
Long-Term Clinical Outcome and Prognostic Factors of Children and Adolescents with Localized Rhabdomyosarcoma Treated on the CWS-2002P Protocol

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
Statistical Considerations
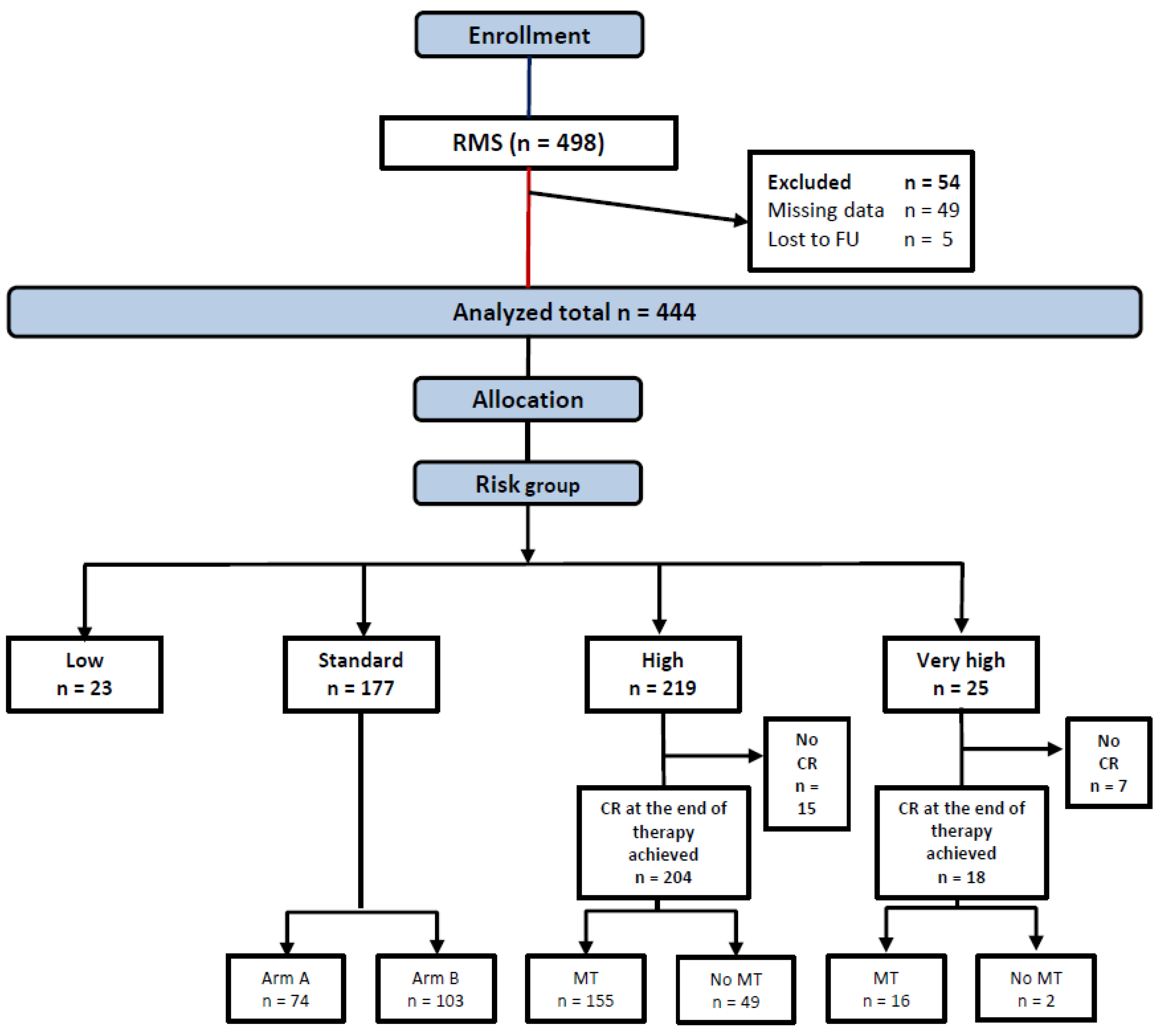
3. Results
3.1. Patients Characteristics
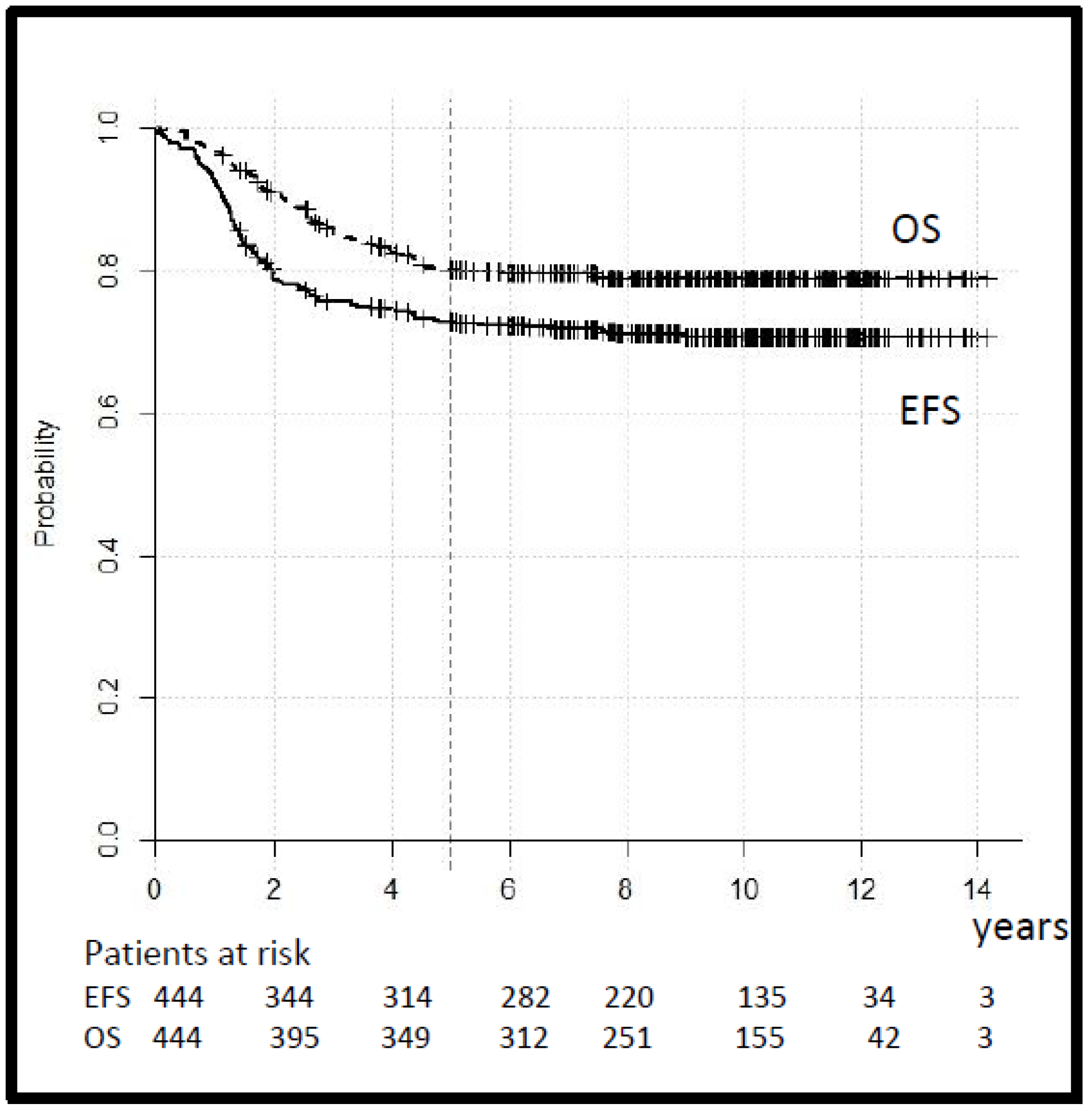
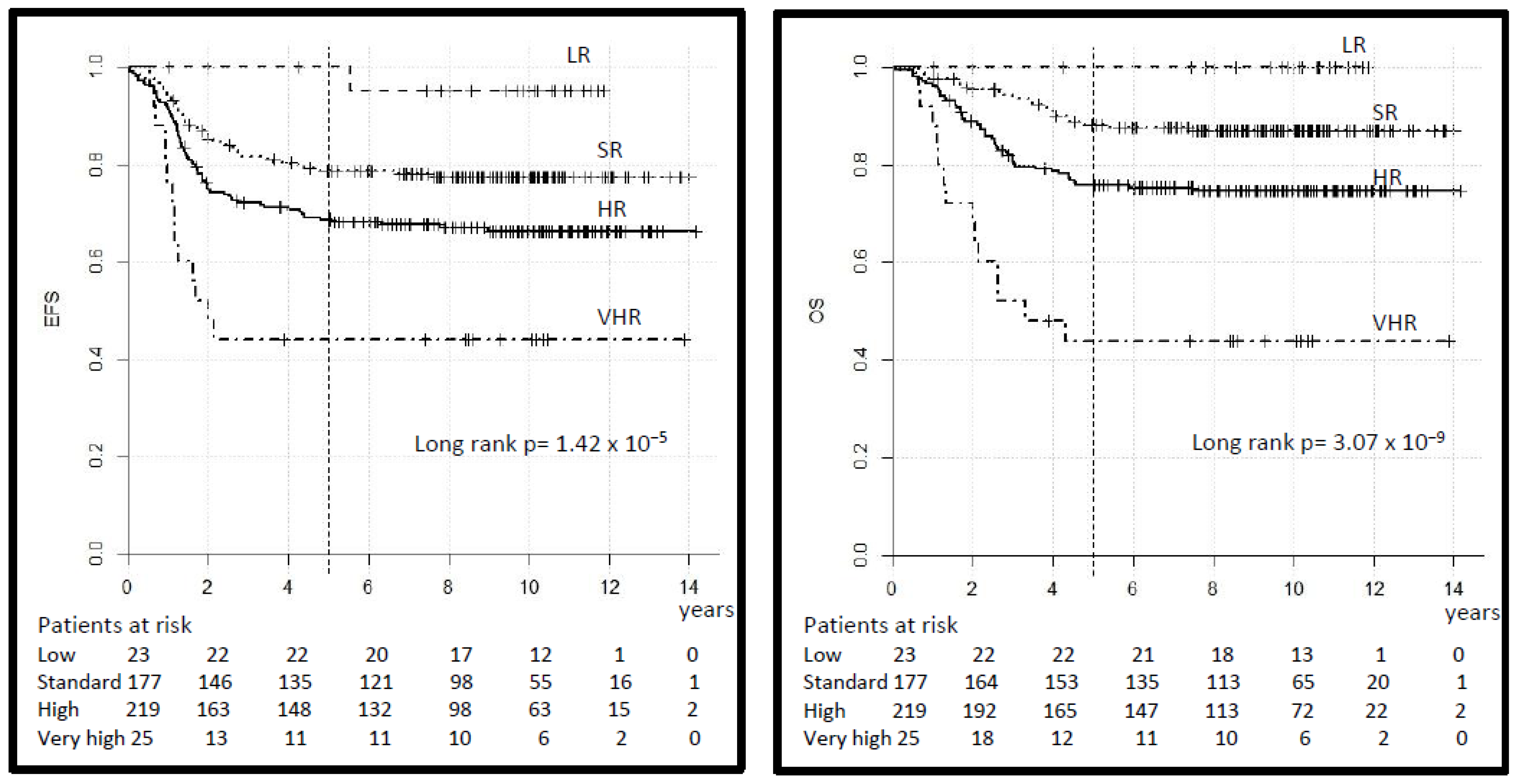
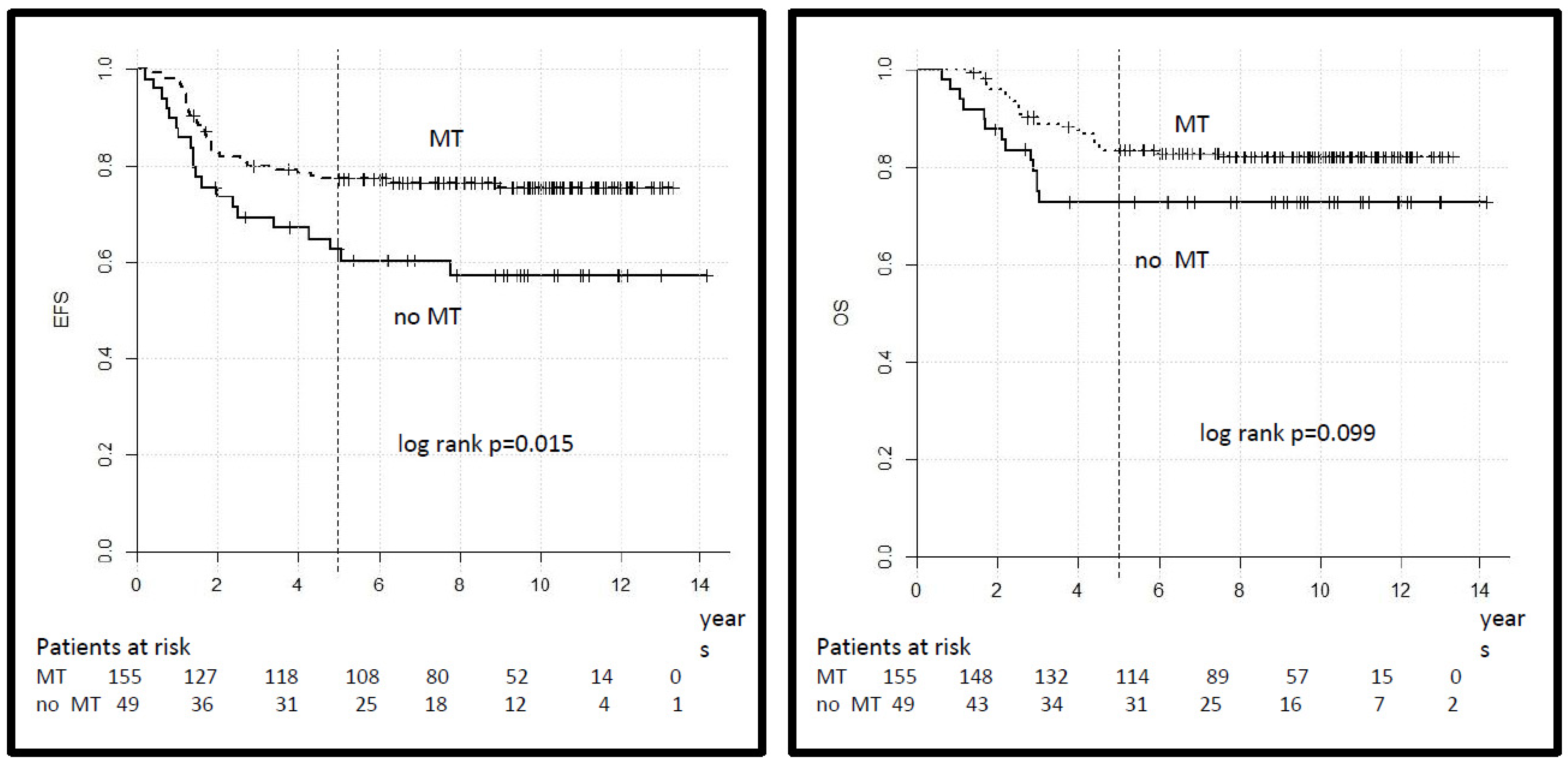
3.2. Outcome
3.3. Toxicities
3.4. Univariate and Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arndt, C.A.; Bisogno, G.; Koscielniak, E. Fifty years of rhabdomyosarcoma studies on both sides of the pond and lessons learned. Cancer Treat. Rev. 2018, 68, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.C.; Rey, A.; Bouvet, N.; Ellershaw, C.; Flamant, F.; Habrand, J.L.; Marsden, H.B.; Martelli, H.; de Toledo, J.S.; Spicer, R.D.; et al. Treatment of Nonmetastatic Rhabdomyosarcoma in Childhood and Adolescence: Third Study of the International Society of Paediatric Oncology—SIOP Malignant Mesenchymal Tumor 89. J. Clin. Oncol. 2005, 23, 2618–2628. [Google Scholar] [CrossRef] [PubMed]
- Meza, J.L.; Anderson, J.; Pappo, A.S.; Meyer, W.H.; Children’s Oncology Group. Analysis of prognostic factors in patients with nonmetastatic rhabdomyosarcoma treated on intergroup rhabdomyosarcoma studies III and IV: The Children’s Oncology Group. J. Clin. Oncol. 2006, 24, 3844–3851. [Google Scholar] [CrossRef] [PubMed]
- Hibbitts, E.; Chi, Y.Y.; Hawkins, D.S.; Barr, F.G.; Bradley, J.A.; Dasgupta, R.; Meyer, W.H.; Rodeberg, D.A.; Rudzinski, E.R.; Spunt, S.L.; et al. Refinement of risk stratification for childhood rhabdomyosarcoma using FOXO1 fusion status in addition to established clinical outcome predictors: A report from the Children’s Oncology Group. Cancer Med. 2019, 8, 6437–6448. [Google Scholar] [CrossRef] [Green Version]
- Koscielniak, E.; Jürgens, H.; Winkler, K.; Bürger, D.; Herbst, M.; Keim, M.; Bernhard, G.; Treuner, J. Treatment of soft tissue sarcoma in childhood and adolescence: A report of the german cooperative soft tissue sarcoma study. Cancer 1992, 70, 2557–2567. [Google Scholar] [CrossRef]
- Koscielniak, E.; Harms, D.; Henze, G.; Jürgens, H.; Gadner, H.; Herbst, M.; Klingebiel, T.; Schmidt, B.F.; Morgan, M.; Knietig, R.; et al. Results of Treatment for Soft Tissue Sarcoma in Childhood and Adolescence: A Final Report of the German Cooperative Soft Tissue Sarcoma Study CWS-86. J. Clin. Oncol. 1999, 17, 3706–3719. [Google Scholar] [CrossRef]
- Dantonello, T.M.; Int-Veen, C.; Harms, D.; Leuschner, I.; Schmidt, B.F.; Herbst, M.; Juergens, H.; Scheel-Walter, H.-G.; Bielack, S.S.; Klingebiel, T.; et al. Cooperative Trial CWS-91 for Localized Soft Tissue Sarcoma in Children, Adolescents, and Young Adults. J. Clin. Oncol. 2009, 27, 1446–1455. [Google Scholar] [CrossRef]
- Treuner, J.; Brecht, I.B.; Mattke, A.D.; Harms, D.; Gadner, H.; Kazanowska, B.; Marky, I.; Koscielniak, E. Interim report of the CWS-96 study: Results of the treatment for soft tissue sarcomas in childhood. Med. Pediatr. Oncol. 2003, 41, 278. [Google Scholar]
- Oberlin, O.; Rey, A.; De Toledo, J.S.; Martelli, H.; Jenney, M.E.M.; Scopinaro, M.; Bergeron, C.; Merks, J.H.M.; Bouvet, N.; Ellershaw, C.; et al. Randomized Comparison of Intensified Six-Drug Versus Standard Three-Drug Chemotherapy for High-Risk Nonmetastatic Rhabdomyosarcoma and Other Chemotherapy-Sensitive Childhood Soft Tissue Sarcomas: Long-Term Results FROM the International Society of Pediatric Oncology MMT95 Study. J. Clin. Oncol. 2012, 30, 2457–2465. [Google Scholar] [CrossRef]
- Bisogno, G.; Jenney, M.; Bergeron, C.; Melcón, S.G.; Ferrari, A.; Oberlin, O.; Carli, M.; Stevens, M.; Kelsey, A.; De Paoli, A.; et al. Addition of dose-intensified doxorubicin to standard chemotherapy for rhabdomyosarcoma (EpSSG RMS 2005): A multicentre, open-label, randomised controlled, phase 3 trial. Lancet Oncol. 2018, 19, 1061–1071. [Google Scholar] [CrossRef]
- Bisogno, G.; Jenney, M.; Merks, J.H.M.; Minard-Colin, V.; Daragjati, J.; Zanetti, I.; Gallego, S.; Shipley, J.; Ferrari, A.; Chisholm, J.; et al. Assessing the risk profile of rhabdomyosarcoma patients in a new classification system for the next European Pediatric Soft Tisue Sarcoma Study Group (EpSSG) protocol. Pediatr. Blood Cancer 2019, 66 (Suppl. 4), 63. [Google Scholar]
- Newton, W.A., Jr.; Gehan, E.A.; Webber, B.L.; Marsden, H.B.; Van Unnik, A.J.M.; Hamoudi, A.B.; Tsokos, M.C.; Shimada, H.; Harms, D.; Schmidt, D.; et al. Classification of rhabdomyosarcomas and related sarcomas. Pathologic aspects and proposal for a new classification—An Intergroup Rhabdomyosarcoma Study. Cancer 1995, 76, 1073–1085. [Google Scholar] [CrossRef]
- Rodary, C.; Flamant, F.; Donaldson, S.S. An attempt to use a common staging system in rhabdomyosarcoma: A report of an international workshop initiated by the international society of pediatric oncology (SIOP). Med. Pediatr. Oncol. 1989, 17, 210–215. [Google Scholar] [CrossRef]
- Maurer, H.M.; Crist, W.; Lawrence, W.; Ragab, A.H.; Raney, R.B.; Webber, B.; Wharam, M.; Vietti, T.J.; Beltangady, M.; Gehan, E.A.; et al. The Intergroup Rhabdomyosarcoma Study-I. A final report. Cancer 1988, 61, 209–220. [Google Scholar] [CrossRef]
- Dantonello, T.M.; Stark, M.; Timmermann, B.; Fuchs, J.; Selle, B.; Linderkamp, C.; Handgretinger, R.; Hagen, R.; Cdm, S.F.; Kube, S.; et al. Tumour volume reduction after neoadjuvant chemotherapy impacts outcome in localised embryonal rhabdomyosarcoma. Pediatr. Blood Cancer 2014, 62, 16–23. [Google Scholar] [CrossRef]
- Walterhouse, D.O.; Pappo, A.S.; Meza, J.L.; Breneman, J.C.; Hayes-Jordan, A.; Parham, D.M.; Cripe, T.P.; Anderson, J.R.; Meyer, W.H.; Hawkins, D.S. Reduction of cyclophosphamide dose for patients with subset 2 low-risk rhabdomyosarcoma is associated with an increased risk of recurrence: A report from the Soft Tissue Sarcoma Committee of the Children’s Oncology Group. Cancer 2017, 123, 2368–2375. [Google Scholar] [CrossRef]
- Walterhouse, D.O.; Pappo, A.S.; Meza, J.L.; Breneman, J.C.; Hayes-Jordan, A.A.; Parham, D.M.; Cripe, T.P.; Anderson, J.R.; Meyer, W.H.; Hawkins, D.S. Shorter-duration therapy using vincristine, dactinomycin, and lower-dose cyclophosphamide with or without radiotherapy for patients with newly diagnosed low-risk rhabdomyosarcoma: A report from the Soft Tissue Sarcoma Committee of the Children’s Oncology Group. J. Clin. Oncol. 2014, 32, 3547–3552. [Google Scholar]
- Casey, D.L.; Chi, Y.Y.; Donaldson, S.S.; Hawkins, D.S.; Tian, J.; Arndt, C.A.; Rodeberg, D.A.; Routh, J.C.; Lautz, T.B.; Gupta, A.A.; et al. Increased local failure for patients with intermediate-risk rhabdomyosarcoma on ARST0531: A report from the Children’s Oncology Group. Cancer 2019, 125, 3242–3248. [Google Scholar] [CrossRef]
- Rodary, C.; Gehan, E.A.; Flamant, F.; Treuner, J.; Carli, M.; Auquier, A.; Maurer, H. Prognostic factors in 951 nonmetastatic rhabdomyosarcoma in children: A report from the international rhabdomyosarcoma workshop. Med. Pediatr. Oncol. 1991, 19, 89–95. [Google Scholar] [CrossRef]
- Arndt, C.A. Role of Doxorubicin in rhabdomyosarcoma: Is the answer knowable? In American Society of Clinical Oncology Educational Book; American Society of Clinical Oncology: Alexandria, VA, USA, 2012; Volume 3, pp. 621–623. [Google Scholar]
- Klingebiel, T.; Boos, J.; Beske, F.; Hallmen, E.; Int-Veen, C.; Dantonello, T.; Treuner, J.; Gadner, H.; Marky, I.; Kazanowska, B.; et al. Treatment of children with metastatic soft tissue sarcoma with oral maintenance compared to high dose chemotherapy: Report of the HD CWS-96 trial. Pediatr. Blood Cancer 2008, 50, 739–745. [Google Scholar] [CrossRef]
- Bisogno, G.; De Salvo, G.L.; Bergeron, C.; Melcón, S.G.; Merks, J.H.; Kelsey, A.; Martelli, H.; Minard-Colin, V.; Orbach, D.; Glosli, H.; et al. Vinorelbine and continuous low-dose cyclophosphamide as maintenance chemotherapy in patients with high-risk rhabdomyosarcoma (RMS 2005): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2019, 20, 1566–1575. [Google Scholar] [CrossRef]
- Rudzinski, E.R.; Kelsey, A.; Vokuhl, C.; Linardic, C.M.; Shipley, J.; Hettmer, S.; Koscielniak, E.; Hawkins, D.S.; Bisogno, G. Pathology of childhood rhabdomyosarcoma: A consensus opinion document from the Children’s Oncology Group, European Paediatric Soft Tissue Sarcoma Study Group, and the Cooperative Weichteilsarkom Studiengruppe. Pediatr. Blood Cancer 2021, 68, e28798. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Group | Pathology | IRS Group | Site | LN Stage | Size and Age |
|---|---|---|---|---|---|
| Low (LR) | eRMS | I | Any | N0 | Favorable |
| Standard (SR) | eRMS | I | Any | N0 | Unfavorable |
| eRMS | II, III | Favorable | N0 | Any | |
| eRMS | II, III | Unfavorable | N0 | Favorable | |
| High (HR) | eRMS | II, III | Unfavorable | N0 | Unfavorable |
| eRMS | II, III | Any | N1 | Any | |
| aRMS | I, II, III | Any | N0 | Any | |
| Very High (VHR) | aRMS | I, II, III | Any | N1 | Any |
| Risk Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Low | Standard | High | Very High | ||||||
| No. | % | No. | % | No. | % | No. | % | No. | % | |
| 444 | 100 | 23 | 5 | 117 | 40 | 219 | 49 | 25 | 6 | |
| Variable | ||||||||||
| Sex | ||||||||||
| Male | 260 | 58 | 21 | 91 | 103 | 58 | 123 | 56 | 13 | 54 |
| Female | 184 | 42 | 2 | 9 | 74 | 42 | 96 | 44 | 12 | 46 |
| Age | ||||||||||
| ≤10 years | 331 | 74 | 23 | 100 | 135 | 76 | 162 | 74 | 11 | 46 |
| >10 years | 113 | 25 | - | - | 42 | 24 | 57 | 26 | 14 | 54 |
| Histology | ||||||||||
| aRMS fusion positive | 53 | 12 | - | - | - | - | 34 | 16 | 19 | 76 |
| aRMS fusion negative | 7 | 2 | - | - | - | - | 7 | 4 | - | - |
| aRMS fusion unknown | 21 | 4 | - | - | - | 14 | 7 | 6 | 31 | |
| Non-aRMS | 363 | 82 | 23 | 100 | 177 | 100 | 163 | 74 | - | - |
| Tumor site | ||||||||||
| EXT | 38 | 9 | - | - | 4 | 2 | 30 | 14 | 4 | 15 |
| HN-nPM | 45 | 10 | 2 | 9 | 22 | 12 | 19 | 9 | 2 | 8 |
| HN-PM | 114 | 26 | - | - | 26 | 15 | 76 | - | 12 | 46 |
| ORBITA | 44 | 10 | - | - | 41 | 23 | 3 | 1 | - | - |
| GU-BP | 50 | 11 | - | - | 21 | 12 | 29 | 13 | - | 4 |
| GU-nBP | 80 | 18 | 21 | 91 | 53 | 30 | 6 | 3 | - | - |
| OTH | 72 | 16 | - | - | 10 | 6 | 55 | - | 7 | 27 |
| Not specified | 1 | - | - | - | - | 1 | - | - | - | |
| Tumor size | ||||||||||
| ≤5 cm | 223 | 50 | 23 | 100 | 132 | 74 | 62 | 28 | 6 | 23 |
| >5 cm | 206 | 47 | - | - | 42 | 24 | 145 | 66 | 19 | 77 |
| Not specified | 15 | 3 | - | - | 3 | 2 | 12 | 6 | - | - |
| IRSG | ||||||||||
| I | 55 | 12 | 23 | 100 | 27 | 15 | 5 | 2 | - | - |
| II | 67 | 15 | - | - | 43 | 24 | 23 | 11 | 1 | 4 |
| III | 322 | 73 | - | - | 107 | 61 | 191 | 87 | 24 | 96 |
| Tumor invasiveness | ||||||||||
| T1 | 210 | 47 | 19 | 83 | 115 | 65 | 70 | 32 | 6 | 27 |
| T2 | 204 | 46 | 3 | 13 | 54 | 31 | 129 | 59 | 18 | 69 |
| TX | 30 | 7 | 1 | 4 | 8 | 4 | 20 | 9 | 1 | 4 |
| Regional lymph nodes | ||||||||||
| N0 | 350 | 79 | 23 | 100 | 169 | 96 | 158 | 73 | - | - |
| N1 | 66 | 15 | - | - | - | - | 41 | 18 | 25 | 100 |
| NX | 28 | 6 | - | - | 8 | 4 | 20 | 9 | - | - |
| Risk Group | |||||
|---|---|---|---|---|---|
| Low n = 23 | Standard n = 177 | High n = 219 | Very High n = 25 | Total n = 444 | |
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| 1st Complete remission (CR) achieved | 23 (100) | 172 (97) | 204 (93) | 18 (73) | 417 (94) |
| Failures | |||||
| Local | 1 (4) | 26 (15) | 37 (17) | 4 (16) | 68 (15) |
| Metastatic | - | - | 6 (3) | 3 (12) | 9 (2) |
| Combined | - | 3 (2) | 5 (2) | - | 8 (2) |
| Progression | - | 6 (3) | 18 (8) | 7 (28) | 31 (7) |
| Not specified | - | 1 () | 3 (1) | - | 4 (1) |
| Total failures | 1 (4) | 36 (20) | 69 (32) | 14 (56) | 120 (27) |
| Sec malignancy | 0 | 13 | 9 | 0 | 22 |
| Alive | 23 (100) | 155 (88) | 165 (75) | 11 (44) | 354 (80) |
| Dead | 0 | 22 (12) | 54 (25) | 14 (56) | 90 (20) |
| DOD | 0 | 20 | 51 | 14 | 85 |
| DOT | 0 | 0 | 1 | 0 | 1 |
| DoOT | 0 | 0 | 2 | 0 | 2 |
| DOC | 0 | 2 | 0 | 0 | 2 |
| Median follow-up years (IQR) | 9.8 (7.8–10.6) | 9.9 (7.7–10.6) | 9.7 (7.4–11.3) | 9.3 (8.4–10.2) | 9.6 (7.6–10.9) |
| EFS 5 years rate% (95% CI) | 100 | 79 (72–84) | 69 (63–75) | 42 (23–61) | 73 (69–77) |
| EFS 10 years rate% (95% CI) | 95 (72–84) | 77 (70–84) | 67 (71–83) | 42 (23–61) | 71 (67–75) |
| OS 5 years rate% (95% CI) | 100 | 88 (83–93) | 76 (70–82) | 42 (23–61) | 80 (76–84) |
| OS 10 years rate% (95% CI) | 100 | 87 (84–90) | 75 (69–81) | 42 (23–61) | 79 (75–83) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koscielniak, E.; Blank, B.; Vokuhl, C.; Kazanowska, B.; Ladenstein, R.; Niggli, F.; Ljungman, G.; Handgretinger, R.; Seitz, G.; Fuchs, J.; et al. Long-Term Clinical Outcome and Prognostic Factors of Children and Adolescents with Localized Rhabdomyosarcoma Treated on the CWS-2002P Protocol. Cancers 2022, 14, 899. https://doi.org/10.3390/cancers14040899
Koscielniak E, Blank B, Vokuhl C, Kazanowska B, Ladenstein R, Niggli F, Ljungman G, Handgretinger R, Seitz G, Fuchs J, et al. Long-Term Clinical Outcome and Prognostic Factors of Children and Adolescents with Localized Rhabdomyosarcoma Treated on the CWS-2002P Protocol. Cancers. 2022; 14(4):899. https://doi.org/10.3390/cancers14040899
Chicago/Turabian StyleKoscielniak, Ewa, Bernd Blank, Christian Vokuhl, Bernarda Kazanowska, Ruth Ladenstein, Felix Niggli, Gustaf Ljungman, Rupert Handgretinger, Guido Seitz, Jörg Fuchs, and et al. 2022. "Long-Term Clinical Outcome and Prognostic Factors of Children and Adolescents with Localized Rhabdomyosarcoma Treated on the CWS-2002P Protocol" Cancers 14, no. 4: 899. https://doi.org/10.3390/cancers14040899
APA StyleKoscielniak, E., Blank, B., Vokuhl, C., Kazanowska, B., Ladenstein, R., Niggli, F., Ljungman, G., Handgretinger, R., Seitz, G., Fuchs, J., Fröhlich, B., Scheer, M., Wessalowski, R., Schmid, I., Sparber-Sauer, M., & Klingebiel, T. (2022). Long-Term Clinical Outcome and Prognostic Factors of Children and Adolescents with Localized Rhabdomyosarcoma Treated on the CWS-2002P Protocol. Cancers, 14(4), 899. https://doi.org/10.3390/cancers14040899