
The Prognostic Role of Intratumoral Stromal Content in Lobular Breast Cancer

 ,
,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
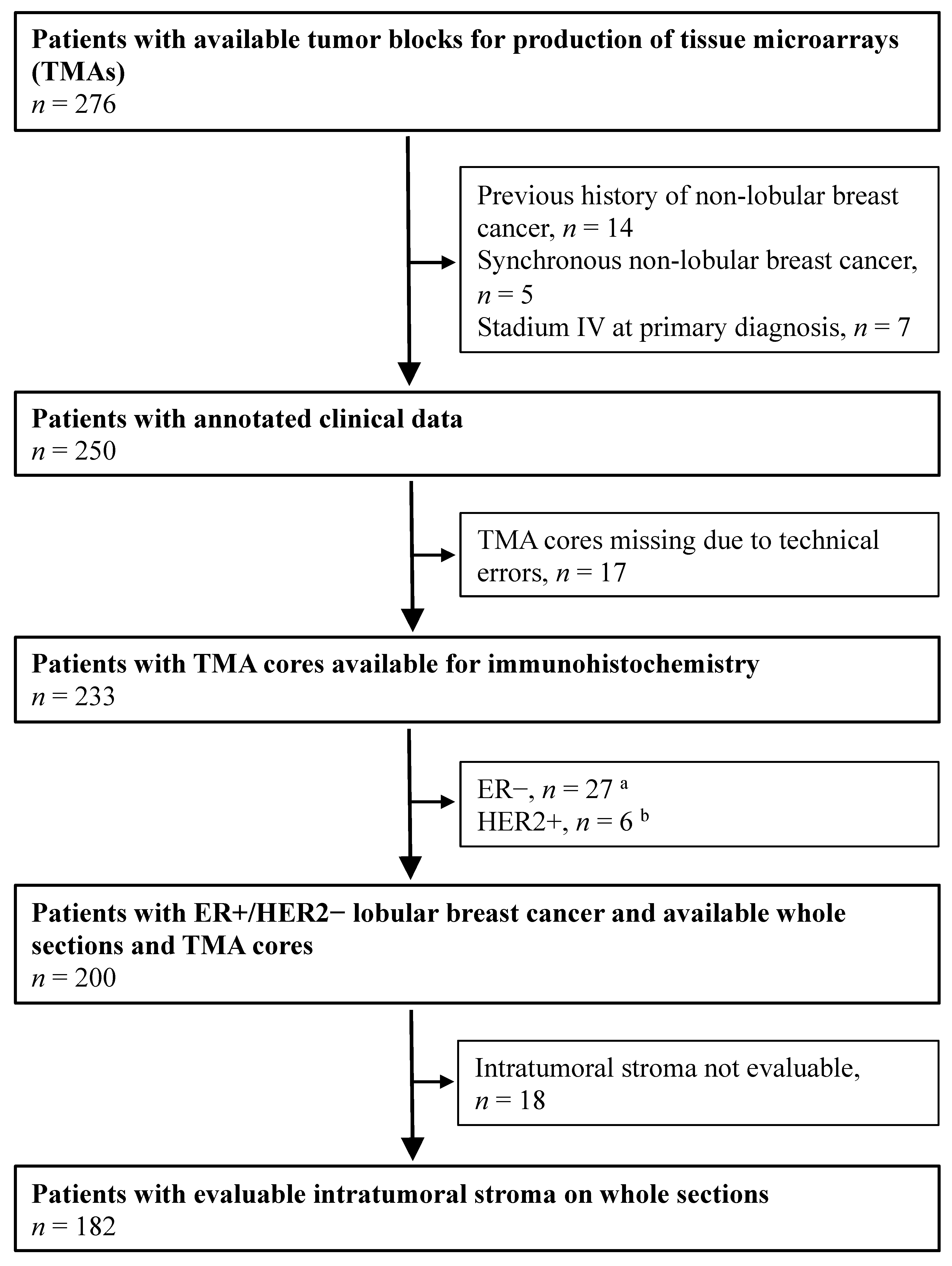
2.1. Study Population
2.2. Immunohistochemical Assays of PR and Ki67
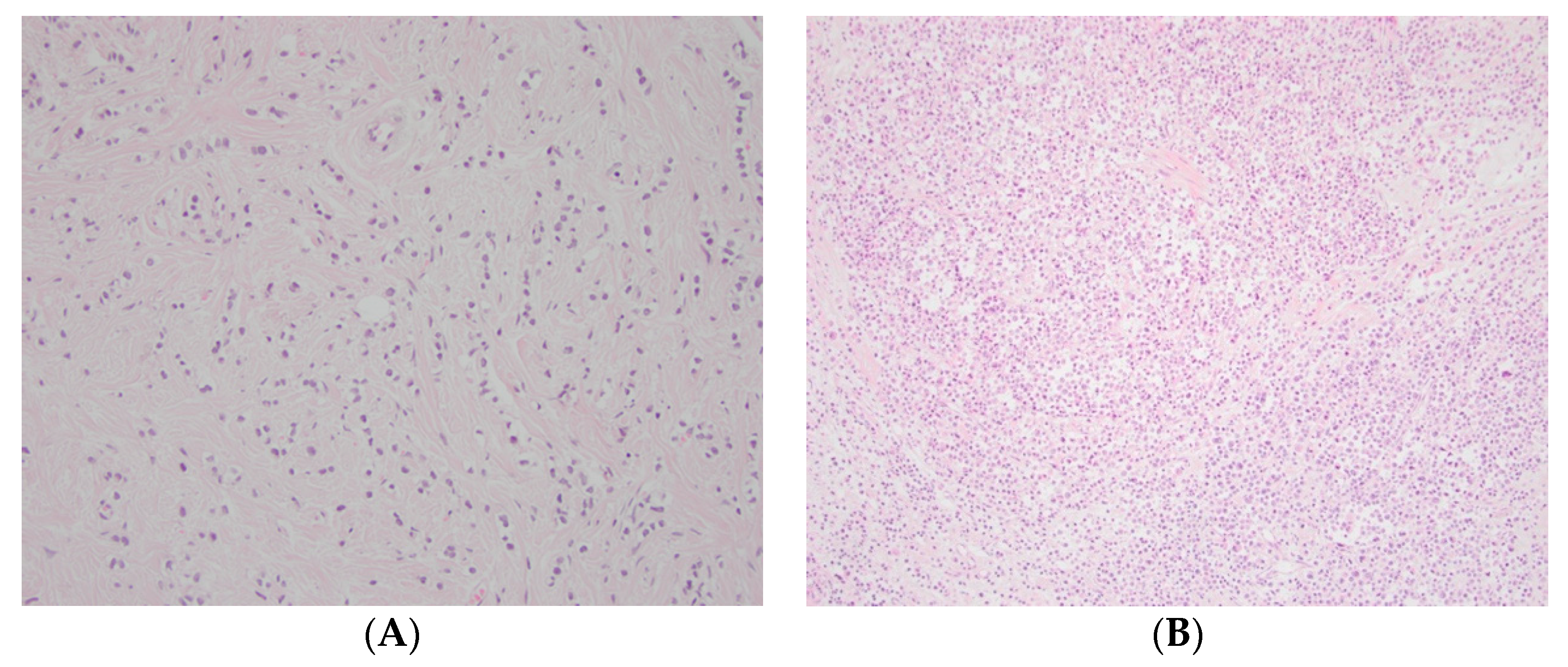
2.3. Assessment of Intratumoral Stromal Content
2.4. Statistical Analysis
3. Results
3.1. Intratumoral Stromal Content and Association with Other Clinicopathological Variables
3.2. Breast Cancer Mortality
3.3. Exploratory Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Christgen, M.; Steinemann, D.; Kühnle, E.; Länger, F.; Gluz, O.; Harbeck, N.; Kreipe, H. Lobular breast cancer: Clinical, molecular and morphological characteristics. Pathol. Res. Pract. 2016, 212, 583–597. [Google Scholar] [CrossRef] [PubMed]
- Martinez, V.; Azzopardi, J.G. Invasive lobular carcinoma of the breast: Incidence and variants. Histopathology 1979, 3, 467–488. [Google Scholar] [CrossRef] [PubMed]
- Barroso-Sousa, R.; Metzger-Filho, O. Differences between invasive lobular and invasive ductal carcinoma of the breast: Results and therapeutic implications. Ther. Adv. Med. Oncol. 2016, 8, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Millar, E.K.; Browne, L.H.; Beretov, J.; Lee, K.; Lynch, J.; Swarbrick, A.; Graham, P.H. Tumour Stroma Ratio Assessment Using Digital Image Analysis Predicts Survival in Triple Negative and Luminal Breast Cancer. Cancers 2020, 12, 3749. [Google Scholar] [CrossRef]
- Nakagawa, S.; Miki, Y.; Miyashita, M.; Hata, S.; Takahashi, Y.; Rai, Y.; Sagara, Y.; Ohi, Y.; Hirakawa, H.; Tamaki, K.; et al. Tumor microenvironment in invasive lobular carcinoma: Possible therapeutic targets. Breast Cancer Res. Treat. 2016, 155, 65–75. [Google Scholar] [CrossRef]
- Pietras, K.; Östman, A. Hallmarks of cancer: Interactions with the tumor stroma. Exp. Cell Res. 2010, 316, 1324–1331. [Google Scholar] [CrossRef]
- El Bairi, K.; Haynes, H.R.; Blackley, E.; Fineberg, S.; Shear, J.; Turner, S.; De Freitas, J.R.; Sur, D.; Amendola, L.C.; Gharib, M.; et al. The tale of TILs in breast cancer: A report from The International Immuno-Oncology Biomarker Working Group. NPJ Breast Cancer 2021, 7, 150. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Roeke, T.; Sobral-Leite, M.; Dekker, T.J.A.; Wesseling, J.; Smit, V.T.H.B.M.; Tollenaar, R.A.E.M.; Schmidt, M.K.; Mesker, W.E. The prognostic value of the tumour-stroma ratio in primary operable invasive cancer of the breast: A validation study. Breast Cancer Res. Treat. 2017, 166, 435–445. [Google Scholar] [CrossRef]
- Moorman, A.; Vink, R.; Heijmans, H.; Van Der Palen, J.; Kouwenhoven, E. The prognostic value of tumour-stroma ratio in triple-negative breast cancer. Eur. J. Surg. Oncol. 2012, 38, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Downey, C.L.; Simpkins, S.A.; White, J.; Holliday, D.L.; Jones, J.L.; Jordan, L.B.; Kulka, J.; Pollock, S.; Rajan, S.S.; Thygesen, H.H.; et al. The prognostic significance of tumour–stroma ratio in oestrogen receptor-positive breast cancer. Br. J. Cancer 2014, 110, 1744–1747. [Google Scholar] [CrossRef]
- Mesker, W.E.; Junggeburt, J.M.C.; Szuhai, K.; De Heer, P.; Morreau, H.; Tanke, H.J.; Tollenaar, R.A.E.M. The Carcinoma–Stromal Ratio of Colon Carcinoma Is an Independent Factor for Survival Compared to Lymph Node Status and Tumor Stage. Cell. Oncol. 2007, 29, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liang, C.; Chen, M.; Su, W. Association between tumor-stroma ratio and prognosis in solid tumor patients: A systematic review and meta-analysis. Oncotarget 2016, 7, 68954–68965. [Google Scholar] [CrossRef] [PubMed]
- De Kruijf, E.M.; Van Nes, J.G.; Van De Velde, C.J.; Putter, H.; Smit, V.T.; Liefers, G.J.; Kuppen, P.J.; Tollenaar, R.A.; Mesker, W.E. Tumor-stroma ratio in the primary tumor is a prognostic factor in early breast cancer patients, especially in triple-negative carcinoma patients. Breast Cancer Res. Treat. 2011, 125, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.J.H.; Vangangelt, K.M.H.; Van Pelt, G.W.; Dekker, T.; Tollenaar, R.A.E.M.; Mesker, W.E. The prognostic value of tumour–stroma ratio in primary breast cancer with special attention to triple-negative tumours: A review. Breast Cancer Res. Treat. 2019, 173, 55–64. [Google Scholar] [CrossRef]
- Dekker, T.J.; Van De Velde, C.J.; Van Pelt, G.W.; Kroep, J.R.; Julien, J.P.; Smit, V.T.; Tollenaar, R.A.; Mesker, W.E. Prognostic significance of the tumor-stroma ratio: Validation study in node-negative premenopausal breast cancer patients from the EORTC perioperative chemotherapy (POP) trial (10854). Breast Cancer Res. Treat. 2013, 139, 371–379. [Google Scholar] [CrossRef]
- Vangangelt, K.M.H.; Van Pelt, G.W.; Engels, C.C.; Putter, H.; Liefers, G.J.; Smit, V.T.H.B.M.; Tollenaar, R.A.E.M.; Kuppen, P.J.K.; Mesker, W.E. Prognostic value of tumor-stroma ratio combined with the immune status of tumors in invasive breast carcinoma. Breast Cancer Res. Treat. 2018, 168, 601–612. [Google Scholar] [CrossRef]
- Vangangelt, K.M.H.; Green, A.R.; Heemskerk, I.M.F.; Cohen, D.; Van Pelt, G.W.; Sobral-Leite, M.; Schmidt, M.K.; Putter, H.; Rakha, E.A.; Tollenaar, R.A.; et al. The prognostic value of the tumor–stroma ratio is most discriminative in patients with grade III or triple-negative breast cancer. Int. J. Cancer 2020, 146, 2296–2304. [Google Scholar] [CrossRef]
- Gujam, F.J.A.; Edwards, J.; Mohammed, Z.M.A.; Going, J.; McMillan, D. The relationship between the tumour stroma percentage, clinicopathological characteristics and outcome in patients with operable ductal breast cancer. Br. J. Cancer 2014, 111, 157–165. [Google Scholar] [CrossRef]
- Downey, C.L.; Thygesen, H.H.; Sharma, N.; Shaaban, A.M. Prognostic significance of tumour stroma ratio in inflammatory breast cancer. SpringerPlus 2015, 4, 68. [Google Scholar] [CrossRef]
- Narbe, U.; Bendahl, P.-O.; Grabau, D.; Rydén, L.; Ingvar, C.; Fernö, M. Invasive lobular carcinoma of the breast: Long-term prognostic value of Ki67 and histological grade, alone and in combination with estrogen receptor. SpringerPlus 2014, 3, 70. [Google Scholar] [CrossRef] [PubMed]
- Narbe, U.; Sjostrom, M.; Forsare, C.; Bendahl, P.O.; Alkner, S.; Leeb-Lundberg, L.M.F.; Lovgren, K.; Ryden, L.; Ingvar, C.; Ferno, M. The estrogen receptor coactivator AIB1 is a new putative prognostic biomarker in ER-positive/HER2-negative invasive lobular carcinoma of the breast. Breast Cancer Res. Treat. 2019, 175, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Burstein, H.J.; Winer, E.P.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.-J.; et al. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann. Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Metzger Filho, O.; Giobbie-Hurder, A.; Mallon, E.; Gusterson, B.; Viale, G.; Winer, E.P.; Thurlimann, B.; Gelber, R.D.; Colleoni, M.; Ejlertsen, B.; et al. Relative Effectiveness of Letrozole Compared with Tamoxifen for Patients with Lobular Carcinoma in the BIG 1-98 Trial. J. Clin. Oncol. 2015, 33, 2772–2779. [Google Scholar] [CrossRef]
- Rakha, E.A.; El-Sayed, M.E.; Powe, D.G.; Green, A.; Habashy, H.O.; Grainge, M.; Robertson, J.F.; Blamey, R.; Gee, J.; Nicholson, R.I.; et al. Invasive lobular carcinoma of the breast: Response to hormonal therapy and outcomes. Eur. J. Cancer 2008, 44, 73–83. [Google Scholar] [CrossRef]
- Vangangelt, K.M.H.; Kramer, C.J.H.; Bastiaannet, E.; Putter, H.; Cohen, D.; Van Pelt, G.W.; Rakha, E.A.; Green, A.R.; Tollenaar, R.A.E.M.; Mesker, W.E. The intra-tumoural stroma in patients with breast cancer increases with age. Breast Cancer Res. Treat. 2020, 179, 37–45. [Google Scholar] [CrossRef]
- Mesker, W.E.; Dekker, T.J.; De Kruijf, E.M.; Engels, C.C.; Van Pelt, G.W.; Smit, V.T.; Tollenaar, R.A. Comment on: The prognostic significance of tumour-stroma ratio in oestrogen receptor-positive breast cancer. Br. J. Cancer 2015, 112, 1832–1833. [Google Scholar] [CrossRef][Green Version]
- Downey, C.L.; Simpkins, S.A.; Holliday, D.L.; Jones, J.L.; Jordan, L.B.; Kulka, J.; Hanby, A.M.; Speirs, V. Reponse to: Comment on, ‘Tumour-stroma ratio (TSR) in oestrogen-positive breast cancer patients’. Br. J. Cancer 2015, 112, 1833–1834. [Google Scholar] [CrossRef][Green Version]
- Ahn, S.; Cho, J.; Sung, J.-Y.; Lee, J.E.; Nam, S.J.; Kim, K.-M.; Cho, E.Y. The prognostic significance of tumor-associated stroma in invasive breast carcinoma. Tumor Biol. 2012, 33, 1573–1580. [Google Scholar] [CrossRef]
- Vangangelt, K.M.; Tollenaar, L.S.; Van Pelt, G.W.; De Kruijf, E.M.; Dekker, T.; Kuppen, P.J.; Tollenaar, R.A.; Mesker, W.E. The prognostic value of tumor-stroma ratio in tumor-positive axillary lymph nodes of breast cancer patients. Int. J. Cancer 2018, 143, 3194–3200. [Google Scholar] [CrossRef] [PubMed]
- Park, C.K.; Jung, W.H.; Koo, J.S. Expression of cancer-associated fibroblast-related proteins differs between invasive lobular carcinoma and invasive ductal carcinoma. Breast Cancer Res. Treat. 2016, 159, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Barth, P.J.; Ebrahimsade, S.; Ramaswamy, A.; Moll, R. CD34+ fibrocytes in invasive ductal carcinoma, ductal carcinoma in situ, and benign breast lesions. Virchows Arch. 2002, 440, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, A.; Moll, R.; Barth, P.J. CD34 + fibrocytes in tubular carcinomas and radial scars of the breast. Virchows Arch. 2003, 443, 536–540. [Google Scholar] [CrossRef]
- Westhoff, C.C.; Jank, P.; Jacke, C.O.; Albert, U.-S.; Ebrahimsade, S.; Barth, P.J.; Moll, R. Prognostic relevance of the loss of stromal CD34 positive fibroblasts in invasive lobular carcinoma of the breast. Virchows Arch. 2020, 477, 717–724. [Google Scholar] [CrossRef]
- McCart Reed, A.E.; Kalinowski, L.; Simpson, P.T.; Lakhani, S.R. Invasive lobular carcinoma of the breast: The increasing importance of this special subtype. Breast Cancer Res. 2021, 23, 6. [Google Scholar] [CrossRef]
- Desmedt, C.; Salgado, R.; Fornili, M.; Pruneri, G.; Van Den Eynden, G.; Zoppoli, G.; Rothé, F.; Buisseret, L.; Garaud, S.; Willard-Gallo, K.; et al. Immune Infiltration in Invasive Lobular Breast Cancer. JNCI J. Natl. Cancer Inst. 2018, 110, 768–776. [Google Scholar] [CrossRef]
- Tille, J.-C.; Vieira, A.; Saint-Martin, C.; Djerroudi, L.; Furhmann, L.; Bidard, F.-C.; Kirova, Y.; Tardivon, A.; Reyal, F.; Carton, M.; et al. Tumor-infiltrating lymphocytes are associated with poor prognosis in invasive lobular breast carcinoma. Mod. Pathol. 2020, 33, 2198–2207. [Google Scholar] [CrossRef]
- Dennison, J.B.; Shahmoradgoli, M.; Liu, W.; Ju, Z.; Meric-Bernstam, F.; Perou, C.M.; Sahin, A.A.; Welm, A.L.; Oesterreich, S.; Sikora, M.J.; et al. High Intratumoral Stromal Content Defines Reactive Breast Cancer as a Low-risk Breast Cancer Subtype. Clin. Cancer Res. 2016, 22, 5068–5078. [Google Scholar] [CrossRef]
- Farmer, P.; Bonnefoi, H.; Anderle, P.; Cameron, D.A.; Wirapati, P.; Becette, V.; André, S.; Piccart-Gebhart, M.; Campone, M.; Brain, E.; et al. A stroma-related gene signature predicts resistance to neoadjuvant chemotherapy in breast cancer. Nat. Med. 2009, 15, 68–74. [Google Scholar] [CrossRef]
- Sonnenblick, A.; Salmon-Divon, M.; Salgado, R.; Dvash, E.; Pondé, N.; Zahavi, T.; Salmon, A.; Loibl, S.; Denkert, C.; Joensuu, H.; et al. Reactive stroma and trastuzumab resistance in HER2-positive early breast cancer. Int. J. Cancer 2020, 147, 266–276. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 182 | High Stroma (n = 82) | Low Stroma (n = 100) | p-Value |
|---|---|---|---|---|
| Age, median (range) | 63 (39–85) | 63 (37–85) | 62 (40–86) | 0.581 a |
| Menopause | 0.326 b | |||
| Pre | 43 | 17 | 26 | |
| Post | 133 | 64 | 69 | |
| Missing | 6 | |||
| Size | 0.281 b | |||
| 0–20 mm | 103 | 49 | 54 | |
| >20mm | 76 | 30 | 46 | |
| Missing | 3 | |||
| Nodal status | 0.359 b | |||
| 0 | 107 | 54 | 53 | |
| 1–3 | 27 | 11 | 16 | |
| 4+ | 39 | 15 | 24 | |
| Missing | 9 | |||
| NHG | <0.001 b | |||
| 1 | 22 | 19 | 3 | |
| 2 | 145 | 62 | 83 | |
| 3 | 13 | 0 | 13 | |
| Missing | 2 | |||
| PR | 0.827 b | |||
| <1% | 35 | 16 | 19 | |
| ≥1% | 142 | 62 | 80 | |
| Missing | 5 | |||
| ≤20% | 46 | 19 | 27 | 0.661 b |
| >20% | 131 | 59 | 72 | |
| Missing | 5 | |||
| Ki67 | 0.049 b | |||
| Low (<24%) | 161 | 74 | 87 | |
| High (≥24%) | 12 | 2 | 10 | |
| Missing | 9 | |||
| Luminal | 0.012 b | |||
| Luminal A-like | 111 | 57 | 54 | |
| Luminal B-like | 63 | 20 | 43 | |
| Missing | 8 | |||
| Surgery | 0.568 b | |||
| BCS | 43 | 21 | 22 | |
| Mastectomy | 139 | 61 | 78 | |
| Endocrine treatment c | 0.159 b | |||
| Yes | 72 | 28 | 44 | |
| No | 109 | 54 | 55 | |
| Missing | 1 | |||
| Chemotherapy c | 0.503 b | |||
| Yes | 5 | 3 | 2 | |
| No | 176 | 79 | 97 | |
| Missing | 1 | |||
| Recurrence d | 0.018 b | |||
| Yes | 75 | 26 | 49 | |
| No | 107 | 56 | 51 |
| Variables | n | Univariable 10 Years | Multivariable (n = 157) 10 Years | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age (years) | 182 | 0.94 | 0.91–0.97 | <0.001 | 0.93 | 0.89–0.98 | 0.002 |
| Size (0–20 vs. >20 mm) | 179 | 3.56 | 1.78–7.14 | <0.001 | 1.64 | 0.64–4.21 | 0.304 |
| Nodal status | |||||||
| N0 | 107 | 1.00 | 1.00 | ||||
| N1 (1–3+) | 27 | 1.66 | 0.58–4.71 | 0.342 | 0.67 | 0.17–2.68 | 0.566 |
| N ≥ 2 (4+) | 39 | 5.92 | 2.85–12.33 | <0.001 | 2.83 | 1.02–7.80 | 0.045 |
| NHG (3grps) | |||||||
| 1 | 22 | 0.22 | 0.03–1.61 | 0.136 | 1.05 | 0.12–9.55 | 0.967 |
| 2 | 145 | 1.00 | 1.00 | ||||
| 3 | 13 | 3.93 | 1.51–10.21 | 0.005 | 5.68 | 1.81–17.86 | 0.003 |
| PR (≤1 vs. >1%) | 177 | 0.64 | 0.30–1.37 | 0.248 | 0.24 | 0.08–0.72 | 0.010 |
| Ki67 (high vs. low) | 173 | 5.33 | 2.30–12.36 | <0.001 | 4.00 | 1.41–11.33 | 0.009 |
| Stroma (high vs. low) | 182 | 0.43 | 0.21–0.89 | 0.023 | 0.45 | 0.16–1.26 | 0.128 |
| ET (yes vs. no) | 181 | 0.52 | 0.27–1.00 | 0.048 | 0.58 | 0.22–1.52 | 0.270 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsare, C.; Vistrand, S.; Ehinger, A.; Lövgren, K.; Rydén, L.; Fernö, M.; Narbe, U. The Prognostic Role of Intratumoral Stromal Content in Lobular Breast Cancer. Cancers 2022, 14, 941. https://doi.org/10.3390/cancers14040941
Forsare C, Vistrand S, Ehinger A, Lövgren K, Rydén L, Fernö M, Narbe U. The Prognostic Role of Intratumoral Stromal Content in Lobular Breast Cancer. Cancers. 2022; 14(4):941. https://doi.org/10.3390/cancers14040941
Chicago/Turabian StyleForsare, Carina, Sara Vistrand, Anna Ehinger, Kristina Lövgren, Lisa Rydén, Mårten Fernö, and Ulrik Narbe. 2022. "The Prognostic Role of Intratumoral Stromal Content in Lobular Breast Cancer" Cancers 14, no. 4: 941. https://doi.org/10.3390/cancers14040941
APA StyleForsare, C., Vistrand, S., Ehinger, A., Lövgren, K., Rydén, L., Fernö, M., & Narbe, U. (2022). The Prognostic Role of Intratumoral Stromal Content in Lobular Breast Cancer. Cancers, 14(4), 941. https://doi.org/10.3390/cancers14040941