
Comparison of Active Surveillance to Stereotactic Radiosurgery for the Management of Patients with an Incidental Frontobasal Meningioma—A Sub-Analysis of the IMPASSE Study

 , , , ,
, , , ,  ,
,  , , add
Show full author list
, , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Study Procedures
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Unmatched Population and Meningioma Characteristics
3.2. Matched Population and Meningioma Characteristics
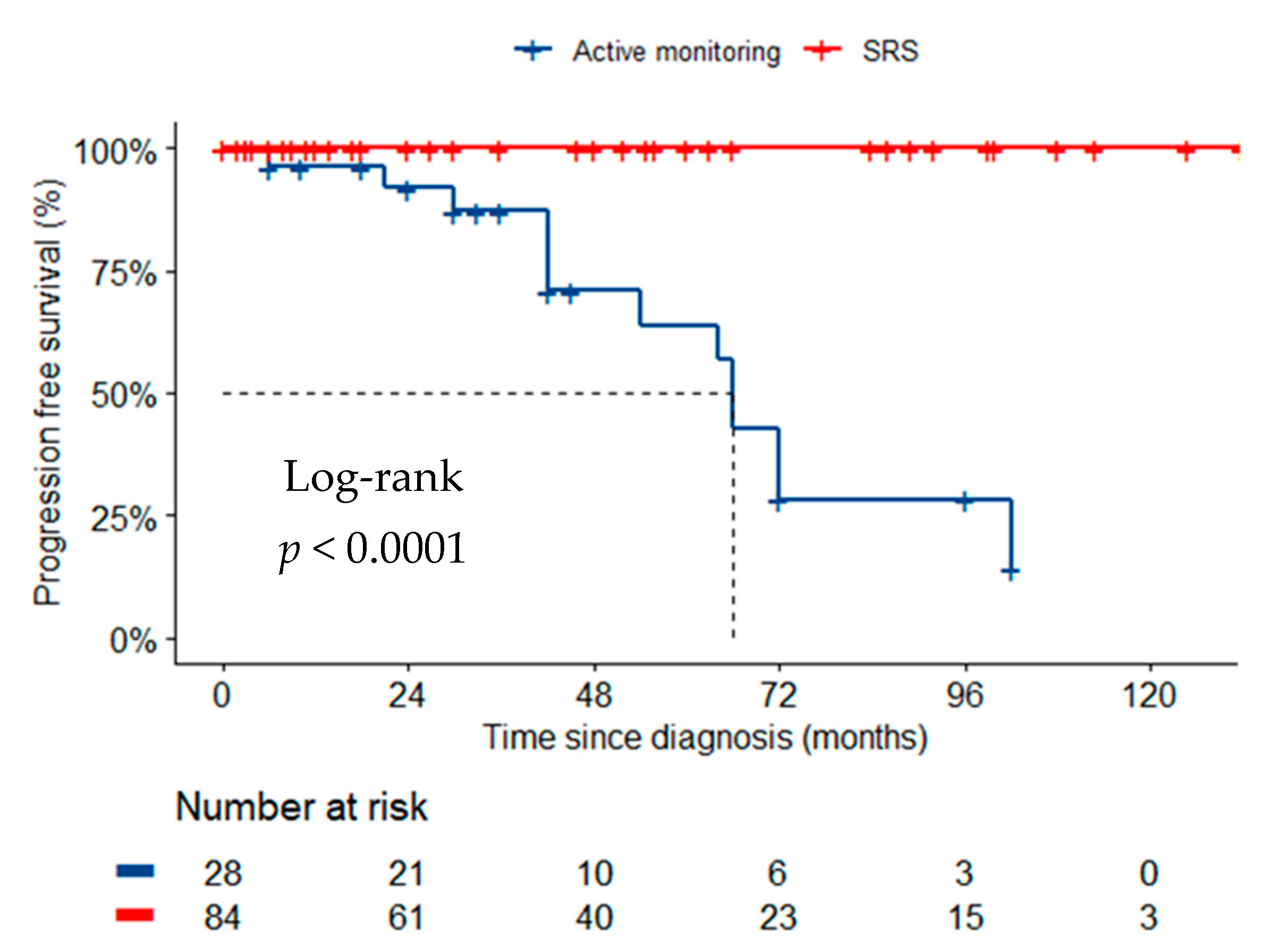
3.3. Radiologic and Clinical Outcomes in the Unmatched Cohorts
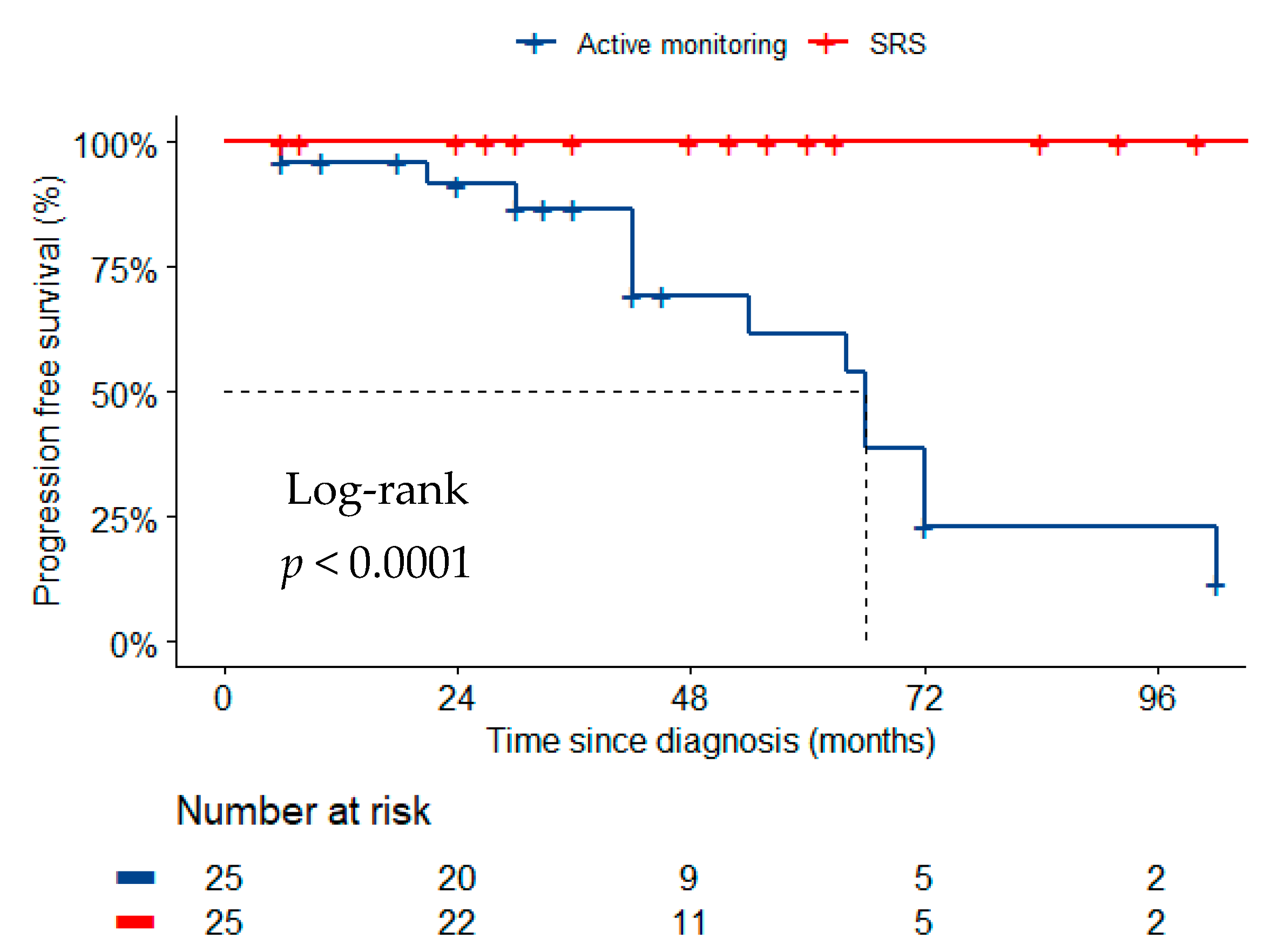
3.4. Radiological and Clinical Outcomes in the Matched Cohorts
3.5. Need for Surgery or Further Radiation Therapy
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morris, Z.; Whiteley, W.N.; Longstreth, W.T.; Weber, F.; Lee, Y.-C.; Tsushima, Y.; Alphs, H.; Ladd, S.C.; Warlow, C.; Wardlaw, J.M.; et al. Incidental findings on brain magnetic resonance imaging: Systematic review and meta-analysis. BMJ 2009, 339, b3016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bos, D.; Poels, M.M.F.; Adams, H.H.H.; Akoudad, S.; Cremers, L.G.M.; Zonneveld, H.I.; Hoogendam, Y.Y.; Verhaaren, B.; Verlinden, V.J.A.; Verbruggen, J.G.J.; et al. Prevalence, Clinical Management, and Natural Course of Incidental Findings on Brain MR Images: The Population-based Rotterdam Scan Study. Radiology 2016, 281, 507–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EANO Guideline on the Diagnosis and Management of Meningiomas|Neuro-Oncology|Oxford Academic. Available online: https://academic.oup.com/neuro-oncology/advance-article-abstract/doi/10.1093/neuonc/noab150/6310843?redirectedFrom=fulltext (accessed on 15 October 2021).
- Behbahani, M.; Skeie, G.O.; Eide, G.E.; Hausken, A.; Lund-Johansen, M.; Skeie, B.S. A prospective study of the natural history of incidental meningioma—Hold your horses! Neuro-Oncol. Pract. 2019, 6, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Brugada-Bellsolà, F.; Teixidor Rodríguez, P.; Rodríguez-Hernández, A.; Garcia-Armengol, R.; Tardáguila, M.; González-Crespo, A.; Domínguez, C.J.; Rimbau, J.M. Growth prediction in asymptomatic meningiomas: The utility of the AIMSS score. Acta Neurochir. 2019, 161, 2233–2240. [Google Scholar] [CrossRef] [PubMed]
- Islim, A.I.; Kolamunnage-Dona, R.; Mohan, M.; Moon, R.D.C.; Crofton, A.; Haylock, B.J.; Rathi, N.; Brodbelt, A.R.; Mills, S.J.; Jenkinson, M.D. A prognostic model to personalize monitoring regimes for patients with incidental asymptomatic meningiomas. Neuro-Oncology 2020, 22, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Clark, V.E.; Erson-Omay, E.Z.; Serin, A.; Yin, J.; Cotney, J.; Ozduman, K.; Avşar, T.; Li, J.; Murray, P.B.; Henegariu, O.; et al. Genomic analysis of non-NF2 meningiomas reveals mutations in TRAF7, KLF4, AKT1, and SMO. Science 2013, 339, 1077–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meling, T.R.; Da Broi, M.; Scheie, D.; Helseth, E. Meningiomas: Skull base versus non-skull base. Neurosurg. Rev. 2019, 42, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Islim, A.I.; Mohan, M.; Moon, R.D.C.; Srikandarajah, N.; Mills, S.J.; Brodbelt, A.R.; Jenkinson, M.D. Incidental intracranial meningiomas: A systematic review and meta-analysis of prognostic factors and outcomes. J. Neurooncol. 2019, 142, 211–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinzi, V.; Biagioli, E.; Roberto, A.; Galli, F.; Rizzi, M.; Chiappa, F.; Brenna, G.; Fariselli, L.; Floriani, I. Radiosurgery for intracranial meningiomas: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2017, 113, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, J.P.; Starke, R.M.; Kano, H.; Kaufmann, A.M.; Mathieu, D.; Zeiler, F.A.; West, M.; Chao, S.T.; Varma, G.; Chiang, V.L.S.; et al. Gamma Knife radiosurgery for sellar and parasellar meningiomas: A multicenter study: Clinical article. J. Neurosurg. 2014, 120, 1268–1277. [Google Scholar] [CrossRef] [PubMed]
- Gande, A.; Kano, H.; Bowden, G.; Mousavi, S.H.; Niranjan, A.; Flickinger, J.C.; Lunsford, L.D. Gamma Knife radiosurgery of olfactory groove meningiomas provides a method to preserve subjective olfactory function. J. Neurooncol. 2014, 116, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, J.; Pikis, S.; Islim, A.I.; Chen, C.-J.; Bunevicius, A.; Peker, S.; Samanci, Y.; Nabeel, A.M.; Reda, W.A.; Tawadros, S.R.; et al. An International Multicenter Matched Cohort Analysis of Incidental Meningioma Progression during Active Surveillance or after Stereotactic Radiosurgery: The IMPASSE Study. Neuro-Oncology 2021, 24, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Proposed Response Assessment and Endpoints for Meningioma Clinical Trials: Report from the Response Assessment in Neuro-Oncology Working Group|Neuro-Oncology|Oxford Academic. Available online: https://academic.oup.com/neuro-oncology/article/21/1/26/5076187 (accessed on 15 October 2021).
- Yao, X.; Wei, T.; Zhang, H.; Li, J.; Tang, A.; Ren, K. The Natural Growth Rate of Skull Base Meningiomas Compared with Non-Skull Base Meningiomas. J. Craniofac. Surg. 2019, 30, 1231–1233. [Google Scholar] [CrossRef] [PubMed]
- Slower growth of skull base meningiomas compared with non–skull base meningiomas based on volumetric and biological studies in. J. Neurosurg. 2012, 116, 574–580. Available online: https://thejns.org/view/journals/j-neurosurg/116/3/article-p574.xml (accessed on 15 October 2021). [CrossRef] [PubMed] [Green Version]
- Kreßner, M.; Arlt, F.; Riepl, W.; Meixensberger, J. Prognostic factors of microsurgical treatment of intracranial meningiomas—A multivariate analysis. PLoS ONE 2018, 13, e0202520. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Baseline Characteristic | Total (n = 112) | SRS (n = 84) | Active Surveillance (n = 28) | p |
|---|---|---|---|---|
| Age (years), mean (SD) | 58.8 (12.8) | 57.6 (12.5) | 62.1 (13.3) | 0.113 |
| Sex, N (%) | 0.251 | |||
| Male | 27 (24.1) | 18 (21.4) | 9 (32.1) | |
| Female | 85 (75.9) | 66 (78.6) | 19 (67.9) | |
| KPS, median (IQR) | 90 (90–100) | 90 (90–100) | 95 (75–100) | 0.754 |
| Meningioma volume (cm3), median (IQR) | 2.0 (1.0–4.0) | 2.0 (1.0–4) | 1.7 (0.9–3.1) | 0.137 |
| Laterality, N (%) | 0.505 | |||
| Right | 29 (25.9) | 23 (27.4) | 6 (21.4) | |
| Left | 42 (37.5) | 30 (35.7) | 12 (42.9) | |
| Midline | 29 (25.9) | 19 (22.6) | 10 (35.7) | |
| Missing | 12 (10.7) | 12 (14.3) | 0 (0) |
| Baseline Characteristic | SRS (n = 25) | Active Surveillance (n = 25) | p |
|---|---|---|---|
| Age (years), mean (SD) | 59.7 (9.9) | 60.8 (11.3) | 0.702 |
| Sex, N (%) | 0.185 | ||
| Male | 4 (16.0) | 8 (32.0) | |
| Female | 21 (84.0) | 17 (68.0) | |
| KPS, median (IQR) | 90 (90–95) | 100 (80–100) | 0.405 |
| Meningioma volume (cm3), median (IQR) | 2.0 (1.0–5.5) | 1.7 (0.9–2.9) | 0.272 |
| Laterality, N (%) | 0.424 | ||
| Right | 7 (33.3) | 5 (20.0) | |
| Left | 9 (42.9) | 10 (40.0) | |
| Midline | 5 (23.8) | 10 (40.0) | |
| Missing | 4 (16.0) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islim, A.I.; Mantziaris, G.; Pikis, S.; Chen, C.-J.; Bunevicius, A.; Peker, S.; Samanci, Y.; Nabeel, A.M.; Reda, W.A.; Tawadros, S.R.; et al. Comparison of Active Surveillance to Stereotactic Radiosurgery for the Management of Patients with an Incidental Frontobasal Meningioma—A Sub-Analysis of the IMPASSE Study. Cancers 2022, 14, 1300. https://doi.org/10.3390/cancers14051300
Islim AI, Mantziaris G, Pikis S, Chen C-J, Bunevicius A, Peker S, Samanci Y, Nabeel AM, Reda WA, Tawadros SR, et al. Comparison of Active Surveillance to Stereotactic Radiosurgery for the Management of Patients with an Incidental Frontobasal Meningioma—A Sub-Analysis of the IMPASSE Study. Cancers. 2022; 14(5):1300. https://doi.org/10.3390/cancers14051300
Chicago/Turabian StyleIslim, Abdurrahman I., Georgios Mantziaris, Stylianos Pikis, Ching-Jen Chen, Adomas Bunevicius, Selçuk Peker, Yavuz Samanci, Ahmed M. Nabeel, Wael A. Reda, Sameh R. Tawadros, and et al. 2022. "Comparison of Active Surveillance to Stereotactic Radiosurgery for the Management of Patients with an Incidental Frontobasal Meningioma—A Sub-Analysis of the IMPASSE Study" Cancers 14, no. 5: 1300. https://doi.org/10.3390/cancers14051300
APA StyleIslim, A. I., Mantziaris, G., Pikis, S., Chen, C.-J., Bunevicius, A., Peker, S., Samanci, Y., Nabeel, A. M., Reda, W. A., Tawadros, S. R., El-Shehaby, A. M. N., Abdelkarim, K., Emad, R. M., Delabar, V., Mathieu, D., Lee, C.-C., Yang, H.-C., Liscak, R., May, J., ... Jenkinson, M. D. (2022). Comparison of Active Surveillance to Stereotactic Radiosurgery for the Management of Patients with an Incidental Frontobasal Meningioma—A Sub-Analysis of the IMPASSE Study. Cancers, 14(5), 1300. https://doi.org/10.3390/cancers14051300