
Impact of Surgeon’s Experience in Rigid versus Elastic MRI/TRUS-Fusion Biopsy to Detect Significant Prostate Cancer Using Targeted and Systematic Cores

 , , ,
, , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
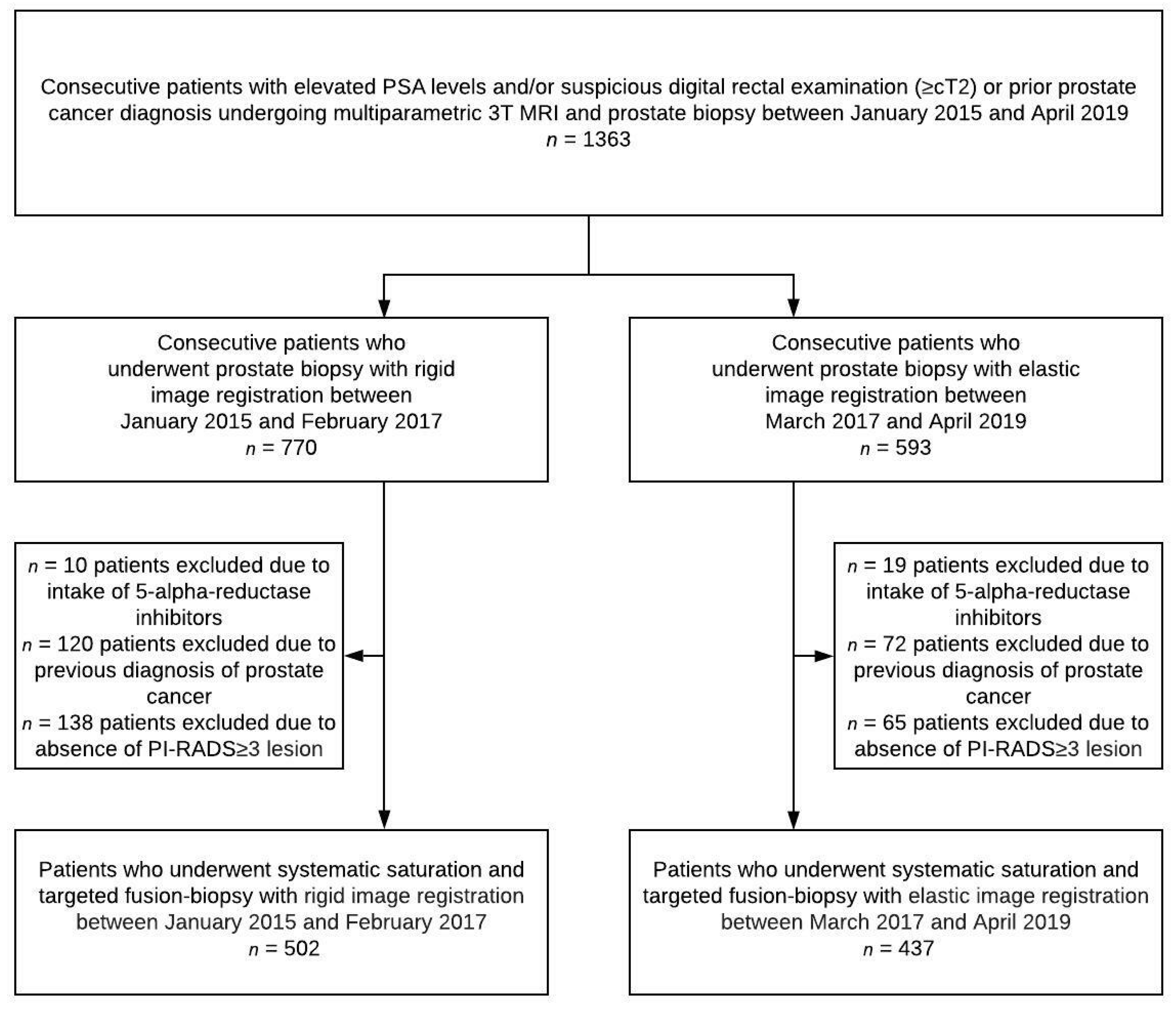
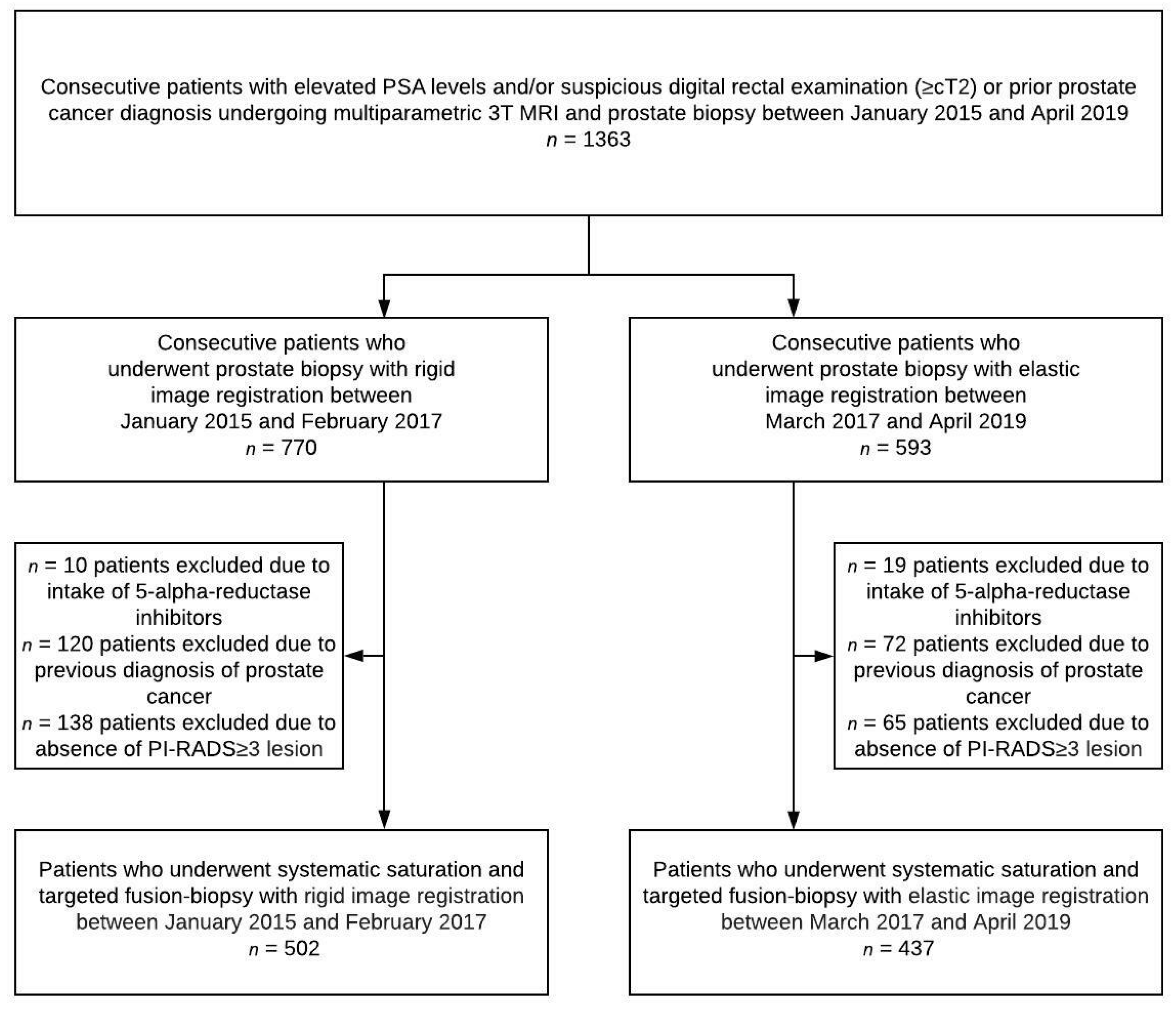
2.1. Study Population
2.2. MRI Analysis
2.3. Biopsy
2.4. Pathology
2.5. Statistical Analysis
3. Results

{kind=link}
| Rigid System | Elastic System | p Value | |
|---|---|---|---|
| Men included in study, n | 502 | 437 | |
| Men with significant prostate cancer, n (%) | 233 (46) | 201 (46) | 0.39 |
| Men with insignificant prostate cancer, n (%) | 81 (16) | 59 (14) | 0.39 |
| Age, years, median (IQR) | 65 (58–71) | 65 (59–70) | 0.30 |
| PSA level, ng/mL, median (IQR) | 7.7 (5.4–11.6) | 7.6 (5.4–10.8) | 0.38 |
| Suspicious DRE finding (≥T2), n (%) | 176 (35) | 121 (28) | 0.02 |
| Prostate volume, mL, median (IQR) | 44 (31–62) | 50 (34–73) | 0.001 |
| PSA density, ng/mL2, median (IQR) | 0.17 (0.11–0.27) | 0.15 (0.09–0.25) | 0.02 |
| Biopsies per patient, median (IQR) | 29 (26–33) | 34 (29–39) | 1.00 |
| Systematic biopsies per patient, median (IQR) | 24 (20–26) | 25 (22–29) | 0.89 |
| Targeted biopsies per lesion, median (IQR) | 4 (3–5) | 5 (4–6) | 0.84 |
| Number of lesions PI-RADS ≥ 3, n | 839 | 766 | |
| Patients with one PI-RADS ≥ 3 lesion, n (%) | 272 (54) | 205 (47) | |
| Patients with two PI-RADS ≥ 3 lesions, n (%) | 157 (31) | 158 (36) | |
| Patients with three PI-RADS ≥ 3 lesions, n (%) | 48 (10) | 57 (13) | |
| Patients with ≥ four PI-RADS ≥ 3 lesions, n (%) | 25 (5) | 17 (4) | |
| Overall PI-RADS score 3 lesions, n (%) | 367 (44) | 310 (40) | |
| Overall PI-RADS score 4 lesions, n (%) | 333 (40) | 332 (43) | |
| Overall PI-RADS score 5 lesions, n (%) | 139 (17) | 124 (16) | |
| Number of investigators performing biopsy, n | 17 | 17 | |
| Investigator experience > 200 biopsies, n (%) | 4 (24) | 5 (29) | |
| Investigator experience 100–200 biopsies, n (%) | 7 (41) | 5 (29) | |
| Investigator experience < 100 biopsies, n (%) | 6 (35) | 7 (41) | |
| Number of biopsies performed by investigators with >200 biopsies, n (%) | 146 (29) | 162 (37) | 0.009 |
| Number of biopsies performed by investigators with 100–200 biopsies, n (%) | 130 (26) | 201 (46) | <0.001 |
| Number of biopsies performed by investigators with <100 biopsies, n (%) | 226 (45) | 74 (17) | <0.001 |
| Rigid Targeted Biopsy (n = 233 Men with sPC) | Elastic Targeted Biopsy (n = 201 Men with sPC) | Difference (Confidence Interval) | p Value | |
|---|---|---|---|---|
| sPC detected by TB, % | 220/233 (94) | 175/201 (87) | 7 (1.5–12) | 0.02 |
| Highly experienced surgeons | 79/86 (92) | 55/59 (92) | 0 (−9.0–11) | 1.00 |
| Intermediate experienced surgeons | 105/109 (96) | 47/51 (92) | 4 (−3.8–15) | 0.58 |
| Low experienced surgeons | 36/38 (95) | 74/91 (82) | 13 (−11–24) | 0.05 |
| Highly Experienced (n = 145) | Intermediate Experienced (n = 160) | Difference (Confidence Interval) | p Value | |
|---|---|---|---|---|
| sPC detection (%) | 134/145 (92) | 152/160 (95) | −3.0 (−9.1–2.7) | 0.58 |
| Intermediate Experienced (n = 160) | Low Experienced (n = 129) | Difference D(Confidence Interval) | p Value | |
| sPC detection (%) | 152/160 (95) | 110/129 (85) | 10 (3.1–18) | 0.008 |
| Rigid System | Elastic System | p Value | |
|---|---|---|---|
| Number of patients | 13 | 26 | |
| Prostate volume, ml, median (IQR) | 42 (31–62) | 45 (28–70) | 0.43 |
| Number of lesions PI-RADS ≥ 3 | 27 | 43 | |
| PI-RADS score 3 lesion, n (%) | 11 (41) | 9 (21) | |
| PI-RADS score 4 lesion, n (%) | 11 (41) | 27 (63) | |
| PI-RADS score 5 lesion, n (%) | 5 (19) | 7 (16) | |
| Location of the lesion in the peripheral zone, n (%) | 17 (63) | 37 (86) | |
| Location of the lesion in the transitional zone, n (%) | 9 (33) | 6 (14) | |
| Location of the lesion in the anterior stroma, n (%) | 1 (4) | 0 (0) | |
| Volume of the lesion, mL, median (IQR) | 0.3 (0.1–0.8) | 0.4 (0.2–0.8) | 0.95 |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADC | apparent diffusion coefficient |
| CI | confidence interval |
| DRE | digital rectal examination |
| DWI | diffusion-weighted images |
| ETB | elastic targeted fusion-biopsy |
| FB | fusion biopsy |
| GS | Gleason score |
| ISUP | International Society of Urological Pathology |
| mpMRI | multiparametric magnetic resonance imaging |
| PC | prostate cancer |
| PI-RADS | Prostate Imaging Reporting and Data System |
| PSA | prostate specific antigen |
| RP | radical prostatectomy |
| RTB | rigid targeted fusion-biopsy |
| SB | systematic saturation biopsy |
| sPC | significant prostate cancer |
| TB | targeted fusion-biopsy |
| TRUS | transrectal ultrasound |
References
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- van der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouviere, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Padhani, A.R.; Weinreb, J.; Rosenkrantz, A.B.; Villeirs, G.; Turkbey, B.; Barentsz, J. Prostate Imaging-Reporting and Data System Steering Committee: PI-RADS v2 Status Update and Future Directions. Eur. Urol. 2019, 75, 385–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas, H.A.; Hotker, A.M.; Goldman, D.A.; Moskowitz, C.S.; Gondo, T.; Matsumoto, K.; Ehdaie, B.; Woo, S.; Fine, S.W.; Reuter, V.E.; et al. Updated prostate imaging reporting and data system (PIRADS v2) recommendations for the detection of clinically significant prostate cancer using multiparametric MRI: Critical evaluation using whole-mount pathology as standard of reference. Eur. Radiol. 2016, 26, 1606–1612. [Google Scholar] [CrossRef] [Green Version]
- Delongchamps, N.B.; Peyromaure, M.; Schull, A.; Beuvon, F.; Bouazza, N.; Flam, T.; Zerbib, M.; Muradyan, N.; Legman, P.; Cornud, F.B. Prebiopsy Magnetic Resonance Imaging and Prostate Cancer Detection: Comparison of Random and Targeted Biopsies. J. Urol. 2013, 189, 493–499. [Google Scholar] [CrossRef]
- Wegelin, O.; van Melick, H.H.; Hooft, L.; Bosch, J.R.; Reitsma, H.B.; Barentsz, J.O.; Somford, D.M. Comparing Three Different Techniques for Magnetic Resonance Imaging-targeted Prostate Biopsies: A Systematic Review of In-bore versus Magnetic Resonance Imaging-transrectal Ultrasound fusion versus Cognitive Registration. Is There a Preferred Technique? Eur. Urol. 2017, 71, 517–531. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Wegelin, O.; Exterkate, L.; van der Leest, M.; Kummer, J.A.; Vreuls, W.; de Bruin, P.C.; Bosch, J.; Barentsz, J.O.; Somford, D.M.; van Melick, H.H. The FUTURE Trial: A Multicenter Randomised Controlled Trial on Target Biopsy Techniques Based on Magnetic Resonance Imaging in the Diagnosis of Prostate Cancer in Patients with Prior Negative Biopsies. Eur. Urol. 2019, 75, 582–590. [Google Scholar] [CrossRef]
- Grummet, J.P.; Weerakoon, M.; Huang, S.; Lawrentschuk, N.; Frydenberg, M.; Moon, D.A.; O’Reilly, M.; Murphy, D. Sepsis and ‘superbugs’: Should we favour the transperineal over the transrectal approach for prostate biopsy? Br. J. Urol. 2013, 114, 384–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasabwala, K.; Patel, N.; Cricco-Lizza, E.; Shimpi, A.A.; Weng, S.; Buchmann, R.M.; Motanagh, S.; Wu, Y.; Banerjee, S.; Khani, F.; et al. The Learning Curve for Magnetic Resonance Imaging/Ultrasound Fusion-guided Prostate Biopsy. Eur. Urol. Oncol. 2019, 2, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J. Screening, risk assessment, and the approach to therapy in patients with prostate cancer. Cancer 2010, 117, 1123–1135. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.N.; Pedrosa, I.; Donato, F., Jr.; Roehrborn, C.G.; Rofsky, N.M. MR Imaging–Transrectal US Fusion for Targeted Prostate Biopsies: Implications for Diagnosis and Clinical Management. RadioGraphics 2015, 35, 696–708. [Google Scholar] [CrossRef] [PubMed]
- Hale, G.R.; Czarniecki, M.; Cheng, A.; Bloom, J.B.; Seifabadi, R.; Gold, S.A.; Rayn, K.N.; Sabarwal, V.K.; Mehralivand, S.; Choyke, P.L.; et al. Comparison of Elastic and Rigid Registration during Magnetic Resonance Imaging/Ultrasound Fusion-Guided Prostate Biopsy: A Multi-Operator Phantom Study. J. Urol. 2018, 200, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Onofrey, J.A.; Staib, L.H.; Sarkar, S.; Venkataraman, R.; Nawaf, C.B.; Sprenkle, P.C.; Papademetris, X. Learning Non-rigid Deformations for Robust, Constrained Point-based Registration in Image-Guided MR-TRUS Prostate Intervention. Med. Image Anal. 2017, 39, 29–43. [Google Scholar] [CrossRef]
- Görtz, M.; Radtke, J.P.; Hatiboglu, G.; Schütz, V.; Tosev, G.; Güttlein, M.; Leichsenring, J.; Stenzinger, A.; Bonekamp, D.; Schlemmer, H.-P.; et al. The Value of Prostate-specific Antigen Density for Prostate Imaging-Reporting and Data System 3 Lesions on Multiparametric Magnetic Resonance Imaging: A Strategy to Avoid Unnecessary Prostate Biopsies. Eur. Urol. Focus 2021, 7, 325–331. [Google Scholar] [CrossRef]
- Bonekamp, D.; Schelb, P.; Wiesenfarth, M.; Kuder, T.A.; Deister, F.; Stenzinger, A.; Nyarangi-Dix, J.; Röthke, M.; Hohenfellner, M.; Schlemmer, H.-P.; et al. Histopathological to multiparametric MRI spatial mapping of extended systematic sextant and MR/TRUS-fusion-targeted biopsy of the prostate. Eur. Radiol. 2018, 29, 1820–1830. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Kuru, T.H.; Wadhwa, K.; Chang, R.T.M.; Echeverria, L.M.C.; Roethke, M.; Polson, A.; Rottenberg, G.; Koo, B.; Lawrence, E.M.; Seidenader, J.; et al. Definitions of terms, processes and a minimum dataset for transperineal prostate biopsies: A standardization approach of the Ginsburg Study Group for Enhanced Prostate Diagnostics. Br. J. Urol. 2013, 112, 568–577. [Google Scholar] [CrossRef]
- Radtke, J.P.; Schwab, C.; Wolf, M.B.; Freitag, M.T.; Alt, C.D.; Kesch, C.; Popeneciu, I.V.; Huettenbrink, C.; Gasch, C.; Klein, T.; et al. Multiparametric Magnetic Resonance Imaging (MRI) and MRI–Transrectal Ultrasound Fusion Biopsy for Index Tumor Detection: Correlation with Radical Prostatectomy Specimen. Eur. Urol. 2016, 70, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sopyllo, K.; Erickson, A.; Mirtti, T. Grading Evolution and Contemporary Prognostic Biomarkers of Clinically Significant Prostate Cancer. Cancers 2021, 13, 628. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.M.; Kasivisvanathan, V.; Eggener, S.; Emberton, M.; Fütterer, J.J.; Gill, I.S.; Iii, R.L.G.; Hadaschik, B.; Klotz, L.; Margolis, D.J.; et al. Standards of Reporting for MRI-targeted Biopsy Studies (START) of the Prostate: Recommendations from an International Working Group. Eur. Urol. 2013, 64, 544–552. [Google Scholar] [CrossRef]
- Siddiqui, M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/Ultrasound Fusion–Guided Biopsy With Ultrasound-Guided Biopsy for the Diagnosis of Prostate Cancer. JAMA J. Am. Med Assoc. 2015, 313, 390–397. [Google Scholar] [CrossRef]
- Cornud, F.; Roumiguié, M.; De Longchamps, N.B.; Ploussard, G.; Bruguière, E.; Portalez, D.; Malavaud, B. Precision Matters in MR Imaging–targeted Prostate Biopsies: Evidence from a Prospective Study of Cognitive and Elastic Fusion Registration Transrectal Biopsies. Radiology 2018, 287, 534–542. [Google Scholar] [CrossRef]
- Hansen, N.L.; Barrett, T.; Lloyd, T.; Warren, A.; Samel, C.; Bratt, O.; Kastner, C. Optimising the number of cores for magnetic resonance imaging -guided targeted and systematic transperineal prostate biopsy. BJU Int. 2020, 125, 260–269. [Google Scholar] [CrossRef] [Green Version]
- Tschirdewahn, S.; Wiesenfarth, M.; Bonekamp, D.; Püllen, L.; Reis, H.; Panic, A.; Kesch, C.; Darr, C.; Heß, J.; Giganti, F.; et al. Detection of Significant Prostate Cancer Using Target Saturation in Transperineal Magnetic Resonance Imaging/Transrectal Ultrasonography–fusion Biopsy. Eur. Urol. Focus 2020, 7, 1300–1307. [Google Scholar] [CrossRef]
- Sonmez, G.; Demirtas, T.; Tombul, S.T.; Ozturk, F.; Demirtas, A. What is the ideal number of biopsy cores per lesion in targeted prostate biopsy? Prostate Int. 2020, 8, 112–115. [Google Scholar] [CrossRef]
- Sokolakis, I.; Pyrgidis, N.; Koneval, L.; Krebs, M.; Thurner, A.; Kübler, H.; Hatzichristodoulou, G. Usability and diagnostic accuracy of different MRI/ultrasound-guided fusion biopsy systems for the detection of clinically significant and insignificant prostate cancer: A prospective cohort study. World J. Urol. 2021, 39, 4101–4108. [Google Scholar] [CrossRef]
- Halstuch, D.; Baniel, J.; Lifshitz, D.; Sela, S.; Ber, Y.; Margel, D. Characterizing the learning curve of MRI-US fusion prostate biopsies. Prostate Cancer Prostatic Dis. 2019, 22, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Calio, B.P.; Sidana, A.; Sugano, D.; Gaur, S.; Maruf, M.; Jain, A.L.; Merino, M.J.; Choyke, P.L.; Wood, B.J.; Pinto, P.A.; et al. Risk of Upgrading from Prostate Biopsy to Radical Prostatectomy Pathology—Does Saturation Biopsy of Index Lesion during Multiparametric Magnetic Resonance Imaging-Transrectal Ultrasound Fusion Biopsy Help? J. Urol. 2018, 199, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Gaziev, G.; Wadhwa, K.; Barrett, T.; Koo, B.C.; Gallagher, F.A.; Serrao, E.; Frey, J.; Seidenader, J.; Carmona, L.; Warren, A.; et al. Defining the learning curve for multiparametric magnetic resonance imaging (MRI) of the prostate using MRI-transrectal ultrasonography (TRUS) fusion-guided transperineal prostate biopsies as a validation tool. Br. J. Urol. 2014, 117, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Mager, R.; Brandt, M.P.; Borgmann, H.; Gust, K.M.; Haferkamp, A.; Kurosch, M. From novice to expert: Analyzing the learning curve for MRI-transrectal ultrasonography fusion-guided transrectal prostate biopsy. Int. Urol. Nephrol. 2017, 49, 1537–1544. [Google Scholar] [CrossRef]
- Gayet, M.; Van Der Aa, A.; Beerlage, H.P.; Schrier, B.P.; Mulders, P.F.A.; Wijkstra, H. The value of magnetic resonance imaging and ultrasonography (MRI/US)-fusion biopsy platforms in prostate cancer detection: A systematic review. Br. J. Urol. 2015, 117, 392–400. [Google Scholar] [CrossRef]
- Venderink, W.; de Rooij, M.; Sedelaar, J.M.; Huisman, H.J.; Fütterer, J.J. Elastic Versus Rigid Image Registration in Magnetic Resonance Imaging–transrectal Ultrasound Fusion Prostate Biopsy: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2018, 4, 219–227. [Google Scholar] [CrossRef]
- Arsov, C.; Rabenalt, R.; Blondin, D.; Quentin, M.; Hiester, A.; Godehardt, E.; Gabbert, H.E.; Becker, N.; Antoch, G.; Albers, P.; et al. Prospective Randomized Trial Comparing Magnetic Resonance Imaging (MRI)-guided In-bore Biopsy to MRI-ultrasound Fusion and Transrectal Ultrasound-guided Prostate Biopsy in Patients with Prior Negative Biopsies. Eur. Urol. 2015, 68, 713–720. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Dufour, R.; Moore, C.M.; Ahmed, H.U.; Abd-Alazeez, M.; Charman, S.C.; Freeman, A.; Allen, C.; Kirkham, A.; Van Der Meulen, J.; et al. Transperineal Magnetic Resonance Image Targeted Prostate Biopsy Versus Transperineal Template Prostate Biopsy in the Detection of Clinically Significant Prostate Cancer. J. Urol. 2013, 189, 860–866. [Google Scholar] [CrossRef]
- Ahdoot, M.; Wilbur, A.R.; Reese, S.E.; Lebastchi, A.H.; Mehralivand, S.; Gomella, P.; Bloom, J.; Gurram, S.; Siddiqui, M.; Pinsky, P.; et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N. Engl. J. Med. 2020, 382, 917–928. [Google Scholar] [CrossRef]
- Baco, E.; Ukimura, O.; Rud, E.; Vlatkovic, L.; Svindland, A.; Aron, M.; Palmer, S.; Matsugasumi, T.; Marien, A.; Bernhard, J.-C.; et al. Magnetic Resonance Imaging–Transectal Ultrasound Image-fusion Biopsies Accurately Characterize the Index Tumor: Correlation with Step-sectioned Radical Prostatectomy Specimens in 135 Patients. Eur. Urol. 2015, 67, 787–794. [Google Scholar] [CrossRef]
- Loeb, S.; Vellekoop, A.; Ahmed, H.U.; Catto, J.; Emberton, M.; Nam, R.; Rosario, D.J.; Scattoni, V.; Lotan, Y. Systematic Review of Complications of Prostate Biopsy. Eur. Urol. 2013, 64, 876–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Görtz, M.; Nyarangi-Dix, J.N.; Pursche, L.; Schütz, V.; Reimold, P.; Schwab, C.; Stenzinger, A.; Sültmann, H.; Duensing, S.; Schlemmer, H.-P.; et al. Impact of Surgeon’s Experience in Rigid versus Elastic MRI/TRUS-Fusion Biopsy to Detect Significant Prostate Cancer Using Targeted and Systematic Cores. Cancers 2022, 14, 886. https://doi.org/10.3390/cancers14040886
Görtz M, Nyarangi-Dix JN, Pursche L, Schütz V, Reimold P, Schwab C, Stenzinger A, Sültmann H, Duensing S, Schlemmer H-P, et al. Impact of Surgeon’s Experience in Rigid versus Elastic MRI/TRUS-Fusion Biopsy to Detect Significant Prostate Cancer Using Targeted and Systematic Cores. Cancers. 2022; 14(4):886. https://doi.org/10.3390/cancers14040886
Chicago/Turabian StyleGörtz, Magdalena, Joanne Nyaboe Nyarangi-Dix, Lars Pursche, Viktoria Schütz, Philipp Reimold, Constantin Schwab, Albrecht Stenzinger, Holger Sültmann, Stefan Duensing, Heinz-Peter Schlemmer, and et al. 2022. "Impact of Surgeon’s Experience in Rigid versus Elastic MRI/TRUS-Fusion Biopsy to Detect Significant Prostate Cancer Using Targeted and Systematic Cores" Cancers 14, no. 4: 886. https://doi.org/10.3390/cancers14040886
APA StyleGörtz, M., Nyarangi-Dix, J. N., Pursche, L., Schütz, V., Reimold, P., Schwab, C., Stenzinger, A., Sültmann, H., Duensing, S., Schlemmer, H.-P., Bonekamp, D., Hohenfellner, M., & Radtke, J. P. (2022). Impact of Surgeon’s Experience in Rigid versus Elastic MRI/TRUS-Fusion Biopsy to Detect Significant Prostate Cancer Using Targeted and Systematic Cores. Cancers, 14(4), 886. https://doi.org/10.3390/cancers14040886