
The Impact of Surgical Practice on Oncological Outcomes in Robot-Assisted Radical Hysterectomy for Early-Stage Cervical Cancer, Spanish National Registry

 , , , , and
, , , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Surgery and Adjuvant Treatment
2.3. Oncological Outcomes and Audit of Quality Indicators
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Clinical and Pathological Characteristics
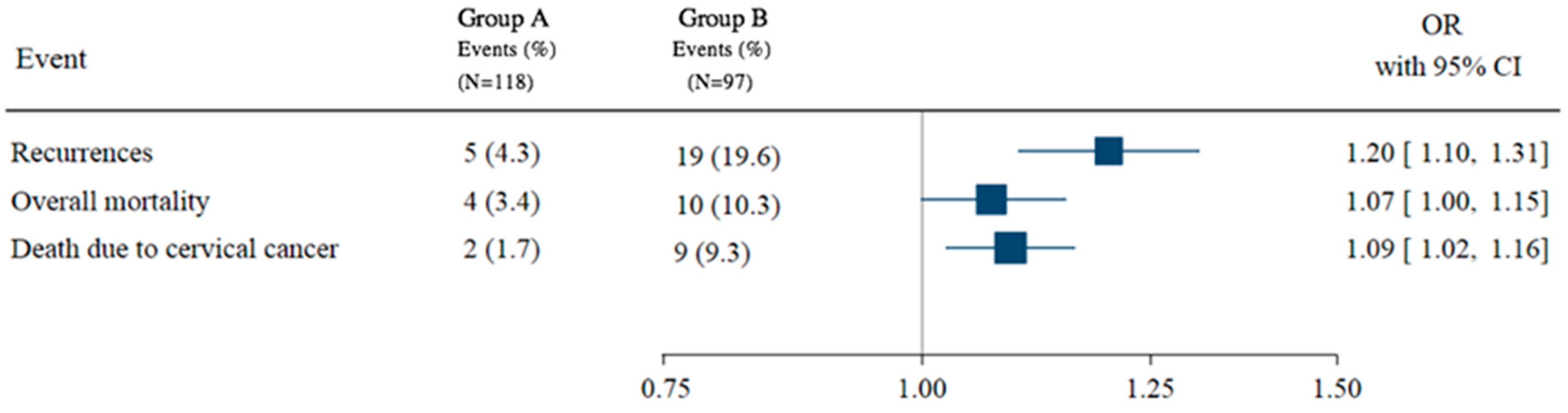
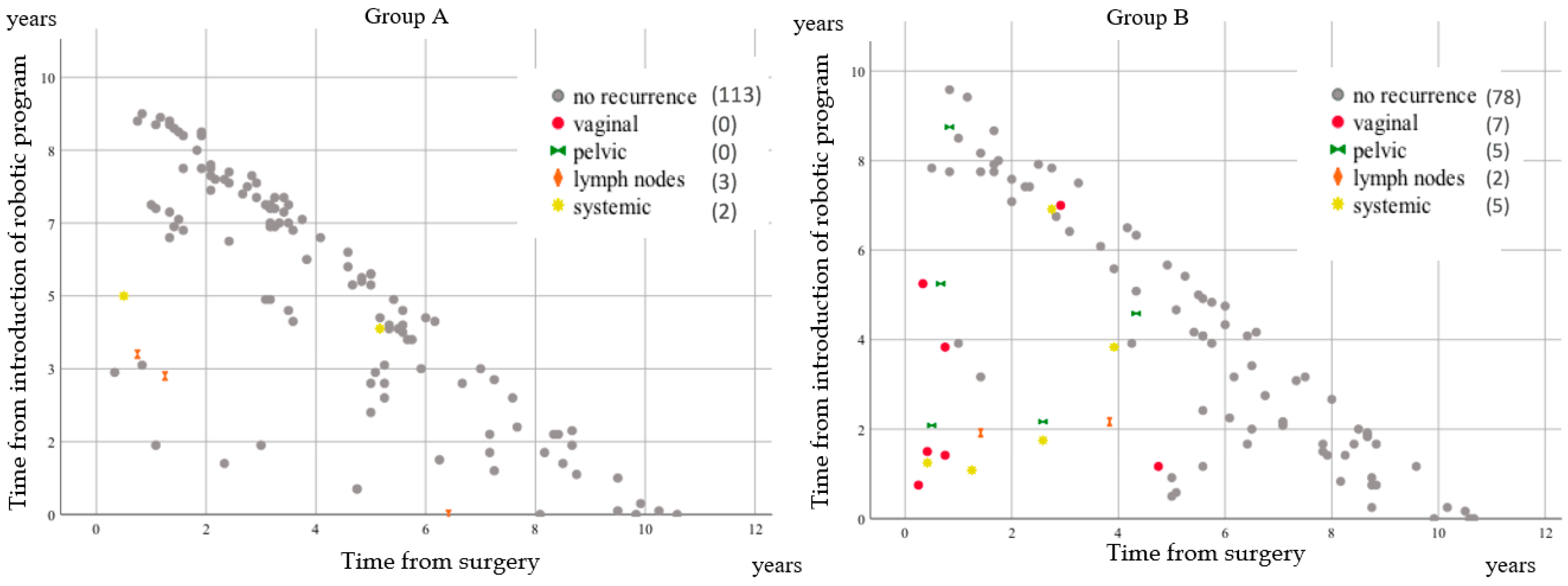
3.2. Oncological Outcomes
3.3. Audit of the Quality Indicators
3.4. Surgical Assessment of the Two Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Nitecki, R.; Ramirez, P.T.; Frumovitz, M.; Krause, K.J.; Tergas, A.I.; Wright, J.D.; Rauh-Hain, J.A.; Melamed, A. Survival after Minimally Invasive vs. Open Radical Hysterectomy for Early-Stage Cervical Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2020, 6, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Chiva, L.; Zanagnolo, V.; Querleu, D.; Martin-Calvo, N.; Arévalo-Serrano, J.; Cǎpîlna, M.E.; Fagotti, A.; Kucukmetin, A.; Mom, C.; Chakalova, G.; et al. SUCCOR study: An international European cohort observational study comparing minimally invasive surgery versus open abdominal radical hysterectomy in patients with stage IB1 cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Planchamp, F.; Fischerova, D.; Fotopoulou, C.; Kohler, C.; Landoni, F.; Mathevet, P.; Naik, R.; Ponce, J.; Raspagliesi, F.; et al. European Society of Gynaecological Oncology quality indicators for surgical treatment of cervical cancer. Int. J. Gynecol. Cancer 2020, 30, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boria, F.; Chiva, L.; Zanagnolo, V.; Querleu, D.; Martin-Calvo, N.; Căpîlna, M.E.; Fagotti, A.; Kucukmetin, A.; Mom, C.; Chakalova, G.; et al. Radical hysterectomy in early cervical cancer in Europe: Characteristics, outcomes and evaluation of ESGO quality indicators. Int. J. Gynecol. Cancer 2021, 31, 1212–1219. [Google Scholar] [CrossRef]
- Falconer, H.; Palsdottir, K.; Stalberg, K.; Dahm-Kähler, P.; Ottander, U.; Lundin, E.S.; Wijk, L.; Kimmig, R.; Jensen, P.T.; Eriksson, A.G.Z.; et al. Robot-assisted approach to cervical cancer (RACC): An international multi-center, open-label randomized controlled trial. Int. J. Gynecol. Cancer 2019, 29, 1072–1076. [Google Scholar] [CrossRef]
- Meigs, J.V. Radical hysterectomy with bilateral pelvic node dissections: A report of 100 patients operated on five or more years ago. Am. J. Obstet. Gynecol. 1951, 62, 854–870. [Google Scholar] [CrossRef]
- Kt, S.S. An improved radical hysterectomy with fewer urological complications and with no loss of therapeutic results for invasive cervical cancer. Baillieres Clin. Obs. Gynaecol. 1988, 2, 953–962. [Google Scholar]
- Kuwabara, Y.; Suzuki, M.; Hashimoto, M.; Furugen, Y.; Yoshida, K.M.N. New method to prevent bladder dysfunction after radical hysterectomy for uterine cervical cancer. J. Obs. Gynaecol. Res. 2000, 26, 1–8. [Google Scholar] [CrossRef]
- Rvz, G.J.P. Class II radical hysterectomy shows less morbidity and good treatment efficacy compared to class III. Gynecol. Oncol. 1991, 40, 21–24. [Google Scholar]
- Magrina, J.F.; Goodrich, M.A.; Lidner, T.K.; Weaver, A.L.; Cornella, J.L.P.K. Modified radical hysterectomy in the treatment of early squamous cervical cancer. Gynecol. Oncol 1999, 72, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Landoni, F.; Maneo, A.; Cormio, G.; Perego, P.; Milani, R.; Caruso, O.; Mangioni, C. Class II versus class III radical hysterectomy in stage IB-IIA cervical cancer: A prospective randomized study. Gynecol. Oncol. 2001, 80, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Wertheim, E. The extended abdominal operation for carcinoma uteri (based on 500 operative cases). Am. J. Obstet. Dis. Women Child. 1912, 66, 169–232. [Google Scholar]
- Muallem, M.Z. A New Anatomic and Staging-Oriented Classification of Radical Hysterectomy. Cancers 2021, 13, 3326. [Google Scholar] [CrossRef]
- Sedlis, A.; Bundy, B.N.; Rotman, M.Z.; Lentz, S.S.; Muderspach, L.I.; Zaino, R.J. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A gynecologic oncology group study. Gynecol. Oncol. 1999, 73, 177–183. [Google Scholar] [CrossRef]
- Rosenthal, R.; Hoffmann, H.; Clavien, P.A.; Bucher, H.C.; Dell-Kuster, S. Definition and classification of intraoperative complications (classic): Delphi study and pilot evaluation. World J. Surg. 2015, 39, 1663–1671. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The clavien-dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C.S.E. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Querleu, D.M.C. Classification of radical hysterectomy. Lancet Oncol. 2008, 9, 297–300. [Google Scholar] [CrossRef]
- Verleye, L.; Vergote, I.; Reed, N.; Ottevanger, P.B. Quality assurance for radical hysterectomy for cervical cancer: The view of the European Organization for Research and Treatment of Cancer—Gynecological Cancer Group ( EORTC-GCG ). Ann. Oncol. 2009, 20, 1631–1638. [Google Scholar] [CrossRef]
- Lee, B.; Kim, K.; Park, Y.; Lim, M.C.; Bristow, R.E. Impact of hospital care volume on clinical outcomes of laparoscopic radical hysterectomy for cervical cancer: A systematic review and meta-analysis. Medicine 2018, 97, e13445. [Google Scholar] [CrossRef] [PubMed]
- Alfonzo, E.; Wallin, E.; Ekdahl, L.; Staf, C.; Rådestad, A.F.; Reynisson, P.; Stålberg, K.; Falconer, H.; Persson, J.; Dahm-Kähler, P. No survival difference between robotic and open radical hysterectomy for women with early-stage cervical cancer: Results from a nationwide population-based cohort study. Eur. J. Cancer 2019, 116, 169–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, K.; Shimada, M.; Yamaguchi, S.; Matoda, M.; Nakanishi, T.; Kikkawa, F.; Ohmichi, M.; Okamoto, A.; Sugiyama, T.; Mikami, M. Association of Radical Hysterectomy Surgical Volume and Survival for Early-Stage Cervical Cancer. Obstet. Gynecol. 2019, 133, 1086–1098. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Matsuzaki, S.; Mandelbaum, R.S.; Chang, E.J.; Matsushima, K.; Grubbs, B.H.; Roman, L.D.; Wright, J.D.; California, S.; Angeles, L.; et al. Minimally invasive radical hysterectomy for early-stage cervical cancer: Volume-outcome relationship in the early experience period. Gynecol. Oncol. 2020, 158, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Ponce, J.; Fernandez-Gonzalez, S.; Gil-Moreno, A.; Coronado, P.J.; De la Rosa, J.; Nabais, H.; Hernández, G.; Taltavull, A.; Gilabert-Estelles, J.; Martínez-Román, S.; et al. Risk factors for recurrence after robot-assisted radical hysterectomy for early-stage cervical cancer: A multicenter retrospective study. Cancers 2020, 12, 3387. [Google Scholar] [CrossRef]
- Chacón, E.; Manzour, N.; Mínguez, J.Á.; Vázquez, D.; Castellano, T.; Lorenzo, L.S.; Salas, D.; Alcazar, J.L.; Gonzalez-Martin, A.; Chiva, L.M. Succor cone: Is it cervical conization a protective maneuver. Int. J. Gynecol. Cancer 2020, 30, A7–A8. [Google Scholar]
- Bizzarri, N.; Pedone Anchora, L.; Kucukmetin, A.; Ratnavelu, N.; Korompelis, P.; Carbone, V.; Fedele, C.; Bruno, M.; Vizzielli, G.; Gallotta, V.; et al. Protective Role of Conization Before Radical Hysterectomy in Early-Stage Cervical Cancer: A Propensity-Score Matching Study. Ann. Surg. Oncol. 2021, 28, 3585–3594. [Google Scholar] [CrossRef]
- Armbrust, R.; Chen, F.; Richter, R.; Muallem, M.Z.; Mustea, A.; Holthaus, B.; Sehouli, J. Results of a German wide survey towards current surgical approach in early stage cervical cancer noggo monitor 11. Sci. Rep. 2021, 11, 9774. [Google Scholar] [CrossRef]
- Lécuru, F.; Mathevet, P.; Querleu, D.; Leblanc, E.; Morice, P.; Daraï, E.; Marret, H.; Magaud, L.; Gillaizeau, F.; Chatellier, G.; et al. Bilateral negative sentinel nodes accurately predict absence of lymph node metastasis in early cervical cancer: Results of the SENTICOL study. J. Clin. Oncol. 2011, 29, 1686–1691. [Google Scholar] [CrossRef]
- Cibula, D.; Dusek, J.; Jarkovsky, J.; Dundr, P.; Querleu, D.; Van Der Zee, A.; Kucukmetin, A.; Kocian, R. A prospective multicenter trial on sentinel lymph node biopsy in patients with early-stage cervical cancer (SENTIX). Int. J. Gynecol. Cancer 2019, 29, 212–215. [Google Scholar] [CrossRef]
- Kocian, R.; Slama, J.; Fischerova, D.; Germanova, A.; Burgetova, A.; Dusek, L.; Dundr, P.; Nemejcova, K.; Jarkovsky, J.; Sebestova, S.; et al. Micrometastases in sentinel lymph nodes represent a significant negative prognostic factor in early-stage cervical cancer: A single-institutional retrospective cohort study. Cancers 2020, 12, 1438. [Google Scholar] [CrossRef] [PubMed]
- Guani, B.; Balaya, V.; Magaud, L.; Lecuru, F.; Mathevet, P. The clinical impact of low-volume lymph nodal metastases in early-stage cervical cancer: The senticol 1 and senticol 2 trials. Cancers 2020, 12, 1061. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Items | Patients | Recurrences (%) | ||
|---|---|---|---|---|
| Center (a) | 53 | 1 (1.9) |  | Group A |
| Center (b) | 46 | 3 (6.5) | ||
| Center (c) | 19 | 1 (5.3) | ||
| Center (d) | 55 | 13 (23.6) |  | Group B |
| Center (e) | 42 | 6 (16.7) | ||
| Center (f) | 9 | - | ||
| Center (g) | 6 | - | ||
| Center (h) | 5 | - | ||
| Center (i) | 2 | - | ||
| Center (j) | 2 | - | ||
| Total | 239 | 24 |
| Items | Group A (n = 118) | Group B (n = 97) | p-Value | Group A (n = 118) | Group B (n = 97) | p-Value * |
|---|---|---|---|---|---|---|
| Age (mean, sd) | 47.0 ± 10.8 | 49.7 ± 10.7 | 0.068 | 49.1 ± 11.0 | 48.8 ± 10.5 | 0.839 |
| BMI (%) | ||||||
| <25 | 51 (43.6) | 36 (37.1) | 0.337 | 48 (40.2) | 39 (40.2) | 0.996 |
| ≥25 | 66 (56.4) | 61 (62.9) | 70 (59.8) | 58 (59.8) | ||
| Histology (%) | ||||||
| Squamous cell carcinoma | 70 (59.3) | 61 (62.9) | 0.274 | 73 (61.6) | 61 (62.9) | 0.927 |
| Adenocarcinoma | 45 (38.1) | 30 (30.9) | 41 (35) | 32 (33) | ||
| Others | 3 (2.5) | 6 (6.2) | 4 (3.4) | 4 (4.1) | ||
| Size (%) | ||||||
| <20 mm | 68 (57.6) | 70 (72.2) | 0.027 | 77 (65) | 62 (63.9) | 0.874 |
| >20 mm | 50 (42.4) | 27 (27.8) | 41 (35) | 35 (36.1) | ||
| Grade (%) | ||||||
| Grade 1 | 31 (26.3) | 34 (35) | 0.163 | 40 (33.3) | 30 (30.9) | 0.708 |
| Grade 2–3 | 87 (73.7) | 63 (65) | 78 (66.7) | 67 (69.1) | ||
| Lymphovascular invasion (%) | ||||||
| No | 89 (75.4) | 86 (88.7) | 0.013 | 96 (81.2) | 78 (80.4) | 0.885 |
| Yes | 29 (24.6) | 11 (11.3) | 22 (18.8) | 19 (19.6) | ||
| Adjuvant treatment (%) | ||||||
| No | 83 (70.3) | 74 (76.3) | 0.328 | 86 (72.7) | 70 (72.2) | 0.937 |
| Yes | 35 (29.7) | 23 (23.7) | 32 (27.3) | 27 (27.8) | ||
| Nodal status (%) | ||||||
| Negative | 108 (91.5) | 86 (88.7) | 0.014 | 104 (88.0) | 87 (89.7) | 0.731 |
| Positive | 8 (6.8) | 2 (2.1) | 5 (4.3) | 5 (5.2) | ||
| Not assessed | 2 (1.7) | 9 (9.3) | 9 (7.7) | 5 (5.2) |
| ESGO Quality Indicator | Target Value | Group A | Group B |
|---|---|---|---|
| QI 1-Number of radical procedures (parametrectomies) in cervical cancer performed per center per year | ≥15 | 8.9 | 6.7 |
| QI 2-Surgery performed or supervised by a certified gynecologic oncologist or a trained surgeon dedicated to gynecological cancers | 100% | 100% | 100% |
| QI 3-Center participating in ongoing clinical trials in gynecological cancers | ≥1 | ≥5 | <1 |
| QI 4-Treatment discussed at a multidisciplinary team meeting | 100% | 100% | 100% |
| QI 5-Required pre-operative investigation | 100% | 92.5% | 80.7% |
| QI 6-Minimum required elements in surgical reports | 100% | 100% | 100% |
| QI 7-Minimum required elements in pathology and pathology reports | ≥ 90% | 100% | 100% |
| QI 8-Structured prospective reporting of follow-up and 30-day post-operative morbidity | ≥90% | 100% | 100% |
| Indicators | Group A | Group B | p-Value |
|---|---|---|---|
| Number of robotic procedures per center per year | 40.1 | 32.2 | 0.0400 |
| Ratio of the number of robotic radical hysterectomies to the number of surgeons per year | 4.4 | 4.3 | 0.850 |
| Surgeons in gynecologic oncology per center | 4.3 | 5 | 0.079 |
| Surgical time, minutes (mean ± SD) | 258.6 ± 51.8 | 221.9 ± 70.9 | <0.001 |
| Sentinel lymph node biopsy performed (%) | 88/118 (74.6) | 11/97 (11.3) | <0.001 |
| Pelvic lymphadenectomies performed (%) | 109/118 (92.4) | 85/97 (87.6) | 0.258 |
| Right pelvic lymph nodes, median (range) | 9 (1–26) | 9 (1–21) | 0.840 |
| Left pelvic lymph nodes, median (range) | 8 (3–27) | 7 (2–24) | 0.424 |
| Type of radical hysterectomy *, n (%) | 0.203 | ||
| A | 0 | 12/97 (12.4) | |
| B1 | 34/118 (28.8) | 17/97 (17.5) | |
| B2 | 3/118 (2.5) | 6/97 (6.2) | |
| C1 | 81/118 (68.6) | 62/97(63.9) | |
| Clear surgical margins (%) | 117/118 (99.2) | 93/97 (95.9) | 0.113 |
| Intrauterine manipulator, n (%) | 98/118 (83.1) | 55/97 (56.7) | <0.001 |
| Nerve sparing technique, n (%) | 118/118 (100) | 96/97 (99) | 0.451 |
| Hospital stay (in days), median (range) | 3 (1–21) | 3 (1–13) | 0.478 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandez-Gonzalez, S.; Ponce, J.; Martínez-Maestre, M.Á.; Barahona, M.; Gómez-Hidalgo, N.R.; Díaz-Feijoo, B.; Casajuana, A.; Gracia, M.; Frias-Gomez, J.; Benavente, Y.; et al. The Impact of Surgical Practice on Oncological Outcomes in Robot-Assisted Radical Hysterectomy for Early-Stage Cervical Cancer, Spanish National Registry. Cancers 2022, 14, 698. https://doi.org/10.3390/cancers14030698
Fernandez-Gonzalez S, Ponce J, Martínez-Maestre MÁ, Barahona M, Gómez-Hidalgo NR, Díaz-Feijoo B, Casajuana A, Gracia M, Frias-Gomez J, Benavente Y, et al. The Impact of Surgical Practice on Oncological Outcomes in Robot-Assisted Radical Hysterectomy for Early-Stage Cervical Cancer, Spanish National Registry. Cancers. 2022; 14(3):698. https://doi.org/10.3390/cancers14030698
Chicago/Turabian StyleFernandez-Gonzalez, Sergi, Jordi Ponce, María Ángeles Martínez-Maestre, Marc Barahona, Natalia R. Gómez-Hidalgo, Berta Díaz-Feijoo, Andrea Casajuana, Myriam Gracia, Jon Frias-Gomez, Yolanda Benavente, and et al. 2022. "The Impact of Surgical Practice on Oncological Outcomes in Robot-Assisted Radical Hysterectomy for Early-Stage Cervical Cancer, Spanish National Registry" Cancers 14, no. 3: 698. https://doi.org/10.3390/cancers14030698
APA StyleFernandez-Gonzalez, S., Ponce, J., Martínez-Maestre, M. Á., Barahona, M., Gómez-Hidalgo, N. R., Díaz-Feijoo, B., Casajuana, A., Gracia, M., Frias-Gomez, J., Benavente, Y., Costas, L., Martí, L., Melero, L., Silvan, J. M., Beiro, E., Lobo, I., De la Rosa, J., Coronado, P. J., & Gil-Moreno, A. (2022). The Impact of Surgical Practice on Oncological Outcomes in Robot-Assisted Radical Hysterectomy for Early-Stage Cervical Cancer, Spanish National Registry. Cancers, 14(3), 698. https://doi.org/10.3390/cancers14030698