
Risk Factors for Female Breast Cancer: A Population Cohort Study



Simple Summary
Abstract
1. Introduction
2. Materials and Methods
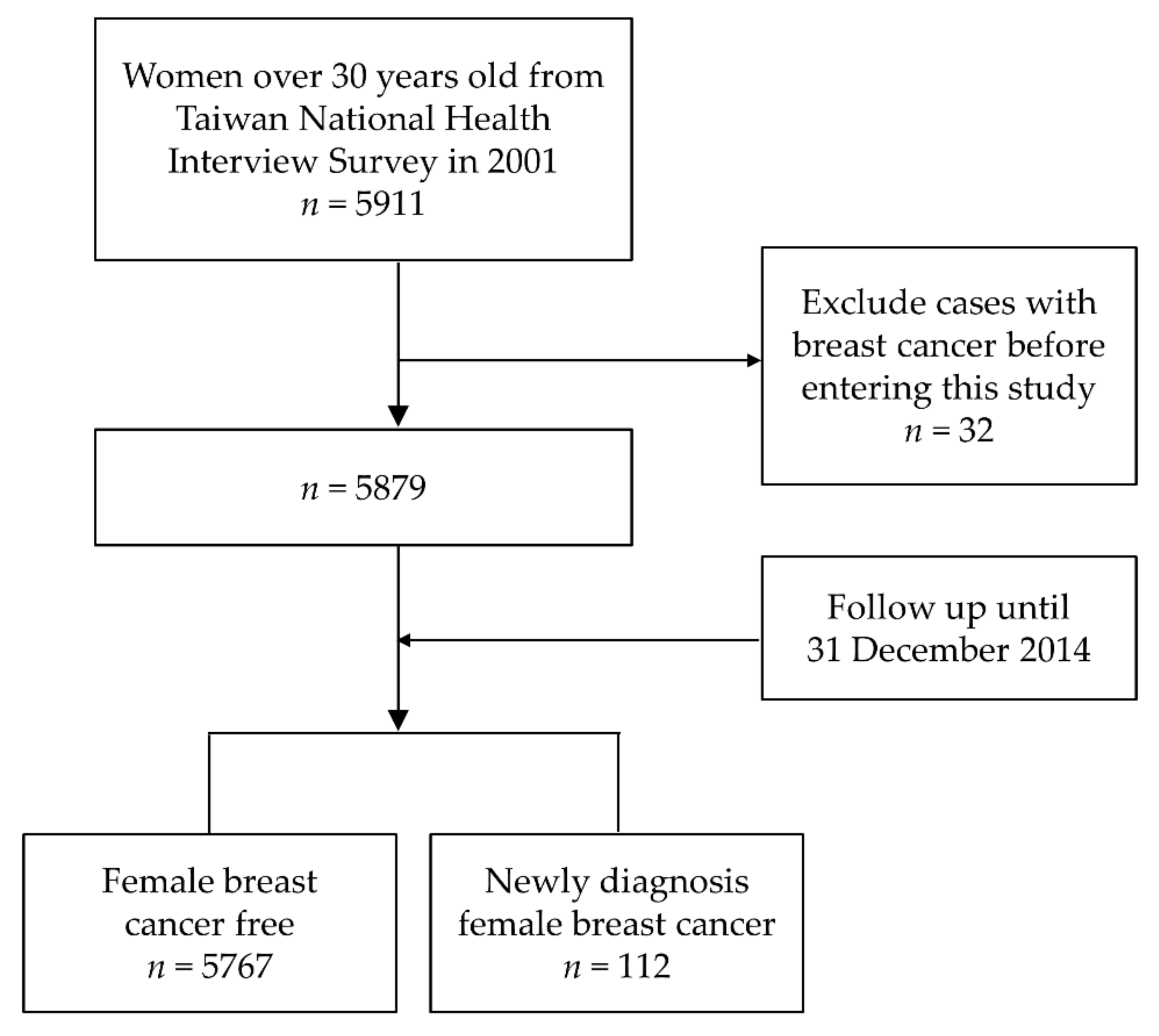
2.1. Study Cohort and Baseline Characteristics
2.2. Follow-Up and Determination of Female Breast Cancer
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 2 September 2019).
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The Global Burden of Cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef] [PubMed]
- Golubnitschaja, O.; Debald, M.; Yeghiazaryan, K.; Kuhn, W.; Pesta, M.; Costigliola, V.; Grech, G. Breast cancer epidemic in the early twenty-first century: Evaluation of risk factors, cumulative questionnaires and recommendations for preventive measures. Tumor Biol. 2016, 37, 12941–12957. [Google Scholar] [CrossRef] [PubMed]
- Stuckey, A. Breast cancer: Epidemiology and risk factors. Clin. Obstet. Gynecol. 2011, 54, 96–102. [Google Scholar] [CrossRef]
- Hayes, J.; Richardson, A.; Frampton, C. Population attributable risks for modifiable lifestyle factors and breast cancer in New Zealand women. Intern. Med. J. 2013, 43, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- McPherson, K.; Steel, C.M.; Dixon, J.M. ABC of breast diseases. Breast cancer-epidemiology, risk factors, and genetics. BMJ 2000, 321, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Tamakoshi, K.; Yatsuya, H.; Wakai, K.; Suzuki, S.; Nishio, K.; Lin, Y.; Niwa, Y.; Kondo, T.; Yamamoto, A.; Tokudome, S.; et al. Impact of menstrual and reproductive factors on breast cancer risk in Japan: Results of the JACC study. Cancer Sci. 2005, 96, 57–62. [Google Scholar] [CrossRef]
- Kawai, M.; Minami, Y.; Kuriyama, S.; Kakizaki, M.; Kakugawa, Y.; Nishino, Y.; Ishida, T.; Fukao, A.; Tsuji, I.; Ohuchi, N. Reproductive factors, exogenous female hormone use and breast cancer risk in Japanese: The Miyagi Cohort Study. Cancer Causes Control 2010, 21, 135–145. [Google Scholar] [CrossRef]
- Beral, V.; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet 2003, 362, 419–427. [Google Scholar] [CrossRef]
- Romieu, I.; Scoccianti, C.; Chajes, V.; de Batlle, J.; Biessy, C.; Dossus, L.; Baglietto, L.; Clavel-Chapelon, F.; Overvad, K.; Olsen, A.; et al. Alcohol intake and breast cancer in the European prospective investigation into cancer and nutrition. Int. J. Cancer 2015, 137, 1921–1930. [Google Scholar] [CrossRef]
- Luo, J.; Margolis, K.L.; Wactawski-Wende, J.; Horn, K.; Messina, C.; Stefanick, M.L.; Tindle, H.A.; Tong, E.; Rohan, T.E. Association of active and passive smoking with risk of breast cancer among postmenopausal women: A prospective cohort study. BMJ 2011, 342, d1016. [Google Scholar] [CrossRef]
- Sieri, S.; Krogh, V.; Ferrari, P.; Berrino, F.; Pala, V.; Thiebaut, A.C.; Tjonneland, A.; Olsen, A.; Overvad, K.; Jakobsen, M.U.; et al. Dietary fat and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition. Am. J. Clin. Nutr. 2008, 88, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.J.; Wu, W.Y.; Yen, A.M.; Fann, J.C.; Chen, S.L.; Chiu, S.Y.; Chen, H.H.; Chiou, S.T. Body mass index and breast cancer: Analysis of a nation-wide population-based prospective cohort study on 1,393,985 Taiwanese women. Int. J. Obes. 2016, 40, 524–530. [Google Scholar] [CrossRef] [PubMed]
- McTiernan, A.; Kooperberg, C.; White, E.; Wilcox, S.; Coates, R.; Adams-Campbell, L.L.; Woods, N.; Ockene, J.; Women’s Health Initiative Cohort Study. Recreational physical activity and the risk of breast cancer in postmenopausal women: The Women’s Health Initiative Cohort Study. JAMA 2003, 290, 1331–1336. [Google Scholar] [CrossRef]
- Lynch, B.M. Sedentary behavior and cancer: A systematic review of the literature and proposed biological mechanisms. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2691–2709. [Google Scholar] [CrossRef] [PubMed]
- Chuang, S.C.; Wu, G.J.; Lu, Y.S.; Lin, C.H.; Hsiung, C.A. Associations between Medical Conditions and Breast Cancer Risk in Asians: A Nationwide Population-Based Study in Taiwan. PLoS ONE 2015, 10, e0143410. [Google Scholar] [CrossRef]
- Chang, H.Y.; Chiou, C.J.; Lin, M.C.; Lin, S.H.; Tai, T.Y. A population study of the self-care behaviors and their associated factors of diabetes in Taiwan: Results from the 2001 National Health Interview Survey in Taiwan. Prev. Med. 2005, 40, 344–348. [Google Scholar] [CrossRef]
- Health Promotion Administration. National Health Interview Survey. Taiwan. Available online: https://www.hpa.gov.tw/Pages/List.aspx?nodeid=106 (accessed on 22 January 2021).
- Stanford, J.L.; Hartge, P.; Brinton, L.A.; Hoover, R.N.; Brookmeyer, R. Factors influencing the age at natural menopause. J. Chronic Dis. 1987, 40, 995–1002. [Google Scholar] [CrossRef]
- Wang, C.Y.; Shih, S.R.; Huang, K.C. Increasing risk of diabetes mellitus in postmenopausal women with newly diagnosed primary breast cancer. J. Diabetes Investig. 2020, 11, 490–498. [Google Scholar] [CrossRef]
- Wu, T.Y.; Majeed, A.; Kuo, K.N. An overview of the healthcare system in Taiwan. Lond. J. Prim. Care 2010, 3, 115–119. [Google Scholar] [CrossRef]
- Cheng, T.M. Reflections on the 20th anniversary of Taiwan’s single-payer National Health Insurance System. Health Aff. 2015, 34, 502–510. [Google Scholar] [CrossRef]
- National Health Insurance Administration. National Health Insurance Annual Report 2017–2018; Ministry of Health and Welfare: Taipei, Taiwan, 2017.
- Lin, T.T.; Yang, Y.H.; Liao, M.T.; Tsai, C.T.; Hwang, J.J.; Chiang, F.T.; Chen, P.C.; Lin, J.L.; Lin, L.Y. Primary prevention of atrial fibrillation with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in patients with end-stage renal disease undergoing dialysis. Kidney Int. 2015, 88, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.M.; Chuang, Y.W.; Yu, M.C.; Chen, C.H.; Yang, C.K.; Huang, S.T.; Lin, C.L.; Shu, K.H.; Kao, C.H. Risk of cancer in patients with polycystic kidney disease: A propensity-score matched analysis of a nationwide, population-based cohort study. Lancet Oncol. 2016, 17, 1419–1425. [Google Scholar] [CrossRef]
- Lu, T.H.; Lee, M.C.; Chou, M.C. Accuracy of cause-of-death coding in Taiwan: Types of miscoding and effects on mortality statistics. Int. J. Epidemiol. 2000, 29, 336–343. [Google Scholar] [CrossRef]
- Health Promotion Administration. Cancer Registry Annual Report. Taiwan. 2014. Available online: https://www.hpa.gov.tw/Pages/ashx/File.ashx?FilePath=~/File/Attach/7330/File_6792.pdf (accessed on 20 February 2021).
- Nishio, K.; Niwa, Y.; Toyoshima, H.; Tamakoshi, K.; Kondo, T.; Yatsuya, H.; Yamamoto, A.; Suzuki, S.; Tokudome, S.; Lin, Y.; et al. Consumption of soy foods and the risk of breast cancer: Findings from the Japan Collaborative Cohort (JACC) Study. Cancer Causes Control 2007, 18, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Z.J.; Jorgensen, J.T.; Gron, R.; Brauner, E.V.; Lynge, E. Active smoking and risk of breast cancer in a Danish nurse cohort study. BMC Cancer 2017, 17, 556. [Google Scholar] [CrossRef]
- Jones, M.E.; Schoemaker, M.J.; McFadden, E.C.; Wright, L.B.; Johns, L.E.; Swerdlow, A.J. Night shift work and risk of breast cancer in women: The Generations Study cohort. Br. J. Cancer 2019, 121, 172–179. [Google Scholar] [CrossRef]
- Gram, I.T.; Park, S.Y.; Maskarinec, G.; Wilkens, L.R.; Haiman, C.A.; Le Marchand, L. Smoking and breast cancer risk by race/ethnicity and oestrogen and progesterone receptor status: The Multiethnic Cohort (MEC) study. Int. J. Epidemiol. 2019, 48, 501–511. [Google Scholar] [CrossRef]
- Veron, L.; Gelot, A.; Gusto, G.; Arveux, P.; Delaloge, S.; Boutron-Ruault, M.C. Modifiable risk factors for advanced vs. early breast cancer in the French E3N cohort. Int. J. Cancer 2020, 146, 850–860. [Google Scholar] [CrossRef]
- Lin, C.-H.; Yap, Y.S.; Lee, K.-H.; Im, S.-A.; Naito, Y.; Yeo, W.; Ueno, T.; Kwong, A.; Li, H.; Huang, S.-M.; et al. Contrasting Epidemiology and Clinicopathology of Female Breast Cancer in Asians vs the US Population. J. Natl. Cancer Inst. 2019, 111, 1298–1306. [Google Scholar] [CrossRef]
- Lin, C.H.; Liau, J.Y.; Lu, Y.S.; Huang, C.S.; Lee, W.C.; Kuo, K.T.; Shen, Y.C.; Kuo, S.H.; Lan, C.; Liu, J.M.; et al. Molecular subtypes of breast cancer emerging in young women in Taiwan: Evidence for more than just westernization as a reason for the disease in Asia. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1807–1814. [Google Scholar] [CrossRef]
- Cohen, S.S.; Matthews, C.E.; Bradshaw, P.T.; Lipworth, L.; Buchowski, M.S.; Signorello, L.B.; Blot, W.J. Sedentary behavior, physical activity, and likelihood of breast cancer among Black and White women: A report from the Southern Community Cohort Study. Cancer Prev. Res. 2013, 6, 566–576. [Google Scholar] [CrossRef][Green Version]
- Nomura, S.J.; Dash, C.; Rosenberg, L.; Palmer, J.; Adams-Campbell, L.L. Sedentary time and breast cancer incidence in African American women. Cancer Causes Control 2016, 27, 1239–1252. [Google Scholar] [CrossRef] [PubMed]
- Nomura, S.J.O.; Dash, C.; Sheppard, V.B.; Bowen, D.; Allison, M.; Barrington, W.; Chlebowski, R.; Coday, M.; Hou, L.; Howard, B.; et al. Sedentary time and postmenopausal breast cancer incidence. Cancer Causes Control CCC 2017, 28, 1405–1416. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Eshak, E.S.; Liu, K.; Muraki, I.; Cui, R.; Iso, H.; Tamakoshi, A. Television Viewing Time and Breast Cancer Incidence for Japanese Premenopausal and Postmenopausal Women: The JACC Study. Cancer Res. Treat. 2019, 51, 1509–1517. [Google Scholar] [CrossRef]
- Hunter, R.F.; Murray, J.M.; Coleman, H.G. The association between recreational screen time and cancer risk: Findings from the UK Biobank, a large prospective cohort study. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 97. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Bayona, R.; Gardeazabal, I.; Romanos-Nanclares, A.; Fernandez-Lazaro, C.I.; Alvarez-Alvarez, I.; Ruiz-Canela, M.; Gea, A.; Martinez-Gonzalez, M.A.; Santisteban, M.; Toledo, E. Leisure-time physical activity, sedentary behavior, and risk of breast cancer: Results from the SUN (‘Seguimiento Universidad De Navarra’) project. Prev. Med. 2021, 148, 106535. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhao, H.; Peng, C. Association of sedentary behavior with the risk of breast cancer in women: Update meta-analysis of observational studies. Ann. Epidemiol. 2015, 25, 687–697. [Google Scholar] [CrossRef]
- Friedenreich, C.; Lynch, B. Can living a less sedentary life decrease breast cancer risk in women? Women’s Health 2012, 8, 5–7. [Google Scholar] [CrossRef]
- Lynch, B.M.; Friedenreich, C.M.; Winkler, E.A.; Healy, G.N.; Vallance, J.K.; Eakin, E.G.; Owen, N. Associations of objectively assessed physical activity and sedentary time with biomarkers of breast cancer risk in postmenopausal women: Findings from NHANES (2003–2006). Breast Cancer Res. Treat. 2011, 130, 183–194. [Google Scholar] [CrossRef]
- Wiseman, A.J.; Lynch, B.M.; Cameron, A.J.; Dunstan, D.W. Associations of change in television viewing time with biomarkers of postmenopausal breast cancer risk: The Australian Diabetes, Obesity and Lifestyle Study. Cancer Causes Control 2014, 25, 1309–1319. [Google Scholar] [CrossRef]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Reeves, G.K.; Pirie, K.; Beral, V.; Green, J.; Spencer, E.; Bull, D.; Million Women Study, C. Cancer incidence and mortality in relation to body mass index in the Million Women Study: Cohort study. BMJ 2007, 335, 1134. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Anderson, C.; Lippman, S.M. Physical activity, sedentary behaviour, diet, and cancer: An update and emerging new evidence. Lancet Oncol. 2017, 18, e457–e471. [Google Scholar] [CrossRef]
- Hamburg, N.M.; McMackin, C.J.; Huang, A.L.; Shenouda, S.M.; Widlansky, M.E.; Schulz, E.; Gokce, N.; Ruderman, N.B.; Keaney, J.F., Jr.; Vita, J.A. Physical inactivity rapidly induces insulin resistance and microvascular dysfunction in healthy volunteers. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2650–2656. [Google Scholar] [CrossRef]
- Alibegovic, A.C.; Hojbjerre, L.; Sonne, M.P.; van Hall, G.; Stallknecht, B.; Dela, F.; Vaag, A. Impact of 9 days of bed rest on hepatic and peripheral insulin action, insulin secretion, and whole-body lipolysis in healthy young male offspring of patients with type 2 diabetes. Diabetes 2009, 58, 2749–2756. [Google Scholar] [CrossRef]
- Kumar, J.; Muntner, P.; Kaskel, F.J.; Hailpern, S.M.; Melamed, M.L. Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001–2004. Pediatrics 2009, 124, e362–e370. [Google Scholar] [CrossRef]
- McCullough, M.L.; Rodriguez, C.; Diver, W.R.; Feigelson, H.S.; Stevens, V.L.; Thun, M.J.; Calle, E.E. Dairy, calcium, and vitamin D intake and postmenopausal breast cancer risk in the Cancer Prevention Study II Nutrition Cohort. Cancer Epidemiol. Biomark. Prev. 2005, 14, 2898–2904. [Google Scholar] [CrossRef]
- Tamimi, R.M.; Byrne, C.; Colditz, G.A.; Hankinson, S.E. Endogenous hormone levels, mammographic density, and subsequent risk of breast cancer in postmenopausal women. J. Natl. Cancer Inst. 2007, 99, 1178–1187. [Google Scholar] [CrossRef]
- Monninkhof, E.M.; Peeters, P.H.; Schuit, A.J. Design of the sex hormones and physical exercise (SHAPE) study. BMC Public Health 2007, 7, 232. [Google Scholar] [CrossRef]
- Chazelas, E.; Srour, B.; Desmetz, E.; Kesse-Guyot, E.; Julia, C.; Deschamps, V.; Druesne-Pecollo, N.; Galan, P.; Hercberg, S.; Latino-Martel, P.; et al. Sugary drink consumption and risk of cancer: Results from NutriNet-Sante prospective cohort. BMJ 2019, 366, l2408. [Google Scholar] [CrossRef]
- Hodge, A.M.; Bassett, J.K.; Milne, R.L.; English, D.R.; Giles, G.G. Consumption of sugar-sweetened and artificially sweetened soft drinks and risk of obesity-related cancers. Public Health Nutr. 2018, 21, 1618–1626. [Google Scholar] [CrossRef]
- Romanos-Nanclares, A.; Toledo, E.; Gardeazabal, I.; Jimenez-Moleon, J.J.; Martinez-Gonzalez, M.A.; Gea, A. Sugar-sweetened beverage consumption and incidence of breast cancer: The Seguimiento Universidad de Navarra (SUN) Project. Eur. J. Nutr. 2019, 58, 2875–2886. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; McKeown, N.M.; Hwang, S.J.; Hoffmann, U.; Jacques, P.F.; Fox, C.S. Sugar-Sweetened Beverage Consumption Is Associated With Change of Visceral Adipose Tissue Over 6 Years of Follow-Up. Circulation 2016, 133, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Godinho-Mota, J.C.M.; Martins, K.A.; Vaz-Goncalves, L.; Mota, J.F.; Soares, L.R.; Freitas-Junior, R. Visceral adiposity increases the risk of breast cancer: A case-control study. Nutr. Hosp. 2018, 35, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Keadle, S.K.; Troiano, R.P.; Kahle, L.; Koster, A.; Brychta, R.; van Domelen, D.; Caserotti, P.; Chen, K.Y.; Harris, T.B.; et al. Accelerometer-measured dose-response for physical activity, sedentary time, and mortality in US adults. Am. J. Clin. Nutr. 2016, 104, 1424–1432. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Items | Cases/Person-Years | 95% CI of HR 1 | HR 1 (95% CI) | p | ||
|---|---|---|---|---|---|---|---|
| Hypertension | No | 95 | 63,428 |  | Referent | ||
| Yes | 17 | 9026 | 1.14 | (0.63–2.05) | 0.669 | ||
| Diabetes | No | 104 | 69,133 | Referent | |||
| Yes | 8 | 3320 | 1.58 | (0.75–3.32) | 0.230 | ||
| Hyperlipidemia | No | 105 | 69,571 | Referent | |||
| Yes | 7 | 2882 | 1.57 | (0.72–3.43) | 0.262 | ||
| Parity | Continuous | 0.84 | (0.74–0.96) | 0.009 | |||
| Nulliparous | 12 | 5776 | Referent | ||||
| 1–3 children | 75 | 45,331 | 0.74 | (0.40–1.37) | 0.341 | ||
| ≥4 children | 25 | 21,346 | 0.41 | (0.19–0.89) | 0.024 | ||
| p for trend | 0.013 | ||||||
| Hormone therapy | No | 98 | 66,187 | Referent | |||
| Yes | 14 | 6267 | 1.48 | (0.84–2.62) | 0.173 | ||
| Postmenopause | No | 80 | 52,546 | Referent | |||
| Yes | 32 | 19,907 | 0.90 | (0.43–1.90) | 0.784 | ||
| Body mass index | Continuous | 1.03 | (0.98–1.08) | 0.278 | |||
| <24 kg/m2 | 55 | 40,029 | Referent | ||||
| ≥24 to <27 kg/m2 | 33 | 22,679 | 1.03 | (0.66–1.62) | 0.882 | ||
| ≥27 kg/m2 | 24 | 9745 | 1.77 | (1.09–2.87) | 0.020 | ||
| p for trend | 0.044 | ||||||
| Alcohol intake | No | 104 | 62,533 | Referent | |||
| Yes | 8 | 9921 | 0.49 | (0.24–1.01) | 0.052 | ||
| Smoking | No | 105 | 67,225 | Referent | |||
| Yes | 7 | 5228 | 0.87 | (0.40–1.87) | 0.717 | ||
| Exercise | No | 50 | 36,295 | Referent | |||
| Yes | 62 | 36,158 | 1.23 | (0.85–1.79) | 0.269 | ||
| Time spent sitting | Continuous | 1.03 | (0.98–1.09) | 0.229 | |||
| 0–2.9 h/day | 14 | 16,291 | Referent | ||||
| ≥3 h/day | 98 | 56,162 | 2.04 | (1.17–3.57) | 0.013 | ||
| Sugary drink intake | No | 33 | 26,726 | Referent | |||
| Yes | 79 | 45,728 | 1.45 | (0.96–2.19) | 0.080 | ||
| Meat intake | Almost every day | 43 | 28,407 | Referent | |||
| 1–5 times per week | 52 | 34,693 | 0.99 | (0.66–1.48) | 0.941 | ||
| <1 time per week | 17 | 9353 | 1.17 | (0.66–2.08) | 0.584 | ||
| p for trend | 0.688 | ||||||
| Vegetable intake | Almost every day | 99 | 63,665 | Referent | |||
| 3–5 times per week | 9 | 6642 | 0.87 | (0.44–1.73) | 0.697 | ||
| ≤2 times per week | 4 | 2146 | 1.20 | (0.44–3.26) | 0.724 | ||
| p for trend | 0.981 | ||||||
| Fruit intake | Almost every day | 75 | 46,777 | Referent | |||
| 3–5 times per week | 18 | 13,678 | 0.82 | (0.49–1.38) | 0.460 | ||
| ≤2 times per week | 19 | 11,999 | 0.98 | (0.59–1.63) | 0.939 | ||
| p for trend | 0.765 | ||||||
| Variable Group | n | (%) |
|---|---|---|
| Age (years) | ||
| 30–39 | 1724 | (29.3) |
| 40–54 | 2334 | (39.7) |
| ≥55 | 1821 | (31.0) |
| Continuous (mean ± standard deviation) | 49.73 ± 13.91 | |
| Area | ||
| Taipei, New Taipei, Keelung | 1561 | (26.6) |
| Taoyuan–Hsinchu–Miaoli, Taichung–Changhua–Nantou | 1765 | (30.0) |
| Other | 2553 | (43.4) |
| Education | ||
| Elementary school and under | 2849 | (48.5) |
| Junior high school | 870 | (14.8) |
| Senior high school and above | 2160 | (36.7) |
| Marital status | ||
| Married | 4464 | (75.9) |
| Widowed | 809 | (13.8) |
| Other | 606 | (10.3) |
| Household monthly income | ||
| USD ≤1000 | 1475 | (25.1) |
| USD 1001–2333 | 2525 | (42.9) |
| USD ≥2334 | 1879 | (32.0) |
| Variables | HR 1 (95% CI) | p | |
|---|---|---|---|
| Age (years) | 1.01 | (1.00, 1.03) | 0.111 |
| Parity (ordinal) | 0.63 | (0.44, 0.91) | 0.013 |
| Body mass index (ordinal) | 1.34 | (1.04, 1.71) | 0.022 |
| Alcohol intake | 0.50 | (0.24, 1.02) | 0.056 |
| Time spent sitting ≥3 h/day | 1.89 | (1.08, 3.32) | 0.026 |
| Sugary drink intake | 1.46 | (0.96, 2.21) | 0.074 |
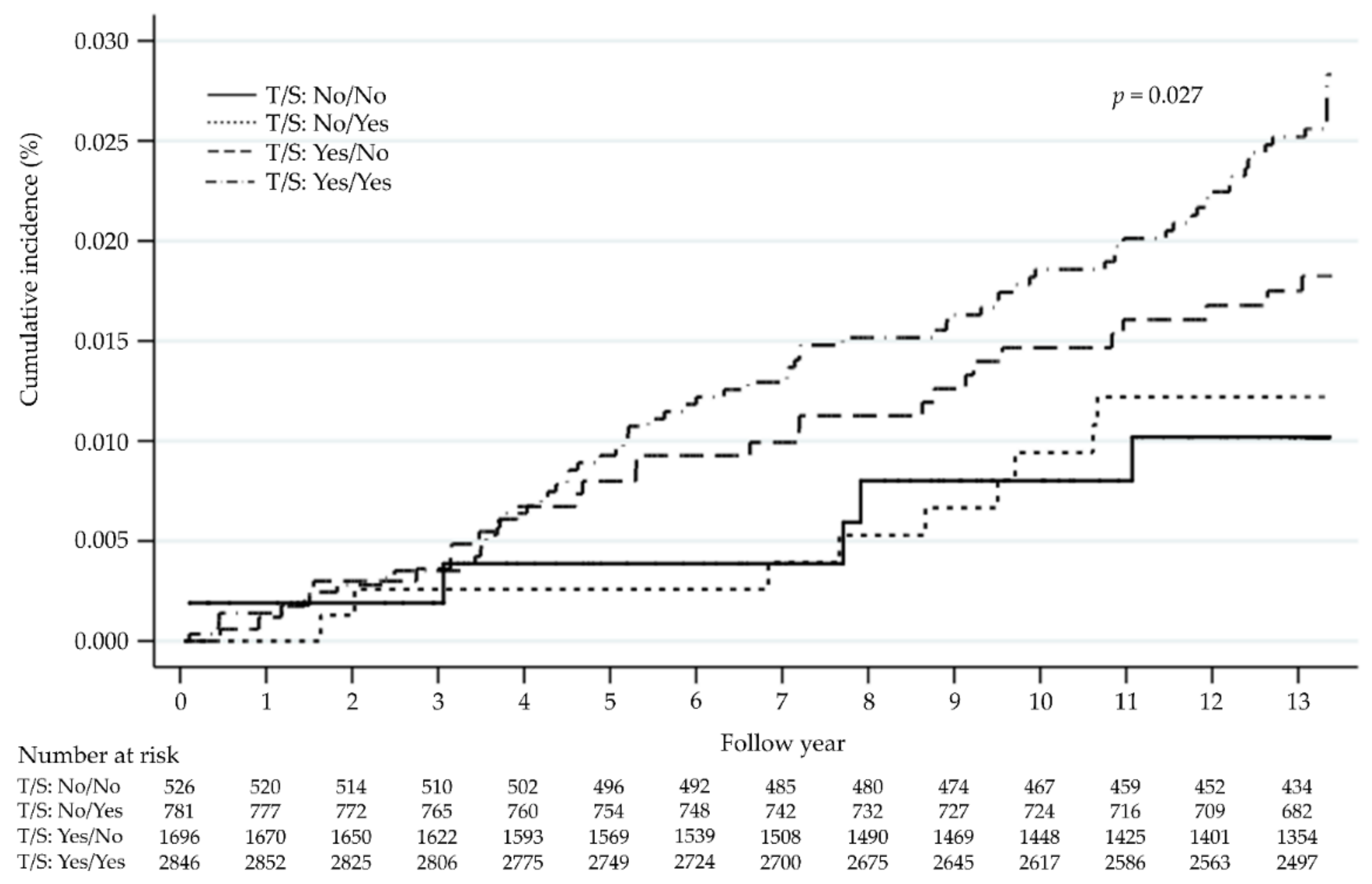
| Time Spent Sitting ≥3 h/day | Sugary Drink Intake | HR 1 (95% CI) | p | |
|---|---|---|---|---|
| No | No | Referent | ||
| No | Yes | 1.22 | (0.41, 3.64) | 0.726 |
| Yes | No | 1.69 | (0.65, 4.37) | 0.282 |
| Yes | Yes | 2.51 | (1.01, 6.23) | 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-C.; Lin, C.-H.; Huang, S.-P.; Chen, M.; Lee, T.-S. Risk Factors for Female Breast Cancer: A Population Cohort Study. Cancers 2022, 14, 788. https://doi.org/10.3390/cancers14030788
Wang Y-C, Lin C-H, Huang S-P, Chen M, Lee T-S. Risk Factors for Female Breast Cancer: A Population Cohort Study. Cancers. 2022; 14(3):788. https://doi.org/10.3390/cancers14030788
Chicago/Turabian StyleWang, Yu-Chiao, Ching-Hung Lin, Shih-Pei Huang, Mingchih Chen, and Tian-Shyug Lee. 2022. "Risk Factors for Female Breast Cancer: A Population Cohort Study" Cancers 14, no. 3: 788. https://doi.org/10.3390/cancers14030788
APA StyleWang, Y.-C., Lin, C.-H., Huang, S.-P., Chen, M., & Lee, T.-S. (2022). Risk Factors for Female Breast Cancer: A Population Cohort Study. Cancers, 14(3), 788. https://doi.org/10.3390/cancers14030788