

Acute Pancreatitis Increases the Risk of Gastrointestinal Cancer in Type 2 Diabetic Patients: A Korean Nationwide Cohort Study

 , , , , ,
, , , , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset
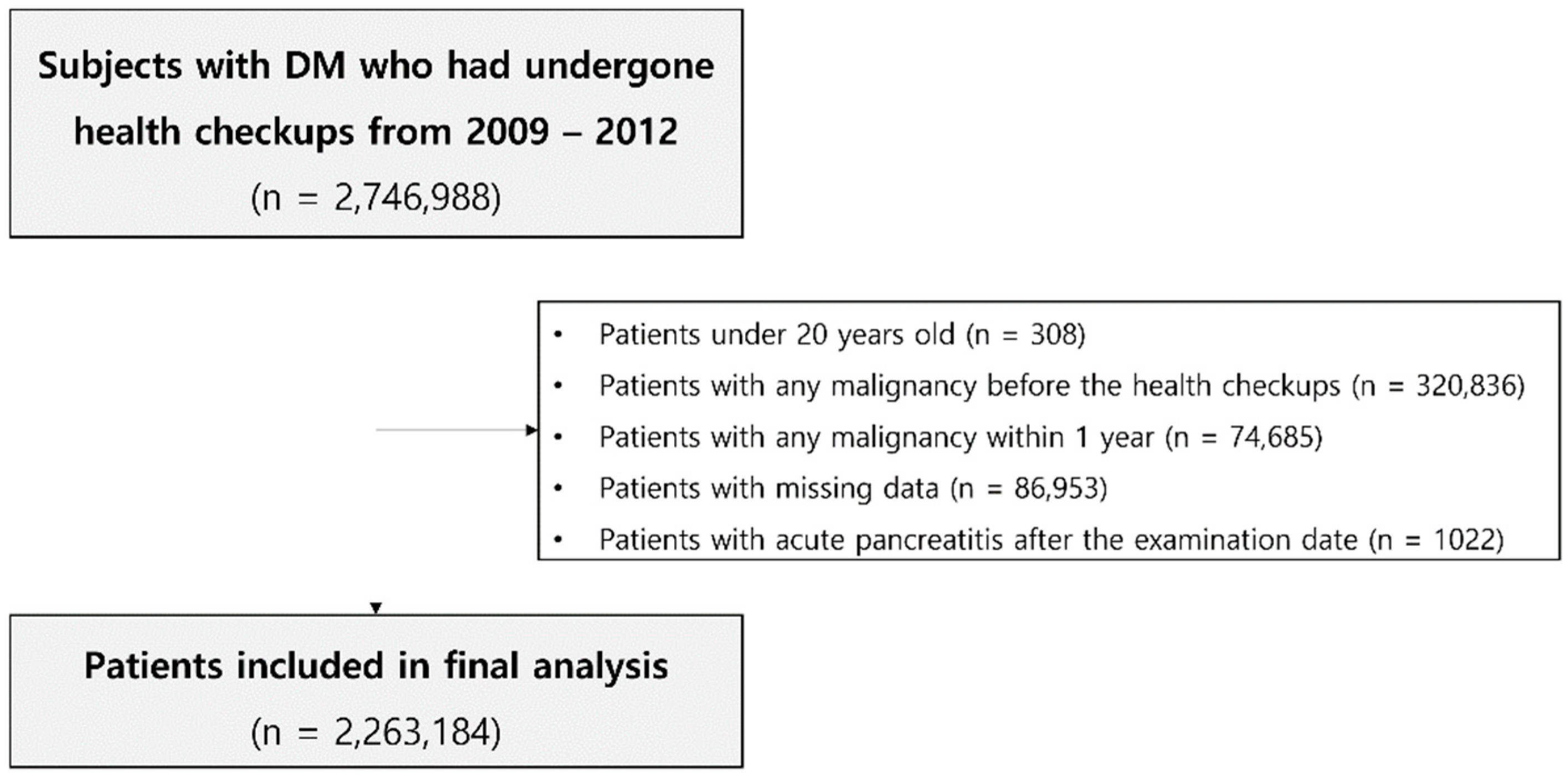
2.2. Study Population and Design
2.3. Predictor, Outcome Variables and Definitions
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Cancer Incidence According to History of AP in Type 2 DM Patients
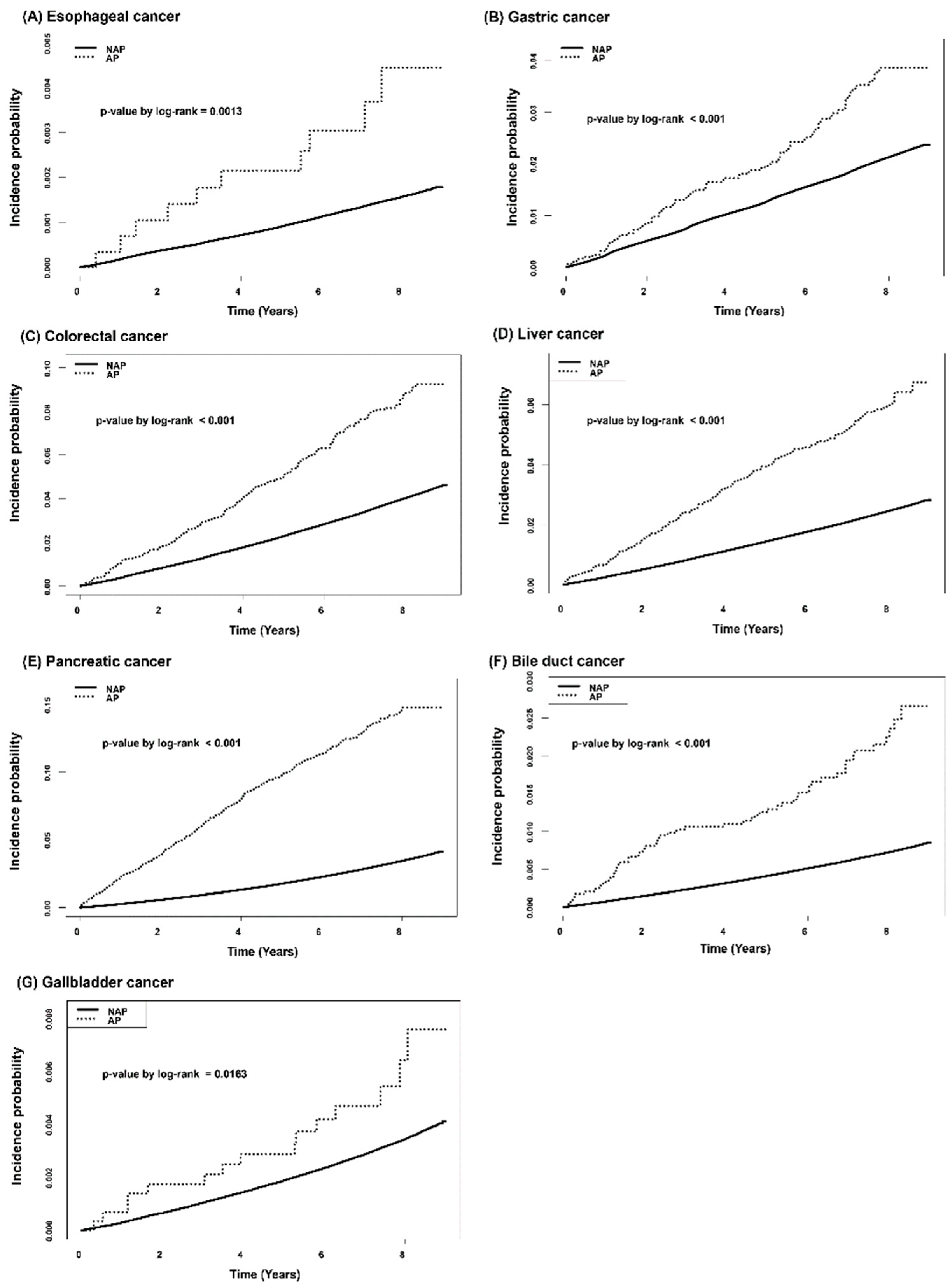
3.3. Cumulative Incidence of Gastrointestinal Cancer According to the History of AP in Type 2 DM Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsilidis, K.K.; Kasimis, J.C.; Lopez, D.S.; Ntzani, E.E.; Ioannidis, J.P. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies. BMJ 2015, 350, g7607. [Google Scholar] [CrossRef] [PubMed]
- Ling, S.; Brown, K.; Miksza, J.K.; Howells, L.; Morrison, A.; Issa, E.; Yates, T.; Khunti, K.; Davies, M.J.; Zaccardi, F. Association of Type 2 Diabetes With Cancer: A Meta-analysis With Bias Analysis for Unmeasured Confounding in 151 Cohorts Comprising 32 Million People. Diabetes Care 2020, 43, 2313–2322. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and cancer: A consensus report. Diabetes Care 2010, 33, 1674–1685. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Pearson-Stuttard, J.; Zhou, B.; Kontis, V.; Bentham, J.; Gunter, M.J.; Ezzati, M. Worldwide burden of cancer attributable to diabetes and high body-mass index: A comparative risk assessment. Lancet Diabetes Endocrinol 2018, 6, 95–104. [Google Scholar] [CrossRef]
- Suh, S.; Kim, K.W. Diabetes and cancer: Cancer should be screened in routine diabetes assessment. Diabetes Metab. J. 2019, 43, 733–743. [Google Scholar] [CrossRef]
- Cao, J.; Yan, W.; Ma, X.; Huang, H.; Yan, H. Insulin-like growth factor 2 mRNA-binding protein 2—A potential link between type 2 diabetes mellitus and cancer. J. Clin. Endocrinol. Metab. 2021, 106, 2807–2818. [Google Scholar] [CrossRef]
- Boxhoorn, L.; Voermans, R.P.; Bouwense, S.A.; Bruno, M.J.; Verdonk, R.C.; Boermeester, M.A.; van Santvoort, H.C.; Besselink, M.G. Acute pancreatitis. Lancet 2020, 396, 726–734. [Google Scholar] [CrossRef]
- Woodmansey, C.; McGovern, A.P.; McCullough, K.A.; Whyte, M.B.; Munro, N.M.; Correa, A.C.; Gatenby, P.A.C.; Jones, S.A.; de Lusignan, S. Incidence, Demographics, and Clinical Characteristics of Diabetes of the Exocrine Pancreas (Type 3c): A Retrospective Cohort Study. Diabetes Care 2017, 40, 1486–1493. [Google Scholar] [CrossRef]
- Kirkegård, J.; Cronin-Fenton, D.; Heide-Jørgensen, U.; Mortensen, F.V. Acute pancreatitis and pancreatic cancer risk: A nationwide matched-cohort study in denmark. Gastroenterology 2018, 154, 1729–1736. [Google Scholar] [CrossRef]
- Sadr-Azodi, O.; Oskarsson, V.; Discacciati, A.; Videhult, P.; Askling, J.; Ekbom, A. Pancreatic cancer following acute pancreatitis: A population-based matched cohort study. Am. J. Gastroenterol. 2018, 113, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The national health insurance service-national sample cohort (nhis-nsc), south korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Song, S.O.; Jung, C.H.; Song, Y.D.; Park, C.Y.; Kwon, H.S.; Cha, B.S.; Park, J.Y.; Lee, K.U.; Ko, K.S.; Lee, B.W. Background and data configuration process of a nationwide population-based study using the korean national health insurance system. Diabetes Metab. J. 2014, 38, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Mederos, M.A.; Reber, H.A.; Girgis, M.D. Acute pancreatitis: A review. JAMA 2021, 325, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Uhlenhopp, D.J.; Then, E.O.; Sunkara, T.; Gaduputi, V. Epidemiology of esophageal cancer: Update in global trends, etiology and risk factors. Clin. J. Gastroenterol. 2020, 13, 1010–1021. [Google Scholar] [CrossRef]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Midha, S.; Chawla, S.; Garg, P.K. Modifiable and non-modifiable risk factors for pancreatic cancer: A review. Cancer Lett. 2016, 381, 269–277. [Google Scholar] [CrossRef]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef]
- Karimi, P.; Islami, F.; Anandasabapathy, S.; Freedman, N.D.; Kamangar, F. Gastric cancer: Descriptive epidemiology, risk factors, screening, and prevention. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 700–713. [Google Scholar] [CrossRef]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Rothwell, J.A.; Jenab, M.; Karimi, M.; Truong, T.; Mahamat-Saleh, Y.; Ferrari, P.; Dashti, S.G.; Kühn, T.; Cross, A.J.; Severi, G.; et al. Metabolic syndrome and risk of gastrointestinal cancers: An investigation using large-scale molecular data. Clin. Gastroenterol. Hepatol. 2021, 20, e1338–e1352. [Google Scholar] [CrossRef]
- Mikolasevic, I.; Milic, S.; Orlic, L.; Poropat, G.; Jakopcic, I.; Franjic, N.; Klanac, A.; Kristo, N.; Stimac, D. Metabolic syndrome and acute pancreatitis. Eur. J. Intern. Med. 2016, 32, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Fujihara, S.; Mori, H.; Kobara, H.; Nishiyama, N.; Kobayashi, M.; Oryu, M.; Masaki, T. Metabolic syndrome, obesity, and gastrointestinal cancer. Gastroenterol. Res. Pract. 2012, 2012, 483623. [Google Scholar] [CrossRef] [PubMed]
- Schisterman, E.F.; Cole, S.R.; Platt, R.W. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology 2009, 20, 488–495. [Google Scholar] [CrossRef]
- Greenland, S. Invited commentary: Variable selection versus shrinkage in the control of multiple confounders. Am. J. Epidemiol. 2008, 167, 523–529. [Google Scholar] [CrossRef]
- Lee, P.J.; Papachristou, G.I. New insights into acute pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 479–496. [Google Scholar] [CrossRef]
- Das, S.L.; Singh, P.P.; Phillips, A.R.; Murphy, R.; Windsor, J.A.; Petrov, M.S. Newly diagnosed diabetes mellitus after acute pancreatitis: A systematic review and meta-analysis. Gut 2014, 63, 818–831. [Google Scholar] [CrossRef]
- Mikó, A.; Farkas, N.; Garami, A.; Szabó, I.; Vincze, Á.; Veres, G.; Bajor, J.; Alizadeh, H.; Rakonczay, Z., Jr.; Vigh, É.; et al. Preexisting diabetes elevates risk of local and systemic complications in acute pancreatitis: Systematic review and meta-analysis. Pancreas 2018, 47, 917–923. [Google Scholar] [CrossRef]
- Hart, P.A.; Bradley, D.; Conwell, D.L.; Dungan, K.; Krishna, S.G.; Wyne, K.; Bellin, M.D.; Yadav, D.; Andersen, D.K.; Serrano, J.; et al. Diabetes following acute pancreatitis. Lancet Gastroenterol. Hepatol. 2021, 6, 668–675. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, S.H.; Huh, G.; Chun, J.W.; You, M.S.; Paik, W.H.; Ryu, J.K.; Kim, Y.T. The association between use of statin or aspirin and pancreatic ductal adenocarcinoma: A nested case-control study in a Korean nationwide cohort. Cancer Med. 2019, 8, 7419–7430. [Google Scholar] [CrossRef] [PubMed]
- Kirkegård, J.; Mortensen, F.V.; Cronin-Fenton, D. chronic pancreatitis and pancreatic cancer risk: A systematic review and meta-analysis. Am. J. Gastroenterol. 2017, 112, 1366–1372. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | AP n (%) | NAP n (%) | p-Value | |
|---|---|---|---|---|
| Total patients | 2930 | 2,260,254 | ||
| Age (years) | Mean ± SD | 55.33 ± 11.97 | 56.08 ± 12.51 | 0.0012 |
| 20–39 years | 215 (7.34) | 212,649 (9.41) | <0.0001 | |
| 40–64 years | 2038 (69.56) | 1,443,511 (63.86) | ||
| ≥65 years | 677 (23.11) | 604,094 (26.73) | ||
| Sex | Male | 2291 (78.19) | 1,356,957 (60.04) | <0.0001 |
| BMI level (kg/m2) | <18.5 | 135 (4.61) | 32,546 (1.44) | <0.0001 |
| 18.5–23 | 1069 (36.48) | 552,683 (24.45) | ||
| 23–25 | 656 (22.39) | 560,987 (24.82) | ||
| 25–30 | 918 (31.33) | 936,682 (41.44) | ||
| 30–35 | 139 (4.74) | 156,792 (6.94) | ||
| ≥35 | 13 (0.44) | 20,564 (0.91) | ||
| Smoking | Never | 1039 (35.46) | 1,244,509 (55.06) | <0.0001 |
| Former | 499 (17.03) | 395,058 (17.48) | ||
| Current | 1392 (47.51) | 620,687 (27.46) | ||
| Alcohol | None | 1433 (48.91) | 1,257,753 (55.65) | <0.0001 |
| Mild | 930 (31.74) | 767,704 (33.97) | ||
| Heavy | 567 (19.35) | 234,797 (10.39) | ||
| Income | Low, 20% | 698 (23.82) | 436,796 (19.32) | <0.0001 |
| Regular Exercise | 594 (20.27) | 460,796 (20.39) | 0.879 | |
| Hypertension | 1602 (54.68) | 1,226,280 (54.25) | 0.647 | |
| Dyslipidemia | 1219 (41.6) | 897,765 (39.72) | 0.0372 | |
| DM severity | DM over 5 years | 840 (28.67) | 646,766 (28.61) | 0.9483 |
| Insulin user | 891 (30.41) | 167,745 (7.42) | <0.0001 | |
| Over two OHA | 1356 (46.28) | 851,265 (37.66) | <0.0001 | |
| Development of chronic pancreatitis during study period | 589 (14.81%) | 2341 (0.11%) | <0.0001 |
| AP (n = 2930) | NAP (n = 2,260,254) | p-Value | ||
|---|---|---|---|---|
| n (%) | n (%) | |||
| Overall | 902 (30.78) | 415,217 (18.37) | <0.0001 | |
| Gastrointestinal cancer | Esophagus | 10 (0.34) | 3222 (0.14) | 0.0044 |
| Stomach | 89 (3.04) | 43,882 (1.94) | <0.0001 | |
| Colon and rectum | 210 (7.17) | 82,274 (3.64) | <0.0001 | |
| Liver | 150 (5.12) | 50,544 (2.24) | <0.0001 | |
| Pancreas | 358 (12.22) | 69,453 (3.07) | <0.0001 | |
| Bile duct | 56 (1.91) | 14,883 (0.66) | <0.0001 | |
| Gallbladder | 15 (0.51) | 7035 (0.31) | 0.0514 | |
| Other cancer | Prostate | 166 (5.67) | 96,315 (4.26) | 0.0002 |
| Lung | 109 (3.72) | 55,480 (2.45) | <0.0001 | |
| Thyroid | 25 (0.85) | 24,398 (1.08) | 0.2363 | |
| Bladder | 23 (0.78) | 20,328 (0.9) | 0.5122 | |
| Corpus | 3 (0.1) | 3118 (0.14) | 0.6042 | |
| Larynx | 12 (0.41) | 2211 (0.1) | <0.0001 | |
| Multiple myeloma | 12 (0.41) | 5869 (0.26) | 0.1112 | |
| Kidney | 7 (0.24) | 10,176 (0.45) | 0.0877 | |
| Lymphoma | 6 (0.20) | 5074 (0.22) | 0.8217 | |
| Leukemia | 3 (0.1) | 3305 (0.15) | 0.5348 | |
| Breast | 8 (0.27) | 10,431 (0.46) | 0.1324 | |
| Ovary | 7 (0.24) | 11,381 (0.5) | 0.0431 | |
| Testicle | 3 (0.1) | 1252 (0.06) | 0.2802 | |
| Oral cavity and pharynx | 2 (0.07) | 1784 (0.08) | 0.8371 | |
| Cervix | 2 (0.07) | 3828 (0.17) | 0.1833 | |
| Nerves | 6 (0.2) | 4470 (0.2) | 0.932 | |
| Skin | 11 (0.38) | 7689 (0.34) | 0.7434 |
| Type | IR * | HR for Gastrointestinal Cancer Development in AP Group | ||||
|---|---|---|---|---|---|---|
| AP | NAP | Crude HR (95% CI) | Adjusted HR (95% CI) ** | Adjusted HR (95% CI) *** | Adjusted HR (95% CI) **** | |
| Esophagus | 0.514 | 0.195 | 2.877 (1.547–5.353) | 2.079 (1.117–3.869) | 1.947 (1.045–3.627) | 1.624 (0.852–3.095) |
| Stomach | 4.638 | 2.677 | 1.978 (1.606–2.435) | 1.770 (1.437–2.179) | 1.712 (1.39–2.108) | 1.637 (1.323–2.025) |
| Colon, Rectum | 11.169 | 5.053 | 2.606 (2.276–2.984) | 2.504 (2.187–2.868) | 2.367 (2.067–2.711) | 2.183 (1.899–2.51) |
| Liver | 7.878 | 3.084 | 3.074 (2.619–3.609) | 2.760 (2.351–3.24) | 2.527 (2.152–2.968) | 2.216 (1.874–2.621) |
| Pancreas | 19.705 | 4.247 | 6.266 (5.647–6.952) | 6.180 (5.569–6.857) | 5.659 (5.099–6.281) | 4.558 (4.078–5.095) |
| Bile duct | 2.900 | 0.901 | 5.135 (3.95–6.676) | 4.783 (3.677–6.222) | 4.606 (3.539–5.994) | 3.996 (3.031–5.269) |
| Gallbladder | 0.771 | 0.425 | 2.466 (1.485–4.093) | 2.469 (1.487–4.10) | 2.415 (1.454–4.012) | 2.445 (1.459–4.099) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, J.H.; Paik, W.H.; Jang, D.K.; Kim, M.K.; Ryu, J.K.; Kim, Y.-T.; Han, K.; Lee, S.H. Acute Pancreatitis Increases the Risk of Gastrointestinal Cancer in Type 2 Diabetic Patients: A Korean Nationwide Cohort Study. Cancers 2022, 14, 5696. https://doi.org/10.3390/cancers14225696
Choi JH, Paik WH, Jang DK, Kim MK, Ryu JK, Kim Y-T, Han K, Lee SH. Acute Pancreatitis Increases the Risk of Gastrointestinal Cancer in Type 2 Diabetic Patients: A Korean Nationwide Cohort Study. Cancers. 2022; 14(22):5696. https://doi.org/10.3390/cancers14225696
Chicago/Turabian StyleChoi, Jin Ho, Woo Hyun Paik, Dong Kee Jang, Min Kyu Kim, Ji Kon Ryu, Yong-Tae Kim, Kyungdo Han, and Sang Hyub Lee. 2022. "Acute Pancreatitis Increases the Risk of Gastrointestinal Cancer in Type 2 Diabetic Patients: A Korean Nationwide Cohort Study" Cancers 14, no. 22: 5696. https://doi.org/10.3390/cancers14225696
APA StyleChoi, J. H., Paik, W. H., Jang, D. K., Kim, M. K., Ryu, J. K., Kim, Y.-T., Han, K., & Lee, S. H. (2022). Acute Pancreatitis Increases the Risk of Gastrointestinal Cancer in Type 2 Diabetic Patients: A Korean Nationwide Cohort Study. Cancers, 14(22), 5696. https://doi.org/10.3390/cancers14225696