
Particle Beam Therapy for Intrahepatic and Extrahepatic Biliary Duct Carcinoma: A Multi-Institutional Retrospective Data Analysis

 ,
,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
3.1. Patient Characteristics
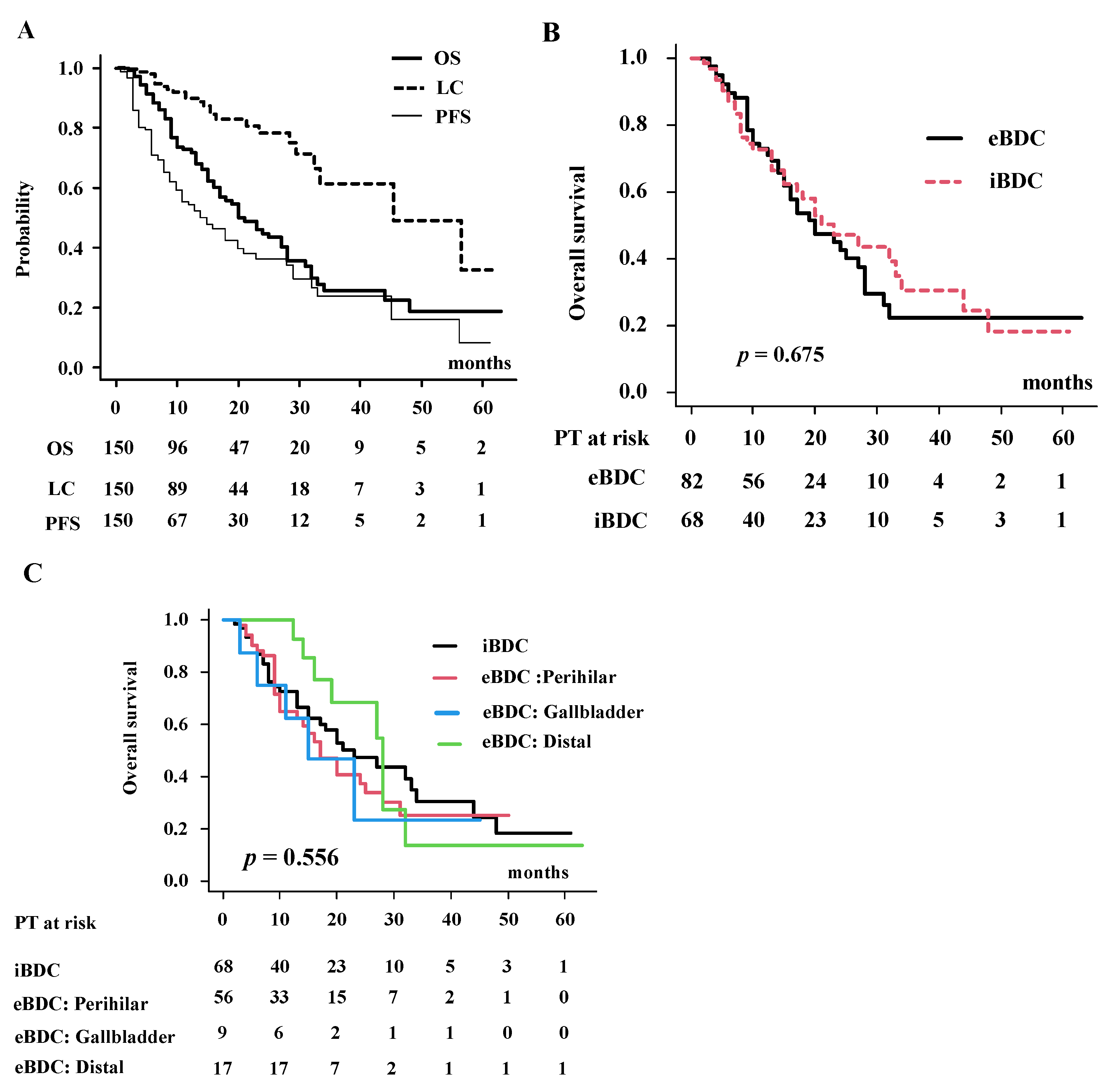
3.2. Local Control, Progression-Free Survival, Failure Pattern and Overall Survival Rate in Total Population
3.3. Detailed Analysis of Overall Survival Rate in eBDC and iBDC
3.4. Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, G.; Liu, Q.; Wu, Y.; Liu, Z.; Lu, W.; Li, S.; Pan, G.; Chen, X. The global, regional and national burden of the gallbladder and biliary duct carcinoma and its attributable risk factors in 195 countries and territories, 1990 to 2017: A systematic analysis for the Global Burden of Disease Study 2017. Cancer 2021, 127, 2238–2250. [Google Scholar] [CrossRef]
- Jarnagin, W.R.; Shoup, M. Surgical management of cholangiocarcinoma. Semin. Liver Dis. 2004, 24, 189–199. [Google Scholar] [CrossRef]
- Esnaola, N.F.; Meyer, J.E.; Karachristos, A.; Maranki, J.L.; Camp, E.R.; Denlinger, C.S. Evaluation and management of intrahepatic and extrahepatic cholangiocarcinoma. Cancer 2016, 122, 1349–1369. [Google Scholar] [CrossRef]
- Keane, F.K.; Zhu, A.X.; Hong, T.S. Radiotherapy for Biliary Tract Cancers. Semin. Radiat. Oncol. 2018, 28, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Kopek, N.; Holt, M.I.; Hansen, A.T.; Høyer, M. Stereotactic body radiotherapy for unresectable cholangiocarcinoma. Radiother. Oncol. 2010, 94, 47–52. [Google Scholar] [CrossRef]
- Sandler, K.A.; Veruttipong, D.; Agopian, V.G.; Finn, R.S.; Hong, J.C.; Kaldas, F.M.; Sadeghi, S.; Busuttil, R.W.; Lee, P. Stereotactic body radiotherapy (SBRT) for locally advanced extrahepatic and intrahepatic cholangiocarcinoma. Adv. Radiat. Oncol. 2016, 1, 237–243. [Google Scholar] [CrossRef]
- Kozak, M.M.; Toesca, D.A.S.; von Eyben, R.; Pollom, E.L.; Chang, D.T. Stereotactic Body Radiation Therapy for Cholangiocarcinoma: Optimizing Locoregional Control with Elective Nodal Irradiation. Adv. Radiat. Oncol. 2019, 5, 77–84. [Google Scholar] [CrossRef]
- Makita, C.; Nakamura, T.; Takada, A.; Takayama, K.; Suzuki, M.; Ishikawa, Y.; Azami, Y.; Kato, T.; Tsukiyama, I.; Kikuchi, Y. Clinical outcomes and toxicity of proton beam therapy for advanced cholangiocarcinoma. Radiat. Oncol. 2014, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Ohkawa, A.; Mizumoto, M.; Ishikawa, H.; Abei, M.; Fukuda, K.; Hashimoto, T.; Sakae, T.; Tsuboi, K.; Okumura, T.; Sakurai, H.H. Proton beam therapy for unresectable intrahepatic cholangiocarcinoma. J. Gastroenterol. Hepatol. 2015, 30, 957–963. [Google Scholar] [CrossRef]
- Shimizu, S.; Okumura, T.; Oshiro, Y.; Fukumitsu, N.; Fukuda, K.; Ishige, K.; Hasegawa, N.; Numajiri, H.; Murofushi, K.; Ohnishi, K.; et al. Clinical outcomes of previously untreated patients with unresectable intrahepatic cholangiocarcinoma following proton beam therapy. Radiat. Oncol. 2019, 14, 241. [Google Scholar] [CrossRef] [PubMed]
- Kasuya, G.; Terashima, K.; Shibuya, K.; Toyama, S.; Ebner, D.K.; Tsuji, H.; Okimoto, T.; Ohno, T.; Shioyama, Y.; Nakano, T.; et al. Japan Carbon-Ion Radiation Oncology Study Group. Carbon-ion radiotherapy for cholangiocarcinoma: A multi-institutional study by the Japan carbon-ion radiation oncology study group (J-CROS). Oncotarget 2019, 10, 4369–4379. [Google Scholar] [CrossRef] [PubMed]
- Borger, D.R.; Tanabe, K.K.; Fan, K.C.; Lopez, H.U.; Fantin, V.R.; Straley, K.S.; Schenkein, D.P.; Hezel, A.F.; Ancukiewicz, M.; Liebman, H.M.; et al. Frequent mutation of isocitrate dehydrogenase (IDH)1 and IDH2 in cholangiocarcinoma identified through broad-based tumor genotyping. Oncologist 2012, 17, 72–79. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Tao, R.; Krishnan, S.; Bhosale, P.R.; Javle, M.M.; Aloia, T.A.; Shroff, R.T.; Kaseb, A.O.; Bishop, A.J.; Swanick, C.W.; Koay, E.J.; et al. Ablative Radiotherapy Doses Lead to a Substantial Prolongation of Survival in Patients with Inoperable Intrahepatic Cholangiocarcinoma: A Retrospective Dose Response Analysis. J. Clin. Oncol. 2016, 34, 219–226. [Google Scholar] [CrossRef]
- Crane, C.H.; Macdonald, K.O.; Vauthey, J.N.; Yehuda, P.; Brown, T.; Curley, S.; Wong, A.; Delclos, M.; Charnsangavej, C.; Janjan, N.A. Limitations of conventional doses of chemoradiation for unresectable biliary cancer. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 969–974. [Google Scholar] [CrossRef]
- Avila, S.; Smani, D.A.; Koay, E.J. Radiation dose escalation for locally advanced unresectable intrahepatic and extrahepatic cholangiocarcinoma. Chin. Clin. Oncol. 2020, 9, 10. [Google Scholar] [CrossRef]
- De, B.; Tran Cao, H.S.; Vauthey, J.N.; Manzar, G.S.; Corrigan, K.L.; Raghav, K.P.S.; Lee, S.S.; Tzeng, C.D.; Minsky, B.D.; Smith, G.L.; et al. Ablative liver radiotherapy for unresected intrahepatic cholangiocarcinoma: Patterns of care and survival in the United States. Cancer 2022, 128, 2529–2539. [Google Scholar] [CrossRef]
- Hong, T.S.; Wo, J.Y.; Yeap, B.Y.; Ben-Josef, E.; McDonnell, E.I.; Blaszkowsky, L.S.; Kwak, E.L.; Allen, J.N.; Clark, J.W.; Goyal, L.; et al. Multi-institutional phase II study of high-dose hypofractionated proton beam therapy in patients with localized, unresectable hepatocellular carcinoma and intrahepatic cholangiocarcinoma. J. Clin. Oncol. 2016, 34, 460–468. [Google Scholar] [CrossRef]
- Alden, M.E.; Mohiuddin, M. The impact of radiation dose in combined external beam and intraluminal Ir-192 brachytherapy for bile duct cancer. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Foo, M.L.; Gunderson, L.L.; Bender, C.E.; Buskirk, S.J. External radiation therapy and transcatheter iridium in the treatment of extrahepatic bile duct carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, E.T.; Guo, M.; Mitra, N.; Metz, J.M. Brachytherapy in the treatment of cholangiocarcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, Y.; Ogawa, K.; Oikawa, H.; Onishi, H.; Kanesaka, N.; Tamamoto, T.; Kosugi, T.; Hatano, K.; Kobayashi, M.; Ito, Y.; et al. Impact of intraluminal brachytherapy on survival outcome for radiation therapy for unresectable biliary tract cancer: A propensity-score matched-pair analysis. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 822–829. [Google Scholar] [CrossRef]
- Kollar, L.; Rengan, R. Stereotactic body radiotherapy. Semin. Oncol. 2014, 41, 776–789. [Google Scholar] [CrossRef]
- Lee, J.; Yoon, W.S.; Koom, W.S.; Rim, C.H. Efficacy of stereotactic body radiotherapy for unresectable or recurrent cholangiocarcinoma: A meta-analysis and systematic review. Strahlenther. Onkol. 2019, 195, 93–102. [Google Scholar] [CrossRef]
- Kang, M.J.; Lim, J.; Han, S.S.; Park, H.M.; Kim, S.W.; Lee, W.J.; Woo, S.M.; Kim, T.H.; Won, Y.J.; Park, S.J. Distinct prognosis of biliary tract cancer according to tumor location, stage and treatment: A population-based study. Sci. Rep. 2022, 12, 10206. [Google Scholar] [CrossRef]
- Terashima, K.; Okada, N. Particle beam therapy for biliary duct carcinoma (proton and heavy iron beam radiotherapy). J. Jpn. Biliary Assoc. 2018, 32, 114–123. (In Japanese) [Google Scholar]
- Elganainy, D.; Holliday, E.B.; Taniguchi, C.M.; Smith, G.L.; Shroff, R.; Javle, M.; Raghav, K.; Kaseb, A.; Aloia, T.A.; Vauthey, J.N.; et al. Dose escalation of radiotherapy in unresectable extrahepatic cholangiocarcinoma. Cancer Med. 2018, 7, 4880–4892. [Google Scholar] [CrossRef]
- Brunner, T.B.; Blanck, O.; Lewitzki, V.; Abbasi-Senger, N.; Momm, F.; Riesterer, O.; Duma, M.N.; Wachter, S.; Baus, W.; Gerum, S.; et al. Stereotactic body radiotherapy dose and its impact on local control and overall survival of patients for locally advanced intrahepatic and extrahepatic cholangiocarcinoma. Radiother. Oncol. 2019, 132, 42–47. [Google Scholar] [CrossRef]
- Brunner, T.B.; Schwab, D.; Meyer, T.; Sauer, R. Chemoradiation may prolong survival of patients with non-bulky unresectable extrahepatic biliary carcinoma. A retrospective analysis. Strahlenther. Onkol. 2004, 180, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.; von Weyhern, C.; Fend, F.; Schneider, J.; Neu, B.; Meining, A.; Weidenbach, H.; Schmid, R.M.; Prinz, C. Endoscopic transpapillary brush cytology and forceps biopsy in patients with hilar cholangiocarcinoma. World J. Gastroenterol. 2008, 14, 1097–1101. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Strata | Total (n = 150) | eBDC (n = 82) | iBDC (n = 68) | p-Value |
|---|---|---|---|---|---|
| No. (%) or Median (range) | |||||
| Age | 74.00 (50.00, 94.00) | 76.00 (53.00, 92.00) | 73.50 (50.00, 94.00) | 0.488 | |
| Gender | Female | 53 (35.3) | 25 (36.8) | 28 (34.1) | 0.864 |
| Male | 97 (64.6) | 43 (63.2) | 54 (65.9) | ||
| Performance status | 0 | 120 (80.0) | 62 (75.6) | 58 (85.3) | 0.579 |
| 1 | 21 (14.0) | 14 (17.1) | 7 (10.3) | ||
| 2 | 6 (4.0) | 4 (4.9) | 2 (2.9) | ||
| 3 | 3 (2.0) | 2 (2.4) | 1 (1.5) | ||
| Child-Pugh class | Normal-A | 137 (91.3) | 76 (92.7) | 61 (89.7) | 0.430 |
| B | 12 (8.0) | 5 (6.1) | 7 (10.3) | ||
| C | 1 (0.7) | 1 (1.2) | 0 (0.0) | ||
| Diagnosis | Pathological | 66 (44.0) | 42 (51.2) | 24 (35.3) | 0.069 |
| Imaging+ tumor markers | 84 (56.0) | 40 (48.8) | 44 (64.7) | ||
| Jaundice | No | 97 (64.7) | 40 (48.8) | 57 (83.8) | <0.001 |
| Yes | 53 (35.3) | 42 (51.2) | 11 (16.2) | ||
| Operability | No | 134 (89.3) | 73 (89.0) | 61 (89.7) | 1 |
| Yes | 16 (10.7) | 9 (11.0) | 7 (10.3) | ||
| Proton or Carbon | Proton | 140 (98.7) | 82 (100) | 66 (97.1) | 0.39 |
| Carbon | 2 (1.3) | 0 (0.0) | 2 (2.9) | ||
| Vascular invasion | No | 69 (46.0) | 42 (51.2) | 27 (39.7) | 0.189 |
| Yes | 81 (54.0) | 40 (48.8) | 41 (60.3) | ||
| Primary location | iBDC | 68 (45.3) | - | 68 (100) | NA |
| eBDC: Perihilar | 56 (37.3) | 56 (68.3) | - | ||
| Gallbladder | 9 (6.0) | 9 (11.0) | - | ||
| Distal | 17 (11.3) | 17 (20.7) | - | ||
| T category | 1 | NA | Hilar:GB:Distal = 3:0:7 | 22 (32.8) | NA |
| 2 | NA | Hilar:GB:Distal = 15:1:6 | 28 (41.8) | ||
| 3 | NA | Hilar:GB:Distal = 10:6:3 | 7 (10.4) | ||
| 4 | NA | Hilar:GB:Distal = 28:2:1 | 10 (14.9) | ||
| N category | 0 | 118 (78.7) | 59 (72.0) | 59 (86.8) | 0.03 |
| 1 | 32 (21.3) | 23 (28.0) | 9 (13.2) | ||
| Tumor size (diameter) | cm3 | 4.00 (1.00, 15.30) | 3.00 (1.00, 9.00) | 5.05 (1.00, 15.30) | <0.001 |
| GTV | cm3 | 31.87 (0.00, 1526.00) | 18.66 (0.00, 467.06) | 63.70 (1.28, 1526.00) | <0.001 |
| CTV | cm3 | 79.99 (9.80, 1526.00) | 57.39 (11.72, 588.62) | 117.28 (9.80, 1526.00) | <0.001 |
| Distance between tumor and intestine | <1 cm | 85 (56.7) | 63 (76.8) | 22 (32.4) | <0.001 |
| ≥1 cm | 65 (43.3) | 19 (23.2) | 46 (67.6) | ||
| Pre-RT chemotherapy | No | 93 (62.0) | 47 (57.3) | 46 (67.6) | 0.238 |
| Yes | 57 (38.0) | 35 (42.7) | 22 (32.4) | ||
| Concurrent chemotherapy | No | 74 (49.3) | 42 (51.2) | 52 (76.5) | 0.002 |
| Yes | 56 (37.3) | 40 (48.8) | 16 (23.5) | ||
| Post-RT chemotherapy | No | 85 (56.7) | 43 (52.4) | 42 (61.8) | 0.193 |
| Yes | 51 (34.0) | 33 (40.2) | 18 (26.5) | ||
| Unknown | 14 (9.3) | 6 (7.3) | 8 (11.8) | ||
| Baseline CEA level | ng/mL | 3.65 (<0.50, 3807.60) | 3.35 (<0.50, 79.40) | 4.00 (<0.60, 3807.60) | 0.073 |
| Radiation dose | GyRBE | 70.20 (44.00, 77.00) | 70.00 (44.00, 77.00) | 72.60 (60.00, 77.00) | <0.001 |
| Number of fractions | fr | 25.00 (10.00, 38.00) | 26.00 (20.00, 38.00) | 22.00 (10.00, 38.00) | <0.001 |
| Prescribed dose in EQD2 | Gy | 76.00 (44.00, 91.30) | 72.92 (44.00, 87.40) | 80.47 (70.00, 91.30) | <0.001 |
| Variable | Strata | Univariate Analysis | Multivariate Analysis | |
|---|---|---|---|---|
| p-Value | Hazard Ratio (95% CI) | p-Value | ||
| Age | Sequential | 0.88 | ||
| Gender | Male vs. Female | 0.77 | ||
| Performance status | 0–1 vs. 2–3 | 0.301 | ||
| Location | iBDC vs. eBDC | 0.68 | ||
| Operability | No vs. Yes | 0.282 | ||
| Diagnosis | Pathological vs. others | 0.928 | ||
| Jaundice | No vs. Yes | 0.974 | ||
| N category | 0 vs. 1 | 0.77 | ||
| Tumor diameter | <6.3 cm vs. 6.3 cm≤ | 0.136 | 1.66 (0.86–3.20) | 0.129 |
| GTV | <28 cm3 vs. 28 cm3≤ | 0.3 | ||
| CTV | <75 cm3 vs. 75 cm3≤ | 0.299 | ||
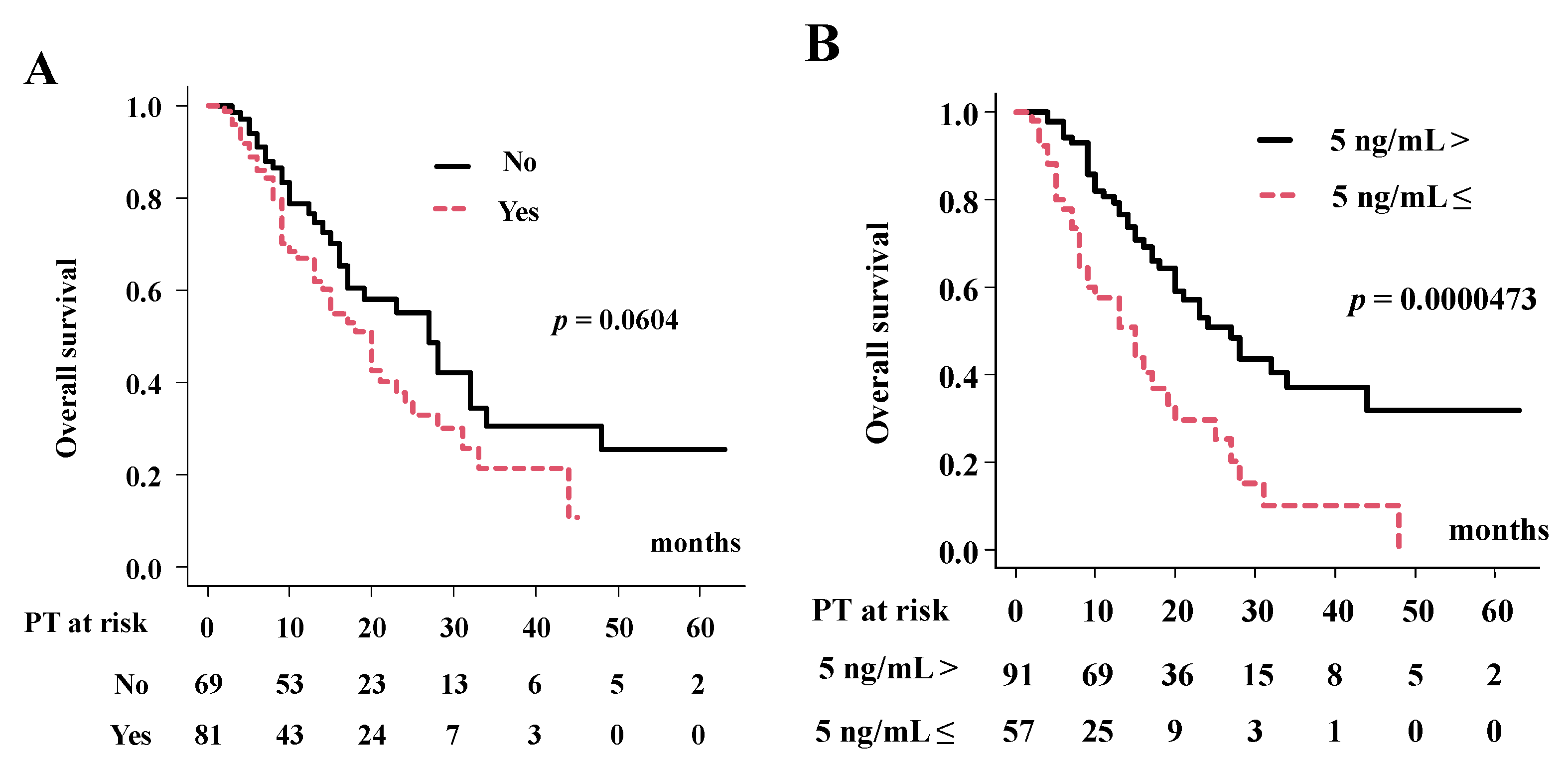
| Vascular invasion | No vs. Yes | 0.0668 | 2.26 (1.24–4.11) | 0.007 |
| Baseline CEA level | <5 ng/mL vs. 5 ng/mL≤ | 0.0264 | 3.18 (1.83–5.52) | <0.0001 |
| Distance from GI | <1 cm vs. 1 cm≤ | 0.2696 | ||
| Radiation dose in EQD2 | EQD2 < 67 Gy vs. EQD2 ≥ 67 Gy | 0.0356 | 0.371 (0.19–0.72) | 0.003 |
| Chemotherapy | No vs. Yes | 0.5849 | ||
| Neoadjuvant | 0.3315 | |||
| Concurrent | 0.3652 | |||
| Adjuvant | 0.3315 | |||
| Status | All Patients | (%) | iBDC | eBDC |
|---|---|---|---|---|
| Alive, no progression | 29 | (19.3%) | 17 | 23 |
| Progression | 80 | (53.3%) | 39 | 41 |
| Local failure (inside radiation field) | 29 | (19.3%) | 13 | 16 |
| Intrahepatic failure outside irradiated field | 29 | (19.3%) | 16 | 13 |
| Lymph node | 12 | (8.0%) | 7 | 5 |
| Distant metastasis | 26 | (17.3%) | 12 | 14 |
| Detail place of distant metastases | Lung 10, Peritoneum 2, Bone 1, Submental Lymph Node 1 | Lung 4, Bone 2, Peritoneum 6, Abdominal wall 2, Pleural 1, Rectum 1 | ||
| Alive with disease progression | 35 | (23.3%) | 18 | 17 |
| Dead of disease with progression | 45 | (30.0%) | 21 | 24 |
| Dead of other causes, no progression | 29 | (19.3%) | 11 | 18 |
| Variable | Strata | Univariate Analysis | Multivariate Analysis | |
|---|---|---|---|---|
| p-Value | Hazard Ratio (95% CI) | p-Value | ||
| Age | Sequential | 0.33 | ||
| Gender | Male vs. Female | 0.83 | ||
| Performance status | 0–1 vs. 2–3 | 0.85 | ||
| Operability | No vs. Yes | 0.346 | ||
| Diagnosis | Pathological vs. others | 0.406 | ||
| Jaundice | No vs. Yes | 0.957 | ||
| N category | 0 vs. 1 | 0.914 | ||
| Tumor diameter | <6.3 cm vs. 6.3 cm≤ | 0.194 | ||
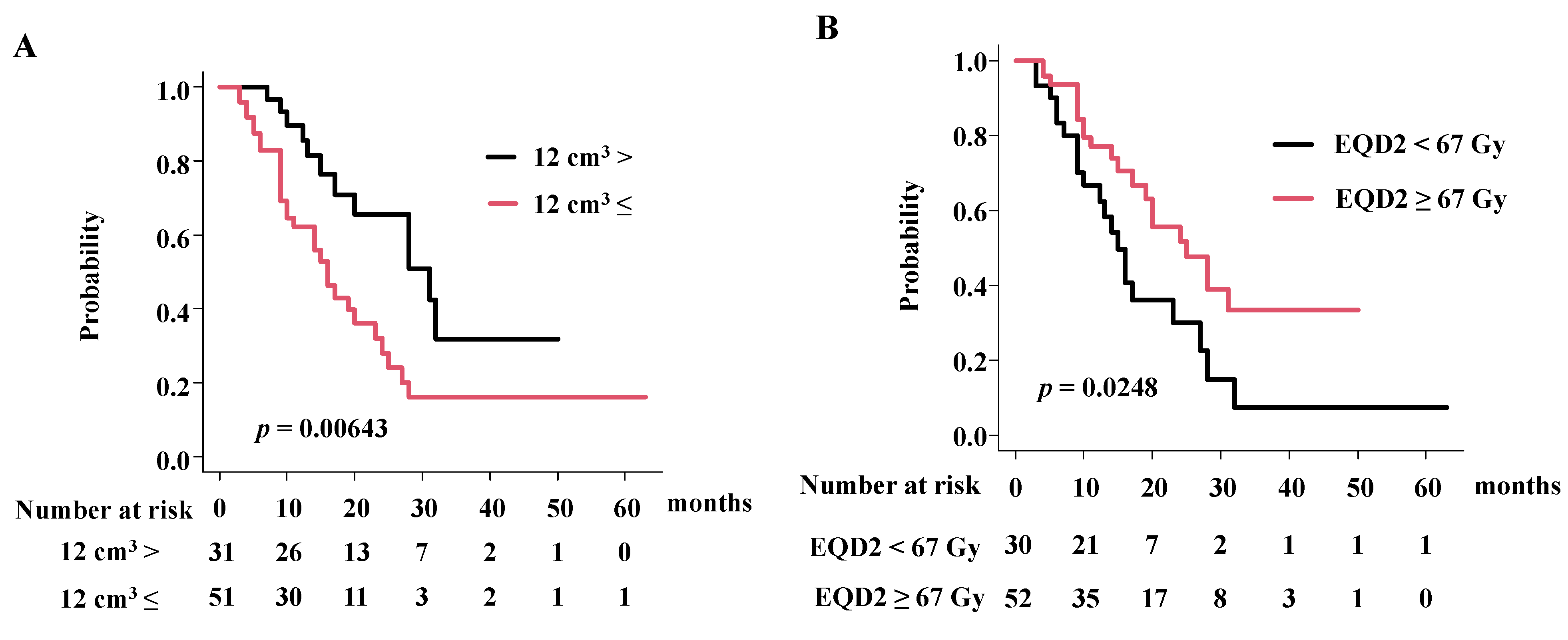
| GTV | <12 cm3 vs. 12 cm3≤ | 0.075 | 2.30 (1.14–4.66) | 0.01 |
| CTV | <75 cm3 vs. 75 cm3≤ | 0.371 | ||
| Vascular invasion | No vs. Yes | 0.354 | ||
| Baseline CEA level | <5 ng/mL vs. 5 ng/mL≤ | 0.097 | 1.55 (0.76–3.15) | 0.219 |
| Distance from GI | <1 cm vs. 1 cm≤ | 0.776 | ||
| Radiation dose in EQD2 | EQD2 < 67 Gy vs. EQD2 ≥ 67 Gy | 0.030 | 0.45 (0.24–0.87) | 0.018 |
| Chemotherapy | No vs. Yes | 0.850 | ||
| Neoadjuvant | 0.351 | |||
| Concurrent | 0.312 | |||
| Adjuvant | 0.125 | 0.57(0.29–1.12) | 0.10 | |
| Variable | Strata | Univariate Analysis | Multivariate Analysis | |
|---|---|---|---|---|
| p-Value | Hazard Ratio (95% CI) | p-Value | ||
| Age | Sequential | 0.277 | ||
| Gender | Male vs. Female | 0.459 | ||
| Performance status | 0–1 vs. 2–3 | 0.906 | ||
| Operability | No vs. Yes | 0.564 | ||
| Diagnosis | Pathological vs. others | 0.441 | ||
| Jaundice | No vs. Yes | 0.644 | ||
| N category | 0 vs. 1 | 0.597 | ||
| Tumor diameter | <6.3 cm vs. 6.3 cm≤ | 0.597 | ||
| GTV | <28 cm3 vs. 28 cm3≤ | 0.67 | ||
| CTV | <75 cm3 vs. 75 cm3≤ | 0.313 | ||
| Vascular invasion | No vs. Yes | 0.074 | 2.15 (0.95–4.87) | 0.065 |
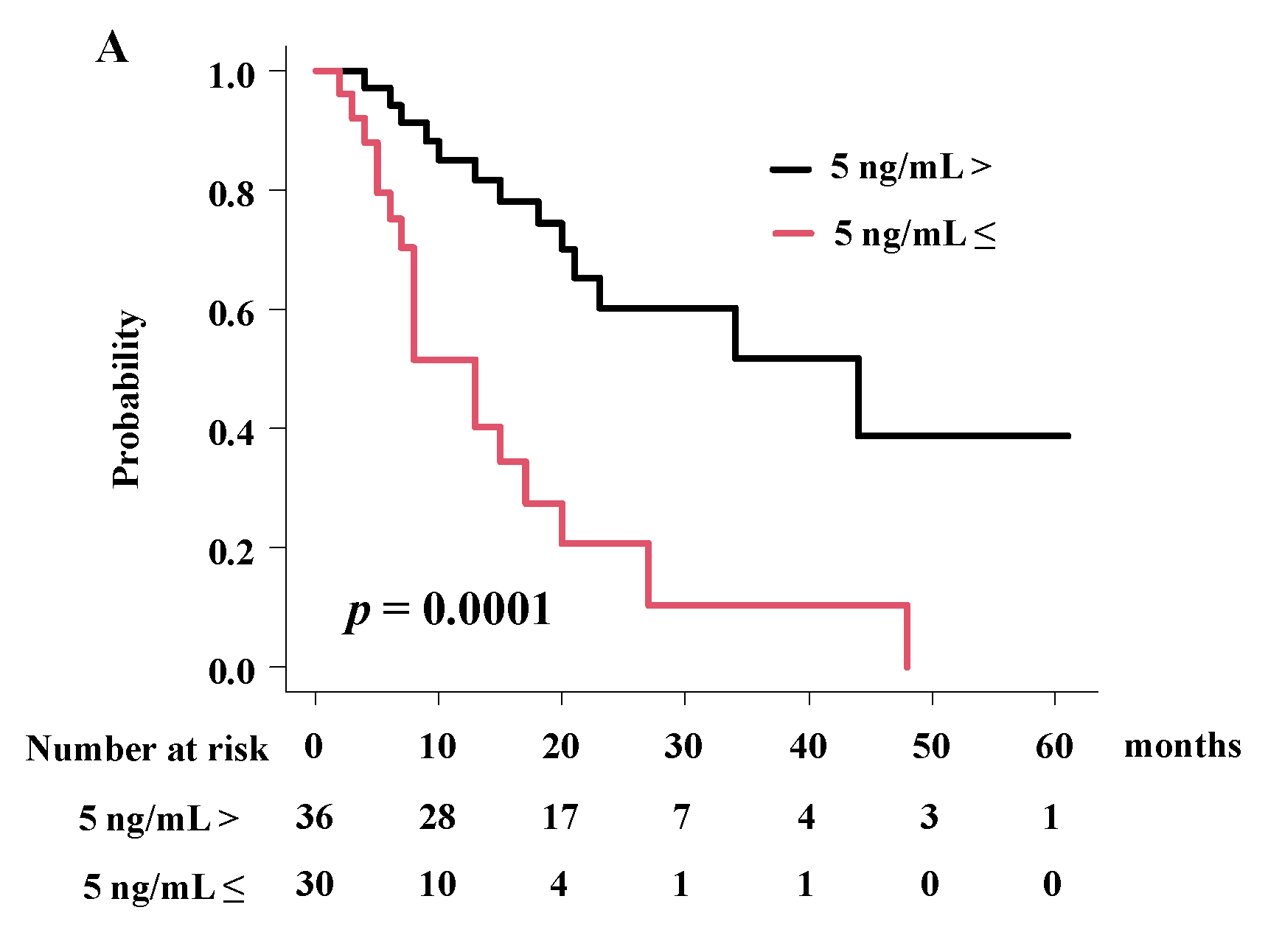
| Baseline CEA level | <5 ng/mL vs. 5 ng/mL≤ | 0.0003 | 4.08 (1.93–8.63) | 0.0002 |
| Distance from GI | <1 cm vs. 1 cm≤ | 0.295 | ||
| Radiation dose in EQD2 | EQD2 < 67 Gy vs. EQD2 ≥ 67 Gy | NA | ||
| Chemotherapy | No vs. Yes | 0.3926 | ||
| Neoadjuvant | 0.273 | |||
| Concurrent | 0.623 | |||
| Adjuvant | 0.273 | |||
| Location | Toxicity | Acute Toxicity Grade ≥ 3 PT NO (%) | Late Toxicity Grade ≥ 3 PT NO (%) |
|---|---|---|---|
| Gastrointestinal | Duodenal perforation | 1 (1.1%) | |
| Duodenal bleeding | 2 (1.3%) | ||
| Bile duct | Bile duct stenosis | 2 (2.2%) | 1 (1.1%) |
| Liver | Failure | 1 (1.1%) | |
| Total | 2 (2.2%) | 4* (2.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamazaki, H.; Kimoto, T.; Suzuki, M.; Murakami, M.; Suzuki, O.; Takagi, M.; Katoh, N.; Arimura, T.; Ogino, T.; Ogino, H. Particle Beam Therapy for Intrahepatic and Extrahepatic Biliary Duct Carcinoma: A Multi-Institutional Retrospective Data Analysis. Cancers 2022, 14, 5864. https://doi.org/10.3390/cancers14235864
Yamazaki H, Kimoto T, Suzuki M, Murakami M, Suzuki O, Takagi M, Katoh N, Arimura T, Ogino T, Ogino H. Particle Beam Therapy for Intrahepatic and Extrahepatic Biliary Duct Carcinoma: A Multi-Institutional Retrospective Data Analysis. Cancers. 2022; 14(23):5864. https://doi.org/10.3390/cancers14235864
Chicago/Turabian StyleYamazaki, Hideya, Takuya Kimoto, Motohisa Suzuki, Masao Murakami, Osamu Suzuki, Masaru Takagi, Norio Katoh, Takeshi Arimura, Takashi Ogino, and Hiroyuki Ogino. 2022. "Particle Beam Therapy for Intrahepatic and Extrahepatic Biliary Duct Carcinoma: A Multi-Institutional Retrospective Data Analysis" Cancers 14, no. 23: 5864. https://doi.org/10.3390/cancers14235864
APA StyleYamazaki, H., Kimoto, T., Suzuki, M., Murakami, M., Suzuki, O., Takagi, M., Katoh, N., Arimura, T., Ogino, T., & Ogino, H. (2022). Particle Beam Therapy for Intrahepatic and Extrahepatic Biliary Duct Carcinoma: A Multi-Institutional Retrospective Data Analysis. Cancers, 14(23), 5864. https://doi.org/10.3390/cancers14235864