
Salvage Radiotherapy versus Observation for Biochemical Recurrence following Radical Prostatectomy for Prostate Cancer: A Matched Pair Analysis

 , , ,
, , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Radiotherapy
2.3. Outcomes
2.4. Statistical Analyses
3. Results
3.1. Descriptive Statistics
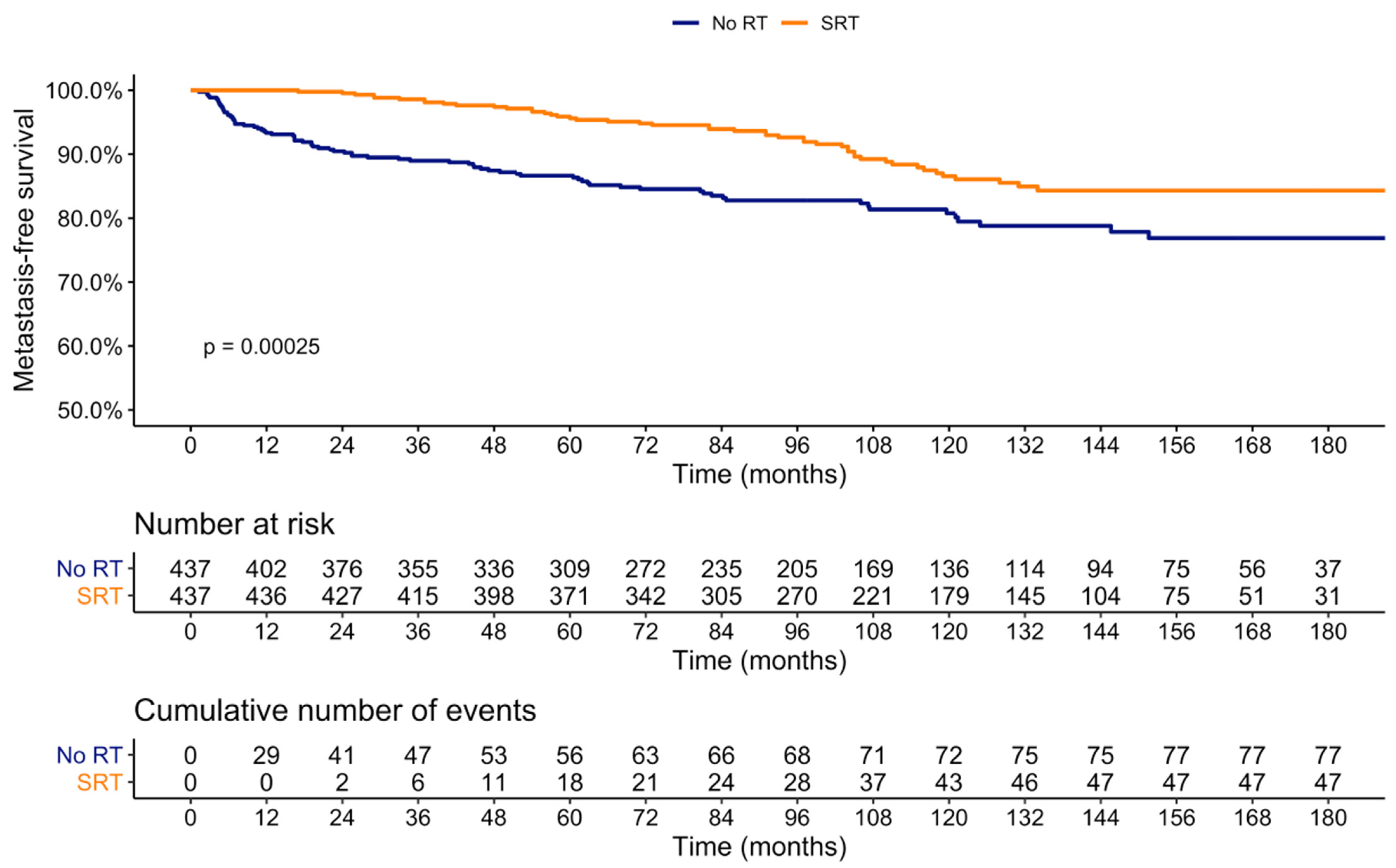
3.2. Impact of SRT on Metastasis
3.3. Impact of SRT on Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II—2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Grivas, N.; de Bruin, D.; Barwari, K.; van Muilekom, E.; Tillier, C.; van Leeuwen, P.J.; Wit, E.; Kroese, W.; van der Poel, H. Ultrasensitive prostate-specific antigen level as a predictor of biochemical progression after robot-assisted radical prostatectomy: Towards risk adapted follow-up. J. Clin. Lab. Anal. 2018, 33, e22693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tendulkar, R.D.; Agrawal, S.; Gao, T.; Efstathiou, J.A.; Pisansky, T.M.; Michalski, J.M.; Koontz, B.F.; Hamstra, D.A.; Feng, F.Y.; Liauw, S.L.; et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy After Radical Prostatectomy. J. Clin. Oncol. 2016, 34, 3648–3654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartkowiak, D.; Siegmann, A.; Böhmer, D.; Budach, V.; Wiegel, T. The impact of prostate-specific antigen persistence after radical prostatectomy on the efficacy of salvage radiotherapy in patients with primary N0 prostate cancer. BJU Int. 2019, 124, 785–791. [Google Scholar] [CrossRef]
- Trock, B.J.; Han, M.; Freedland, S.J.; Humphreys, E.B.; DeWeese, T.L.; Partin, A.W.; Walsh, P.C. Prostate cancer-specific survival following salvage radiotherapy vs observation in men with biochemical recurrence after radical prostatectomy. JAMA 2008, 299, 2760–2769. [Google Scholar] [CrossRef] [Green Version]
- Cotter, S.E.; Chen, M.H.; Moul, J.W.; Lee, W.R.; Koontz, B.F.; Anscher, M.S.; Robertson, C.N.; Walther, P.J.; Polascik, T.J.; D’Amico, A.V. Salvage radiation in men after prostate-specific antigen failure and the risk of death. Cancer 2011, 117, 3925–3932. [Google Scholar] [CrossRef]
- Preisser, F.; Chun, F.K.H.; Pompe, R.S.; Heinze, A.; Salomon, G.; Graefen, M.; Huland, H.; Tilki, D. Persistent Prostate-Specific Antigen after Radical Prostatectomy and Its Impact on Oncologic Outcomes. Eur. Urol. 2019, 76, 106–114. [Google Scholar] [CrossRef]
- Bandini, M.; Marchioni, M.; Preisser, F.; Zaffuto, E.; Tian, Z.; Tilki, D.; Montorsi, F.; Shariat, S.F.; Saad, F.; Briganti, A.; et al. Survival after radical prostatectomy or radiotherapy for locally advanced (cT3) prostate cancer. World J. Urol. 2018, 36, 1399–1407. [Google Scholar] [CrossRef]
- Preisser, F.; van den Bergh, R.C.N.; Gandaglia, G.; Ost, P.; Surcel, C.I.; Sooriakumaran, P.; Montorsi, F.; Graefen, M.; van der Poel, H.; de la Taille, A.; et al. Effect of Extended Pelvic Lymph Node Dissection on Oncologic Outcomes in Patients with D’Amico Intermediate and High Risk Prostate Cancer Treated with Radical Prostatectomy: A Multi-Institutional Study. J. Urol. 2020, 203, 338–343. [Google Scholar] [CrossRef]
- Stish, B.J.; Pisansky, T.M.; Harmsen, W.S.; Davis, B.J.; Tzou, K.S.; Choo, R.; Buskirk, S.J. Improved Metastasis-Free and Survival Outcomes with Early Salvage Radiotherapy in Men with Detectable Prostate-Specific Antigen after Prostatectomy for Prostate Cancer. J. Clin. Oncol. 2016, 34, 3864–3871. [Google Scholar] [CrossRef]
- Siegmann, A.; Bottke, D.; Faehndrich, J.; Brachert, M.; Lohm, G.; Miller, K.; Bartkowiak, D.; Hinkelbein, W.; Wiegel, T. Salvage radiotherapy after prostatectomy—What is the best time to treat? Radiother. Oncol. 2012, 103, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.; Bolla, M.; Briganti, A.; Carroll, P.; Cozzarini, C.; Joniau, S.; van Poppel, H.; Roach, M.; Stephenson, A.; Wiegel, T.; et al. Early salvage radiotherapy following radical prostatectomy. Eur. Urol. 2014, 65, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Bottke, D.; Bartkowiak, D.; Siegmann, A.; Thamm, R.; Böhmer, D.; Budach, V.; Wiegel, T. Effect of early salvage radiotherapy at PSA <0.5 ng/mL and impact of post-SRT PSA nadir in post-prostatectomy recurrent prostate cancer. Prostate Cancer Prostatic Dis. 2019, 22, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; Bandini, M.; Mazzone, E.; Nazzani, S.; Marchioni, M.; Tian, Z.; Saad, F.; Pompe, R.S.; Shariat, S.F.; Heinzer, H.; et al. Validation of the Social Security Administration Life Tables (2004–2014) in Localized Prostate Cancer Patients within the Surveillance, Epidemiology, and End Results database. Eur. Urol. Focus 2019, 5, 807–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pompe, R.S.; Gild, P.; Karakiewicz, P.I.; Bock, L.-P.; Schlomm, T.; Steuber, T.; Graefen, M.; Huland, H.; Tian, Z.; Tilki, D. Long-term cancer control outcomes in patients with biochemical recurrence and the impact of time from radical prostatectomy to biochemical recurrence. Prostate 2018, 78, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Feng, Z.; Trock, B.J.; Humphreys, E.B.; Carducci, M.A.; Partin, A.W.; Walsh, P.C.; Eisenberger, M.A. The natural history of metastatic progression in men with prostate-specific antigen recurrence after radical prostatectomy: Long-term follow-up. BJU Int. 2012, 109, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Markowski, M.C.; Chen, Y.; Feng, Z.; Cullen, J.; Trock, B.J.; Suzman, D.; Antonarakis, E.S.; Paller, C.J.; Rosner, I.; Han, M.; et al. PSA Doubling Time and Absolute PSA Predict Metastasis-free Survival in Men With Biochemically Recurrent Prostate Cancer after Radical Prostatectomy. Clin. Genitourin. Cancer 2019, 17, 470–475.e1. [Google Scholar] [CrossRef]
- Jackson, W.C.; Johnson, S.B.; Feng, F.Y.; Hamstra, D.A. Salvage radiation therapy improves metastasis-free survival for clinically aggressive and indolent prostate cancer recurrences after radical prostatectomy. Am. J. Clin. Oncol. 2015, 38, 367–372. [Google Scholar] [CrossRef]
- Jairath, N.K.; Dal Pra, A.; Vince, R.; Dess, R.T.; Jackson, W.C.; Tosoian, J.J.; McBride, S.M.; Zhao, S.G.; Berlin, A.; Mahal, B.A.; et al. A Systematic Review of the Evidence for the Decipher Genomic Classifier in Prostate Cancer. Eur. Urol. 2021, 79, 374–383. [Google Scholar] [CrossRef]
- Broggi, G.; Lo Giudice, A.; Di Mauro, M.; Asmundo, M.G.; Pricoco, E.; Piombino, E.; Caltabiano, R.; Morgia, G.; Russo, G.I. SRSF-1 and microvessel density immunohistochemical analysis by semi-automated tissue microarray in prostate cancer patients with diabetes (DIAMOND study). Prostate 2021, 81, 882–892. [Google Scholar] [CrossRef]
- Vale, C.L.; Fisher, D.; Kneebone, A.; Parker, C.; Pearse, M.; Richaud, P.; Sargos, P.; Sydes, M.R.; Brawley, C.; Brihoum, M.; et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020, 396, 1422–1431. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Before 1:1 Matching | After 1:1 Matching | |||||
|---|---|---|---|---|---|---|
| No RT (n = 1229) | SRT (n = 603) | SMD | No SRT (n = 437) | SRT (n = 437) | SMD | |
| Age, mean (sd) | 64.51 (6.3) | 63.43 (6.2) | 0.172 | 63.6 (6.5) | 63.8 (6.1) | 0.032 |
| Year of surgery, mean (sd) | 2005 (6.4) | 2004 (4.8) | 0.125 | 2005 (5.2) | 2004 (4.7) | 0.077 |
| PSA, ng/mL, mean (sd) | 11.76 (11.43) | 12.96 (12.19) | 0.102 | 12.1 (11.9) | 12.1 (10.8) | 0.001 |
| Pathologic Gleason, n (%) | 0.774 | 0.028 | ||||
| GG1 | 167 (13.6) | 207 (34.3) | 130 (29.7) | 131 (30.0) | ||
| GG2 | 615 (50.1) | 183 (30.3) | 165 (37.8) | 165 (37.8) | ||
| GG3 | 353 (28.7) | 94 (15.6) | 90 (20.6) | 87 (19.9) | ||
| GG4 | 23 (1.9) | 78 (12.9) | 17 (3.9) | 19 (4.3) | ||
| GG5 | 70 (5.7) | 41 (6.8) | 35 (8.0) | 35 (8.0) | ||
| Pathologic stage, n (%) | 0.205 | 0.056 | ||||
| pT2 | 557 (45.3) | 324 (53.7) | 229 (52.4) | 227 (51.9) | ||
| pT3a | 383 (31.2) | 181 (30.0) | 132 (30.2) | 136 (31.1) | ||
| pT3b | 266 (21.6) | 89 (14.8) | 67 (15.3) | 68 (15.6) | ||
| pT4 | 23 (1.9) | 9 (1.5) | 9 (2.1) | 6 (1.4) | ||
| Positive surgical margin, n (%) | 305 (24.8) | 251 (41.6) | 0.443 | 155 (35.5) | 167 (38.2) | 0.057 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| HR (95%-CI) | p-Value | HR (95%-CI) | p-Value | |
| No sRT (reference) | - | - | - | - |
| sRT | 0.52 (0.36–0.74) | <0.001 | 0.37 (0.25–0.53) | <0.001 |
| Year of surgery | 1.21 (1.16–1.27) | <0.001 | 1.22 (1.16–1.28) | <0.001 |
| Age | 0.99 (0.97–1.02) | 0.7 | 0.97 (0.94–0.99) | 0.01 |
| Preoperative PSA | 1.01 (0.99–1.02) | 0.2 | 0.99 (0.98–1.02) | 0.9 |
| Pathologic stage ≤ T2c (reference) | - | - | - | - |
| Pathologic stage T3a | 2.36 (1.54–3.62) | <0.001 | 2.24 (1.42–3.52) | <0.001 |
| Pathologic stage T3b | 4.02 (2.55–6.34) | <0.001 | 4.01 (2.41–6.67) | <0.001 |
| Pathologic stage T4 | 3.33 (1.19–9.34) | 0.02 | 5.98 (1.93–18.6) | <0.01 |
| GG1 (reference) | - | - | - | - |
| GG2 | 2.34 (1.31–4.18) | <0.01 | 1.50 (0.82–2.76) | 0.2 |
| GG3 | 4.91 (2.72–8.89) | <0.001 | 2.02 (1.05–3.92) | 0.03 |
| GG4–5 | 8.58 (4.72–15.6) | <0.001 | 4.16 (2.13–8.11) | <0.001 |
| Positive surgical margin | 0.77 (0.53–1.13) | 0.2 | 0.72 (0.49–1.07) | 0.1 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| HR (95%-CI) | p-Value | HR (95%-CI) | p-Value | |
| No sRT (reference) | - | - | - | - |
| sRT | 0.68 (0.46–0.99) | 0.04 | 0.64 (0.43–0.96) | 0.03 |
| Year of surgery | 0.98 (0.94–1.03) | 0.4 | 0.99 (0.95–1.05) | 0.9 |
| Age | 1.04 (1.01–1.07) | 0.04 | 1.04 (1.01–1.07) | 0.04 |
| Preoperative PSA | 1.02 (1.01–1.03) | <0.001 | 1.01 (0.99–1.02) | 0.2 |
| Pathologic stage ≤ T2c (reference) | - | - | - | - |
| Pathologic stage T3a | 2.57 (1.57–4.22) | <0.001 | 1.93 (1.14–3.26) | 0.01 |
| Pathologic stage T3b | 5.51 (3.31–9.15) | <0.001 | 3.68 (2.11–6.42) | <0.001 |
| Pathologic stage T4 | 4.96 (1.90–12.9) | <0.01 | 3.18 (1.17–8.65) | 0.02 |
| GG1 (reference) | - | - | - | - |
| GG2 | 1.58 (0.92–2.69) | 0.1 | 1.42 (0.81–2.47) | 0.2 |
| GG3 | 3.07 (1.73–5.46) | <0.001 | 2.16 (1.15–4.06) | 0.02 |
| GG4–5 | 4.63 (2.55–8.41) | <0.001 | 2.82 (1.48–5.37) | <0.01 |
| Positive surgical margin | 1.75 (1.19–2.56) | <0.01 | 1.38 (0.93–2.06) | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tilki, D.; Preisser, F.; Thamm, R.; Pompe, R.S.; Chun, F.K.-H.; Graefen, M.; Siegmann, A.; Böhmer, D.; Budach, V.; Wiegel, T. Salvage Radiotherapy versus Observation for Biochemical Recurrence following Radical Prostatectomy for Prostate Cancer: A Matched Pair Analysis. Cancers 2022, 14, 740. https://doi.org/10.3390/cancers14030740
Tilki D, Preisser F, Thamm R, Pompe RS, Chun FK-H, Graefen M, Siegmann A, Böhmer D, Budach V, Wiegel T. Salvage Radiotherapy versus Observation for Biochemical Recurrence following Radical Prostatectomy for Prostate Cancer: A Matched Pair Analysis. Cancers. 2022; 14(3):740. https://doi.org/10.3390/cancers14030740
Chicago/Turabian StyleTilki, Derya, Felix Preisser, Reinhard Thamm, Raisa S. Pompe, Felix K.-H. Chun, Markus Graefen, Alessandra Siegmann, Dirk Böhmer, Volker Budach, and Thomas Wiegel. 2022. "Salvage Radiotherapy versus Observation for Biochemical Recurrence following Radical Prostatectomy for Prostate Cancer: A Matched Pair Analysis" Cancers 14, no. 3: 740. https://doi.org/10.3390/cancers14030740
APA StyleTilki, D., Preisser, F., Thamm, R., Pompe, R. S., Chun, F. K.-H., Graefen, M., Siegmann, A., Böhmer, D., Budach, V., & Wiegel, T. (2022). Salvage Radiotherapy versus Observation for Biochemical Recurrence following Radical Prostatectomy for Prostate Cancer: A Matched Pair Analysis. Cancers, 14(3), 740. https://doi.org/10.3390/cancers14030740