
Is Timing of Steroid Exposure Prior to Immune Checkpoint Inhibitor Initiation Associated with Treatment Outcomes in Melanoma? A Population-Based Study

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
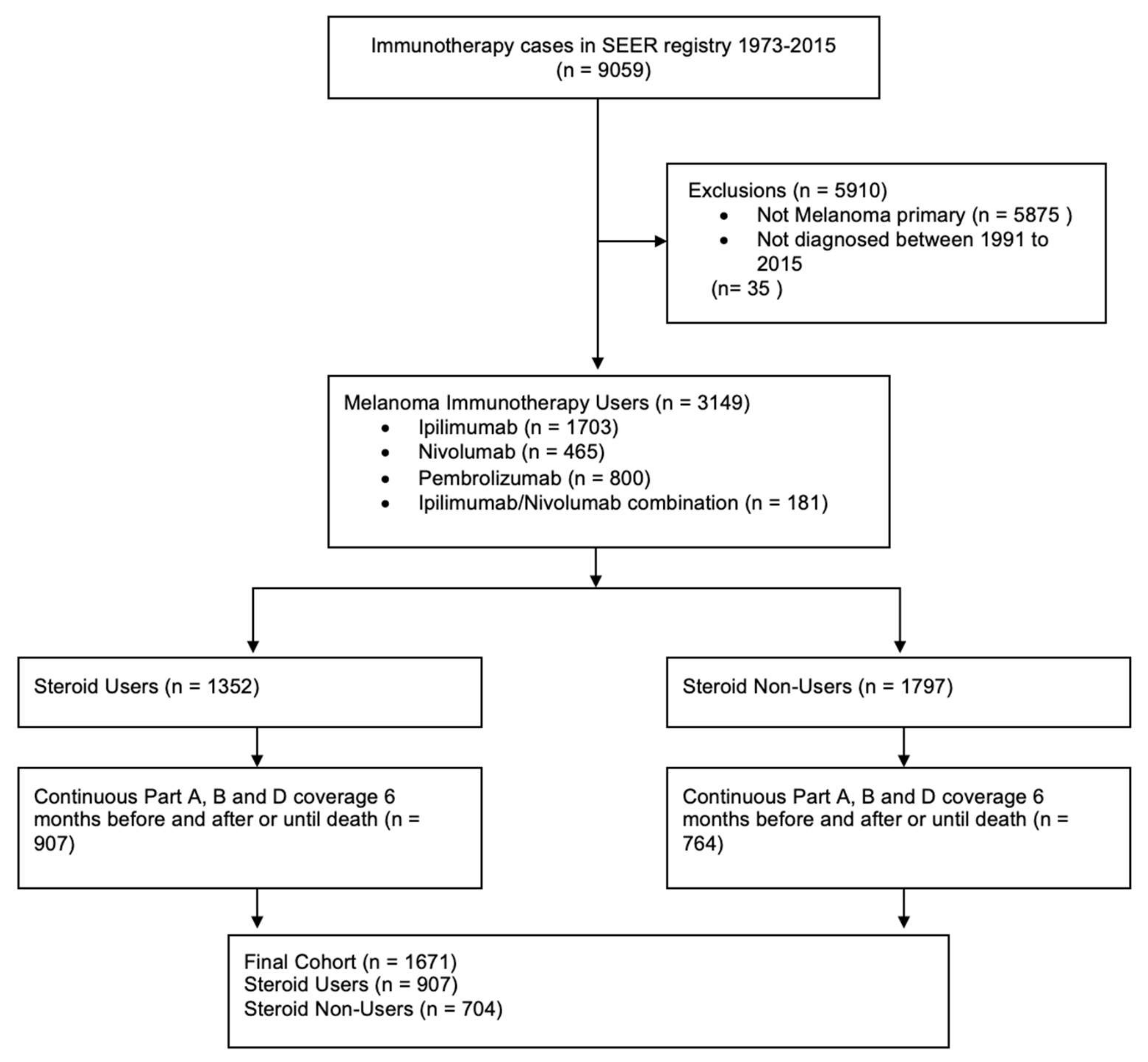
2. Materials and Methods
2.1. Data Source
2.2. Study Participants
2.3. Drug Exposures
2.4. Steroid-Exposure Timing
2.5. Endpoints
2.6. Descriptive Variables
2.7. Statistical Analysis
2.8. Modeling All-Cause Mortality (ACM)
2.9. Modeling Hospitalizations
2.10. Pre-Planned Evaluation of Unmeasured Confounding Effects
3. Results
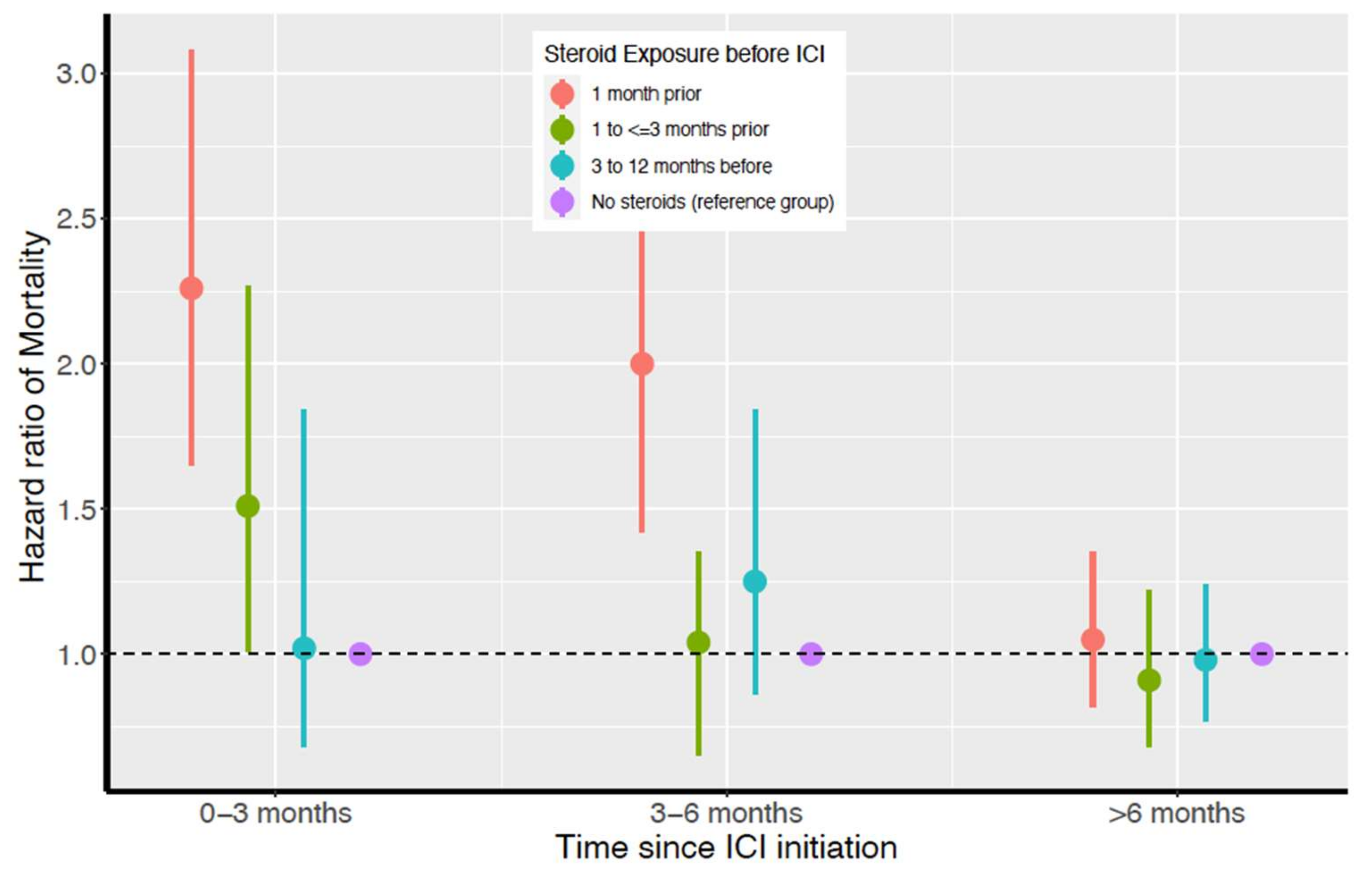
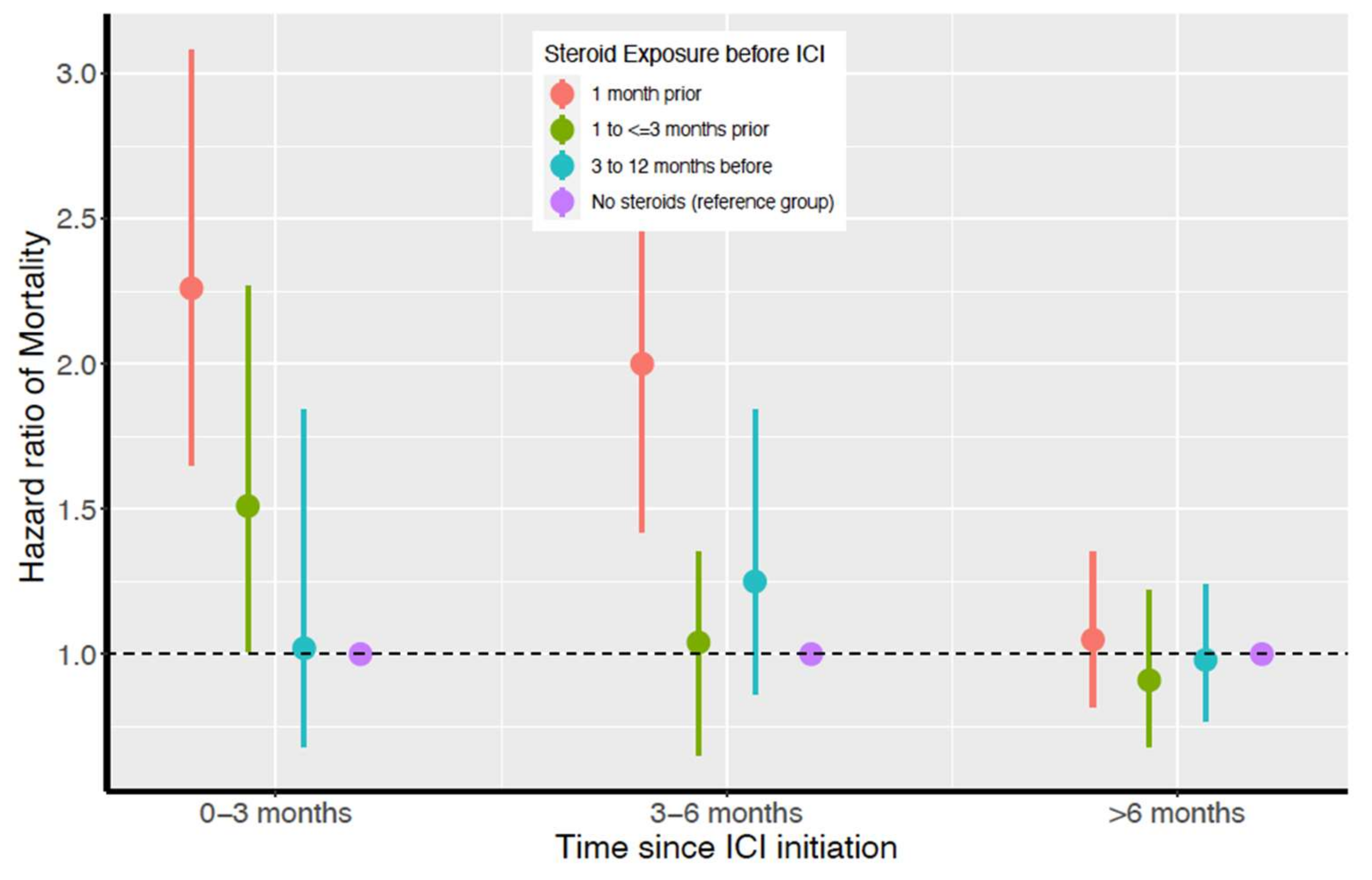
3.1. ACM and Steroid Exposure Prior to ICI Initiation
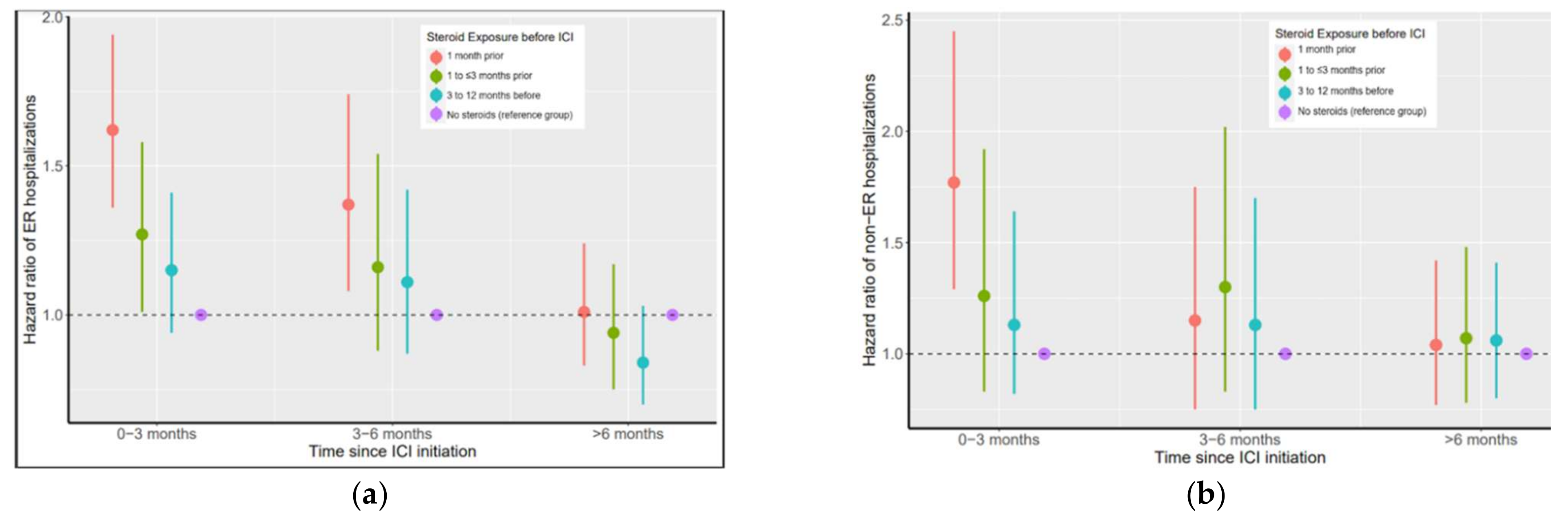
3.2. ER-Hospitalization Risk and Timing of Steroid Exposure before ICI initiation
3.3. Non-ER-Hospitalization Risk and Steroid Exposure before ICI Initiation
3.4. Pre-Planned Analysis to Evaluate Unmeasured Confounding
4. Discussion
4.1. Potential Mechanisms
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Bishop, K.; Kosary, C. SEER Cancer Statistics Review (CSR) 1975–2014. Available online: https://seer.cancer.gov/archive/csr/1975_2014/ (accessed on 2 September 2021).
- El Aziz, M.A.A.; Facciorusso, A.; Nayfeh, T.; Saadi, S.; Elnaggar, M.; Cotsoglou, C.; Sacco, R. Immune Checkpoint Inhibitors for Unresectable Hepatocellular Carcinoma. Vaccines 2020, 8, 616. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, E.D.; Drake, C.G.; Scher, H.I.; Fizazi, K.; Bossi, A.; Van den Eertwegh, A.J.M.; Krainer, M.; Houede, N.; Santos, R.; Mahammedi, H.; et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): A multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014, 15, 700–712. [Google Scholar] [CrossRef] [Green Version]
- Leighl, N.; Gandhi, L.; Hellmann, M.D.; Horn, L.; Ahn, M.-J.; Garon, E.B.; Hui, R.; Ramalingam, S.S.; Zhang, J.; Lubiniecki, G. Pembrolizumab for NSCLC: Immune-mediated adverse events and corticosteroid use. J. Thorac. Oncol. 2015, 10, S233. [Google Scholar]
- Coit, D.G.; Thompson, J.A.; Albertini, M.R.; Barker, C.; Carson, W.E. NCCN guidelines version 2.2019 cutaneous melanoma. J. Natl. Compr. Canc. Netw. 2019, 17, 367–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.-F.; Testori, A.; Grob, J.J.; et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef] [Green Version]
- Eggermont, A.M.M.; Blank, C.U.; Mandalà, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Lichinitser, M.; Khattak, A.; Carlino, M.S.; et al. Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma. N. Engl. J. Med. 2018, 378, 1789–1801. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.-A.; Reed, K.; et al. Nivolumab plus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune Checkpoint Blockade: A Common Denominator Approach to Cancer Therapy. Cancer Cell 2015, 27, 450–461. [Google Scholar] [CrossRef] [Green Version]
- Warner, A.B.; A Postow, M. Combination Controversies: Checkpoint Inhibition Alone or in Combination for the Treatment of Melanoma? Oncology 2018, 32, 228–234. [Google Scholar] [PubMed]
- Callahan, M.K.; Kluger, H.; Postow, M.A.; Segal, N.H.; Lesokhin, A.; Atkins, M.B.; Kirkwood, J.M.; Krishnan, S.; Bhore, R.; Horak, C.; et al. Nivolumab Plus Ipilimumab in Patients with Advanced Melanoma: Updated Survival, Response, and Safety Data in a Phase I Dose-Escalation Study. J. Clin. Oncol. 2018, 36, 391–398. [Google Scholar] [CrossRef]
- Coutinho, A.E.; Chapman, K.E. The anti-inflammatory and immunosuppressive effects of glucocorticoids, recent developments and mechanistic insights. Mol. Cell. Endocrinol. 2011, 335, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Lossignol, D. A little help from steroids in oncology. J. Transl. Intern. Med. 2016, 4, 52–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, J.; Rao, K.; Pastorino, S.; Kesari, S. Corticosteroids in brain cancer patients: Benefits and pitfalls. Expert Rev. Clin. Pharmacol. 2011, 4, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Yennurajalingam, S.; Bruera, E. Role of corticosteroids for fatigue in advanced incurable cancer: Is it a ‘wonder drug’ or ‘deal with the devil’. Curr. Opin. Support. Palliat. Care 2014, 8, 346–351. [Google Scholar] [CrossRef]
- Hardy, J.R.; Rees, E.; Ling, J.; Burman, R.; Feuer, D.; Broadley, K.; Stone, P. A prospective survey of the use of dexamethasone on a palliative care unit. Palliat. Med. 2001, 15, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Signorelli, D.; Ghidini, M.; Ghidini, A.; Pizzutilo, E.G.; Ruggieri, L.; Cabiddu, M.; Borgonovo, K.; Dognini, G.; Brighenti, M.; et al. Association of Steroids Use with Survival in Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Cancers 2020, 12, 546. [Google Scholar] [CrossRef] [Green Version]
- Schadendorf, D.; Hodi, F.S.; Robert, C.; Weber, J.; Margolin, K.; Hamid, O.; Patt, D.; Chen, T.-T.; Berman, D.M.; Wolchok, J.D. Pooled Analysis of Long-Term Survival Data from Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. J. Clin. Oncol. 2015, 33, 1889–1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajwa, R.; Cheema, A.; Khan, T.; Amirpour, A.; Paul, A.; Chaughtai, S.; Patel, S.; Patel, T.; Bramson, J.; Gupta, V.; et al. Adverse Effects of Immune Checkpoint Inhibitors (Programmed Death-1 Inhibitors and Cytotoxic T-Lymphocyte-Associated Protein-4 Inhibitors): Results of a Retrospective Study. J. Clin. Med. Res. 2019, 11, 225–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ksienski, D.; Wai, E.S.; Croteau, N.; Fiorino, L.; Brooks, E.; Poonja, Z.; Fenton, D.; Geller, G.; Glick, D.; Lesperance, M. Efficacy of Nivolumab and Pembrolizumab in Patients with Advanced Non–Small-Cell Lung Cancer Needing Treatment Interruption Because of Adverse Events: A Retrospective Multicenter Analysis. Clin. Lung Cancer 2018, 20, e97–e106. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.S.; Kähler, K.C.; Hauschild, A. Management of Immune-Related Adverse Events and Kinetics of Response with Ipilimumab. J. Clin. Oncol. 2012, 30, 2691–2697. [Google Scholar] [CrossRef]
- Langhoff, E.; Ladefoged, J.; Dickmeiss, E. The immunosuppressive potency of various steroids on peripheral blood lymphocytes, T cells, NK and K cells. Int. J. Immunopharmacol. 1985, 7, 483–489. [Google Scholar] [CrossRef]
- Arbour, K.C.; Mezquita, L.; Long, N.; Rizvi, H.; Auclin, E.; Ni, A.; Martínez-Bernal, G.; Ferrara, R.; Lai, W.V.; Hendriks, L.E.L.; et al. Impact of Baseline Steroids on Efficacy of Programmed Cell Death-1 and Programmed Death-Ligand 1 Blockade in Patients with Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 2872–2878. [Google Scholar] [CrossRef] [PubMed]
- Fucà, G.; Galli, G.; Poggi, M.; Russo, G.L.; Proto, C.; Imbimbo, M.; Ferrara, R.; Zilembo, N.; Ganzinelli, M.; Sica, A.; et al. Modulation of peripheral blood immune cells by early use of steroids and its association with clinical outcomes in patients with metastatic non-small cell lung cancer treated with immune checkpoint inhibitors. ESMO Open 2019, 4, e000457. [Google Scholar] [CrossRef] [Green Version]
- Surveillance, Epidemiology, and End Results (SEER) Program, SEER*Stat Databases: November 2019 Submission. Available online: www.seer.cancer.gov (accessed on 8 August 2020).
- Medicare Manuals General Information, Eligibility, Policy and Entitlement. Available online: https://www.cms.gov/regulations-and-guidance/guidance/manuals/downloads/ge101c03.pdf (accessed on 3 April 2021).
- Centers for Medicare & Medicaid Services (CMS), HHS, Medicaid Services Medicare Program; Medicare Prescription Drug Benefit. Available online: https://pubmed.ncbi.nlm.nih.gov/15678603/ (accessed on 23 March 2021).
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Regression models and life-tables. J. R. Stat. Soc. Series B Stat. Methodol. 1972, 34, 187–202. [Google Scholar] [CrossRef]
- Therneau, T.; Grambsch, P. Modeling Survival Data: Extending the Cox Model, 1st ed.; Springer: New York, NY, USA, 2000. [Google Scholar]
- Tsai, M.-H.; Xirasagar, S.; Carroll, S.; Bryan, C.S.; Gallagher, P.J.; Davis, K.; Jauch, E.C. Reducing High-Users’ Visits to the Emergency Department by a Primary Care Intervention for the Uninsured: A Retrospective Study. Inq. J. Heal. Care Organ. Prov. Financing 2018, 55, 29591539. [Google Scholar] [CrossRef]
- Andersen, P.K.; Gill, R.D. Cox’s regression model for counting processes: A large sample study. Ann. Stat. 1982, 10, 1100–1120. [Google Scholar] [CrossRef]
- Haneuse, S.; VanderWeele, T.J.; Arterburn, D. Using the E-Value to Assess the Potential Effect of Unmeasured Confounding in Observational Studies. JAMA 2019, 321, 602–603. [Google Scholar] [CrossRef] [PubMed]
- Drakaki, A.; Luhn, P.; Wakelee, H.; Dhillon, P.K.; Kent, M.; Shim, J.; Degaonkar, V.; Hoang, T.; McNally, V.; Chui, S.Y.; et al. 47O Association of systemic corticosteroids with overall survival in patients receiving cancer immunotherapy for advanced melanoma, non-small cell lung cancer or urothelial cancer in routine clinical practice. Ann. Oncol. 2019, 30, xi16–xi17. [Google Scholar] [CrossRef]
- Scott, S.C.; Pennell, N.A. Early Use of Systemic Corticosteroids in Patients with Advanced NSCLC Treated with Nivolumab. J. Thorac. Oncol. 2018, 13, 1771–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Im, S.J.; Hashimoto, M.; Gerner, M.Y.; Lee, J.; Kissick, H.T.; Burger, M.C.; Shan, Q.; Hale, J.S.; Lee, J.; Nasti, T.H.; et al. Defining CD8+ T cells that provide the proliferative burst after PD-1 therapy. Nature 2016, 537, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Xing, K.; Gu, B.; Zhang, P.; Wu, X. Dexamethasone enhances programmed cell death 1 (PD-1) expression during T cell activation: An insight into the optimum application of glucocorticoids in anti-cancer therapy. BMC Immunol. 2015, 16, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nivolumab in Treating Patients with Autoimmune Disorders and Advanced, Metastatic, or Unresectable Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03816345 (accessed on 8 August 2021).
- Nivolumab in Patients with Advanced Non-Small Cell Lung Cancer and Pre-Existing Autoimmune Disease. Available online: https://clinicaltrials.gov/ct2/show/NCT03656627 (accessed on 8 August 2021).



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Participants (N = 1671) | No Steroids (N = 807) | Steroids (N = 864) | p-Value |
|---|---|---|---|---|
| Sex | 0.088 | |||
| Male | 1189 (71.2) | 590 (73.1) | 599 (69.2) | |
| Female | 482 (28.9) | 217 (26.9) | 265 (30.7) | |
| Race | 0.702 | |||
| White | 1626 (97.3) | 784 (97.2) | 842 (97.5) | |
| Non-white | 45 (2.7) | 23 (2.9) | 22 (2.5) | |
| Marital status | 0.234 | |||
| Missing and unknown | 193 (11.6) | 86 (10.7) | 107 (12.4) | |
| Single (never married), Unmarried or domestic partner (same sex or opposite sex or unregistered) | 196 (11.7) | 97 (12.0) | 99 (11.5) | |
| Widowed, divorced, and separated | 254 (15.2) | 136 (16.9) | 118 (13.7) | |
| Married (including common law) | 1028 (61.5) | 488 (60.5) | 540 (62.5) | |
| Age at diagnosis, median (IQR) | 69 (63–75) | 69 (64–76) | 68 (63–74) | |
| Age at diagnosis | 0.009 | |||
| <60 | 244 (14.6) | 113 (14.0) | 131 (15.2) | |
| 60–69 | 648 (38.8) | 295 (36.6) | 353 (40.9) | |
| 70–79 | 583 (32.9) | 283 (35.1) | 300 (34.7) | |
| 80+ | 196 (11.7) | 116 (14.4) | 80 (9.3) | |
| Age at first ICI use, median (IQR) | 75 (70–81) | 75 (70–81) | 74 (69–80) | |
| Year of diagnosis | 0.554 | |||
| 1991–1999 | 107 (6.4) | 46 (6.0) | 61 (6.7) | |
| 2000–2005 | 278 (16.6) | 129 (16.9) | 149 (16.4) | |
| 2006–2010 | 470 (28.1) | 204 (26.7) | 266 (29.3) | |
| 2011–2015 | 816 (48.8) | 385 (50.4) | 431 (47.5) | |
| Sequence | 0.094 | |||
| Only | 807 (48.3) | 411 (50.9) | 396 (45.8) | |
| 1st | 691 (41.4) | 313 (38.8) | 378 (43.8) | |
| Subsequent (2nd–11th) | 173 (10.4) | 83 (10.3) | 90 (10.4) | |
| Charlson comorbidity index | 0.043 | |||
| 0 | 973 (58.2) | 495 (61.4) | 478 (55.4) | |
| 1 | 336 (20.1) | 152 (18.9) | 184 (21.3) | |
| ≥2 | 360 (21.5) | 159 (19.7) | 201 (23.2) | |
| SEER region | 0.185 | |||
| Northeast | 386 (23.1) | 196 (24.3) | 190 (21.6) | |
| South | 344 (20.6) | 150 (18.6) | 194 (22.5) | |
| North Central | 132 (7.9) | 69 (8.6) | 63 (7.3) | |
| West | 809 (49.4) | 392 (48.6) | 417 (48.3) | |
| State buy in 1 | 0.080 | |||
| Yes | 255(15.2) | 136 (16.9) | 119 (13.8) | |
| No | 1416 (84.7) | 671 (83.2) | 745 (86.2) | |
| Clinical T stage at diagnosis | 0.01 | |||
| T0 | 91 (5.5) | 32 (4.0) | 59 (6.8) | |
| T1 | 322 (19.3) | 165 (20.5) | 157 (18.2) | |
| T2 | 178 (10.7) | 79 (9.8) | 99 (11.5) | |
| T3 | 70 (4.2) | 36 (4.5) | 34 (3.9) | |
| T4 | 706 (42.3) | 362 (44.9) | 344 (49.1) | |
| TX | 284 (17.0) | 128 (15.9) | 156 (18.1) | |
| Clinical N stage at diagnosis | 0.675 | |||
| N0 | 964 (57.7) | 459 (55.9) | 505 (58.5) | |
| N1 | 210 (12.6) | 109 (13.5) | 101 (11.7) | |
| NX | 119 (7.12) | 59 (7.3) | 60 (6.9) | |
| missing | 377 (22.6) | 180 (22.3) | 197 (22.8) | |
| Clinical M stage at diagnosis | 0.432 | |||
| M0 | 1292 (77.3) | 631 (78.2) | 661 (76.5) | |
| All M1 | 153 (0.1) | 65 (0.1) | 88 (0.1) | |
| MX | 194 (11.6) | 91 (11.3) | 103 (11.9) | |
| Missing | 32 (1.9) | 20 (2.5) | 12 (1.4) | |
| Melanoma specific mortality as of 31 December 2016 | 0.712 | |||
| Dead | 398 (23.8) | 189 (22.4) | 209 (24.2) | |
| Alive | 1273 (76.2) | 618 (76.6) | 655 (75.8) | |
| All-cause mortality as of 31 December 2016 | 0.011 | |||
| Dead | 1031 (61.7) | 482 (59.7) | 549 (63.5) | |
| Alive | 640 (38.3) | 325 (40.3) | 315 (36.5) |
| Timing of Steroid Exposure Prior to ICI Initiation | 0 to ≤3 Months Post ICI Initiation Hazard Ratios 1 (95% CI) | 3 to ≤6 Months Post ICI Initiation Hazard Ratios (95% CI) | ≥6 Months Post ICI Initiation Hazard Ratios (95% CI) |
|---|---|---|---|
| No steroids in 12 months before ICI | Ref | Ref | Ref |
| Steroids ≤ 1 month prior to ICI | 2.26 (1.65–3.08) 2 | 2.00 (1.42–2.82) 2 | 1.05 (0.82–1.35) |
| Steroids 1 to ≤3 months prior to ICI | 1.51 (1.01–2.27) 2 | 1.04 (0.65–1.35) | 0.91 (0.68–1.22) |
| Steroids 3 to 12 months prior to ICI | 1.02 (0.68–1.52) | 1.25 (0.86–1.84) | 0.98 (0.77–1.24) |
| Timing of Steroid Exposure Prior to ICI Initiation | 0 to ≤3 Months Post ICI Initiation Hazard Ratios 1 (95% CI) | 3 to ≤6 Months Post ICI Initiation Hazard Ratios 1 (95% CI) | ≥6 Months Post ICI Initiation Hazard Ratios 1 (95% CI) |
|---|---|---|---|
| No steroids in 12 months before ICI | Ref | Ref | Ref |
| Steroids ≤1 month prior to ICI | 1.62 (1.36–1.94) 2 | 1.37 (1.08–1.74) 2 | 1.01 (0.83–1.24) |
| Steroids 1 to ≤3 months prior to ICI | 1.27 (1.01–1.58) 2 | 1.16 (0.88–1.54) | 0.94 (0.75–1.17) |
| Steroids 3 to 12 months prior to ICI | 1.15 (0.94–1.41) | 1.11 (0.87–1.42) | 0.84 (0.70–1.03) |
| Timing of Steroid Exposure Prior to ICI Initiation | 0 to ≤3 Months Post ICI Initiation Hazard Ratios | 3 to ≤6 Months Post ICI Initiation Hazard Ratios | ≥6 Months Post ICI initiation Hazard Ratios 1 |
|---|---|---|---|
| Steroids ≤ 1 month prior to ICI | 3.27 | 3.44 | 1.58 |
| Steroids 1 to ≤ 3 months prior to ICI | 2.82 | 1.77 | 1.49 |
| Steroids 3 to 12 months prior to ICI | 1.89 | 1.69 | 1.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikita, N.; Banks, J.; Keith, S.W.; Song, A.; Johnson, J.M.; Wilson, M.; Sharma, S.; Lu-Yao, G. Is Timing of Steroid Exposure Prior to Immune Checkpoint Inhibitor Initiation Associated with Treatment Outcomes in Melanoma? A Population-Based Study. Cancers 2022, 14, 1296. https://doi.org/10.3390/cancers14051296
Nikita N, Banks J, Keith SW, Song A, Johnson JM, Wilson M, Sharma S, Lu-Yao G. Is Timing of Steroid Exposure Prior to Immune Checkpoint Inhibitor Initiation Associated with Treatment Outcomes in Melanoma? A Population-Based Study. Cancers. 2022; 14(5):1296. https://doi.org/10.3390/cancers14051296
Chicago/Turabian StyleNikita, Nikita, Joshua Banks, Scott W. Keith, Andrew Song, Jennifer M. Johnson, Melissa Wilson, Swapnil Sharma, and Grace Lu-Yao. 2022. "Is Timing of Steroid Exposure Prior to Immune Checkpoint Inhibitor Initiation Associated with Treatment Outcomes in Melanoma? A Population-Based Study" Cancers 14, no. 5: 1296. https://doi.org/10.3390/cancers14051296
APA StyleNikita, N., Banks, J., Keith, S. W., Song, A., Johnson, J. M., Wilson, M., Sharma, S., & Lu-Yao, G. (2022). Is Timing of Steroid Exposure Prior to Immune Checkpoint Inhibitor Initiation Associated with Treatment Outcomes in Melanoma? A Population-Based Study. Cancers, 14(5), 1296. https://doi.org/10.3390/cancers14051296