
The Risk of Multiple Myeloma Is Reduced in Metformin Initiators: A Retrospective Cohort Study in Taiwanese Patients with Type 2 Diabetes Mellitus


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The Nationwide Database of NHI
2.2. Disease Codes
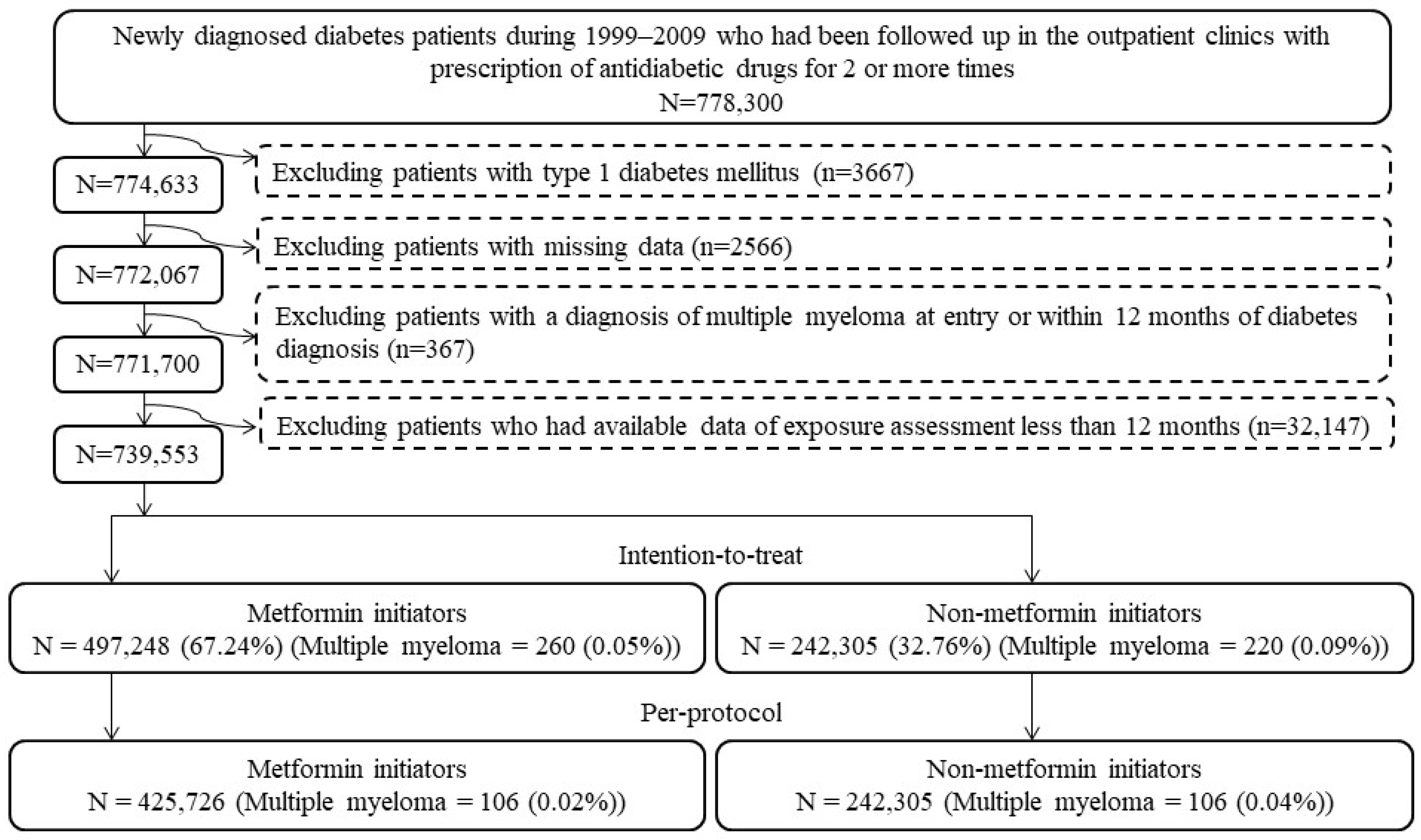
2.3. Enrollment of Study Subjects
2.4. Potential Confounders
2.5. Statistical Analyses
3. Results
4. Discussion
4.1. Main Findings
4.2. Findings in Earlier Studies
4.3. Mechanisms
4.4. Implications
4.5. Strengths
4.6. Limitations
4.7. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kazandjian, D. Multiple myeloma epidemiology and survival: A unique malignancy. Semin. Oncol. 2016, 43, 676–681. [Google Scholar] [CrossRef]
- Rajkumar, S.V. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2022, 97, 1086–1107. [Google Scholar] [CrossRef] [PubMed]
- Cowan, A.J.; Green, D.J.; Kwok, M.; Lee, S.; Coffey, D.G.; Holmberg, L.A.; Tuazon, S.; Gopal, A.K.; Libby, E.N. Diagnosis and management of multiple myeloma: A review. JAMA 2022, 327, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Tentolouris, A.; Ntanasis-Stathopoulos, I.; Eleftheriadou, I.; Malandrakis, P.; Tzeravini, E.; Gavriatopoulou, M. Diabetes mellitus and multiple myeloma; common features of two distinct entities. Diabetes Metab. Res. Rev. 2022, 38, e3535. [Google Scholar] [CrossRef] [PubMed]
- Ragbourne, S.C.; Maghsoodi, N.; Streetly, M.; Crook, M.A. The association between metabolic syndrome and multiple myeloma. Acta Haematol. 2021, 144, 24–33. [Google Scholar] [CrossRef] [PubMed]
- da Cunha Júnior, A.D.; Zanette, D.L.; Pericole, F.V.; Olalla Saad, S.T.; Barreto Campello Carvalheira, J. Obesity as a possible risk factor for progression from monoclonal gammopathy of undetermined significance progression into multiple myeloma: Could myeloma be prevented with metformin treatment? Adv. Hematol. 2021, 2021, 6615684. [Google Scholar] [CrossRef] [PubMed]
- Harbron, R.W.; Pasqual, E. Ionising radiation as a risk factor for lymphoma: A review. J. Radiol. Prot. 2020, 40, R151–R185. [Google Scholar] [CrossRef]
- Tang, C.H.; Liu, H.Y.; Hou, H.A.; Qiu, H.; Huang, K.C.; Siggins, S.; Rothwell, L.A.; Liu, Y. Epidemiology of multiple myeloma in Taiwan, a population based study. Cancer Epidemiol. 2018, 55, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.J.; Mull, N.; Reagan, J.L.; Nemr, S.; Mitri, J. Increased incidence of non-Hodgkin lymphoma, leukemia, and myeloma in patients with diabetes mellitus type 2: A meta-analysis of observational studies. Blood 2012, 119, 4845–4850. [Google Scholar] [CrossRef]
- Zhang, C.; Sha, Y.; Liu, H.; Guo, D.; Jiang, Y.; Hong, L.; Shi, L.; Huang, H. Type 2 diabetes mellitus does not increase the risk of multiple myeloma: A systematic review and meta-analysis. Transl. Cancer Res. 2020, 9, 2884–2894. [Google Scholar] [CrossRef]
- Gong, I.Y.; Cheung, M.C.; Read, S.; Na, Y.; Lega, I.C.; Lipscombe, L.L. Association between diabetes and haematological malignancies: A population-based study. Diabetologia 2021, 64, 540–551. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin significantly reduces incident prostate cancer risk in Taiwanese men with type 2 diabetes mellitus. Eur. J. Cancer 2014, 50, 2831–2837. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and risk of hepatocellular carcinoma in patients with type 2 diabetes. Liver Int. 2018, 38, 2018–2027. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and endometrial cancer risk in Chinese women with type 2 diabetes mellitus in Taiwan. Gynecol. Oncol. 2015, 138, 147–153. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin reduces thyroid cancer risk in Taiwanese patients with type 2 diabetes. PLoS ONE 2014, 9, e109852. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and biliary tract cancer in patients with type 2 diabetes. Front. Oncol. 2020, 10, 587666. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin is associated with a lower risk of non-Hodgkin lymphoma in patients with type 2 diabetes. Diabetes Metab. 2019, 45, 458–464. [Google Scholar] [CrossRef]
- Podhorecka, M. Metformin—Its anti-cancer effects in hematologic malignancies. Oncol. Rev. 2021, 15, 514. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.H.; Luo, S.; O’Brian, K.K.; Thomas, T.S.; Colditz, G.A.; Carlsson, N.P.; Carson, K.R. Association between metformin use and progression of monoclonal gammopathy of undetermined significance to multiple myeloma in US veterans with diabetes mellitus: A population-based retrospective cohort study. Lancet Haematol. 2015, 2, e30–e36. [Google Scholar] [CrossRef]
- Boursi, B.; Weiss, B.M.; Haynes, K.; Mamtani, R.; Yang, Y.X. Reappraisal of risk factors for monoclonal gammopathy of undetermined significance. Am. J. Hematol. 2016, 91, 581–584. [Google Scholar] [CrossRef] [PubMed]
- Boursi, B.; Mamtani, R.; Yang, Y.X.; Weiss, B.M. Impact of metformin on the progression of MGUS to multiple myeloma. Leuk. Lymphoma 2017, 58, 1265–1267. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin is associated with a lower risk of colorectal cancer in Taiwanese patients with type 2 diabetes: A retrospective cohort analysis. Diabetes Metab. 2017, 43, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Chang, L. A Study of Validation on Comorbidity Derived from Claims Data. Master’s Thesis, National Yang-Ming University, Taipei, Taiwan, 2004. Available online: http://etd.lib.nctu.edu.tw/cgi-bin/gs32/ymgsweb.cgi/ccd=ji3XTg/search#result (accessed on 22 February 2020).
- Tseng, C.H. Metformin use and leukemia risk in patients with type 2 diabetes mellitus. Front. Endocrinol. (Lausanne) 2020, 11, 541090. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and primary bone cancer risk in Taiwanese patients with type 2 diabetes mellitus. Bone 2021, 151, 116037. [Google Scholar] [CrossRef]
- Tseng, C.H. Diabetes, insulin use and Helicobacter pylori eradication: A retrospective cohort study. BMC Gastroenterol. 2012, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. The performance of different propensity score methods for estimating marginal hazard ratios. Stat. Med. 2013, 32, 2837–2849. [Google Scholar] [CrossRef]
- Nien, F.J.; Tseng, C.H. A review on the clinical safety of thiazolidinediones. Formos. J. Endocrinol. Metab. 2014, 5 (Suppl. 1), 2–14. [Google Scholar]
- Wang, Y.; Xu, W.; Yan, Z.; Zhao, W.; Mi, J.; Li, J.; Yan, H. Metformin induces autophagy and G0/G1 phase cell cycle arrest in myeloma by targeting the AMPK/mTORC1 and mTORC2 pathways. J. Exp. Clin. Cancer Res. 2018, 37, 63. [Google Scholar] [CrossRef] [PubMed]
- Kocemba-Pilarczyk, K.A.; Trojan, S.; Ostrowska, B.; Lasota, M.; Dudzik, P.; Kusior, D.; Kot, M. Influence of metformin on HIF-1 pathway in multiple myeloma. Pharm. Rep. 2020, 72, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Li, L.; Hu, J.; Li, G.; Zhang, Y.; Dai, X.; De, Z.; Xu, F. Metformin inhibits multiple myeloma serum-induced endothelial cell thrombosis by down-regulating miR-532. Ann. Vasc. Surg. 2022, 85, 347–357.e2. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.K.; Dingli, D. Metformin inhibits IL-6 signaling by decreasing IL-6R expression on multiple myeloma cells. Leukemia 2019, 33, 2695–2709. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Zhou, T.; Doh, H.M.; Trinh, K.R.; Catapang, A.; Lee, J.T.; Braas, D.; Bayley, N.A.; Yamada, R.E.; Vasuthasawat, A.; et al. An HK2 antisense oligonucleotide induces synthetic lethality in HK1-HK2+ multiple myeloma. Cancer Res. 2019, 79, 2748–2760. [Google Scholar] [CrossRef]
- Wu, Z.; Wu, L.; Zou, L.; Wang, M.; Liu, X. Metformin induces myeloma cells necrosis and apoptosis and it is considered for therapeutic use. J. Chemother. 2022, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Abdel Malek, M.A.; Jagannathan, S.; Malek, E.; Sayed, D.M.; Elgammal, S.A.; Abd El-Azeem, H.G.; Thabet, N.M.; Driscoll, J.J. Molecular chaperone GRP78 enhances aggresome delivery to autophagosomes to promote drug resistance in multiple myeloma. Oncotarget 2015, 6, 3098–3110. [Google Scholar] [CrossRef] [PubMed]
- Hanson, D.J.; Nakamura, S.; Amachi, R.; Hiasa, M.; Oda, A.; Tsuji, D.; Itoh, K.; Harada, T.; Horikawa, K.; Teramachi, J.; et al. Effective impairment of myeloma cells and their progenitors by blockade of monocarboxylate transportation. Oncotarget 2015, 6, 33568–33586. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Chen, S.; Xiang, W.; Xiao, M.; Xiao, H. The mechanism of treatment of multiple myeloma with metformin by way of metabolism. Arch. Med. Sci. 2020, 17, 1056–1063. [Google Scholar] [CrossRef] [PubMed]
- Dalva-Aydemir, S.; Bajpai, R.; Martinez, M.; Adekola, K.U.; Kandela, I.; Wei, C.; Singhal, S.; Koblinski, J.E.; Raje, N.S.; Rosen, S.T.; et al. Targeting the metabolic plasticity of multiple myeloma with FDA-approved ritonavir and metformin. Clin. Cancer Res. 2015, 21, 1161–1171. [Google Scholar] [CrossRef]
- Nathwani, N.; Palmer, J.; Synold, T.W.; Salehian, B.; Rosenzweig, M.; Sanchez, J.F.; Hammond, S.N.; Adekola, K.; Tomarchio, V.; Chowdhury, A.; et al. Toxicities associated with metformin/ritonavir combination treatment in relapsed/refractory multiple myeloma. Clin. Lymphoma Myeloma Leuk. 2020, 20, e667–e672. [Google Scholar] [CrossRef] [PubMed]
- Zi, F.M.; He, J.S.; Li, Y.; Wu, C.; Yang, L.; Yang, Y.; Wang, L.J.; He, D.H.; Zhao, Y.; Wu, W.J.; et al. Metformin displays anti-myeloma activity and synergistic effect with dexamethasone in in vitro and in vivo xenograft models. Cancer Lett. 2015, 356, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhao, Y.; Zhang, E.; Yan, H.; Lv, N.; Cai, Z. The synergistic effect of PFK15 with metformin exerts anti-myeloma activity via PFKFB3. Biochem. Biophys. Res. Commun. 2019, 515, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.K.; Wei, C.; Hresko, R.C.; Bajpai, R.; Heitmeier, M.; Matulis, S.M.; Nooka, A.K.; Rosen, S.T.; Hruz, P.W.; Schiltz, G.E.; et al. In silico modeling-based identification of glucose transporter 4 (GLUT4)-selective inhibitors for cancer therapy. J. Biol. Chem. 2015, 290, 14441–14453. [Google Scholar] [CrossRef] [PubMed]
- Gámez, B.; Morris, E.V.; Olechnowicz, S.W.Z.; Webb, S.; Edwards, J.R.; Sowman, A.; Turner, C.J.; Edwards, C.M. The antidiabetic drug metformin acts on the bone microenvironment to promote myeloma cell adhesion to preosteoblasts and increase myeloma tumour burden in vivo. Transl. Oncol. 2022, 15, 101301. [Google Scholar] [CrossRef] [PubMed]
- Schlesser, C.; Meul, T.; Stathopoulos, G.; Meiners, S. Metformin induces resistance of cancer cells to the proteasome inhibitor bortezomib. Biomolecules 2022, 12, 756. [Google Scholar] [CrossRef] [PubMed]
- Maniar, K.; Moideen, A.; Mittal, A.; Patil, A.; Chakrabarti, A.; Banerjee, D. A story of metformin-butyrate synergism to control various pathological conditions as a consequence of gut microbiome modification: Genesis of a wonder drug? Pharmacol. Res. 2017, 117, 103–128. [Google Scholar] [CrossRef]
- Tseng, C.H. The relationship between diabetes mellitus and gastric cancer and the potential benefits of metformin: An extensive review of the literature. Biomolecules 2021, 11, 1022. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin and risk of malignant brain tumors in patients with type 2 diabetes mellitus. Biomolecules 2021, 11, 1226. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin and risk of gingival/periodontal diseases in diabetes patients: A retrospective cohort study. Front. Endocrinol. 2022, 13, 1036885. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin use is associated with a lower risk of inflammatory bowel disease in patients with type 2 diabetes mellitus. J. Crohns Colitis 2021, 15, 64–73. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin use is associated with a reduced risk of acute appendicitis in Taiwanese patients with type 2 diabetes mellitus. Sci. Rep. 2021, 11, 12400. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin reduces the risk of diverticula of intestine in Taiwanese patients with type 2 diabetes mellitus. Front. Pharmacol. 2021, 12, 739141. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin decreases risk of tuberculosis infection in type 2 diabetes patients. J. Clin. Med. 2018, 7, 264. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and Helicobacter pylori infection in patients with type 2 diabetes. Diabetes Care 2018, 41, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. The effect of metformin on male reproductive function and prostate: An updated review. World J. Mens Health 2022, 40, 11–29. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin’s effects on varicocele, erectile dysfunction, infertility and prostate-related diseases: A retrospective cohort study. Front. Pharmacol. 2022, 13, 799290. [Google Scholar] [CrossRef] [PubMed]
- Kistler, K.D.; Rajangam, K.; Faich, G.; Lanes, S. Cardiac event rates in patients with newly diagnosed and relapsed multiple myeloma in US clinical practice. Blood 2012, 120, 2916. [Google Scholar] [CrossRef]
- Efentakis, P.; Psarakou, G.; Varela, A.; Papanagnou, E.D.; Chatzistefanou, M.; Nikolaou, P.E.; Davos, C.H.; Gavriatopoulou, M.; Trougakos, I.P.; Dimopoulos, M.A.; et al. Elucidating carfilzomib’s induced cardiotoxicity in an in vivo model of aging: Prophylactic potential of metformin. Int. J. Mol. Sci. 2021, 22, 10956. [Google Scholar] [CrossRef] [PubMed]
- Proskuriakova, E.; Jada, K.; Kakieu Djossi, S.; Khedr, A.; Neupane, B.; Mostafa, J.A. Mechanisms and potential treatment options of heart failure in patients with multiple myeloma. Cureus 2021, 13, e15943. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and risk of hypertension in Taiwanese patients with type 2 diabetes mellitus. J. Am. Heart Assoc. 2018, 7, e008860. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin use is associated with a lower incidence of hospitalization for atrial fibrillation in patients with type 2 diabetes mellitus. Front. Med. 2021, 7, 592901. [Google Scholar] [CrossRef]
- Tseng, C.H. Metformin use is associated with a lower risk of hospitalization for heart failure in patients with type 2 diabetes mellitus: A retrospective cohort analysis. J. Am. Heart Assoc. 2019, 8, e011640. [Google Scholar] [CrossRef]
- Tseng, C.H. Body mass index and blood pressure in adult type 2 diabetic patients in Taiwan. Circ. J. 2007, 71, 1749–1754. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Liu, B. Statin use and the risk of multiple myeloma: A PRISMA-compliant meta-analysis. Ann. Hematol. 2020, 99, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Grabarek, B.O.; Boroń, D.; Morawiec, E.; Michalski, P.; Palazzo-Michalska, V.; Pach, Ł.; Dziuk, B.; Świder, M.; Zmarzły, N. Crosstalk between statins and cancer prevention and therapy: An update. Pharmaceuticals 2021, 14, 1220. [Google Scholar] [CrossRef] [PubMed]
- Marinac, C.R.; Lee, D.H.; Colditz, G.A.; Rebbeck, T.R.; Rosner, B.; Bustoros, M.; Ghobrial, I.M.; Birmann, B.M. Regular aspirin use and mortality in patients with multiple myeloma. Cancer Epidemiol. Biomark. Prev. 2022, 31, 479–485. [Google Scholar] [CrossRef]
- Liu, H.; Xiong, C.; Liu, J.; Sun, T.; Ren, Z.; Li, Y.; Geng, J.; Li, X. Aspirin exerts anti-tumor effect through inhibiting Blimp1 and activating ATF4/CHOP pathway in multiple myeloma. Biomed. Pharmacother. 2020, 125, 110005. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Metformin (−) | Metformin (+) | Standardized Difference | ||
|---|---|---|---|---|---|
| (n = 242,305) | (n = 497,248) | ||||
| n | % | n | % | ||
| Basic data | |||||
| Age * (years) | 58.53 | 13.24 | 55.85 | 13.27 | −7.97 |
| Sex (men) | 130,885 | 54.02 | 268,493 | 54.00 | 0.23 |
| Time without antidiabetic drugs after diabetes diagnosis * (years) | 1.69 | 1.49 | 1.90 | 1.63 | 16.81 |
| Occupation | |||||
| I | 90,856 | 37.50 | 201,375 | 40.50 | |
| II | 47,896 | 19.77 | 201,375 | 40.50 | 5.00 |
| III | 58,895 | 24.31 | 98,440 | 19.80 | −10.60 |
| IV | 44,658 | 18.43 | 91,520 | 18.41 | −1.77 |
| Living region | |||||
| Taipei | 75,424 | 31.13 | 172,251 | 34.64 | |
| Northern | 27,863 | 11.50 | 64,724 | 13.02 | 5.31 |
| Central | 43,151 | 17.81 | 88,404 | 17.78 | −1.40 |
| Southern | 43,090 | 17.78 | 76,419 | 15.37 | −6.31 |
| Kao-Ping and Eastern | 52,777 | 21.78 | 95,450 | 19.20 | −7.32 |
| Major comorbidities | |||||
| Hypertension | 151,453 | 62.51 | 311,678 | 62.68 | 3.41 |
| Dyslipidemia | 112,992 | 46.63 | 280,842 | 56.48 | 22.43 |
| Obesity | 4554 | 1.88 | 21,773 | 4.38 | 13.84 |
| Diabetes-related complications | |||||
| Nephropathy | 38,439 | 15.86 | 68,263 | 13.73 | −4.86 |
| Eye diseases | 10,265 | 4.24 | 35,298 | 7.10 | 12.61 |
| Stroke | 47,950 | 19.79 | 89,808 | 18.06 | −2.98 |
| Ischemic heart disease | 76,125 | 31.42 | 149,648 | 30.10 | −0.97 |
| Peripheral arterial disease | 28,382 | 11.71 | 28,382 | 5.71 | 2.41 |
| Hypoglycemia | 32,891 | 13.57 | 4075 | 0.82 | −0.60 |
| Medications that are commonly used by diabetes patients | |||||
| Angiotensin-converting enzyme inhibitor/angiotensin receptor blocker | 117,006 | 48.29 | 244,835 | 49.24 | 4.23 |
| Calcium channel blocker | 117,036 | 48.30 | 221,799 | 44.61 | −5.48 |
| Statin | 62,806 | 25.92 | 164,644 | 33.11 | 17.33 |
| Fibrate | 53,605 | 22.12 | 120,126 | 24.16 | 6.27 |
| Aspirin | 94,028 | 38.81 | 198,040 | 39.83 | 4.14 |
| Comorbidities that might affect exposure or outcome | |||||
| Chronic obstructive pulmonary disease | 87,069 | 35.93 | 181,570 | 36.51 | 2.88 |
| Tobacco abuse | 2515 | 1.04 | 8632 | 1.74 | 6.19 |
| Alcohol-related diagnoses | 10,955 | 4.52 | 23,674 | 4.76 | 1.85 |
| Heart failure | 30,372 | 12.53 | 30,372 | 6.11 | −4.77 |
| Parkinson’s disease | 4903 | 2.02 | 8158 | 1.64 | −2.57 |
| Dementia | 12,636 | 5.21 | 21,669 | 4.36 | −3.62 |
| Head injury | 1795 | 0.74 | 5291 | 1.06 | 3.72 |
| Valvular heart disease | 17,158 | 7.08 | 32,891 | 6.61 | −1.36 |
| Helicobacter pylori infection | 895 | 0.37 | 895 | 0.18 | 3.08 |
| Epstein–Barr virus infection | 1239 | 0.51 | 2687 | 0.54 | 0.66 |
| Hepatitis B virus infection | 2758 | 1.14 | 8533 | 1.72 | 5.19 |
| Hepatitis C virus infection | 6971 | 2.88 | 14,303 | 2.88 | 0.57 |
| Human immunodeficiency virus disease | 126 | 0.05 | 262 | 0.05 | 0.14 |
| Cirrhosis of liver without mention of alcohol | 9737 | 4.02 | 15,689 | 3.16 | −4.18 |
| Other chronic nonalcoholic liver disease | 15,042 | 6.21 | 37,844 | 7.61 | 6.18 |
| Autoimmune diseases | 14,130 | 5.83 | 31,922 | 6.42 | 3.25 |
| Organ transplantation | 643 | 0.27 | 776 | 0.16 | −2.17 |
| Insomnia | 41,568 | 17.16 | 95,610 | 19.23 | 6.92 |
| Malaise and fatigue | 6584 | 2.72 | 19,867 | 4.00 | 7.75 |
| History of some disorders of the central nervous system | 40,853 | 16.86 | 87,193 | 17.54 | 2.84 |
| Immunosuppression | 9893 | 4.08 | 16,989 | 3.42 | −3.00 |
| Benign neoplasm of bone and articular cartilage | 671 | 0.28 | 1689 | 0.34 | 1.21 |
| Bone fractures | 37,975 | 15.67 | 83,546 | 16.80 | 3.99 |
| Ocular pterygium | 7482 | 3.09 | 15,316 | 3.08 | 0.65 |
| Disorders of the thyroid gland | 16,356 | 6.75 | 44,442 | 8.94 | 8.82 |
| Nutritional deficiencies | 5725 | 2.36 | 10,176 | 2.05 | −1.93 |
| Depression | 12,424 | 5.13 | 29,444 | 5.92 | 4.10 |
| Cancer | 22,305 | 9.21 | 43,716 | 8.79 | −0.78 |
| Metformin Initiation | Incident Case Number | Cases Followed | Person-Year | Incidence Rate (per 100,000 Person-Years) | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|---|---|
| Intention-to-treat | |||||||
| Metformin (−) | 220 | 242,305 | 1,534,914.14 | 14.33 | 1.000 | ||
| Metformin (+) | 260 | 497,248 | 2,608,969.26 | 9.97 | 0.710 | (0.593–0.850) | 0.0002 |
| Per-protocol | |||||||
| Metformin (−) | 106 | 242,305 | 758,110.62 | 13.98 | 1.000 | ||
| Metformin (+) | 106 | 425,726 | 2,064,133.42 | 5.14 | 0.355 | (0.270–0.466) | <0.0001 |
| Subgroup | Incident Case Number | Cases Followed | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|
| (1) Men | |||||
| Intention-to-treat | |||||
| Metformin (−) | 114 | 130,885 | 1.000 | ||
| Metformin (+) | 146 | 268,493 | 0.762 | (0.596–0.975) | 0.0306 |
| Per-protocol | |||||
| Metformin (−) | 53 | 130,885 | 1.000 | ||
| Metformin (+) | 62 | 229,825 | 0.425 | (0.294–0.616) | <0.0001 |
| (2) Women | |||||
| Intention-to-treat | |||||
| Metformin (−) | 106 | 111,420 | 1.000 | ||
| Metformin (+) | 114 | 228,755 | 0.653 | (0.501–0.851) | 0.0016 |
| Per-protocol | |||||
| Metformin (−) | 53 | 111,420 | 1.000 | ||
| Metformin (+) | 44 | 195,901 | 0.286 | (0.191–0.429) | <0.0001 |
| (3) Age≥ 60 years | |||||
| Intention-to-treat | |||||
| Metformin (−) | 160 | 109,977 | 1.000 | ||
| Metformin (+) | 181 | 184,338 | 0.810 | (0.655–1.003) | 0.0533 |
| Per-protocol | |||||
| Metformin (−) | 80 | 109,977 | 1.000 | ||
| Metformin (+) | 69 | 151,698 | 0.429 | (0.310–0.594) | <0.0001 |
| (4) Age < 60 years | |||||
| Intention-to-treat | |||||
| Metformin (−) | 60 | 132,328 | 1.000 | ||
| Metformin (+) | 79 | 312,910 | 0.715 | (0.510–1.002) | 0.0512 |
| Per-protocol | |||||
| Metformin (−) | 26 | 132,328 | 1.000 | ||
| Metformin (+) | 37 | 274,028 | 0.403 | (0.242–0.671) | 0.0005 |
| Models | Incident Case Number | Cases Followed | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|
| 1. Excluding two consecutive prescriptions of metformin spanning more than 6 months | |||||
| Intention-to-treat | |||||
| Metformin (−) | 220 | 242,305 | 1.000 | ||
| Metformin (+) | 115 | 246,249 | 0.795 | (0.633–1.000) | 0.0500 |
| Per-protocol | |||||
| Metformin (−) | 106 | 242,305 | 1.000 | ||
| Metformin (+) | 27 | 177,989 | 0.285 | (0.187–0.435) | <0.0001 |
| 2. Excluding patients who happened to be treated with incretin-based therapies during follow-up | |||||
| Intention-to-treat | |||||
| Metformin (−) | 211 | 210,110 | 1.000 | ||
| Metformin (+) | 245 | 416,396 | 0.726 | (0.604–0.87) | 0.0007 |
| Per-protocol | |||||
| Metformin (−) | 106 | 210,110 | 1.000 | ||
| Metformin (+) | 98 | 347,493 | 0.384 | (0.291–0.507) | <0.0001 |
| 3. Excluding patients who had ever been treated with thiazolidinediones | |||||
| Intention-to-treat | |||||
| Metformin (−) | 186 | 183,856 | 1.000 | ||
| Metformin (+) | 217 | 364,689 | 0.745 | (0.612–0.907) | 0.0034 |
| Per-protocol | |||||
| Metformin (−) | 102 | 183,856 | 1.000 | ||
| Metformin (+) | 86 | 298,735 | 0.401 | (0.301–0.534) | <0.0001 |
| 4. Excluding patients with a diagnosis of any cancer other than multiple myeloma during follow-up | |||||
| Intention-to-treat | |||||
| Metformin (−) | 220 | 194,986 | 1.000 | ||
| Metformin (+) | 260 | 415,629 | 0.692 | (0.578–0.829) | <0.0001 |
| Per-protocol | |||||
| Metformin (−) | 106 | 194,986 | 1.000 | ||
| Metformin (+) | 106 | 358,038 | 0.338 | (0.258–0.444) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, C.-H. The Risk of Multiple Myeloma Is Reduced in Metformin Initiators: A Retrospective Cohort Study in Taiwanese Patients with Type 2 Diabetes Mellitus. Cancers 2022, 14, 5637. https://doi.org/10.3390/cancers14225637
Tseng C-H. The Risk of Multiple Myeloma Is Reduced in Metformin Initiators: A Retrospective Cohort Study in Taiwanese Patients with Type 2 Diabetes Mellitus. Cancers. 2022; 14(22):5637. https://doi.org/10.3390/cancers14225637
Chicago/Turabian StyleTseng, Chin-Hsiao. 2022. "The Risk of Multiple Myeloma Is Reduced in Metformin Initiators: A Retrospective Cohort Study in Taiwanese Patients with Type 2 Diabetes Mellitus" Cancers 14, no. 22: 5637. https://doi.org/10.3390/cancers14225637
APA StyleTseng, C.-H. (2022). The Risk of Multiple Myeloma Is Reduced in Metformin Initiators: A Retrospective Cohort Study in Taiwanese Patients with Type 2 Diabetes Mellitus. Cancers, 14(22), 5637. https://doi.org/10.3390/cancers14225637