


Genital Lymphedema after Cancer Treatment: A Narrative Review


Simple Summary
Abstract
1. Introduction
2. Frequency and Risk Factors
3. Physical Examination
3.1. In Males
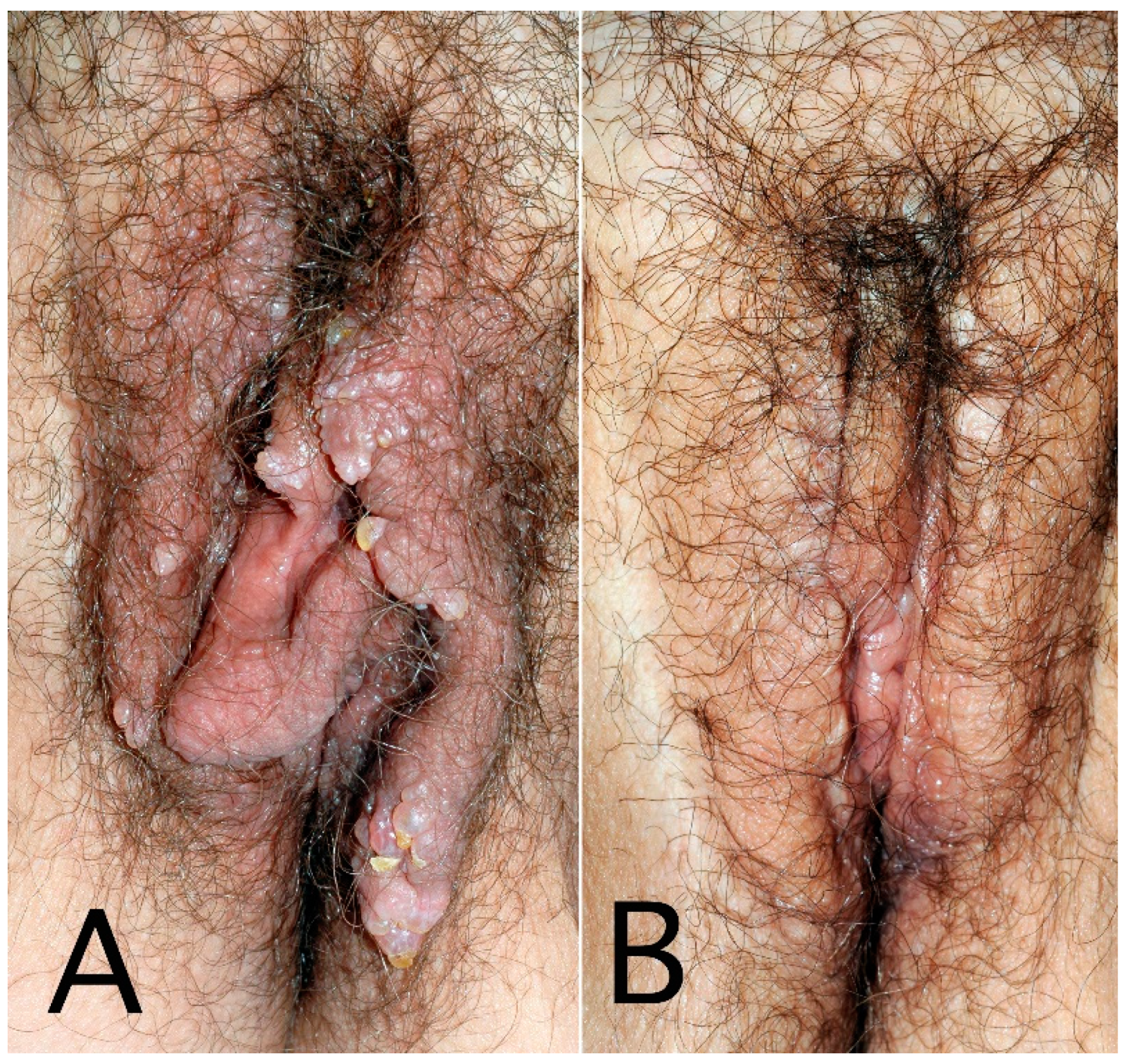
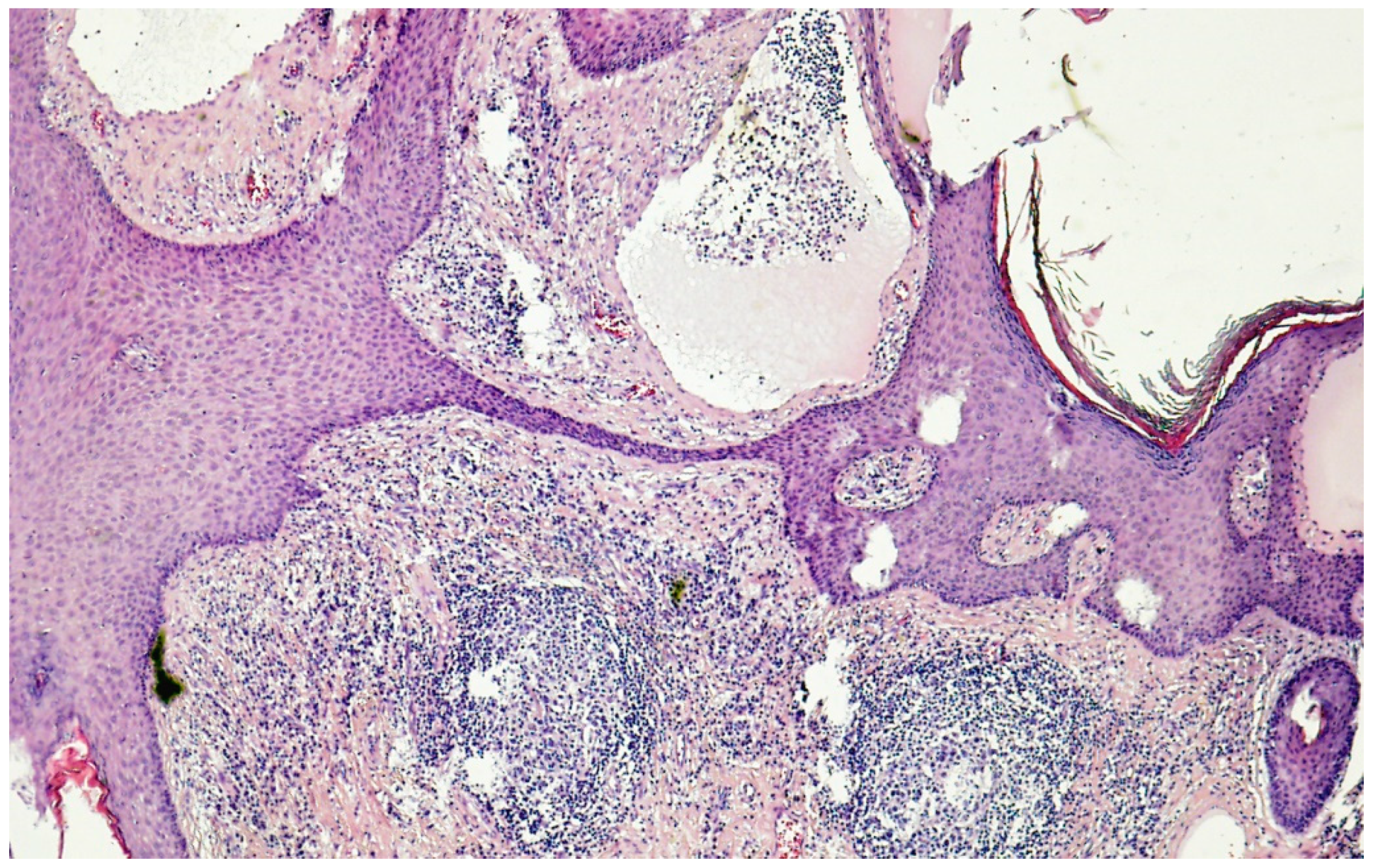
3.2. In Females
4. Complications
5. Quality of Life
6. Explorations
6.1. Diagnosis
6.2. Pitfalls to Avoid
7. Treatments
7.1. Non-Surgical Therapies
7.2. Surgery
7.3. Other Treatments
8. Conclusions
Funding
Conflicts of Interest
References
- Zampell, J.C.; Aschen, S.; Weitman, E.S.; Yan, A.; Elhadad, S.; De Brot Andrade, M.; Mehrara, B.J. Regulation of adipogenesis by lymphatic fluid stasis: Part I. Adipogenesis, fibrosis, and inflammation. Plast. Reconstr. Surg. 2012, 129, 825–834. [Google Scholar] [CrossRef]
- Vignes, S.; Trévidic, P. Lymphedema of male external genitalia: A retrospective study of 33 cases. Ann. Dermatol. Venereol. 2005, 132, 21–25. [Google Scholar] [CrossRef]
- Pérez-Bertólez, S.; Alonso, V. Milroy disease with predominant preputial involvement. Pediatr. Dermatol. 2022, 39, 836–837. [Google Scholar] [CrossRef]
- Gordon, K.; Varney, R.; Keeley, V.; Riches, K.; Jeffery, S.; Van Zanten, M.; Mortimer, P.; Ostergaard, P.; Mansour, S. Update and audit of the St George’s classification algorithm of primary lymphatic anomalies: A clinical and molecular approach to diagnosis. J. Med. Genet. 2020, 57, 653–659. [Google Scholar] [CrossRef]
- Wassef, M.; Blei, F.; Adams, D.; Alomari, A.; Baselga, E.; Berenstein, A.; Burrows, P.; Frieden, I.J.; Garzon, M.C.; Lopez-Gutierrez, J.C.; et al. ISSVA Board and Scientific Committee. Vascular anomalies classification: Recommendations from the International Society for the Study of Vascular Anomalies. Pediatrics 2015, 136, e203–e214. [Google Scholar] [CrossRef]
- Shenoy, R.K. Clinical and pathological aspects of filarial lymphedema and its management. Korean J. Parasitol. 2008, 46, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, Z.M.; Vieira, A.; Xavier, A.T.; Bezerra, G.; Lopes, M.; Bonfim, C.V.; Aguiar-Santos, A.M. Lymphatic filariasis: A systematic review on morbidity and its repercussions in countries in the Americas. Int. J. Environ. Res. Public Health 2021, 19, 316. [Google Scholar] [CrossRef] [PubMed]
- Rockson, S.G.; Rivera, K.K. Estimating the population burden of lymphedema. Ann. N. Y. Acad. Sci. 2008, 1131, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Bernas, M.; Thiadens, S.R.J.; Stewart, P.; Granzow, J. Secondary lymphedema from cancer therapy. Clin. Exp. Metastasis 2022, 39, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Vignes, S.; Bellanger, J. Primary intestinal lymphangiectasia (Waldmann’s disease). Orphanet J. Rare Dis. 2008, 3, 5. [Google Scholar] [CrossRef]
- Keiler, S.; Tyson, P.; Tamburro, J. Metastatic cutaneous Crohn’s disease in children: Case report and review of the literature. Pediatr. Dermatol. 2009, 26, 604–609. [Google Scholar] [CrossRef]
- Alexakis, C.; Gordon, K.; Mellor, R.; Chong, H.; Mortimer, P.; Pollok, R. Ano-genital granulomatosis and Crohn’s disease: A case series of males presenting with genital lymphoedema. J. Crohn’s Colitis 2017, 11, 454–459. [Google Scholar] [CrossRef]
- Pacheco, Y.D.; García-Duque, O.; Fernández-Palacios, J. Penile and scrotal lymphedema associated with hidradenitis suppurativa: Case report and review of surgical options. Cir. Cir. 2018, 86, 84–88. [Google Scholar] [CrossRef]
- Kiely, P.D.; Bland, J.M.; Joseph, A.E.; Mortimer, P.S.; Bourke, B.E. Upper limb lymphatic function in inflammatory arthritis. J. Rheumatol. 1995, 22, 214–217. [Google Scholar] [PubMed]
- Schmit, P.; Prieur, A.M.; Brunelle, F. Juvenile rheumatoid arthritis and lymphoedema: Lymphangiographic aspects. Pediatr. Radiol. 1999, 29, 364–366. [Google Scholar] [CrossRef] [PubMed]
- Dubost, J.J.; Sauvezie, B. Oligoarthrite B27 avec œdèmes et signes généraux: Une forme atypique de spondylarthropathie à début tardif. Ann. Med. Interne 1989, 140, 566–570. [Google Scholar]
- Böhm, M.; Riemann, B.; Luger, T.A.; Bonsmann, G. Bilateral upper limb lymphoedema associated with psoriatic arthritis: A case report and review of the literature. Br. J. Dermatol. 2000, 143, 1297–1301. [Google Scholar] [CrossRef]
- Barete, S.; Calvez, V.; Mouquet, C.; Barrou, B.; Kreis, H.; Dantal, J.; Dorent, R.; Durand, F.; Dimitrov, Y.; Dupin, N.; et al. Clinical features and contribution of virological findings to the management of Kaposi sarcoma in organ-allograft recipients. Arch. Dermatol. 2000, 136, 1452–1458. [Google Scholar] [CrossRef] [PubMed]
- Foureur, N.; Descamps, V.; Lebrun-Vignes, B.; Grossin, M.; Picard-Dahan, C.; Lecerf, V.; Belaich, S.; Crickx, B. Lymphœdème du membre inférieur révélant une fibrose rétropéritonéale d’origine métastatique. Ann. Dermatol. Venereol. 2002, 129, 422–423. [Google Scholar]
- Halm, U.; Berr, F.; Tannapfel, A.; Klöppel, R.; Secknus, R.; Mössner, J. Primary amyloidosis of the mesentery and the retroperitoneum presenting with lymphedema. Am. J. Gastroenterol. 1998, 93, 2299–2300. [Google Scholar] [CrossRef]
- Desai, N.; Heenan, S.; Mortimer, P.S. Sirolimus-associated lymphoedema: Eight new cases and a proposed mechanism. Br. J. Dermatol. 2009, 160, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- Tanabe, N.; Muya, M.; Isonokami, M.; Kozuka, T.; Honda, T.; Ohtani, H. Lymphedema due to chronic penile strangulation: A case report. J. Dermatol. 1996, 23, 648–651. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Galì, A.; Marino, S.; Bramanti, P. Compulsive masturbation and chronic penile lymphedema. Arch. Sex. Behav. 2012, 41, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, R.Q.; Calderoni, D.R.; Garcia, I.F.; Stelini, R.F.; Fregonesi, A.; Kharmandayan, P. Liquid silicone used for esthetic purposes as a potentiator for occurrence of post-radiotherapy genital lymphedema: Case report. Sao Paulo Med. J. 2017, 135, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Kurt, H.; Arnold, C.A.; Payne, J.E.; Miller, M.J.; Skoracki, R.J.; Iwenofu, O.H. Massive localized lymphedema: A clinicopathologic study of 46 patients with an enrichment for multiplicity. Mod. Pathol. 2016, 29, 75–82. [Google Scholar] [CrossRef]
- Flynn, K.J.; Vanni, A.J.; Breyer, B.N.; Erickson, B.A. Adult-acquired buried penis classification and surgical management. Urol. Clin. N. Am. 2022, 49, 479–493. [Google Scholar] [CrossRef] [PubMed]
- Chandler, D.J.; Grijsen, M.L.; Fuller, L.C. With bare feet in the soil: Podoconiosis, a neglected cause of tropical lymphoedema. Dermatology 2021, 237, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Herodotou, C.A.; Burns, R.T.; Whaley, R.; Idrees, M.; Mellon, M.J. Sarcoidosis: A rare cause of penile edema. Urol. Case Rep. 2022, 44, 102167. [Google Scholar] [CrossRef]
- AbuRahma, A.F.; Woodruff, B.A.; Lucente, F.C. Edema after femoropopliteal bypass surgery: Lymphatic and venous theories of causation. J. Vasc. Surg. 1990, 11, 461–467. [Google Scholar] [CrossRef]
- Abraham, G.; Blake, P.G.; Mathews, R.; Bargman, J.M.; Izatt, S.; Oreopoulos, D.G. Genital swelling as a surgical complication of continuous ambulatory peritoneal dialysis. Surg. Gynecol. Obstet. 1990, 170, 306–308. [Google Scholar] [CrossRef]
- Kuroda, K.; Yamamoto, Y.; Yanagisawa, M.; Kawata, A.; Akiba, N.; Suzuki, K.; Naritaka, K. Risk factors and a prediction model for lower limb lymphedema following lymphadenectomy in gynecologic cancer: A hospital-based retrospective cohort study. BMC Women’s Health 2017, 17, 50. [Google Scholar] [CrossRef] [PubMed]
- Kunitake, T.; Kakuma, T.; Ushijima, K. Risk factors for lower limb lymphedema in gynecologic cancer patients after initial treatment. Int. J. Clin. Oncol. 2020, 25, 963–971. [Google Scholar] [CrossRef] [PubMed]
- Noble-Jones, R.; Thomas, M.J.; Quéré, I.; Morgan, K.; Moffatt, C. An international investigation of the education needs of health professionals conservatively managing genital lymphoedema: Survey findings. J. Wound Care 2021, 30, S19–S28. [Google Scholar]
- Simon, L.; Trévidic, P.; Denis, P.; Vignes, S. Vulvar lymphangioma circumscriptum: Comparison of primary and acquired forms in a cohort of 57 patients. J. Eur. Acad. Dermatol. Venereol. 2018, 32, e56–e58. [Google Scholar] [CrossRef] [PubMed]
- Beesley, V.; Janda, M.; Eakin, E.; Obermair, A.; Battistutta, D. Lymphedema after gynecological cancer treatment: Prevalence, correlates, and supportive care needs. Cancer 2007, 109, 2607–2614. [Google Scholar] [CrossRef]
- Torgbenu, E.; Luckett, T.; Buhagiar, M.A.; Phillips, J.L. Guidelines relevant to diagnosis, assessment, and management of lymphedema: A systematic review. Adv. Wound Care 2023, 12, 15–27. [Google Scholar] [CrossRef]
- Yamamoto, T.; Yamamoto, N.; Furuya, M.; Hayashi, A.; Koshima, I. Genital Lymphedema Score: Genital Lymphedema Severity scoring system based on subjective symptoms. Ann. Plast. Surg. 2016, 77, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Stemmer, R. A clinical symptom for the early and differential diagnosis of lymphedema. Vasa 1976, 5, 261–262. [Google Scholar]
- Pestana, I.A.; Greenfield, J.M.; Walsh, M.; Donatucci, C.F.; Erdmann, D. Management of “buried” penis in adulthood: An overview. Plast. Reconstr. Surg. 2009, 124, 1186–1195. [Google Scholar] [CrossRef]
- Mu, X.C.; Tran, T.A.; Dupree, M.; Carlson, J.A. Acquired vulvar lymphangioma mimicking genital warts. A case report and review of the literature. J. Cutan. Pathol 1999, 26, 150–154. [Google Scholar] [CrossRef]
- Plaza, J.A.; Requena, L.; Kazakov, D.V.; Vega, E.; Kacerovska, D.; Reyes, G.; Michal, M.; Suster, S.; Sangueza, M. Verrucous localized lymphedema of genital areas: Clinicopathologic report of 18 cases of this rare entity. J. Am. Acad. Dermatol. 2014, 71, 320–326. [Google Scholar] [CrossRef]
- Dupuy, A.; Benchikhi, H.; Roujeau, J.C.; Bernard, P.; Vaillant, L.; Chosidow, O.; Sassolas, B.; Guillaume, J.C.; Grob, J.J.; Bastuji-Garin, S. Risk factors for erysipelas of the leg (cellulitis): Case-Control study. BMJ 1999, 318, 1591–1594. [Google Scholar] [CrossRef] [PubMed]
- Sekse, R.J.T.; Dunberger, G.; Olesen, M.L.; Østerbye, M.; Seibaek, L. Lived experiences and quality of life after gynaecological cancer—An integrative review. J. Clin. Nurs. 2019, 28, 1393–1421. [Google Scholar] [CrossRef] [PubMed]
- Draeger, D.L.; Sievert, K.D.; Hakenberg, O.W. Cross-sectional patient-reported outcome measuring of health-related quality of life with establishment of cancer- and treatment-specific functional and symptom scales in patients with penile cancer. Clin. Genitourin. Cancer 2018, 16, e1215–e1220. [Google Scholar] [CrossRef]
- Amano, K.; Suzuki, K.; Ito, Y. Changes in quality of life and lower urinary tract symptoms over time in cancer patients after a total prostatectomy: Systematic review and meta-analysis. Support. Care Cancer 2022, 30, 2959–2970. [Google Scholar] [CrossRef]
- Szuba, A.; Shin, W.S.; Strauss, H.W.; Rockson, S. The third circulation: Radionuclide lymphoscintigraphy in the evaluation of lymphedema. J. Nucl. Med. 2003, 44, 43–57. [Google Scholar]
- Lu, Q.; Jiang, Z.; Zhao, Z.; Wu, L.; Wu, G.; Suo, S.; Xu, J. Assessment of the lymphatic system of the genitalia using magnetic resonance lymphography before and after treatment of male genital lymphedema. Medicine 2016, 95, e3755. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Yamamoto, N.; Yoshimatsu, H.; Hayami, S.; Narushima, M.; Koshima, I. Indocyanine green lymphography for evaluation of genital lymphedema in secondary lower extremity lymphedema patients. J. Vasc. Surg. Venous. Lymph. Dis. 2013, 1, 400–405.e1. [Google Scholar] [CrossRef]
- Gómez, F.M.; Martínez-Rodrigo, J.; Martí-Bonmatí, L.; Santos, E.; Forner, I.; Lloret, M.; Pérez-Enguix, D.; García-Marcos, R. Transnodal lymphangiography in the diagnosis and treatment of genital lymphedema. Cardiovasc. Interv. Radiol. 2012, 35, 1488–1491. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Ouvrier, D.; Massalou, D.; Viau, P.; Chevallier, A.; Patouraux, S.; Passeron, T.; Lacour, J.P.; Montaudié, H. Lymphœdème des membres inférieurs révélant une linite gastrique. Ann. Dermatol. Venereol. 2017, 144, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Torio-Padron, N.; Stark, G.B.; Földi, E.; Simunovic, F. Treatment of male genital lymphedema: An integrated concept. J. Plast. Reconstr. Aesthet. Surg. 2015, 68, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Lasinski, B.B.; McKillip Thrift, K.; Squire, D.; Austin, M.K.; Smith, K.M.; Wanchai, A.; Green, J.M.; Stewart, B.R.; Cormier, J.N.; Armer, J.M. A systematic review of the evidence for complete decongestive therapy in the treatment of lymphedema from 2004 to 2011. PM R 2012, 4, 580–601. [Google Scholar] [CrossRef] [PubMed]
- Partsch, H.; Clark, M.; Bassez, S.; Benigni, J.P.; Becker, F.; Blazek, V.; Caprini, J.; Cornu-Thénard, A.; Hafner, J.; Flour, M.; et al. Measurement of lower leg compression in vivo: Recommendations for the performance of measurements of interface pressure and stiffness: Consensus statement. Dermatol. Surg. 2006, 32, 224–232. [Google Scholar] [CrossRef]
- Boris, M.; Weindorf, S.; Lasinski, B.B. The risk of genital edema after external pump compression for lower limb lymphedema. Lymphology 1998, 31, 15–20. [Google Scholar] [PubMed]
- Thompson, B.; Gaitatzis, K.; Janse de Jonge, X.; Blackwell, R.; Koelmeyer, L.A. Manual lymphatic drainage treatment for lymphedema: A systematic review of the literature. J. Cancer Surviv. 2021, 15, 244–258. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.W.; Dayan, J.; Greene, A.K.; MacDonald, J.K.; Masia, J.; Mehrara, B.; Neligan, P.C.; Nguyen, D. Surgical treatment of lymphedema: A systematic review and meta-analysis of controlled trials. Results of a Consensus Conference. Plast. Reconstr. Surg. 2021, 147, 975–993. [Google Scholar] [CrossRef] [PubMed]
- McDougal, W.S. Lymphedema of the external genitalia. J. Urol. 2003, 170, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Daniel, B.W.; Rodriguez, J.R.; Kageyama, T.; Sakai, H.; Fuse, Y.; Tsukuura, R.; Yamamoto, N. Radical reduction and reconstruction for male genital elephantiasis: Superficial circumflex iliac artery perforator (SCIP) lymphatic flap transfer after elephantiasis tissue resection. JPRAS 2022, 75, 870–880. [Google Scholar] [CrossRef]
- Mukenge, S.M.; Catena, M.; Negrini, D.; Ratti, F.; Moriondo, A.; Briganti, A.; Rigatti, P.; Cipriani, F.; Ferla, G. Assessment and follow-up of patency after lymphovenous microsurgery for treatment of secondary lymphedema in external male genital organs. Eur. Urol. 2011, 60, 1114–1119. [Google Scholar] [CrossRef]
- Gennaro, P.; Gabriele, G.; Aboh, I.V.; Cascino, F.; Zerini, F.; Aboud, M.G. Ultramicrosurgery: A new approach to treat primary male genital lymphedema. JPRAS Open 2019, 20, 72–80. [Google Scholar] [CrossRef]
- Garaffa, G.; Christopher, N.; Ralph, D.J. The management of genital lymphoedema. BJU Int. 2008, 102, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Porter, W.; Dinneen, M.; Bunker, C. Chronic penile lymphedema: A report of 6 cases. Arch. Dermatol. 2001, 137, 1108–1110. [Google Scholar]
- Alwaal, A.; McAninch, J.W.; Harris, C.R.; Breyer, B.N. Utilities of split-thickness skin grafting for male genital reconstruction. Urology 2015, 86, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Schook, C.C.; Kulungowski, A.M.; Greene, A.K.; Fishman, S.J. Male genital lymphedema: Clinical features and management in 25 pediatric patients. J. Pediatr. Surg. 2014, 49, 1647–1651. [Google Scholar] [CrossRef] [PubMed]
- Vignes, S.; Arrault, M.; Trévidic, P. Surgical resection of vulva lymphoedema circumscriptum. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 1883–1885. [Google Scholar] [CrossRef]
- Aulia, I.; Yessica, E.C. Surgical management of male genital lymphedema: A systematic review. Arch. Plast. Surg. 2020, 47, 3–8. [Google Scholar] [CrossRef]
- Guiotto, M.; Bramhall, R.J.; Campisi, C.; Raffoul, W.; di Summa, P.G. A systematic review of outcomes after genital lymphedema surgery: Microsurgical reconstruction versus excisional procedures. Ann. Plast. Surg. 2019, 83, e85–e91. [Google Scholar] [CrossRef]
- Huilgol, S.C.; Neill, S.; Barlow, R.J. CO2 laser therapy of vulva lymphangiectasia and lymphangioma circumscriptum. Dermatol. Surg. 2002, 28, 575–577. [Google Scholar]
- Vlastos, A.T.; Malpica, A.; Follen, M. Lymphangioma circumscriptum of the vulva: A review of the literature. Obstet. Gynecol. 2003, 101, 946–954. [Google Scholar] [CrossRef]
- Chang, M.B.; Newman, C.C.; Davis, M.D.; Lehman, J.S. Acquired lymphangiectasia (lymphangioma circumscriptum) of the vulva: Clinicopathologic study of 11 patients from a single institution and 67 from the literature. Int. J. Dermatol. 2016, 55, e482–e487. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Cancer Causes | Diseases |
|---|---|
| Syndromic primary lymphedema with genetic abnormality [4] | RASopathies (rat sarcoma oncogene protein-associated pathologies: Noonan’s syndrome, PTPN11, SOS1, RIT1 gene, ORPHA:568062) Emberger syndrome (GATA2 gene, ORPHA 3226) Lymphedema-distichiasis syndrome (FOXC2, ORPHA:33001) Generalized lymphatic dysplasia (PIEZO1 gene, ORPHA:568062) Hennekam syndrome (CCBE1 gene, ORPHA:2136) |
| Primary intestinal lymphangiectasia (Waldmann’s disease, ORPHA:90362) [10] | Protein-losing enteropathy |
| Chronic inflammatory diseases | Inflammatory bowel diseases: Crohn’s disease (ano-genital granulomatosis), ulcerative colitis [11,12] Hidradenitis suppurativa [13] Chronic rheumatism: ankylosing spondylitis, rheumatoid arthritis, psoriatic arthritis [14,15,16,17] |
| Infectious diseases | Filariasis (Wuchereria bancrofti, Brugia malayi, B. timori) [7] Kaposi’s disease (endemic, epidemic, acquired immunodeficiency disease syndrome, post-transplantation) [18] Mycobacterium, Chlamydiae trachomatis, syphilis, actinomycosis, donovanosis, tuberculosis |
| Retroperitoneal fibrosis | Idiopathic Secondary: cancer, drugs, amyloidosis [19,20] |
| mTOR (mechanistic target of rapamycin) inhibitors (sirolimus, everolimus) | Post-transplantation [21] |
| Sexual behavior | Pathomimia, striction [22] Intensive masturbation [23] Local injection of silicone [24] |
| Morbid obesity, i.e., body mass index > 40 kg/m2 [25,26] | Contributes to buried penis |
| Podoconiosis [27] | Due to long-term exposure to red clay soils |
| Others | Sarcoidosis [28] Femoropopliteal bypass surgery [29] Peritoneal dialysis [30] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vignes, S. Genital Lymphedema after Cancer Treatment: A Narrative Review. Cancers 2022, 14, 5809. https://doi.org/10.3390/cancers14235809
Vignes S. Genital Lymphedema after Cancer Treatment: A Narrative Review. Cancers. 2022; 14(23):5809. https://doi.org/10.3390/cancers14235809
Chicago/Turabian StyleVignes, Stéphane. 2022. "Genital Lymphedema after Cancer Treatment: A Narrative Review" Cancers 14, no. 23: 5809. https://doi.org/10.3390/cancers14235809
APA StyleVignes, S. (2022). Genital Lymphedema after Cancer Treatment: A Narrative Review. Cancers, 14(23), 5809. https://doi.org/10.3390/cancers14235809