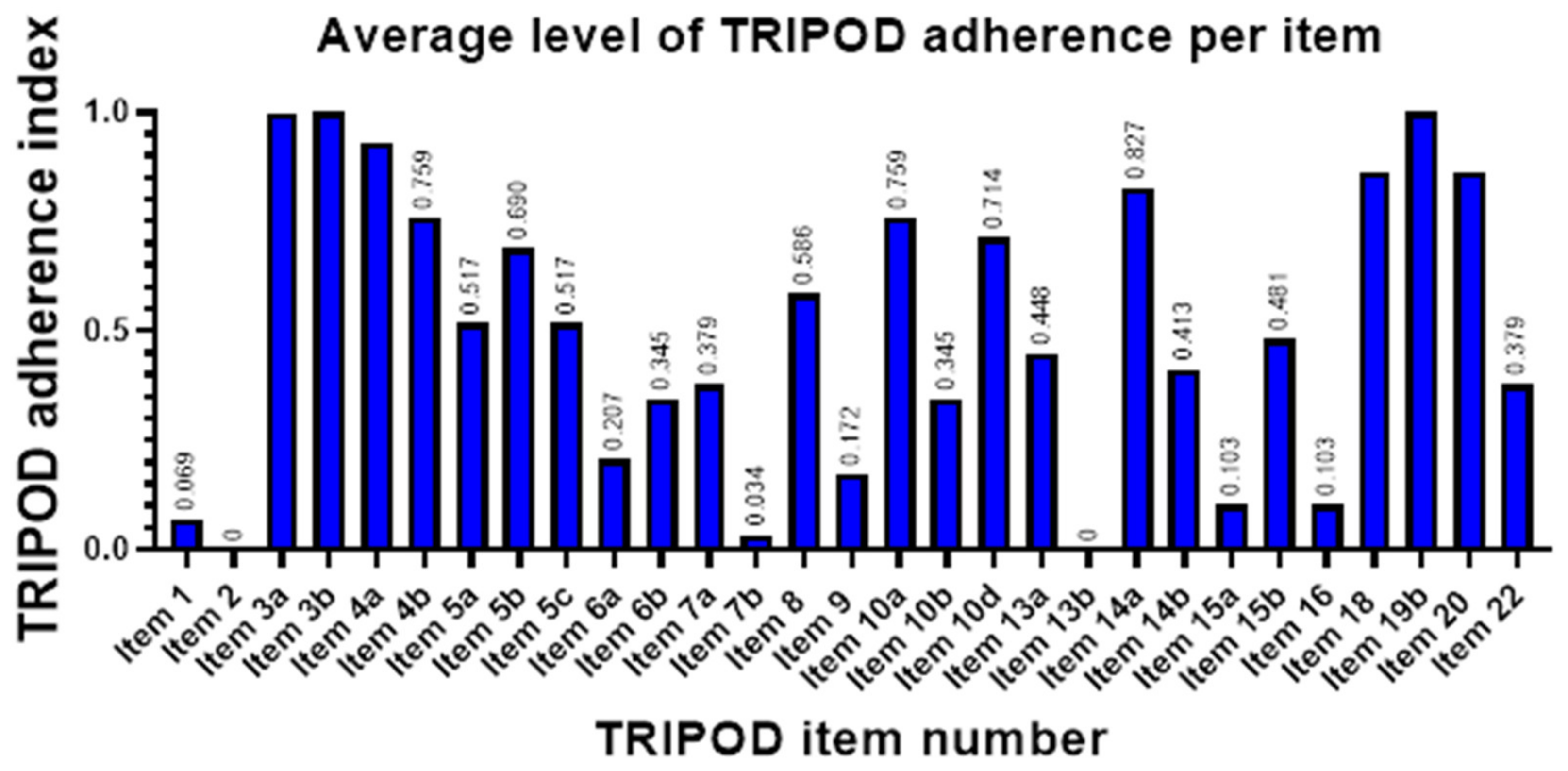
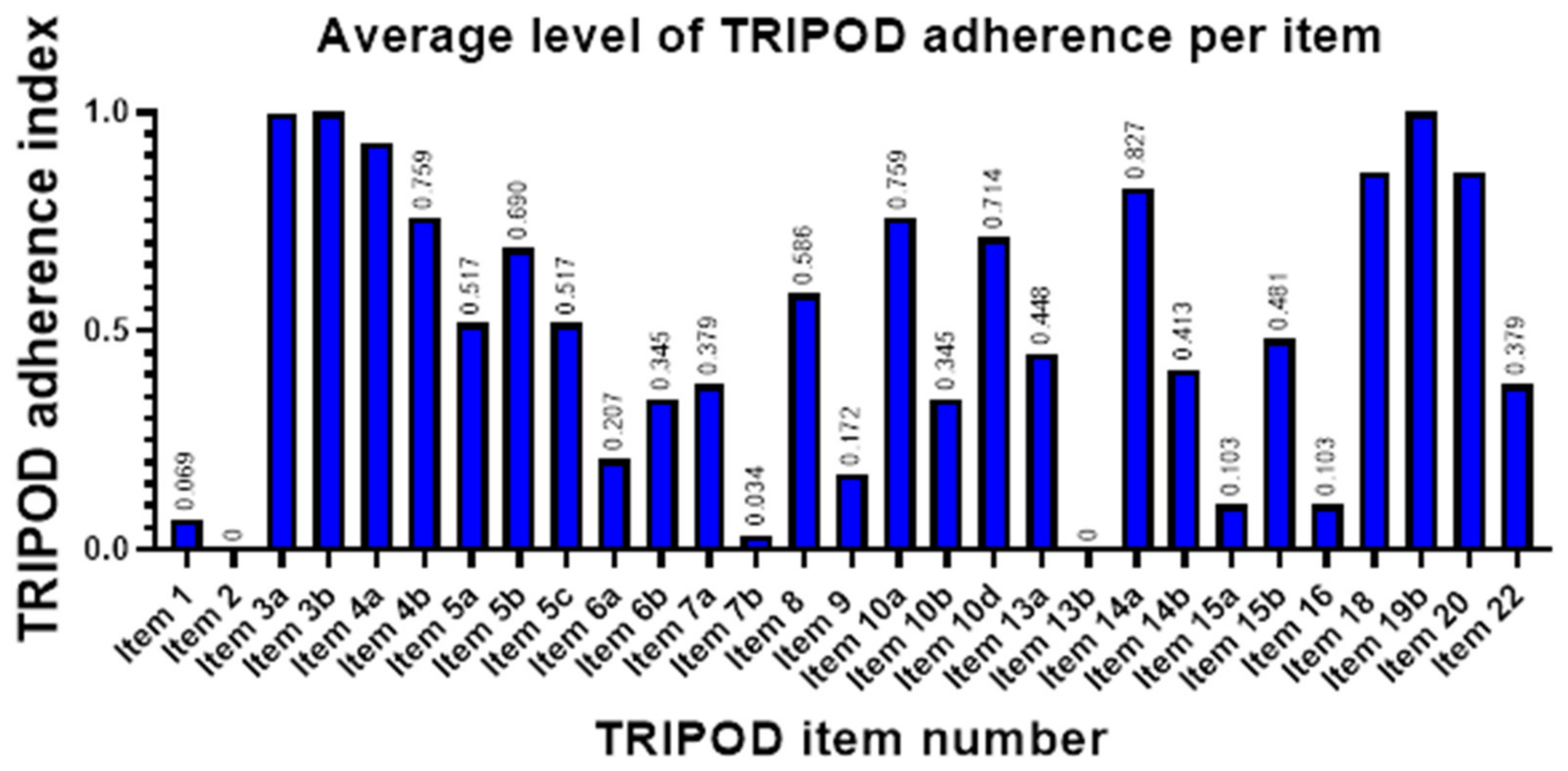
3.4. Quality of Reporting
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Farah, P.; Ondracek, A.; Chen, Y.; Wolinsky, Y.; Stroup, N.E.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006–2010. Neuro Oncol. 2013, 15 (Suppl. 2), ii1–ii56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cagney, D.N.; Martin, A.M.; Catalano, P.J.; Redig, A.J.; Lin, N.U.; Lee, E.Q.; Wen, P.Y.; Dunn, I.F.; Bi, W.L.; Weiss, S.E.; et al. Incidence and prognosis of patients with brain metastases at diagnosis of systemic malignancy: A population-based study. Neuro Oncol. 2017, 19, 1511–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rassy, E.; Zanaty, M.; Azoury, F.; Pavlidis, N. Advances in the management of brain metastases from cancer of unknown primary. Future Oncol. 2019, 15, 2759–2768. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Gittleman, H.; Stetson, L.; Virk, S.M.; Barnholtz-Sloan, J.S. Epidemiology of gliomas. Cancer Treat Res. 2015, 163, 1–14. [Google Scholar]
- Barajas, R.F., Jr.; Cha, S. Metastasis in Adult Brain Tumors. Neuroimaging Clin. N. Am. 2016, 26, 601–620. [Google Scholar] [CrossRef] [Green Version]
- Patchell, R.A.; Tibbs, P.A.; Walsh, J.W.; Dempsey, R.J.; Maruyama, Y.; Kryscio, R.J.; Markesbery, W.R.; Macdonald, J.S.; Young, B. A randomized trial of surgery in the treatment of single metastases to the brain. N. Engl. J. Med. 1990, 322, 494–500. [Google Scholar] [CrossRef]
- Schwartz, K.M.; Erickson, B.J.; Lucchinetti, C. Pattern of T2 hypointensity associated with ring-enhancing brain lesions can help to differentiate pathology. Neuroradiology 2006, 48, 143–149. [Google Scholar] [CrossRef]
- Choy, G.; Khalilzadeh, O.; Michalski, M.; Do, S.; Samir, A.E.; Pianykh, O.S.; Geis, J.R.; Pandharipande, P.V.; Brink, J.A.; Dreyer, K.J. Current Applications and Future Impact of Machine Learning in Radiology. Radiology 2018, 288, 318–328. [Google Scholar] [CrossRef]
- ACR Data Science Institute AI Central. Available online: https://aicentral.acrdsi.org (accessed on 17 January 2022).
- Ebrahimian, S.; Kalra, M.K.; Agarwal, S.; Bizzo, B.C.; Elkholy, M.; Wald, C.; Allen, B.; Dreyer, K.J. FDA-regulated AI algorithms: Trends, strengths, and gaps of validation studies. Acad. Radiol. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Lin, M. What’s Needed to Bridge the Gap Between US FDA Clearance and Real-world Use of AI Algorithms. Acad. Radiol. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Swinburne, N.C.; Schefflein, J.; Sakai, Y.; Oermann, E.K.; Titano, J.J.; Chen, I.; Tadayon, S.; Aggarwal, A.; Doshi, A.; Nael, K. Machine learning for semi-automated classification of glioblastoma, brain metastasis and central nervous system lymphoma using magnetic resonance advanced imaging. Ann. Transl. Med. 2019, 7, 232. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Kim, H.S.; Lee, J.; Cheong, E.N.; Shin, I.; Ahn, S.S.; Shim, W.H. Deep-learned time-signal intensity pattern analysis using an autoencoder captures magnetic resonance perfusion heterogeneity for brain tumor differentiation. Sci. Rep. 2020, 10, 21485. [Google Scholar] [CrossRef] [PubMed]
- Shrot, S.; Salhov, M.; Dvorski, N.; Konen, E.; Averbuch, A.; Hoffmann, C. Application of MR morphologic, diffusion tensor, and perfusion imaging in the classification of brain tumors using machine learning scheme. Neuroradiology 2019, 61, 757–765. [Google Scholar] [CrossRef]
- Yamashita, K.; Yoshiura, T.; Arimura, H.; Mihara, F.; Noguchi, T.; Hiwatashi, A.; Togao, O.; Yamashita, Y.; Shono, T.; Kumazawa, S.; et al. Performance evaluation of radiologists with artificial neural network for differential diagnosis of intra-axial cerebral tumors on MR images. AJNR Am. J. Neuroradiol. 2008, 29, 1153–1158. [Google Scholar] [CrossRef] [Green Version]
- Tateishi, M.; Nakaura, T.; Kitajima, M.; Uetani, H.; Nakagawa, M.; Inoue, T.; Kuroda, J.I.; Mukasa, A.; Yamashita, Y. An initial experience of machine learning based on multi-sequence texture parameters in magnetic resonance imaging to differentiate glioblastoma from brain metastases. J. Neurol. Sci. 2020, 410, 116514. [Google Scholar] [CrossRef]
- Tsolaki, E.; Svolos, P.; Kousi, E.; Kapsalaki, E.; Fountas, K.; Theodorou, K.; Tsougos, I. Automated differentiation of glioblastomas from intracranial metastases using 3T MR spectroscopic and perfusion data. Int. J. Comput. Assist. Radiol. Surg. 2013, 8, 751–761. [Google Scholar] [CrossRef]
- Yang, G.; Jones, T.L.; Barrick, T.R.; Howe, F.A. Discrimination between glioblastoma multiforme and solitary metastasis using morphological features derived from the p:q tensor decomposition of diffusion tensor imaging. NMR Biomed. 2014, 27, 1103–1111. [Google Scholar] [CrossRef]
- Abidin, A.Z.; Dar, I.; D’Souza, A.M.; Lin, E.P.; Wismüller, A. Investigating a quantitative radiomics approach for brain tumor classification. In Medical Imaging 2019: Biomedical Applications in Molecular, Structural, and Functional Imaging; International Society for Optics and Photonics: Bellingham, DC, USA, 2019. [Google Scholar]
- Georgiadis, P.; Cavouras, D.; Kalatzis, I.; Daskalakis, A.; Kagadis, G.C.; Sifaki, K.; Malamas, M.; Nikiforidis, G.; Solomou, E. Improving brain tumor characterization on MRI by probabilistic neural networks and non-linear transformation of textural features. Comput. Methods Programs Biomed. 2008, 89, 24–32. [Google Scholar] [CrossRef]
- Bae, S.; An, C.; Ahn, S.S.; Kim, H.; Han, K.; Kim, S.W.; Park, J.E.; Kim, H.S.; Lee, S.K. Robust performance of deep learning for distinguishing glioblastoma from single brain metastasis using radiomic features: Model development and validation. Sci. Rep. 2020, 10, 12110. [Google Scholar] [CrossRef]
- Artzi, M.; Bressler, I.; Bashat, D.B. Differentiation between glioblastoma, brain metastasis and subtypes using radiomics analysis. J. Magn. Reson. Imaging 2019, 50, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Jones, T.L.; Howe, F.A.; Barrick, T.R. Morphometric model for discrimination between glioblastoma multiforme and solitary metastasis using three-dimensional shape analysis. Magn. Reson. Med. 2016, 75, 2505–2516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, F.; Li, Q.; Jiang, B.; Zhu, X.; Zeng, Q.; Huang, P.; Chen, S.; Zhang, M. Differentiation of supratentorial single brain metastasis and glioblastoma by using peri-enhancing oedema region-derived radiomic features and multiple classifiers. Eur. Radiol. 2020, 30, 3015–3022. [Google Scholar] [CrossRef]
- Meier, R.; de Mortanges, A.P.; Wiest, R.; Knecht, U. Exploratory Analysis of Qualitative MR Imaging Features for the Differentiation of Glioblastoma and Brain Metastases. Front. Oncol. 2020, 10, 581037. [Google Scholar] [CrossRef]
- Zacharaki, E.I.; Wang, S.; Chawla, S.; Yoo, D.S.; Wolf, R.; Melhem, E.R.; Davatzikos, C. Classification of brain tumor type and grade using MRI texture and shape in a machine learning scheme. Magn. Reson. Med. 2009, 62, 1609–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsolaki, E.; Svolos, P.; Kousi, E.; Kapsalaki, E.; Fezoulidis, I.; Fountas, K.; Theodorou, K.; Kappas, C.; Tsougos, I. Fast spectroscopic multiple analysis (FASMA) for brain tumor classification: A clinical decision support system utilizing multi-parametric 3T MR data. Int. J. Comput. Assist. Radiol. Surg. 2015, 10, 1149–1166. [Google Scholar] [CrossRef] [PubMed]
- Zacharaki, E.I.; Kanas, V.G.; Davatzikos, C. Investigating machine learning techniques for MRI-based classification of brain neoplasms. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 821–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svolos, P.; Tsolaki, E.; Kapsalaki, E.; Theodorou, K.; Fountas, K.; Fezoulidis, I.; Tsougos, I. Investigating brain tumor differentiation with diffusion and perfusion metrics at 3T MRI using pattern recognition techniques. Magn. Reson. Imaging 2013, 31, 1567–1577. [Google Scholar] [CrossRef]
- Sachdeva, J.; Kumar, V.; Gupta, I.; Khandelwal, N.; Ahuja, C.K. A package-SFERCB-“Segmentation, feature extraction, reduction and classification analysis by both SVM and ANN for brain tumors”. Appl. Soft Comput. 2016, 47, 151–167. [Google Scholar] [CrossRef]
- Payabvash, S.; Aboian, M.; Tihan, T.; Cha, S. Machine Learning Decision Tree Models for Differentiation of Posterior Fossa Tumors Using Diffusion Histogram Analysis and Structural MRI Findings. Front. Oncol. 2020, 10, 71. [Google Scholar] [CrossRef]
- Qin, J.; Li, Y.; Liang, D.; Zhang, Y.; Yao, W. Histogram analysis of absolute cerebral blood volume map can distinguish glioblastoma from solitary brain metastasis. Medicine 2019, 98, e17515. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Ou, X.; Wang, J.; Guo, W.; Ma, X. Radiomics-Based Machine Learning in Differentiation Between Glioblastoma and Metastatic Brain Tumors. Front. Oncol. 2019, 9, 806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Ramon, R.; Ruiz-Espana, S.; Molla-Olmos, E.; Moratal, D. Glioblastomas and brain metastases differentiation following an MRI texture analysis-based radiomics approach. Phys. Med. 2020, 76, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Shin, I.; Kim, H.; Ahn, S.; Sohn, B.; Bae, S.; Park, J.; Kim, H.; Lee, S.-K. Development and Validation of a Deep Learning–Based Model to Distinguish Glioblastoma from Solitary Brain Metastasis Using Conventional MR Images. Am. J. Neuroradiol. 2021, 42, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Priya, S.; Liu, Y.; Ward, C.; Le, N.H.; Soni, N.; Maheshwarappa, R.P.; Monga, V.; Zhang, H.; Sonka, M.; Bathla, G. Machine learning based differentiation of glioblastoma from brain metastasis using MRI derived radiomics. Sci. Rep. 2021, 11, 10478. [Google Scholar] [CrossRef]
- De Causans, A.; Carré, A.; Roux, A.; Tauziède-Espariat, A.; Ammari, S.; Dezamis, E.; Dhermain, F.; Reuzé, S.; Deutsch, E.; Oppenheim, C. Development of a machine learning classifier based on radiomic features extracted from post-contrast 3D T1-weighted MR images to distinguish glioblastoma from solitary brain metastasis. Front. Oncol. 2021, 11, 638262. [Google Scholar] [CrossRef]
- Liu, Z.; Jiang, Z.; Meng, L.; Yang, J.; Liu, Y.; Zhang, Y.; Peng, H.; Li, J.; Xiao, G.; Zhang, Z. Handcrafted and Deep Learning-Based Radiomic Models Can Distinguish GBM from Brain Metastasis. J. Oncol. 2021, 2021, 5518717. [Google Scholar] [CrossRef]
- Samani, Z.R.; Parker, D.; Wolf, R.; Hodges, W.; Brem, S.; Verma, R. Distinct Tumor Signatures using Deep Learning-based Characterization of the Peritumoral Microenvironment in Glioblastomas and Brain Metastases. Sci. Rep. 2021, 11, 14469. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BMJ 2015, 350, g7594. [Google Scholar] [CrossRef] [Green Version]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Lewis, S.; Clarke, M. Forest plots: Trying to see the wood and the trees. BMJ 2001, 322, 1479–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisner, D.A.; Schnyer, D.M. Support vector machine. In Machine Learning; Elsevier: Amsterdam, The Netherlands, 2020; pp. 101–121. [Google Scholar]
- Ugga, L.; Perillo, T.; Cuocolo, R.; Stanzione, A.; Romeo, V.; Green, R.; Cantoni, V.; Brunetti, A. Meningioma MRI radiomics and machine learning: Systematic review, quality score assessment, and meta-analysis. Neuroradiology 2021, 63, 1293–1304. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.J.; Sunwoo, L.; Baik, S.H.; Bae, Y.J.; Choi, B.S.; Kim, J.H. Brain metastasis detection using machine learning: A systematic review and meta-analysis. Neuro. Oncol. 2021, 23, 214–225. [Google Scholar] [CrossRef] [PubMed]
- Zaharchuk, G.; Gong, E.; Wintermark, M.; Rubin, D.; Langlotz, C. Deep learning in neuroradiology. Am. J. Neuroradiol. 2018, 39, 1776–1784. [Google Scholar] [CrossRef] [Green Version]
- Abrol, A.; Fu, Z.; Salman, M.; Silva, R.; Du, Y.; Plis, S.; Calhoun, V. Deep learning encodes robust discriminative neuroimaging representations to outperform standard machine learning. Nat. Commun. 2021, 12, 353. [Google Scholar] [CrossRef]
- Peng, H.; Gong, W.; Beckmann, C.F.; Vedaldi, A.; Smith, S.M. Accurate brain age prediction with lightweight deep neural networks. Medical image analysis 2021, 68, 101871. [Google Scholar] [CrossRef]
- Chan, H.-P.; Samala, R.K.; Hadjiiski, L.M.; Zhou, C. Deep learning in medical image analysis. Adv. Exp. Med. Biol. 2020, 1213, 3–21. [Google Scholar]
- Valverde, J.M.; Imani, V.; Abdollahzadeh, A.; de Feo, R.; Prakash, M.; Ciszek, R.; Tohka, J. Transfer learning in magnetic resonance brain imaging: A systematic review. J. Imaging 2021, 7, 66. [Google Scholar] [CrossRef]
- McBee, M.P.; Awan, O.A.; Colucci, A.T.; Ghobadi, C.W.; Kadom, N.; Kansagra, A.P.; Tridandapani, S.; Auffermann, W.F. Deep Learning in Radiology. Acad. Radiol. 2018, 25, 1472–1480. [Google Scholar] [CrossRef] [Green Version]
- Ren, Y.; Zhang, L.; Suganthan, P.N. Ensemble classification and regression-recent developments, applications and future directions. IEEE Comput. Intell. Mag. 2016, 11, 41–53. [Google Scholar] [CrossRef]
- Sagi, O.; Rokach, L. Ensemble learning: A survey. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2018, 8, e1249. [Google Scholar] [CrossRef]
- Askaner, K.; Rydelius, A.; Engelholm, S.; Knutsson, L.; Lätt, J.; Abul-Kasim, K.; Sundgren, P. Differentiation between glioblastomas and brain metastases and regarding their primary site of malignancy using dynamic susceptibility contrast MRI at 3T. J. Neuroradiol. 2019, 46, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Suh, C.; Kim, H.; Jung, S.; Kim, S. Diffusion-weighted imaging and diffusion tensor imaging for differentiating high-grade glioma from solitary brain metastasis: A systematic review and meta-analysis. Am. J. Neuroradiol. 2018, 39, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Ahn, D.; Johnson, G.; Cha, S. Peritumoral diffusion tensor imaging of high-grade gliomas and metastatic brain tumors. Am. J. Neuroradiol. 2003, 24, 937–941. [Google Scholar] [PubMed]
- Xu, J.; Glicksberg, B.S.; Su, C.; Walker, P.; Bian, J.; Wang, F. Federated learning for healthcare informatics. J. Healthc. Inform. Res. 2021, 5, 1–19. [Google Scholar] [CrossRef]
- Wichmann, J.L.; Willemink, M.J.; de Cecco, C.N. Artificial Intelligence and Machine Learning in Radiology: Current State and Considerations for Routine Clinical Implementation. Invest. Radiol. 2020, 55, 619–627. [Google Scholar] [CrossRef]
- Althnian, A.; AlSaeed, D.; Al-Baity, H.; Samha, A.; Dris, A.B.; Alzakari, N.; Elwafa, A.A.; Kurdi, H. Impact of Dataset Size on Classification Performance: An Empirical Evaluation in the Medical Domain. Appl. Sci. 2021, 11, 796. [Google Scholar] [CrossRef]
- Balki, I.; Amirabadi, A.; Levman, J.; Martel, A.L.; Emersic, Z.; Meden, B.; Garcia-Pedrero, A.; Ramirez, S.C.; Kong, D.; Moody, A.R. Sample-size determination methodologies for machine learning in medical imaging research: A systematic review. Can. Assoc. Radiol. J. 2019, 70, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Plis, S.M.; Sarwate, A.D.; Wood, D.; Dieringer, C.; Landis, D.; Reed, C.; Panta, S.R.; Turner, J.A.; Shoemaker, J.M.; Carter, K.W. COINSTAC: A privacy enabled model and prototype for leveraging and processing decentralized brain imaging data. Front. Neurosci. 2016, 10, 365. [Google Scholar] [CrossRef] [Green Version]
- Rieke, N.; Hancox, J.; Li, W.; Milletari, F.; Roth, H.R.; Albarqouni, S.; Bakas, S.; Galtier, M.N.; Landman, B.A.; Maier-Hein, K. The future of digital health with federated learning. NPJ Digit. Med. 2020, 3, 119. [Google Scholar] [CrossRef] [PubMed]
- Sheller, M.J.; Edwards, B.; Reina, G.A.; Martin, J.; Pati, S.; Kotrotsou, A.; Milchenko, M.; Xu, W.; Marcus, D.; Colen, R.R. Federated learning in medicine: Facilitating multi-institutional collaborations without sharing patient data. Sci. Rep. 2020, 10, 12598. [Google Scholar] [CrossRef] [PubMed]
- Blanchet, L.; Krooshof, P.; Postma, G.; Idema, A.; Goraj, B.; Heerschap, A.; Buydens, L. Discrimination between metastasis and glioblastoma multiforme based on morphometric analysis of MR images. Am. J. Neuroradiol. 2011, 32, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branco, P.; Torgo, L.; Ribeiro, R. A survey of predictive modelling under imbalanced distributions. arXiv 2015, arXiv:1505.01658. [Google Scholar]
- Noorhalim, N.; Ali, A.; Shamsuddin, S.M. Handling imbalanced ratio for class imbalance problem using smote. In Proceedings of the Third International Conference on Computing, Mathematics and Statistics (iCMS2017), Langkawi, Malaysia, 7–8 November 2017. [Google Scholar]
- Dhiman, P.; Ma, J.; Navarro, C.A.; Speich, B.; Bullock, G.; Damen, J.A.; Kirtley, S.; Hooft, L.; Riley, R.D.; van Calster, B.; et al. Reporting of prognostic clinical prediction models based on machine learning methods in oncology needs to be improved. J. Clin. Epidemiol. 2021, 138, 60–72. [Google Scholar] [CrossRef]
- Mongan, J.; Moy, L.; Kahn, C.E., Jr. Checklist for Artificial Intelligence in Medical Imaging (CLAIM): A Guide for Authors and Reviewers. Radiol. Artif. Intell. 2020, 2, e200029. [Google Scholar] [CrossRef] [Green Version]
- Collins, G.S.; Dhiman, P.; Navarro, C.L.A.; Ma, J.; Hooft, L.; Reitsma, J.B.; Logullo, P.; Beam, A.L.; Peng, L.; van Calster, B.; et al. Protocol for development of a reporting guideline (TRIPOD-AI) and risk of bias tool (PROBAST-AI) for diagnostic and prognostic prediction model studies based on artificial intelligence. BMJ Open 2021, 11, e048008. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Paper | Total Patient Number | Number of Glioma Patients | Number of BM Patients | Ratio of Glioma/met Patients | Solitary BM Only | GBM Only | Tumor Types Studied | Number of Additional Tumors | Number of Patients (Training) | Number of Patients (Validation) | Testing | External Validation | Source of Data | ML Method | Algorithms Used for Classification | Gold Standard for Accuracy | Extracted Feature Types | Best Performing Classifier |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Swinburne et al., 2019 [13] | 26 | 9 | 9 | 1.000 | no | yes | GBM vs. MET vs. PCNSL | 8 (PCSNL) | LOOCV | no | single-center | ML | SVM, MLP | Pathology | Perfusion | MLP (Ktrans on T1CE mask) Accuracy: 83.3% AUC: 0.83 | ||
| Park et al., 2020 [14] | 276 | 137 | 59 | 2.322 | no | yes | GBM vs. MET vs. PCNSL | 80 (PCSNL) | 216 (109 GBM, 58 PCNSL, 49 MET) | 60 (28 GBM, 22 CNSL, 10 MET) | no | multi-center | DL | CNN | Pathology | Perfusion (Temporal Patterns of Time-Signal Intensity Curves from DSC) | CNN (DSC, FLAIR, T1CE)—internally validated AUC: 0.95 Sensitivity: 0.9 Specificity: 0.857 | |
| Shrot et al., 2019 [15] | 141 | 41 | 38 | 1.079 | no | yes | GBM vs. MET vs. PCNSL vs. MEN | 12 (PCSNL), 50 (Meningioma) | LOOCV | no | single-center | ML | Decision tree (SVM) | Pathology | Morphology, Diffusion, Perfusion | Binary hierarchical tree with SVM classifier (T1, T1c, T2, FLAIR, DTI, DSC) Sensitivity: 0.974 Specificity: 0.969 | ||
| Yamashita et al., 2008 [16] | 126 | 95 | 19 | 5.000 | multiple | no | Glioma vs. MET vs. PCNSL | 12 (PCSNL) | LOOCV | no | not specified | ML | 3-layered NNW | Pathology | Clinical, Qualitative/Semantic imaging features | ANN AUC: 0.946 board-certified radiologists without ANN: Accuracy: 87.9% AUC: 0.923 Sensitivity: 0.808 Specificity: 0.903 board-certified radiologists with ANN: Accuracy: 91.5% AUC: 0.946 Sensitivity: 0.868 Specificity: 0.931 | ||
| Blanchet et al., 2011 [17] | 33 | 18 | 15 | 1.200 | solitaty | yes | GBM vs. MET | LOOCV | no | single-center | ML | k-means clustering | Pathology | Shape | k-means clustering (T1, T2) Accuracy: 93.9% | |||
| Tsolaki et al., 2013 [18] | 49 | 35 | 14 | 2.500 | solitary | yes | GBM vs. MET | 10-fold CV | no | single-center | ML | SVM, Naive Bayes, KNN | Pathology | Spectroscopy | SVM (MRS: NAA; rCBV)—peritumoral Accuracy: 98% Sensitivity: 0.98 Specificity: 0.99 SVM (MRS: NAA/Cr; rCBV)—intratumoral Accuracy: 95% Sensitivity: 0.94 Specificity: 0.95 | |||
| Yang et al., 2014 [19] | 48 | 30 | 18 | 1.667 | solitary | yes | GBM vs. MET | LOOCV | no | single-center | ML | QDA, NB, SVM, KNN, NNW (MLP architecture) | Pathology | Shape, Diffusion | Neural Network (DTI) Accuracy: 97.92% AUC: 0.975 Sensitivity: 100% Specificity: 96.55% | |||
| Tateishi et al., 2020 [20] | 127 | 73 | 53 | 1.377 | multiple, largest selected for classification | yes | GBM vs. MET | 5-fold CV | no | single-center | ML | SVM | Pathology, clinical history of path-proven primary cancer | Texture | SVM (T1CE, T2, ADC) AUC: 0.92 | |||
| Abidin et al., 2019 [21] | 52 | 35 | 17 | 2.059 | solitary | yes | GBM vs. MET | stratified 10-fold CV | no | single-center | ML | AdaBoost | Pathology | First-order statistics, Texture, Higher-order-features: Topology (Minkowski functionals), Wavelet-transformed, Local Binary Patterns (LBP) | AdaBoost (Local Binary Pattern, T1CE) AUC: 0.846 | |||
| Bae et al., 2020 [22] | 248 | 159 | 89 | 1.787 | solitary | yes | GBM vs. MET | 166 (109 GBM, 57 MET) | 82 (50 GBM, 32 MET) | yes | single-center | ML and DL | DNN, AdaBoost, (L-SVM, LDA) | Pathology | DL extracted (DL) Shape, First-order statistics, Texture (traditional ML) | Deep Neural Network (T1CE)—internal AUC: 0.986 Deep Neural Network (T1CE)—external AUC: 0.956 Accuracy: 89% Sensitivity: 0.906 pecificity: 0.88 | ||
| Artzi et al., 2019 [23] | 439 | 212 | 227 | 0.934 | solitary | yes | GBM vs. MET vs. MET-subtypes | 5-fold CV | no | single-center | ML | SVM, KNN, decision trees, ensemble classifiers | Pathology | Clinical features, Qualitative/semantic imaging features, Morphology, First-order statistics, Texture, Higher-order features: Wavelet features, Bagof-features | SVM (T1CE) Accuracy: 89% AUC: 0.96 Sensitivity: 0.86 Specificity: 0.85 | |||
| Yang et al., 2016 [24] | 48 | 30 | 18 | 1.667 | solitary | yes | GBM vs. MET | LOOCV | no | single-center | ML | SVM | Pathology | Shape | SVM (DTI, Cluster 1 & 4) Accuracy: 95.83% AUC: 0.983 Sensitivity: 0.9444 Specificity: 0.9667 | |||
| Dong et al., 2020 [25] | 120 | 60 | 60 | 1.000 | solitary | n/a | Glioma vs. MET | 84 (42 GBM, 42 MET) | 36 (18 GBM, 18 MET) | no | single-center | ML | NNW, DT, NB, KNN, SVM | Radiological | Shape, First-order statistics, Texture | Naive Bayes (T1, T1CE, T2) Accuracy: 60% Sensitivity: 0.45 Specificity: 0.75 Combined(LOG) [Decision Tree, SVM, NNW, kNN, NB] Accuracy: 64% Sensitivity: 0.5 Specificity: 0.73 Agreement of all 5 classifier: Accuracy: 94% Sensitivity: 1 Specificity: 0.89 | ||
| Meier et al., 2020 [26] | 109 | 25 | 84 | 0.298 | 231 lesions in 109 patients | yes | GBM vs. MET | stratified 3-fold CV | no | single-center | ML | SVM | Pathology | Qualitative/Semantic imaging features | SVM (Qualitative image features) F1-Score: 0.865 | |||
| Georgiadis et al., 2008 [27] | 67 | 21 | 19 | 1.105 | no | no | Glioma vs. MET vs. MEN | 27 (Meningioma) | external cross-validation (ECV) with 3-fold split | no | single-center | ML | PNN, LSFT-PNN, SVM-RBF, ANN, Cubic LSFT-PNN, Quardratic LSFT-PNN | Radiological | Texture | ANN (T1)—Primary tumors vs. Secondary tumors (MET + Meningioma) Accuracy: 100% | ||
| Tsolaki et al., 2015 [28] | 126 | 80 | 22 | 3.636 | solitary | no | Glioma vs. MET vs. MEN | 24 (Meningioma) | 10-fold cross validation | no | single-center | ML | SVM, Naïve Bayes, k-NN, LDA | Pathology | Spectroscopy, Diffusion, Perfusion | SVM (DWI/DTI/PWI/short TE)—peritumoral Accuracy: 98% SVM (DWI/DTI/PWI/short TE)—intratumoral Accuracy: 96% | ||
| Zacharaki et al., 2009 [27] | 98 | 74 | 24 | 3.083 | no | no | Glioma vs. MET vs. MEN | 4 (Meningioma) | LOOCV | no | single-center | ML | SVM, k-NN, LDA | Pathology | Shape, First-order statistics, Texture | SVM (FLAIR, T2, T1ce, rCBV, T1) Accuracy: 84.7% AUC: 0.882 Sensitivity: 0.882 Specificity: 0.865 | ||
| Zacharaki et al., 2011 [29] | 97 | 73 | 23 | 3.174 | no | no | Glioma vs. MET vs. MEN | LOOCV | no | single-center | ML | VFI, KNN, Naive Bayes | Pathology | Clinical, Shape, First-order | kNN with wrapper evaluator Accuracy: 96.91% | |||
| Svolos et al., 2013 [30] | 115 | 73 | 18 | 4.056 | solitary | no | Glioma vs. MET vs. MEN | 24 (atypical Meningioma) | 10-fold cross validation | no | single-center | ML | SVM | Pathology | Diffusion, Perfusion | SVM (HGG Grade 4 vs. MET) (ADC, FA, rCBV)—peritumoral Accuracy: 96% Sensitivity: 0.98 Specificity: 0.94 | ||
| Sachdeva et al., 2016 [31] | 428 | 177 | 66 | 2.682 | no | no | Glioma vs. MET vs. MEN vs. MED | 97 (Meningioma), 88 (Medulloblastoma) | 40% training, 10% testing, 50% validation | 40% training, 10% testing, 50% validation | 40% training, 10% testing, 50% validation | no | public dataset (PGIMER and SPL datasets) | ML | GA, GA-SVM, GA-ANN | Radiological | First-order statistics, Texture | GA-ANN—no binary classification Accuracy: 94% (imputed) |
| Payabvash et al., 2020 [32] | 248 | 99 | 65 | 1.523 | no | no | Glioma vs. MET vs. MED vs. Hemangioblastoma vs. Ependymoma | Hemangioblastoma (n = 44), Ependymoma (n = 27), Medulloblastoma (n = 26). | 10-fold cross validaiton | no | single center | ML | NB, RF, NN, SVM | Pathology | Clinical (Age), Qualitative/Semantic imaging features, Diffusion | Random Forest—MET vs. All primary tumors Accuracy: 83% AUC: 0.82 Sensitivity: 55.6 Specificity: 92.6 PPV: 73.9 | ||
| Qin et al., 2019 [33] | 42 | 24 | 18 | 1.333 | solitary | yes | GBM vs. MET | 5-fold cross validation | no | single center | ML | Decision trees, LDA, LogReg, linear SVM, KNN | Pathology | First-order, Second-order (Energy) | kNN Accuracy: 92.9% | |||
| Chen et al., 2019 [34] | 134 | n/a | n/a | no | yes | GBM vs. MET | 80% | 20% | no | single center | ML | LDA, SVM, RF, KNN, Gaussian NB | Pathology | Texture | LogReg + Distance correlation Accuracy: 79% AUC: 0.8 Sensitivity: 0.8 Specificity: 0.71 | |||
| Ortiz-Ramón et al., 2020 [35] | 100 | 50 | 50 | 1.000 | no | yes | GBM vs. MET | nested cross-validation | no | single center | ML | random forest (RF), support vector machine (SVM) with linear kernel, k-nearest neighbors (KNN), naïve Bayes (NB) and multilayer perceptron (MLP) | Radiological | Texture | MLP Accuracy: 81% AUC: 0.91 Sensitivity: 0.91 Specificity: 0.8 | |||
| Shin et al., 2021 [36] | 741 | 482 | 259 | 1.861 | solitary | yes | GBM vs. MET | 450 | 48 | 100 | 143 | multi-center | DL | CNN (2D) | Pathology | DL extracted | CNN (2D; T1CE, T2)—internal Accuracy: 89% AUC: 0.889 Sensitivity: 0.939 Precision: 0.852 CNN—external Accuracy: 85.9% AUC: 0.835 Sensitivity: 0.889 Precision: 0.907 | |
| Priya et al., 2021 [37] | 120 | 60 | 60 | 1.000 | no | yes | GBM vs. MET | nested cross-validation | no | single center | ML | Linear (LASSO, Elastic Net) and logistic regression, NNW, SVM- MLP, RF, AdaBoost | Clinico-Radiological | Shape, First-order statistics, Texture | LASSO (T1, T1CE, T2, FLAIR, ADC) Accuracy: 89.2% AUC: 0.953 Sensitivity: 0.887 Specificity: 0.897 | |||
| de Causans et al., 2021 [38] | 180 | 92 | 88 | 1.045 | multiple, largest selected for classification | yes | GBM vs. MET | 143 (71 GBM, 72 BM) | nested cross-validation (10 repeated 5-fold CV) | 37 (21, 16) | no | multi-center | ML | LogReg (Yeo-Johnson scaling features) | Pathology | Shape, First-order statistics, Texture | LogReg (T1CE) Accuracy: 80% Sensitivity: 0.75 Specificity: 0.86 | |
| Liu et al., 2021 [39] | 268 | 140 | 128 | 1.094 | solitary | yes | GBM vs. MET | 208 (110 GBM, 98 BM) | 10-fold cross validation | 60 (30, 30) | no | single center | ML | RF, DT, LogReg, AdaBoost, Gaussian processing, SVM | Pathology | Shape, First-order statistics, Texture, Higher-order: Wavelet-transformed, Laplace of Gaussian | Random Forest (Boruta selection) (T1CE) Accuracy: 85% AUC: 0.97 Sensitivity: 0.84 Specificity: 0.93 | |
| Samani et al., 2021 [40] | 136 | 86 | 50 | 1.720 | no, 3 patients with multifocal metastasis | yes | GBM vs. MET | 108 (66 GBM, 40 BM) | 5-fold cross validation | 30 (20, 10) | no | single center | DL | 2D CNN | Pathology | Diffusion | CNN (2D, DTI, FW-VP map)—patch wise Accuracy: 85% AUC: 0.9 Sensitivity: 0.87 Specificity: 0.81 CNN—majority vote, subject-wise: Accuracy: 93% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jekel, L.; Brim, W.R.; von Reppert, M.; Staib, L.; Cassinelli Petersen, G.; Merkaj, S.; Subramanian, H.; Zeevi, T.; Payabvash, S.; Bousabarah, K.; et al. Machine Learning Applications for Differentiation of Glioma from Brain Metastasis—A Systematic Review. Cancers 2022, 14, 1369. https://doi.org/10.3390/cancers14061369
Jekel L, Brim WR, von Reppert M, Staib L, Cassinelli Petersen G, Merkaj S, Subramanian H, Zeevi T, Payabvash S, Bousabarah K, et al. Machine Learning Applications for Differentiation of Glioma from Brain Metastasis—A Systematic Review. Cancers. 2022; 14(6):1369. https://doi.org/10.3390/cancers14061369
Chicago/Turabian StyleJekel, Leon, Waverly R. Brim, Marc von Reppert, Lawrence Staib, Gabriel Cassinelli Petersen, Sara Merkaj, Harry Subramanian, Tal Zeevi, Seyedmehdi Payabvash, Khaled Bousabarah, and et al. 2022. "Machine Learning Applications for Differentiation of Glioma from Brain Metastasis—A Systematic Review" Cancers 14, no. 6: 1369. https://doi.org/10.3390/cancers14061369
APA StyleJekel, L., Brim, W. R., von Reppert, M., Staib, L., Cassinelli Petersen, G., Merkaj, S., Subramanian, H., Zeevi, T., Payabvash, S., Bousabarah, K., Lin, M., Cui, J., Brackett, A., Mahajan, A., Omuro, A., Johnson, M. H., Chiang, V. L., Malhotra, A., Scheffler, B., & Aboian, M. S. (2022). Machine Learning Applications for Differentiation of Glioma from Brain Metastasis—A Systematic Review. Cancers, 14(6), 1369. https://doi.org/10.3390/cancers14061369