

Prognostic Hematologic Biomarkers Following Immune Checkpoint Inhibition in Metastatic Uveal Melanoma

 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population and Data Sources
2.2. Data Collection and Treatment Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patient, Tumor, and Treatment Characteristics
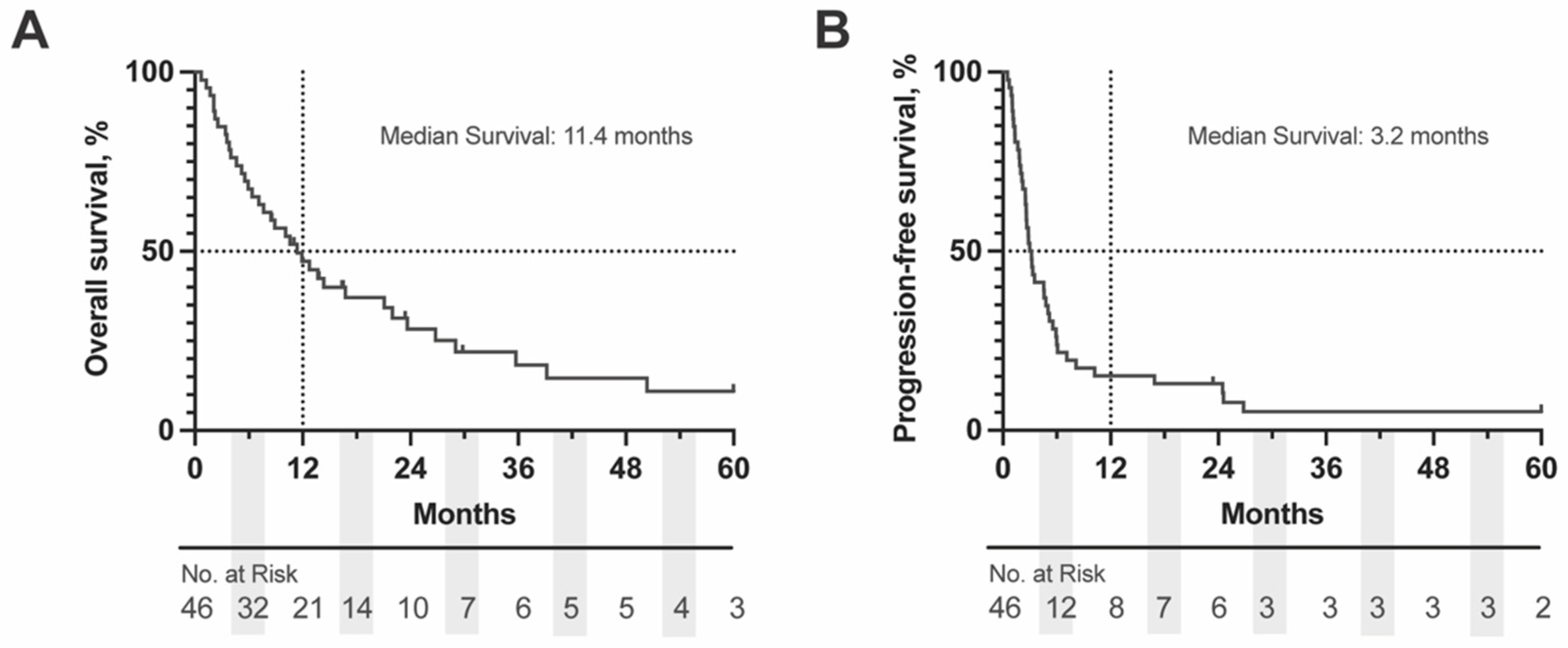
3.2. Survival Outcomes
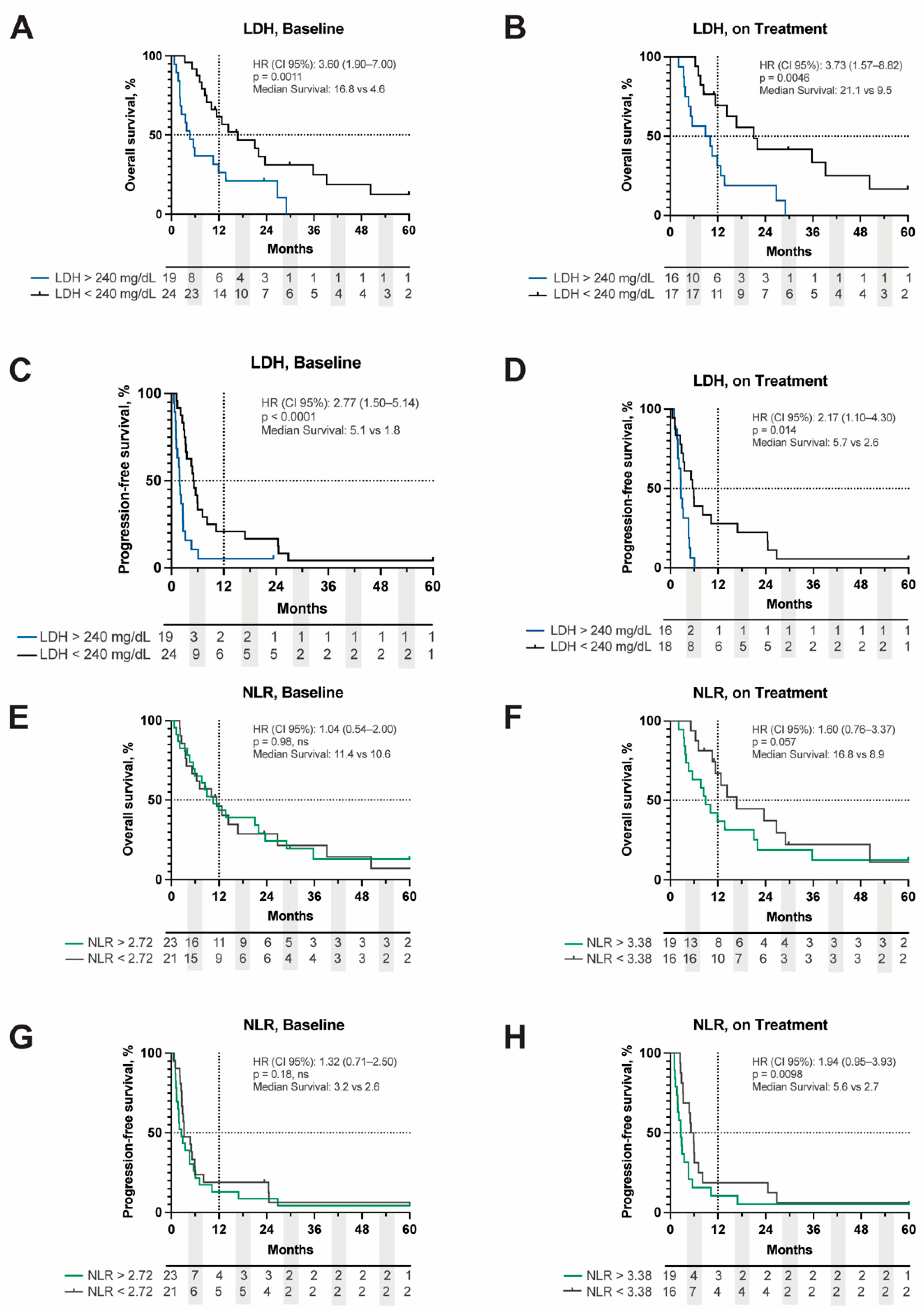
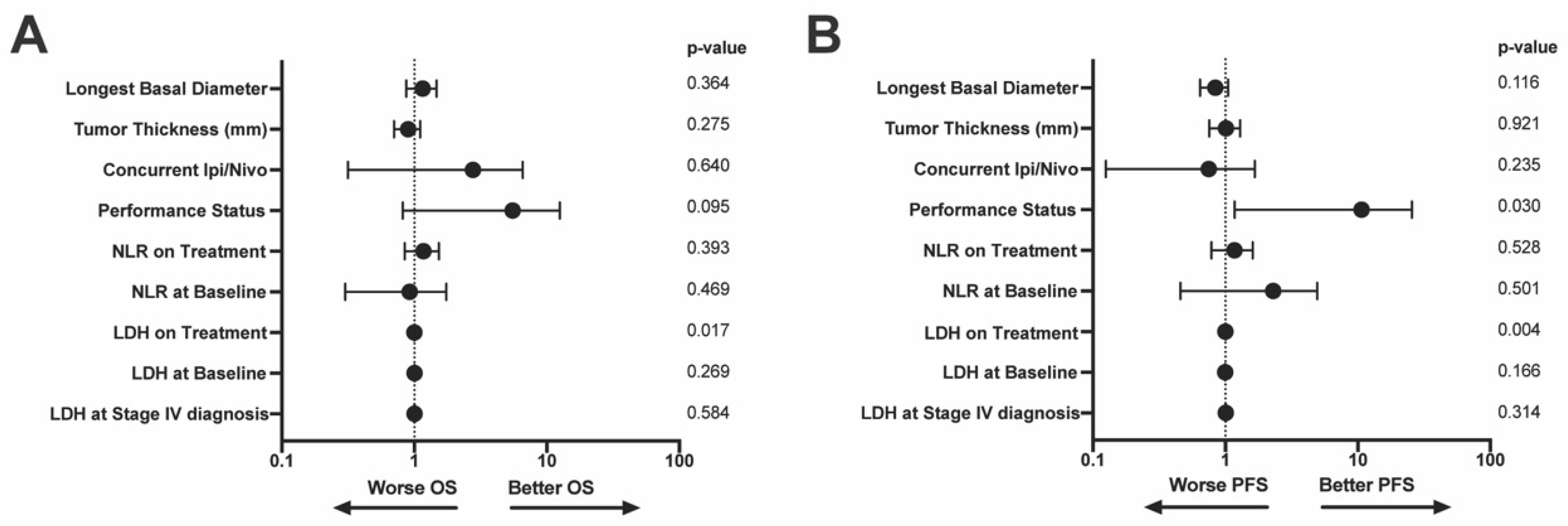
3.3. Hematologic Markers Prognostic for ICI-Response
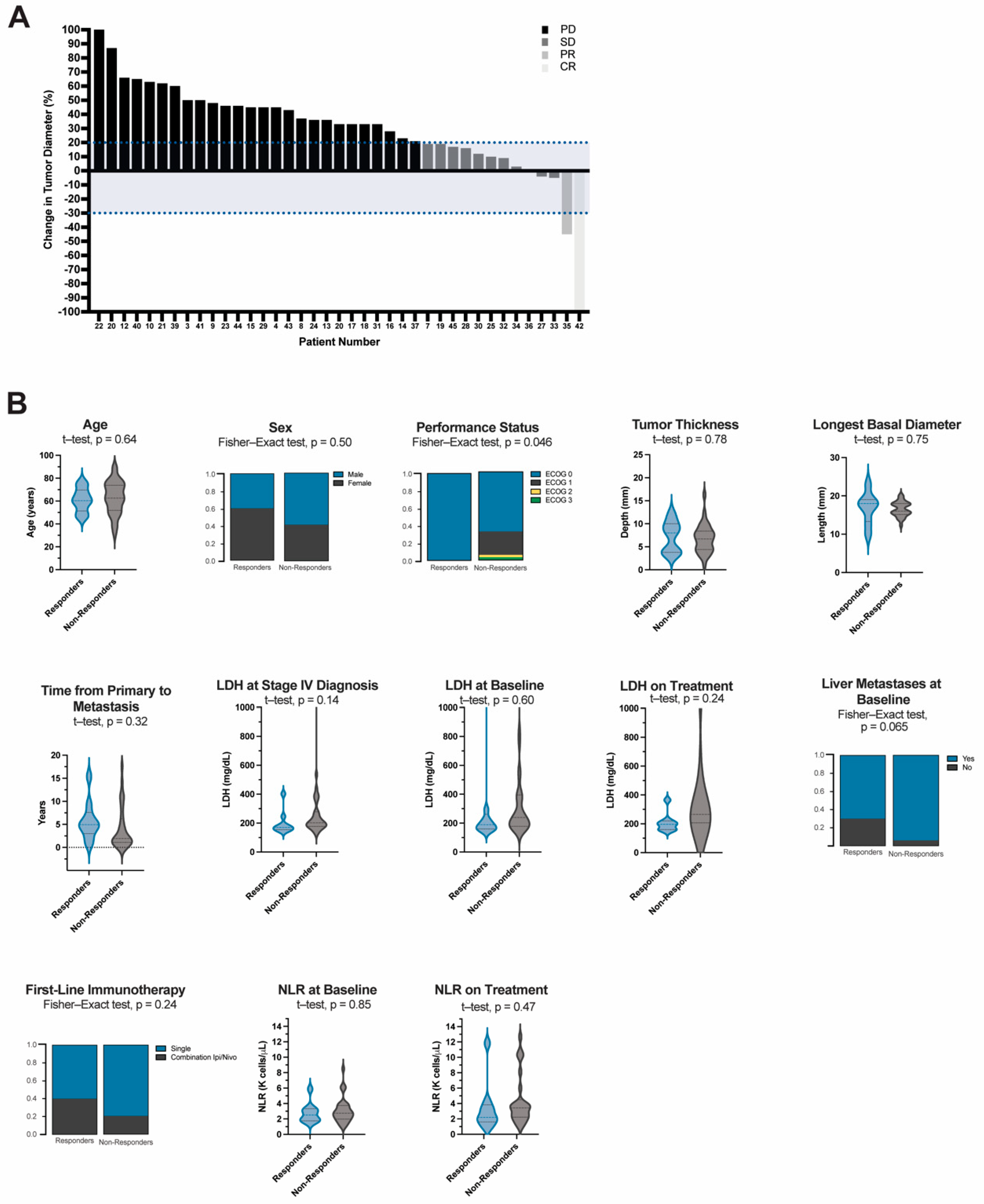
3.4. Patient Factors Associated with Clinical Benefit from ICI
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krantz, B.A.; Dave, N.; Komatsubara, K.M.; Marr, B.P.; Carvajal, R.D. Uveal melanoma: Epidemiology, etiology, and treatment of primary disease. Clin. Ophthalmol. 2017, 11, 279–289. [Google Scholar] [CrossRef]
- Straatsma, B.R.; Fine, S.L.; Earle, J.D.; Hawkins, B.S.; Diener-West, M.; McLaughlin, J.A. Enucleation versus plaque irradiation for choroidal melanoma. Ophthalmology 1988, 95, 1000–1004. [Google Scholar] [CrossRef]
- Collaborative Ocular Melanoma Study Group. Assessment of metastatic disease status at death in 435 patients with large choroidal melanoma in the Collaborative Ocular Melanoma Study (COMS): COMS report no. 15. Arch. Ophthalmol. 2001, 119, 670–676. [Google Scholar] [CrossRef]
- Rossi, E.; Croce, M.; Reggiani, F.; Schinzari, G.; Ambrosio, M.; Gangemi, R.; Tortora, G.; Pfeffer, U.; Amaro, A. Uveal Melanoma Metastasis. Cancers 2021, 13, 5684. [Google Scholar] [CrossRef]
- Croce, M.; Ferrini, S.; Pfeffer, U.; Gangemi, R. Targeted Therapy of Uveal Melanoma: Recent Failures and New Perspectives. Cancers 2019, 11, 846. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.V.; Sullivan, R.J. Developments in the Space of New MAPK Pathway Inhibitors for BRAF-Mutant Melanoma. Clin. Cancer Res. 2019, 25, 5735–5742. [Google Scholar] [CrossRef]
- Carvajal, R.D.; Sosman, J.A.; Quevedo, J.F.; Milhem, M.M.; Joshua, A.M.; Kudchadkar, R.R.; Linette, G.P.; Gajewski, T.F.; Lutzky, J.; Lawson, D.H.; et al. Effect of selumetinib vs chemotherapy on progression-free survival in uveal melanoma: A randomized clinical trial. JAMA 2014, 311, 2397–2405. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, R.D.; Piperno-Neumann, S.; Kapiteijn, E.; Chapman, P.B.; Frank, S.; Joshua, A.M.; Piulats, J.M.; Wolter, P.; Cocquyt, V.; Chmielowski, B.; et al. Selumetinib in Combination with Dacarbazine in Patients with Metastatic Uveal Melanoma: A Phase III, Multicenter, Randomized Trial (SUMIT). J. Clin. Oncol. 2018, 36, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.-A.; Reed, K.; et al. Nivolumab plus ipilimumab in advanced melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef]
- Marseglia, M.; Amaro, A.; Solari, N.; Gangemi, R.; Croce, E.; Tanda, E.; Spagnolo, F.; Filaci, G.; Pfeffer, U.; Croce, M. How to Make Immunotherapy an Effective Therapeutic Choice for Uveal Melanoma. Cancers 2021, 13, 2043. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Pagliara, M.M.; Orteschi, D.; Dosa, T.; Sammarco, M.G.; Caputo, C.G.; Petrone, G.; Rindi, G.; Zollino, M.; Blasi, M.A.; et al. Pembrolizumab as first-line treatment for metastatic uveal melanoma. Cancer Immunol. Immunother. 2019, 68, 1179–1185. [Google Scholar] [CrossRef]
- Pelster, M.S.; Gruschkus, S.K.; Bassett, R.; Gombos, D.S.; Shephard, M.; Posada, L.; Glover, M.S.; Simien, R.; Diab, A.; Hwu, P.; et al. Nivolumab and Ipilimumab in Metastatic Uveal Melanoma: Results from a Single-Arm Phase II Study. J. Clin. Oncol. 2021, 39, 599–607. [Google Scholar] [CrossRef]
- Heppt, M.V.; Amaral, T.; Kähler, K.C.; Heinzerling, L.; Hassel, J.C.; Meissner, M.; Kreuzberg, N.; Loquai, C.; Reinhardt, L.; Utikal, J.; et al. Combined immune checkpoint blockade for metastatic uveal melanoma: A retrospective, multi-center study. J. Immunother. Cancer 2019, 7, 299. [Google Scholar] [CrossRef]
- Piulats, J.M.; Espinosa, E.; de la Cruz Merino, L.; Varela, M.; Carrion, L.A.; Martin-Algarra, S.; Castro, R.L.; Curiel, T.; Abreu, D.R.; Redrado, M.; et al. Nivolumab Plus Ipilimumab for Treatment-Naïve Metastatic Uveal Melanoma: An Open-Label, Multicenter, Phase II Trial by the Spanish Multidisciplinary Melanoma Group (GEM-1402). J. Clin. Oncol. 2021, 39, 586–598. [Google Scholar] [CrossRef]
- Najjar, Y.G.; Navrazhina, K.; Ding, F.; Bhatia, R.; Tsai, K.; Abbate, K.; Durden, B.; Eroglu, Z.; Bhatia, S.; Park, S.; et al. Ipilimumab plus nivolumab for patients with metastatic uveal melanoma: A multicenter, retrospective study. J. Immunother. Cancer 2020, 8, e000331. [Google Scholar] [CrossRef]
- Palmer, S.R.; Erickson, L.A.; Ichetovkin, I.; Knauer, D.J.; Markovic, S.N. Circulating serologic and molecular biomarkers in malignant melanoma. Mayo Clin. Proc. 2011, 86, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Xiong, Y.; Qiao, T.; Li, X.; Jia, L.; Han, Y. Lactate dehydrogenase A: A key player in carcinogenesis and potential target in cancer therapy. Cancer Med. 2018, 7, 6124–6136. [Google Scholar] [CrossRef]
- Xu, J.; Zhao, J.; Wang, J.; Sun, C.; Zhu, X. Prognostic value of lactate dehydrogenase for melanoma patients receiving anti-PD-1/PD-L1 therapy: A meta-analysis. Medicine 2021, 100, e25318. [Google Scholar] [CrossRef] [PubMed]
- Nosrati, A.; Tsai, K.K.; Goldinger, S.M.; Tumeh, P.; Grimes, B.; Loo, K.; Algazi, A.P.; Nguyen-Kim, T.D.L.; Levesque, M.; Dummer, R.; et al. Evaluation of clinicopathological factors in PD-1 response: Derivation and validation of a prediction scale for response to PD-1 monotherapy. Br. J. Cancer 2017, 116, 1141–1147. [Google Scholar] [CrossRef]
- Waninger, J.J.; Ma, V.T.; Journey, S.; Skvarce, J.; Chopra, Z.; Tezel, A.; Bryant, A.K.; Mayo, C.; Sun, Y.; Sankar, K.; et al. Validation of the American Joint Committee on Cancer Eighth Edition Staging of Patients With Metastatic Cutaneous Melanoma Treated With Immune Checkpoint Inhibitors. JAMA Netw. Open 2021, 4, e210980. [Google Scholar] [CrossRef]
- Yu, J.; Green, M.D.; Li, S.; Sun, Y.; Journey, S.N.; Choi, J.E.; Rizvi, S.M.; Qin, A.; Waninger, J.J.; Lang, X.; et al. Liver metastasis restrains immunotherapy efficacy via macrophage-mediated T cell elimination. Nat. Med. 2021, 27, 152–164. [Google Scholar] [CrossRef]
- Poklepovic, A.S.; Carvajal, R.D. Prognostic Value of Low Tumor Burden in Patients with Melanoma. Oncology 2018, 32, e90–e96. [Google Scholar] [PubMed]
- Rodrigues, M.; Mobuchon, L.; Houy, A.; Fiévet, A.; Gardrat, S.; Barnhill, R.L.; Popova, T.; Servois, V.; Rampanou, A.; Mouton, A.; et al. Outlier response to anti-PD1 in uveal melanoma reveals germline MBD4 mutations in hypermutated tumors. Nat. Commun. 2018, 9, 1866. [Google Scholar] [CrossRef] [PubMed]
- Rantala, E.S.; Hernberg, M.M.; Piperno-Neumann, S.; Grossniklaus, H.E.; Kivelä, T.T. Metastatic uveal melanoma: The final frontier. Prog. Retin. Eye Res. 2022, 90, 101041. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, R.D.; Schwartz, G.K.; Tezel, T.; Marr, B.; Francis, J.H.; Nathan, P.D. Metastatic disease from uveal melanoma: Treatment options and future prospects. Br. J. Ophthalmol. 2017, 101, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Mariani, P.; Piperno-Neumann, S.; Servois, V.; Berry, M.; Dorval, T.; Plancher, C.; Couturier, J.; Levy-Gabriel, C.; Rouic, L.L.-L.; Desjardins, L.; et al. Surgical management of liver metastases from uveal melanoma: 16 years’ experience at the Institut Curie. Eur. J. Surg. Oncol. 2009, 35, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Rowcroft, A.; Loveday, B.P.T.; Thomson, B.N.J.; Banting, S.; Knowles, B. Systematic review of liver directed therapy for uveal melanoma hepatic metastases. HPB 2020, 22, 497–505. [Google Scholar] [CrossRef]
- Rietschel, P.; Panageas, K.S.; Hanlon, C.; Patel, A.; Abramson, D.H.; Chapman, P.B. Variates of survival in metastatic uveal melanoma. J. Clin. Oncol. 2005, 23, 8076–8080. [Google Scholar] [CrossRef] [PubMed]
- Grenader, T.; Nash, S.; Adams, R.; Kaplan, R.; Fisher, D.; Maughan, T.; Bridgewater, J. Derived neutrophil lymphocyte ratio is predictive of survival from intermittent therapy in advanced colorectal cancer: A post hoc analysis of the MRC COIN study. Br. J. Cancer 2016, 114, 612–615. [Google Scholar] [CrossRef]
- Capone, M.; Giannarelli, D.; Mallardo, D.; Madonna, G.; Festino, L.; Grimaldi, A.M.; Vanella, V.; Simeone, E.; Paone, M.; Palmieri, G.; et al. Baseline neutrophil-to-lymphocyte ratio (NLR) and derived NLR could predict overall survival in patients with advanced melanoma treated with nivolumab. J. Immunother. Cancer 2018, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, P.F.; Gandini, S.; Battaglia, A.; Alfieri, S.; Di Giacomo, A.M.; Giannarelli, D.; Cappellini, G.C.A.; De Galitiis, F.; Marchetti, P.; Amato, G.; et al. Baseline neutrophil-to-lymphocyte ratio is associated with outcome of ipilimumab-treated metastatic melanoma patients. Br. J. Cancer 2015, 112, 1904–1910. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, E.K.; Flynn, J.R.; Panageas, K.S.; Ferraro, R.A.; Cruz, J.M.S.; Postow, M.A.; Coit, D.G.; Ariyan, C.E. High neutrophil-to-lymphocyte ratio (NLR) is associated with treatment failure and death in patients who have melanoma treated with PD-1 inhibitor monotherapy. Cancer 2020, 126, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Bryant, A.K.; Sankar, K.; Strohbehn, G.W.; Zhao, L.; Elliott, D.; Qin, A.; Yentz, S.; Ramnath, N.; Green, M.D. Prognostic and predictive value of neutrophil-to-lymphocyte ratio with adjuvant immunotherapy in stage III non-small-cell lung cancer. Lung Cancer 2022, 163, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Lalani, A.-K.A.; Xie, W.; Martini, D.J.; Steinharter, J.A.; Norton, C.K.; Krajewski, K.M.; Duquette, A.; Bossé, D.; Bellmunt, J.; Van Allen, E.M.; et al. Change in Neutrophil-to-lymphocyte ratio (NLR) in response to immune checkpoint blockade for metastatic renal cell carcinoma. J. Immunother. Cancer 2018, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.N.; Khoja, L.; Atenafu, E.G.; Hogg, D.; Quirt, I.; Butler, M.; Joshua, A.M. Prognostic factors for first-line therapy and overall survival of metastatic uveal melanoma: The Princess Margaret Cancer Centre experience. Melanoma Res. 2018, 28, 571–577. [Google Scholar] [CrossRef]
- Rantala, E.S.; Hernberg, M.; Kivelä, T.T. Overall survival after treatment for metastatic uveal melanoma: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Warburg, O. On respiratory impairment in cancer cells. Science 1956, 124, 269–270. [Google Scholar] [CrossRef]
- Vander Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-H.; Curtis, J.D.; Maggi, L.B., Jr.; Faubert, B.; Villarino, A.V.; O’Sullivan, D.; Huang, S.C.-C.; van der Windt, G.J.W.; Blagih, J.; Qiu, J.; et al. Posttranscriptional control of T cell effector function by aerobic glycolysis. Cell 2013, 153, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- Husain, Z.; Huang, Y.; Seth, P.; Sukhatme, V.P. Tumor-derived lactate modifies antitumor immune response: Effect on myeloid-derived suppressor cells and NK cells. J. Immunol. 2013, 191, 1486–1495. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed]
- Ny, L.; Jespersen, H.; Karlsson, J.; Alsén, S.; Filges, S.; All-Eriksson, C.; Andersson, B.; Carneiro, A.; Helgadottir, H.; Levin, M.; et al. The PEMDAC phase 2 study of pembrolizumab and entinostat in patients with metastatic uveal melanoma. Nat. Commun. 2021, 12, 5155. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.-P.; Liu, J.-P.; Tao, W.-Q.; Li, H.-M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef] [PubMed]
- Meijer, N.; de Bruyn, D.P.; de Klein, A.; Paridaens, D.; Verdijk, R.M.; Berendschot, T.T.M.; Brosens, E.; Jager, M.J.; Kiliç, E. High C-Reactive Protein Levels Are Related to Better Survival in Patients with Uveal Melanoma. Ophthalmol. Sci. 2022, 2, 100117. [Google Scholar] [CrossRef]
- Bilen, M.A.; Shabto, J.M.; Martini, D.J.; Liu, Y.; Lewis, C.; Collins, H.; Akce, M.; Kissick, H.; Carthon, B.C.; Shaib, W.L.; et al. Sites of metastasis and association with clinical outcome in advanced stage cancer patients treated with immunotherapy. BMC Cancer 2019, 19, 142. [Google Scholar] [CrossRef]
- Koch, E.A.T.; Petzold, A.; Wessely, A.; Dippel, E.; Erdmann, M.; Heinzerling, L.; Hohberger, B.; Knorr, H.; Leiter, U.; Meier, F.; et al. Clinical determinants of long-term survival in metastatic uveal melanoma. Cancer Immunol. Immunother. 2022, 71, 1467–1477. [Google Scholar] [CrossRef]
- Green, M. Hepatic Ablation of Melanoma Metastases to Enhance Immunotherapy Response, a Phase I Clinical Trial (HAMMER I). Available online: https://clinicaltrials.gov/ct2/show/NCT05169957?term=hammer&draw=2&rank=4 (accessed on 6 August 2022).
- Szeligo, B.M.; Ivey, A.D.; Boone, B.A. Poor Response to Checkpoint Immunotherapy in Uveal Melanoma Highlights the Persistent Need for Innovative Regional Therapy Approaches to Manage Liver Metastases. Cancers 2021, 13, 3426. [Google Scholar] [CrossRef]
- Hoefsmit, E.P.; Rozeman, E.A.; Van, T.M.; Dimitriadis, P.; Krijgsman, O.; Conway, J.W.; da Silva, I.P.; van der Wal, J.E.; Ketelaars, S.L.C.; Bresser, K.; et al. Comprehensive analysis of cutaneous and uveal melanoma liver metastases. J. Immunother. Cancer 2020, 8, e001501. [Google Scholar] [CrossRef]
- Klemen, N.D.; Wang, M.; Rubinstein, J.C.; Olino, K.; Clune, J.; Ariyan, S.; Cha, C.; Weiss, S.A.; Kluger, H.M.; Sznol, M. Survival after checkpoint inhibitors for metastatic acral, mucosal and uveal melanoma. J. Immunother. Cancer 2019, 8, e000341. [Google Scholar] [CrossRef] [PubMed]
- Bol, K.F.; Ellebaek, E.; Hoejberg, L.; Bagger, M.M.; Larsen, M.S.; Klausen, T.W.; Køhler, U.H.; Schmidt, H.; Bastholt, L.; Kiilgaard, J.F.; et al. Real-World Impact of Immune Checkpoint Inhibitors in Metastatic Uveal Melanoma. Cancers 2019, 11, 1489. [Google Scholar] [CrossRef] [PubMed]
- Kirchberger, M.C.; Moreira, A.; Erdmann, M.; Schuler, G.; Heinzerling, L. Real world experience in low-dose ipilimumab in combination with PD-1 blockade in advanced melanoma patients. Oncotarget 2018, 9, 28903–28909. [Google Scholar] [CrossRef] [PubMed]
- Field, M.G.; Decatur, C.L.; Kurtenbach, S.; Gezgin, G.; van der Velden, P.A.; Jager, M.J.; Kozak, K.N.; Harbour, J.W. PRAME as an Independent Biomarker for Metastasis in Uveal Melanoma. Clin. Cancer Res. 2016, 22, 1234–1242. [Google Scholar] [CrossRef]
- Saint-Ghislain, M.; Derrien, A.-C.; Geoffrois, L.; Gastaud, L.; Lesimple, T.; Negrier, S.; Penel, N.; Kurtz, J.-E.; Le Corre, Y.; Dutriaux, C.; et al. MBD4 deficiency is predictive of response to immune checkpoint inhibitors in metastatic uveal melanoma patients. Eur. J. Cancer 2022, 173, 105–112. [Google Scholar] [CrossRef]
- Iivanainen, S.; Ahvonen, J.; Knuuttila, A.; Tiainen, S.; Koivunen, J.P. Elevated CRP levels indicate poor progression-free and overall survival on cancer patients treated with PD-1 inhibitors. ESMO Open 2019, 4, e000531. [Google Scholar] [CrossRef]
- Simeone, E.; Gentilcore, G.; Giannarelli, D.; Grimaldi, A.M.; Caracò, C.; Curvietto, M.; Esposito, A.; Paone, M.; Palla, M.; Cavalcanti, E.; et al. Immunological and biological changes during ipilimumab treatment and their potential correlation with clinical response and survival in patients with advanced melanoma. Cancer Immunol. Immunother. 2014, 63, 675–683. [Google Scholar] [CrossRef]
- Riedl, J.M.; Barth, D.A.; Brueckl, W.M.; Zeitler, G.; Foris, V.; Mollnar, S.; Stotz, M.; Rossmann, C.H.; Terbuch, A.; Balic, M.; et al. C-Reactive Protein (CRP) Levels in Immune Checkpoint Inhibitor Response and Progression in Advanced Non-Small Cell Lung Cancer: A Bi-Center Study. Cancers 2020, 12, 2319. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographics | Univariable Analysis | |||||
|---|---|---|---|---|---|---|
| OS | PFS | |||||
| Parameter | Categories | Number (%), n = 46 (100%) | HR (95% CI) | p-Value | HR (95%CI) | p-Value |
| Age (years) | Median (IQR) | 61.8 (20.0) | 1.0 (0.9, 1.0) | 0.33 | 1.0 (1.00, 1.02) | 0.89 |
| Sex | Male | 26 (56.5) | 0.7 (0.4, 1.4) | 0.35 | 0.8 (0.4, 1.5) | 0.46 |
| Female | 20 (43.5) | |||||
| ECOG Performance Status | 0 | 33 (71.7) | 1.9 (0.9, 3.8) | 0.073 | 1.9 (1.0, 3.7) | 0.076 |
| 1 | 11 (23.9) | |||||
| 2 | 1 (2.2) | |||||
| 3 | 1 (2.2) | |||||
| 4 | 0 (0) | |||||
| Sites of Metastasis at Baseline | Liver | 41 (89.1) | 2.0 (0.6. 6.6) | 0.25 | 1.3 (0.5, 3.6) | 0.65 |
| Lung | 21 (47.5) | 1.1 (0.6, 2.1) | 0.8 | 0.9 (0.5, 1.7) | 0.8 | |
| Brain | 3 (6.5) | 1.0 (0.3, 3.5) | 0.95 | 0.7 (0.2, 2.4) | 0.62 | |
| Bone | 11 (23.9) | 1.2 (0.6, 2.5) | 0.6 | 1.3 (0.7, 2.6) | 0.48 | |
| LN | 14 (30.4) | 2.1 (1.1, 4.2) | 0.031 | 1.5 (0.8, 2.8) | 0.24 | |
| Other | 20 (43.5) | 0.6 (0.3, 1.2) | 0.13 | 0.7 (0.4, 1.3) | 0.26 | |
| Liver Only | 14 (30.4) | |||||
| Liver + Extrahepatic. (vs. Liver Only) | 28 (60.9) | 1.4 (0.6, 3.2) | 0.38 | 0.8 (0.4, 1.5) | 0.48 | |
| Extrahepatic Only. (vs. Liver Only) | 4 (8.7) | 0.5 (0.1, 2.3) | 0.36 | 0.7 (0.2, 2.6) | 0.63 | |
| Treatment Characteristics | Univariable Analysis | |||||
|---|---|---|---|---|---|---|
| OS | PFS | |||||
| Parameter | Categories | Number (%), n = 46 (100%) | HR (95% CI) | p-Value | HR (95%CI) | p-Value |
| Enucleation | No | 22 (47.8) | ||||
| Yes | 24 (52.2) | |||||
| Plaque RT | No | 20 (43.5) | ||||
| Yes | 26 (56.5) | |||||
| Lines of Prior Therapy | 0 | 43 (93.5) | 1.3 (0.8, 2.3) | 0.30 | 1.0 (0.6, 1.8) | 0.89 |
| 1 | 2 (4.3) | |||||
| > 1 | 1 (2.2) | |||||
| Immunotherapy | Single ICI | 35 (76.1) | 2.5 (0.9, 6.6) | 0.053 | 2.0 (0.9, 4.1) | 0.076 |
| Combination ICI | 11 (23.9) | 0.4 (0.2, 1.0) | 0.053 | 0.5 (0.2, 1.1) | 0.076 | |
| Cycles of ICI Completed | Median (IQR) | 10 (8) | 0.9 (0.9, 1.0) | 0.009 | 0.9 (0.9, 1.0) | 0.003 |
| Reason for Discontinuation | Progression/Death | 31 (67.4) | ||||
| Toxicity | 11 (23.9) | |||||
| Other | 4 (8.7) | |||||
| IRAE Grade | None | 24 (52.2) | ||||
| Grade 1 | 7 (15.2) | |||||
| Grade 2 | 9 (19.6) | |||||
| Grade 3 | 6 (13.0) | |||||
| Grade 4 | 0 (0) | |||||
| Liver Directed Therapy | None | 23 (50.0) | 0.9 (0.5, 1.8) | 0.8 | 1.0 (0.5, 1.7) | 0.88 |
| Surgical Resection | 2 (4.3) | |||||
| SBRT/RT | 9 (19.6) | |||||
| TACE | 6 (13.0) | |||||
| Radioembolization | 1 (2.2) | |||||
| Multiple | 5 (10.9) | |||||
| Objective Response Rate | CR | 1 (2.2) | ||||
| PR | 1 (2.2) | |||||
| SD | 8 (17.4) | |||||
| PD | 34 (73.9) | |||||
| Unable to Assess | 2 (4.3) | |||||
| Hematologic Biomarkers | Univariable Analysis | |||||
|---|---|---|---|---|---|---|
| OS | PFS | |||||
| Parameter | Categories | Number (%), n = 46 (100%) | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| LDH at Stage IV Diagnosis | Median (IQR) | 209 (83) | ||||
| WNL (< 240 mg/dL) | 29 (63.0) | 2.2 (1.1, 4.3) | 0.038 | 1.6 (0.8, 3.2) | 0.15 | |
| Elevated (> 240 mg/dL) | 14 (30.4) | |||||
| Unknown | 3 (6.5) | |||||
| LDH at Baseline | Median (IQR) | 199 (76) | ||||
| WNL (< 240 mg/dL) | 24 (52.2) | 3.6 (1.9, 7.0) | 0.0011 | 2.8 (1.5, 5.4) | < 0.0001 | |
| Elevated (> 240 mg/dL) | 19 (41.3) | |||||
| Unknown | 3 (6.5) | |||||
| LDH on Treatment | Median (IQR) | 224 (175) | ||||
| WNL (< 240 mg/dL) | 18 (39.1) | 3.7 (1.6, 8.8) | 0.0046 | 2.2 (1.1, 4.3) | 0.0014 | |
| Elevated (> 240 mg/dL) | 16 (34.8) | |||||
| Unknown | 12 (26.1) | |||||
| NLR at Baseline | Median (IQR) | 2.7 (1.5) | ||||
| Below Median | 21 (45.7) | 1.0 (0.5, 2.0) | 0.98 | 1.3 (0.7, 2.5) | 0.18 | |
| ≥ Median | 23 (50.0) | |||||
| Unknown | 2 (4.3) | |||||
| NLR on Treatment | Median (IQR) | 3.2 (1.9) | ||||
| Below Median | 16 (34.8) | 1.6 (0.8, 3.4) | 0.057 | 1.9 (1.0, 3.9) | 0.0098 | |
| ≥ Median | 19 (41.3) | |||||
| Unknown | 11 (23.9) | |||||
| dNLR at Baseline | Median (IQR); n = 45 | 1.7 (0.8) | ||||
| dNLR on Treatment | Median (IQR); n = 36 | 1.8 (1.0) | ||||
| ΔNLR on Treatment | Median (IQR); n = 36 | 0.6 (1.1) | ||||
| ALC at Baseline | Median (IQR), n = 44 | 1.5 (0.8) | ||||
| Below Median | 22 (47.8) | 0.9 (0.5, 1.8) | 0.81 | 0.8 (0.4, 1.4) | 0.38 | |
| ≥ Median | 22 (47.8) | |||||
| Unknown | 2 (4.3) | |||||
| ALC on Treatment | Median (IQR); n = 35 | 1.7 (1.0) | ||||
| Below Median | 17 (37.0) | 0.8 (0.4, 1.7) | 0.52 | 0.7 (0.3, 1.4) | 0.28 | |
| ≥ Median | 18 (39.1) | |||||
| Unknown | 11 (23.9) | |||||
| ANC at Baseline | Median (IQR); n = 44 | 4.1 (1.3) | 0.9 (0.5, 1.7) | 0.73 | 1.2 (0.6, 2.2) | 0.59 |
| Below Median | 21 (45.7) | |||||
| ≥ Median | 23 (50.0) | |||||
| Unknown | 2 (4.3) | |||||
| ANC on Treatment | Median (IQR); n = 35 | 4.9 (3.4) | 0.9 (0.4, 1.8) | 0.70 | 0.9 (0.5, 1.9) | 0.85 |
| Below Median | 17 (37.0) | |||||
| ≥ Median | 18 (39.1) | |||||
| Unknown | 11 (23.9) | |||||
| AEC at Baseline | Median (IQR); n = 44 | 0.1 (0.2) | 0.5 (0.2, 1.2) | 0.11 | 0.7 (0.3, 1.8) | 0.48 |
| Below Median | 5 (10.9) | |||||
| ≥ Median | 39 (84.8) | |||||
| Unknown | 2 (4.3) | |||||
| AEC on Treatment | Median (IQR); n = 35 | 0.2 (0.3) | 1.2 (0.6, 2.6) | 0.61 | 0.8 (0.4, 1.6) | 0.50 |
| Below Median | 18 (39.1) | |||||
| ≥ Median | 17 (37.0) | |||||
| Unknown | 11 (23.9) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waninger, J.J.; Fecher, L.A.; Lao, C.; Yentz, S.; Green, M.D.; Demirci, H. Prognostic Hematologic Biomarkers Following Immune Checkpoint Inhibition in Metastatic Uveal Melanoma. Cancers 2022, 14, 5789. https://doi.org/10.3390/cancers14235789
Waninger JJ, Fecher LA, Lao C, Yentz S, Green MD, Demirci H. Prognostic Hematologic Biomarkers Following Immune Checkpoint Inhibition in Metastatic Uveal Melanoma. Cancers. 2022; 14(23):5789. https://doi.org/10.3390/cancers14235789
Chicago/Turabian StyleWaninger, Jessica J., Leslie A. Fecher, Christopher Lao, Sarah Yentz, Michael D. Green, and Hakan Demirci. 2022. "Prognostic Hematologic Biomarkers Following Immune Checkpoint Inhibition in Metastatic Uveal Melanoma" Cancers 14, no. 23: 5789. https://doi.org/10.3390/cancers14235789
APA StyleWaninger, J. J., Fecher, L. A., Lao, C., Yentz, S., Green, M. D., & Demirci, H. (2022). Prognostic Hematologic Biomarkers Following Immune Checkpoint Inhibition in Metastatic Uveal Melanoma. Cancers, 14(23), 5789. https://doi.org/10.3390/cancers14235789