
The Association between Patient Characteristics and the Efficacy and Safety of Selinexor in Diffuse Large B-Cell Lymphoma in the SADAL Study

 , ,
, ,  , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Endpoints
2.3. Baseline Characteristics
2.4. Statistical Analyses
3. Results
3.1. Demographics
3.2. Duration of Selinexor Treatment
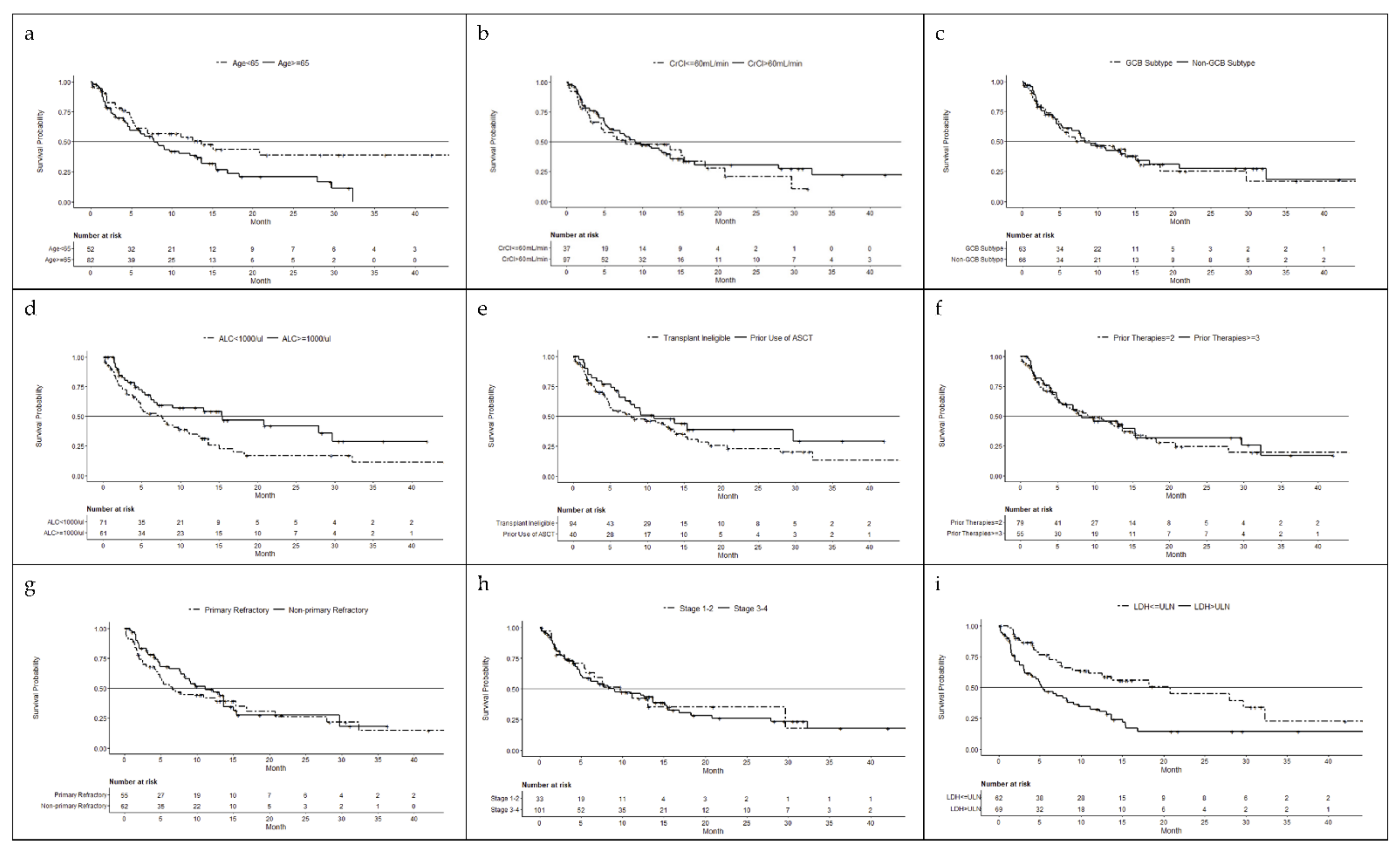
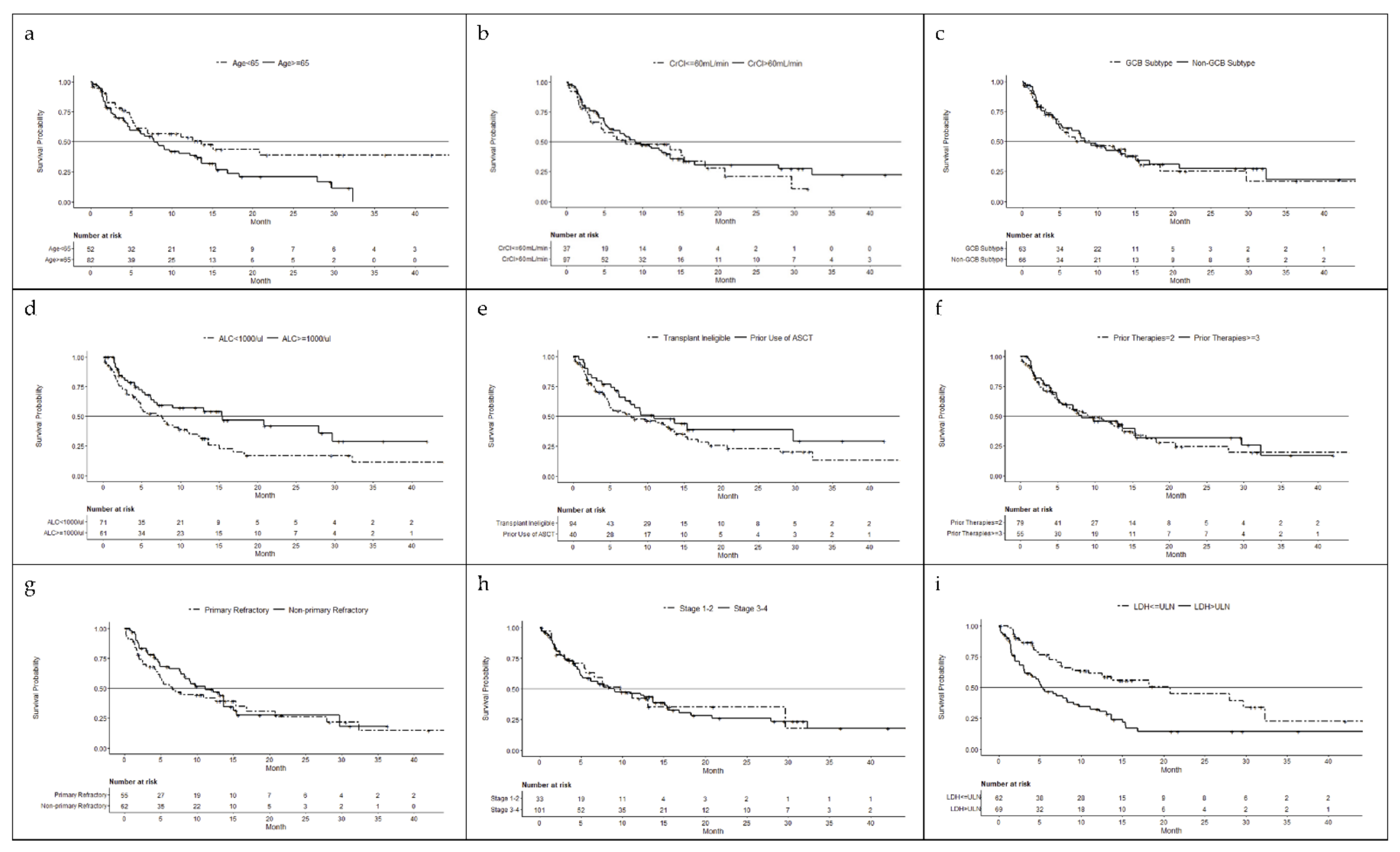
3.3. Efficacy
3.3.1. Age
3.3.2. Renal Function
3.3.3. Germinal Center B-Cell versus Non-Germinal Center B-cell
3.3.4. Absolute Lymphocyte Count
3.3.5. Prior ASCT vs. Transplant Ineligible
3.3.6. Prior Therapy
3.3.7. Disease Refractory Status
3.3.8. Ann Arbor Stage 1 or 2 vs. 3 or 4
3.3.9. Lactate Dehydrogenase >ULN vs. ≤ULN
3.4. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stewart, B.W.; Wild, C.P. (Eds.) World Cancer Report 2014; World Health Organization, International Agency for Research on Cancer, WHO Press: Geneva, Switzerland, 2015; Available online: http://publications.iarc.fr/Non-Series-Publications/World-Cancer-Reports/World-Cancer-Report-2014 (accessed on 22 October 2020).
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. (Eds.) SEER Cancer Statistics Review, 1975–2017; National Cancer Institute: Bethesda, MD, USA, 2020. Available online: https://seer.cancer.gov/statfacts/html/dlbcl.html (accessed on 22 October 2020).
- Pfreundschuh, M.; Trümper, L.; Österborg, A.; Pettengell, R.; Trneny, M.; Imrie, K.; Ma, D.; Gill, D.; Walewski, J.; Zinzani, P.L.; et al. CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: A randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol. 2006, 7, 379–391. [Google Scholar] [CrossRef]
- Coiffier, B.; Lepage, E.; Brière, J.; Herbrecht, R.; Tilly, H.; Bouabdallah, R.; Morel, P.; Van Den Neste, E.; Salles, G.; Gaulard, P.; et al. CHOP Chemotherapy plus Rituximab Compared with CHOP Alone in Elderly Patients with Diffuse Large-B-Cell Lymphoma. N. Engl. J. Med. 2002, 346, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Feugier, P.; Van Hoof, A.; Sebban, C.; Solal-Celigny, P.; Bouabdallah, R.; Fermé, C.; Christian, B.; Lepage, E.; Tilly, H.; Morschhauser, F.; et al. Long-Term Results of the R-CHOP Study in the Treatment of Elderly Patients with Diffuse Large B-Cell Lymphoma: A Study by the Groupe d’Etude des Lymphomes de l’Adulte. J. Clin. Oncol. 2005, 23, 4117–4126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- KYMRIAH (Tisagenlecleucel) Prescribing Information; Novartis Pharmaceuticals Corporation: East Hanover, NJ, USA, 2018.
- YESCARTA (Axicabtagene Ciloleucel) Prescribing Information; Kite Pharma: Santa Monica, CA, USA, 2019.
- Conforti, F.; Wang, Y.; Rodriguez, J.A.; Alberobello, A.T.; Zhang, Y.W.; Giaccone, G. Molecular pathways: Anticancer activity by inhibition of nucleocytoplasmic shuttling. Clin. Cancer Res. 2015, 21, 4508–4513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, D.S.; Bedard, P.L.; Kuruvilla, J.; Siu, L.L.; Razak, A.R. Promising SINEs for embargoing nuclear-cytoplasmic export as an anticancer strategy. Cancer Discov. 2014, 4, 527–537. [Google Scholar] [CrossRef] [Green Version]
- Okamura, M.; Inose, H.; Masuda, S. RNA export through the NPC in eukaryotes. Genes 2015, 6, 124–149. [Google Scholar] [CrossRef]
- Luo, B.; Huang, L.; Gu, Y.; Li, C.; Lu, H.; Chen, G.; Peng, Z.; Feng, Z. Expression of exportin-1 in diffuse large B-cell lymphoma: Immunohistochemistry and TCGA analyses. Int. J. Clin. Exp. Pathol. 2018, 11, 5547–5560, Erratum in Int. J. Clin. Exp. Pathol. 2019, 12, 2817–2818. [Google Scholar]
- Sendino, M.; Omaetxebarria, M.J.; Rodriguez, J.A. Hitting a moving target: Inhibition of the nuclear export receptor XPO1/CRM1 as a therapeutic approach in cancer. Cancer Drug. Resist. 2018, 1, 139–163. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, U.H.; Senapedis, W.; Baloglu, E.; Unger, T.J.; Chari, A.; Vogl, D.; Cornell, R.F. Clinical Implications of Targeting XPO1-mediated Nuclear Export in Multiple Myeloma. Clin. Lymphoma Myeloma Leuk. 2018, 18, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Han, X.; Wang, J.; Shen, Y.; Zhang, N.; Wang, S.; Yao, J.; Shi, Y. CRM1 as a new therapeutic target for non-Hodgkin lymphoma. Leuk. Res. 2015, 39, 38–46. [Google Scholar] [CrossRef]
- Culjkovic-Kraljacic, B.; Baguet, A.; Volpon, L.; Amri, A.; Borden, K.L. The oncogene eIF4E reprograms the nuclear pore complex to promote mRNA export and oncogenic transformation. Cell Rep. 2012, 2, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Parikh, K.; Cang, S.; Sekhri, A.; Liu, D. Selective inhibitors of nuclear export (SINE)—A novel class of anti-cancer agents. J. Hematol. Oncol. 2014, 7, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camus, V.; Miloudi, H.; Taly, A.; Sola, B.; Jardin, F. XPO1 in B cell hematological malignancies: From recurrent somatic mutations to targeted therapy. J. Hematol. Oncol. 2017, 10, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, R.; Cautain, B.; de Pedro, N.; Link, W. Targeting nucleocytoplasmic transport in cancer therapy. Oncotarget 2014, 5, 11–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalakonda, N.; Maerevoet, M.; Cavallo, F.; Follows, G.; Goy, A.; Vermaat, J.S.P.; Casasnovas, O.; Hamad, N.; Zijlstra, J.M.; Bakhshi, S.; et al. Selinexor in patients with relapsed or refractory diffuse large B-cell lymphoma (SADAL): A single-arm, multinational, multicentre, open-label, phase 2 trial. Lancet Haematol. 2020, 7, e511–e522. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Food and Drug Administration 2020. FDA Approves Selinexor for Relapsed/Refractory Diffuse Large B-Cell Lymphoma. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-selinexor-relapsedrefractory-diffuse-large-b-cell-lymphoma (accessed on 15 January 2021).
- Porrata, L.F.; Ristow, K.; Haberman, T.M.; Witzig, T.E.; Inwards, D.J.; Ansell, S.M.; Johnston, P.B.; Micallef, I.N.; Colgan, J.P.; White, W.L.; et al. Absolute Lymphocyte Count at the Time of Relapse Predicts Survival in Patients with Diffuse Large B-Cell Lymphoma. Blood 2008, 112, 1763. [Google Scholar] [CrossRef]
- Karyopharm Therapeutics Inc. XPOVIO (Selinexor) Prescribing Information; Karyopharm Therapeutics Inc.: Newton, MA, USA, 2020. [Google Scholar]
- Kobayashi, Y.; Miura, K.; Hojo, A.; Hatta, Y.; Tanaka, T.; Kurita, D.; Iriyama, N.; Kobayashi, S.; Takeuchi, J. Charlson Comorbidity Index is an independent prognostic factor among elderly patients with diffuse large B-cell lymphoma. J. Cancer Res. Clin. Oncol. 2011, 137, 1079–1084. [Google Scholar] [CrossRef]
- Nishimura, N.; Fukuta, T.; Nishihara, A.; Shirouchi, Y.; Uryu, H.; Inoue, N.; Kusano, Y.; Tsuyama, N.; Takeuchi, K.; Mishima, Y.; et al. Impact of creatinine clearance in patients with diffuse large B-cell lymphoma treated with R-CHOP: A real-world long-term observation analysis at a single institute. Blood 2018, 132 (Suppl. S1), 5399. [Google Scholar] [CrossRef]
- Casasnovas, R.O.; Follows, G.; Zijlstra, J.M.; Vermaat, J.S.; Kalakonda, N.; Choquet, S.; Van Den Neste, E.; Hill, B.; Thieblemont, C.; Cavallo, F.; et al. Comparison of the effectiveness and safety of the oral selective inhibitor of nuclear export, selinexor, in diffuse large B cell lymphoma subtypes. Clin. Lymphoma Myeloma Leuk. 2021, 22, 24–33. [Google Scholar] [CrossRef]
- Oki, Y.; Yamamoto, K.; Kato, H.; Kuwatsuka, Y.; Taji, H.; Kagami, Y.; Morishima, Y. Low absolute lymphocyte count is a poor prognostic marker in patients with diffuse large B-cell lymphoma and suggests patients’ survival benefit from rituximab. Eur. J. Haematol. 2008, 81, 448–453. [Google Scholar] [CrossRef]
- Prochazka, V.; Trneny, M.; Salek, D.; Belada, D.; Kozak, T.; Papajik, T.; Pytlik, R.; Vasova, I.; Sykorova, A.; Jankovska, M.; et al. Median absolute lymphocyte count independently predicts survival of elderly patients with diffuse large B-cell lymphoma treated with R-chemotherapy: Analysis of 651 patients included in the Czech Lymphoma Project. Blood 2010, 116, 2882. [Google Scholar] [CrossRef]
- Panizo, C.; Rodríguez, A.J.; Gutiérrez, G.; Díaz, F.J.; González-Barca, E.; De Oña, R.; Grande, C.; Sancho, J.M.; García-Álvarez, M.F.; Sánchez-González, B.; et al. Evaluation of clinical and biological prognostic factors in relapsed or refractory diffuse large B-cell lymphoma patients after previous treatment with rituximab and chemotherapy: Results of the PRO-R-IPI study. Clin. Lymphoma Myeloma Leuk. 2015, 15, 398–403. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Center for Drug Evaluation and Research. Application No. 761163Orig1s000 Monjuvi. 24 July 2019. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2020/761163Orig1s000MultidisciplineR.pdf (accessed on 6 October 2021).
- Crump, M.; Neelapu, S.S.; Farooq, U.; Neste, E.V.D.; Kuruvilla, J.; Westin, J.; Link, B.K.; Hay, A.; Cerhan, J.R.; Zhu, L.; et al. Outcomes in refractory diffuse large B-cell lymphoma: Results from the international SCHOLAR-1 study. Blood 2017, 130, 1800–1808. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Age | CrCl | ALC a | Transplant | Stage of Disease | LDH b | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <65 years (n = 52) | ≥65 years (n = 82) | ≤60 mL/min (n = 37) | >60 mL/min (n = 97) | <1000/µL (n = 71) | ≥1000/µL (n = 61) | Prior ASCT (n = 40) | Transplant Ineligible (n = 94) | 1 or 2 (n = 33) | 3 or 4 (n = 101) | >ULN (n = 69) | ≤ULN (n = 62) | (N = 134) | |
| Median age, years (min, max) | 57 (35, 64) | 73 (65, 91) | 74 (52, 91) | 65 (35, 83) | 67 (35, 91) | 67 (44, 87) | 64 (41, 77) | 69.5 (35, 91) | 70 (35, 87) | 67 (41, 91) | 65 (35, 86) | 69 (41, 91) | 67 (35, 91) |
| ≥70, n (%) | 0 | 60 (73.2) | 26 (70.3) | 34 (35.1) | 33 (46.5) | 26 (42.6) | 13 (32.5) | 47 (50.0) | 18 (54.5) | 42 (41.6) | 30 (43.5) | 30 (48.4) | 60 (44.8) |
| Male, n (%) | 32 (61.5) | 47 (57.3) | 14 (37.8) | 65 (67.0) | 43 (60.6) | 35 (57.4) | 27 (67.5) | 52 (55.3) | 15 (45.5) | 64 (63.4) | 41 (59.4) | 37 (59.7) | 79 (59.0) |
| DLBCL subtype, n (%) | |||||||||||||
| GCB | 28 (53.8) | 35 (42.7) | 15 (40.5) | 48 (49.5) | 31 (43.7) | 31 (50.8) | 25 (62.5) | 38 (40.4) | 15 (45.5) | 48 (47.5) | 33 (47.8) | 28 (45.2) | 63 (47.0) |
| Non-GCB | 21 (40.4) | 45 (54.9) | 21 (56.8) | 45 (46.4) | 39 (54.9) | 26 (42.6) | 13 (32.5) | 53 (56.4) | 17 (51.5) | 49 (48.5) | 35 (50.7) | 30 (48.4) | 66 (49.3) |
| Non-classified | 3 (5.8) | 2 (2.4) | 1 (2.7) | 4 (4.1) | 1 (1.4) | 4 (6.6) | 2 (5.0) | 3 (3.2) | 1 (3.0) | 4 (4.0) | 1 (1.4) | 4 (6.5) | 5 (3.7) |
| No. prior regimens | |||||||||||||
| Median (min, max) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) | 2 (2, 5) |
| 2, n (%) | 30 (57.7) | 49 (59.8) | 21 (56.8) | 58 (59.8) | 44 (62.0) | 34 (55.7) | 21 (52.5) | 58 (61.7) | 19 (57.6) | 60 (59.4) | 40 (58.0) | 37 (59.7) | 79 (59.0) |
| 3, n (%) | 13 (25.0) | 20 (24.4) | 12 (32.4) | 21 (21.6) | 15 (21.1) | 17 (27.9) | 14 (35.0) | 19 (20.2) | 8 (24.2) | 25 (24.8) | 19 (27.5) | 13 (21.0) | 33 (24.6) |
| 4, n (%) | 6 (11.5) | 10 (12.2) | 3 (8.1) | 13 (13.4) | 9 (12.7) | 7 (11.5) | 3 (7.5) | 13 (13.8) | 4 (12.1) | 12 (11.9) | 7 (10.1) | 9 (14.5) | 16 (11.9) |
| 5, n (%) | 3 (5.8) | 3 (3.7) | 1 (2.7) | 5 (5.2) | 3 (4.2) | 3 (4.9) | 2 (5.0) | 4 (4.3) | 2 (6.1) | 4 (4.0) | 3 (4.3) | 3 (4.8) | 6 (4.5) |
| Prior ASCT, n (%) | 32 (61.5) | 31 (37.8) | 13 (35.1) | 50 (51.5) | 24 (33.8) | 37 (60.7) | 40 (100) | 0 | 9 (27.3) | 31 (30.7) | 17 (24.6) | 23 (37.1) | 40 (29.9) |
| Refractory Status c | |||||||||||||
| Primary, n (%) | 22 (42.3) | 33 (40.2) | 15 (40.5) | 40 (41.2) | 27 (38.0) | 28 (45.9) | 11 (27.5) | 44 (46.8) | 11 (33.3) | 44 (43.6) | 27 (43.6) | 26 (37.7) | 55 (41.0) |
| Non-primary refractory, n (%) | 23 (44.2) | 39 (47.6) | 16 (43.2) | 46 (47.4) | 34 (47.9) | 26 (42.6) | 23 (57.5) | 39 (41.5) | 17 (51.5) | 45 (44.6) | 26 (41.9) | 36 (52.2) | 62 (46.3) |
| ORR a | DOR b | PFS | OS b | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | No. Patients | n (%) | p-Value | Median Months | p-Value | Median Months | p-Value | Median Months | p-Value | Multivariate Analysis p-Value/HR (95%CI) |
| Overall | 134 | 39 (29.1) | -- | 9.3 | -- | 2.6 | 9.0 | |||
| Age | -- | |||||||||
| <65 years | 52 | 19 (36.5) | 0.19 | 9.7 | 0.94 | 3.6 | 0.91 | 13.7 | 0.04 | 0.03/1.7 (1.05,2.78) |
| ≥65 years | 82 | 20 (24.4) | 9.2 | 2.3 | 7.8 | |||||
| CrCl | ||||||||||
| ≤60 mL/min | 37 | 11 (29.7) | 1.00 | 23.0 | 0.24 | 3.5 | 0.66 | 7.8 | 0.59 | |
| >60 mL/min | 97 | 28 (28.9) | 9.2 | 2.3 | 9.1 | |||||
| DLBCL Subtype | ||||||||||
| GCB | 63 | 20 (31.7) | 0.45 | 23 | 0.39 | 3.6 | 0.105 | 9.0 | 0.836 | |
| Non-GCB | 66 | 16 (24.2) | 9.3 | 2.1 | 8.3 | |||||
| Lymphocyte c | ||||||||||
| <1000/µL | 71 | 18 (25.4) | 0.45 | 4.9 | 0.23 | 2.1 | 0.13 | 7.6 | 0.01 | 0.07/1.56 (0.97,251) |
| ≥1000/µL | 61 | 20 (32.8) | 23 | 3.6 | 15.5 | |||||
| Transplant | ||||||||||
| Prior ASCT | 40 | 17 (42.5) | 0.04 | 8.4 | 0.93 | 4.6 | 0.17 | 10.9 | 0.18 | |
| Transplant ineligible | 94 | 22 (23.4) | 9.7 | 2.1 | 7.8 | |||||
| No. Prior Therapies | ||||||||||
| 2 | 79 | 22 (27.8) | 0.85 | 10.4 | 0.40 | 3.7 | 0.35 | 9.1 | 0.76 | |
| ≥3 | 55 | 17 (30.9) | 8.4 | 2.1 | 8.2 | |||||
| Refractory Status d | ||||||||||
| Primary | 55 | 12 (21.8) | 0.11 | 10.4 | 0.75 | 1.9 | 0.02 | 6.6 | 0.46 | |
| Non-primary refractory | 62 | 23 (37.1) | 4.9 | 3.8 | 11.1 | |||||
| Ann Arbor Stage | ||||||||||
| 1 or 2 | 33 | 10 (30.3) | 1.00 | NR | 0.003 | 4.0 | 0.04 | 9.8 | 0.91 | |
| 3 or 4 | 101 | 29 (28.7) | 4.9 | 2.3 | 9.0 | |||||
| LDH e | ||||||||||
| ≤ULN | 62 | 26 (41.9) | 0.004 | 10.4 | 0.98 | 3.8 | 0.004 | 20.8 | <0.001 | <0.001/2.35 (1.45,3.79) |
| >ULN | 69 | 12 (17.4) | 9.7 | 1.9 | 5.4 | |||||
| Adverse Event | Age (Years) | Transplant | Total | ||
|---|---|---|---|---|---|
| <65 | ≥65 | Prior ASCT | Transplant Ineligible | (N = 134) | |
| n (%) | n (%) | n (%) | |||
| Patients with ≥1 AE | 51 (98.1) | 81 (98.8) | 40 (100.0) | 92 (97.9) | 132 (98.5) |
| Thrombocytopenia | 36 (69.2) | 46 (56.1) | 35 (87.5) | 47 (50.0) | 82 (61.2) |
| Nausea | 28 (53.8) | 48 (58.5) | 25 (62.5) | 51 (54.3) | 76 (56.7) |
| Fatigue | 24 (46.2) | 39 (47.6) | 22 (55.0) | 41 (43.6) | 63 (47.0) |
| Anaemia | 23 (44.2) | 34 (41.5) | 19 (47.5) | 38 (40.4) | 57 (42.5) |
| Decreased appetite | 18 (34.6) | 31 (37.8) | 15 (37.5) | 34 (36.2) | 49 (36.6) |
| Diarrhoea | 15 (28.8) | 31 (37.8) | 19 (47.5) | 27 (28.7) | 46 (34.3) |
| Neutropenia | 18 (34.6) | 24 (29.3) | 16 (40.0) | 26 (27.7) | 42 (31.3) |
| Constipation | 17 (32.7) | 23 (28.0) | 16 (40.0) | 24 (25.5) | 40 (29.9) |
| Weight decreased | 13 (25.0) | 27 (32.9) | 12 (30.0) | 28 (29.8) | 40 (29.9) |
| Vomiting | 11 (21.2) | 27 (32.9) | 11 (27.5) | 27 (28.7) | 38 (28.4) |
| Pyrexia | 12 (23.1) | 17 (20.7) | 9 (22.5) | 20 (21.3) | 29 (21.6) |
| Asthenia | 8 (15.4) | 20 (24.4) | 8 (20.0) | 20 (21.3) | 28 (20.9) |
| Cough | 10 (19.2) | 14 (17.1) | 8 (20.0) | 16 (17.0) | 24 (17.9) |
| Dizziness | 7 (13.5) | 12 (14.6) | 5 (12.5) | 14 (14.9) | 19 (14.2) |
| Upper respiratory tract infection | 10 (19.2) | 9 (11.0) | 6 (15.0) | 13 (13.8) | 19 (14.2) |
| Hypotension | 7 (13.5) | 10 (12.2) | 7 (17.5) | 10 (10.6) | 17 (12.7) |
| Oedema peripheral | 3 (5.8) | 13 (15.9) | 5 (12.5) | 11 (11.7) | 16 (11.9) |
| Hyponatraemia | 5 (9.6) | 10 (12.2) | 2 (5.0) | 13 (13.8) | 15 (11.2) |
| Dyspnoea | 5 (9.6) | 9 (11.0) | 3 (7.5) | 11 (11.7) | 14 (10.4) |
| Variable | No. of Patients | Dose Reduction n (%) | Dose Interruption/Withheld n (%) | Duration of Selinexor Treatment Median Weeks (min, max) |
|---|---|---|---|---|
| Overall | 134 | 65 (48.5%) | 86 (64.2%) | 9 (1, 193) |
| Age | ||||
| <65 years | 52 | 26 (50.0%) | 31 (59.6%) | 13.5 (1, 193) |
| ≥65 years | 82 | 39 (47.6%) | 55 (67.1%) | 8 (1, 124) |
| CrCl | ||||
| ≤60 mL/min | 37 | 17 (45.9) | 25 (67.6) | 8 (1, 124) |
| >60 mL/min | 97 | 48 (49.5) | 61 (62.9) | 9 (1, 193) |
| DLBCL Subtype | ||||
| GCB | 63 | 28 (44.4) | 40 (63.5) | 10 (1, 193) |
| non-GCB | 66 | 33 (50.0) | 43 (65.2) | 8 (1, 183) |
| Lymphocyte | ||||
| <1000/µL | 71 | 239 (40.8) | 50 (70.4) | 9 (1, 193) |
| ≥1000/µL | 61 | 34 (55.7) | 34 (55.7) | 9 (1, 183) |
| Transplant | ||||
| Prior ASCT | 40 | 26 (65.0) | 30 (75.0) | 16 (1, 183) |
| Transplant ineligible | 94 | 39 (41.5) | 56 (59.6) | 9 (1, 193) |
| No. Prior Therapies | ||||
| 2 | 79 | 38 (48.1) | 53 (67.1) | 9 (1, 193) |
| ≥3 | 55 | 27 (49.1) | 33 (60.0) | 8 (2, 183) |
| Refractory Status a | ||||
| Primary refractory | 55 | 25 (45.5) | 35 (63.6) | 9 (1, 183) |
| Non-primary refractory | 62 | 32 (51.6) | 45 (72.6) | 11 (1, 124) |
| Ann Arbor Stage | ||||
| 1 or 2 | 33 | 20 (60.6) | 22 (66.7) | 9 (1, 183) |
| 3 or 4 | 101 | 45 (44.6) | 64 (63.4) | 9 (1, 193) |
| LDH b | ||||
| ≤ULN | 62 | 37 (59.7) | 45 (72.6) | 15 (1, 193) |
| >ULN | 69 | 27 (39.1) | 41 (59.4) | 6 (1, 95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zijlstra, J.M.; Follows, G.; Casasnovas, R.-O.; Vermaat, J.S.P.; Kalakonda, N.; Choquet, S.; Hill, B.; Thieblemont, C.; Cavallo, F.; Cruz, F.D.l.; et al. The Association between Patient Characteristics and the Efficacy and Safety of Selinexor in Diffuse Large B-Cell Lymphoma in the SADAL Study. Cancers 2022, 14, 791. https://doi.org/10.3390/cancers14030791
Zijlstra JM, Follows G, Casasnovas R-O, Vermaat JSP, Kalakonda N, Choquet S, Hill B, Thieblemont C, Cavallo F, Cruz FDl, et al. The Association between Patient Characteristics and the Efficacy and Safety of Selinexor in Diffuse Large B-Cell Lymphoma in the SADAL Study. Cancers. 2022; 14(3):791. https://doi.org/10.3390/cancers14030791
Chicago/Turabian StyleZijlstra, Josée M., George Follows, Rene-Olivier Casasnovas, Joost S. P. Vermaat, Nagesh Kalakonda, Sylvain Choquet, Brian Hill, Catherine Thieblemont, Federica Cavallo, Fatima De la Cruz, and et al. 2022. "The Association between Patient Characteristics and the Efficacy and Safety of Selinexor in Diffuse Large B-Cell Lymphoma in the SADAL Study" Cancers 14, no. 3: 791. https://doi.org/10.3390/cancers14030791
APA StyleZijlstra, J. M., Follows, G., Casasnovas, R.-O., Vermaat, J. S. P., Kalakonda, N., Choquet, S., Hill, B., Thieblemont, C., Cavallo, F., Cruz, F. D. l., Kuruvilla, J., Hamad, N., Jaeger, U., Caimi, P., Gurion, R., Warzocha, K., Bakhshi, S., Sancho, J.-M., Schuster, M., ... Maerevoet, M. (2022). The Association between Patient Characteristics and the Efficacy and Safety of Selinexor in Diffuse Large B-Cell Lymphoma in the SADAL Study. Cancers, 14(3), 791. https://doi.org/10.3390/cancers14030791