


Correlation between PD-L1 Expression of Non-Small Cell Lung Cancer and Data from IVIM-DWI Acquired during Magnetic Resonance of the Thorax: Preliminary Results

 ,
,  , ,
, ,  , , , ,
, , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patients’ Clinical Data
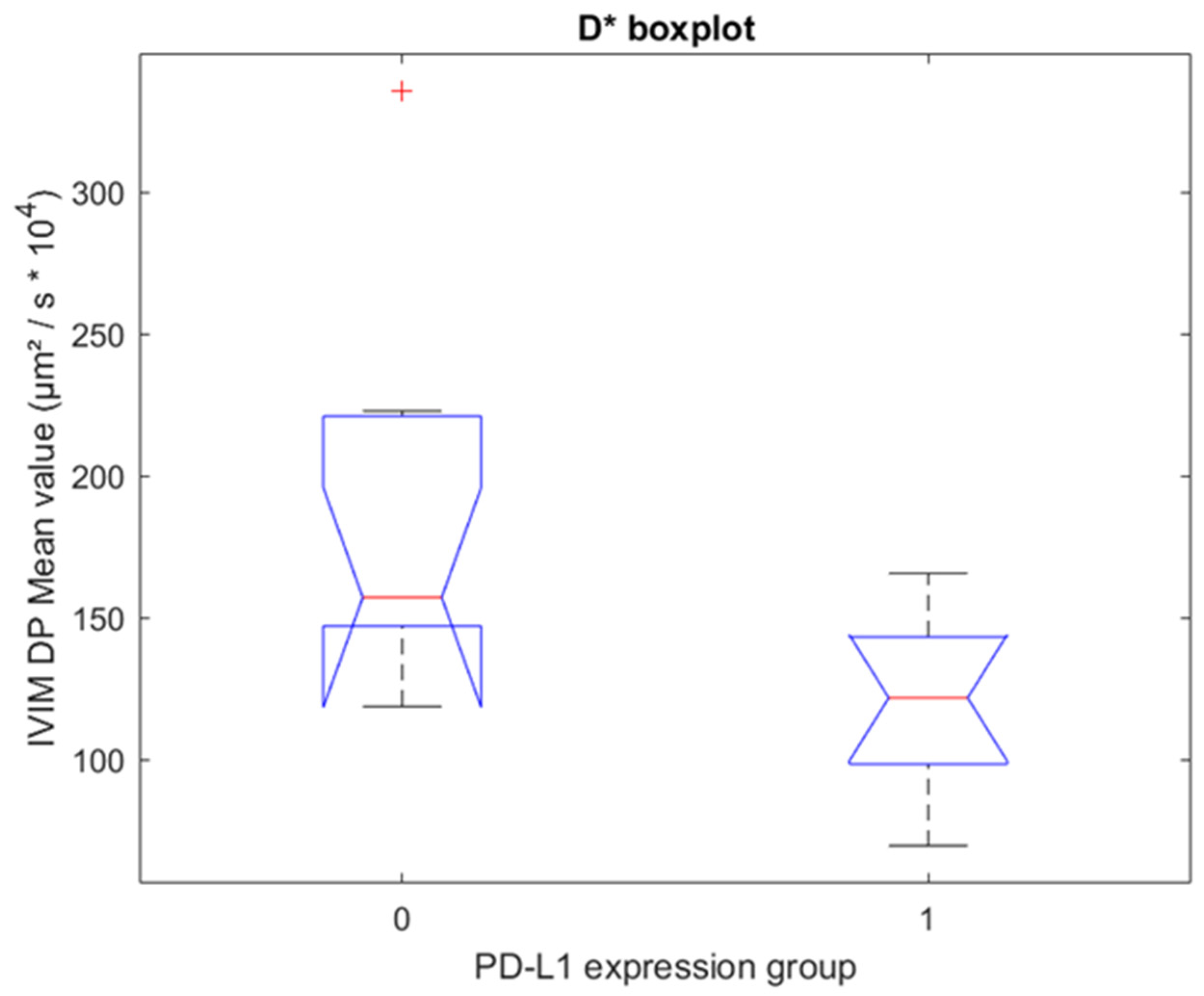
3.2. Correlation of ADC, D, D*, and pf Values with PD-L1 Expression in NSCLC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Ab-del-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef]
- Nicholson, A.G.; Scagliotti, G.; Tsao, M.S.; Yatabe, Y.; Travis, W.D. 2021 WHO Classification of Lung Cancer: A Globally Applicable and Molecular Biomarker-Relevant Classification. J. Thorac. Oncol. 2022, 17, e80–e83. [Google Scholar] [CrossRef] [PubMed]
- de Castro, G.; Kudaba, I.; Wu, Y.-L.; Lopes, G.; Kowalski, D.M.; Turna, H.Z.; Caglevic, C.; Zhang, L.; Karaszewska, B.; Laktionov, K.K.; et al. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy as First-Line Therapy in Patients With Non-Small-Cell Lung Cancer and Programmed Death Ligand-1 Tumor Proportion Score ≥ 1% in the KEYNOTE-042 Study. J. Clin. Oncol. 2022, JCO2102885. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Gadgeel, S.M.; Speranza, G.; Felip, E.; Esteban Gonzalez, E.; Domine Gomez, M.; Hochmair, M.J.; Powell, S.F.; Bischoff, H.; Peled, N.; et al. 973MO KEYNOTE-189 5-year update: First-line pembrolizumab (pembro) + pemetrexed (pem) and platinum vs placebo (pbo) + pem and platinum for metastatic nonsquamous NSCLC. Ann. Oncol. 2022, 33, S992–S993. [Google Scholar] [CrossRef]
- Novello, S.; Kowalski, D.M.; Luft, A.; Gumus, M.; Baz, D.V.; Mazieres, J.; Cid, J.R.; Tafreshi, A.; Cheng, Y.; Lee, K.H.; et al. 5-year update from KEYNOTE-407: Pembrolizumab plus chemotherapy in squamous non-small cell lung cancer (NSCLC). Ann. Oncol. 2022, 33 (Suppl. 7), S448–S554. [Google Scholar] [CrossRef]
- Chen, M.-L.; Shi, A.-H.; Li, X.-T.; Wei, Y.-Y.; Qi, L.-P.; Sun, Y.-S. Is there any correlation between spectral CT imaging parameters and PD-L1 expression of lung adenocarcinoma? Thorac. Cancer 2020, 11, 362–368. [Google Scholar] [CrossRef]
- Kaira, K.; Kuji, I.; Kagamu, H. Value of 18F-FDG-PET to predict PD-L1 expression and outcomes of PD-1 inhibition therapy in human cancers. Cancer Imaging 2021, 21, 11. [Google Scholar] [CrossRef]
- Meier-Schroers, M.; Homsi, R.; Schild, H.H.; Thomas, D. Lung cancer screening with MRI: Characterization of nodules with different non-enhanced MRI sequences. Acta Radiol. 2019, 60, 168–176. [Google Scholar] [CrossRef]
- Koyama, H.; Ohno, Y.; Seki, S.; Nishio, M.; Yoshikawa, T.; Matsumoto, S.; Maniwa, Y.; Itoh, T.; Nishimura, Y.; Sugimura, K. Value of diffusion-weighted MR imaging using various parameters for assessment and characterization of solitary pulmonary nodules. Eur. J. Radiol. 2015, 84, 509–515. [Google Scholar] [CrossRef]
- Koyama, H.; Ohno, Y.; Seki, S.; Nishio, M.; Yoshikawa, T.; Matsumoto, S.; Sugimura, K. Magnetic resonance imaging for lung cancer. J. Thorac. Imaging 2013, 28, 138–150. [Google Scholar] [CrossRef]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Grenier, P.; Cabanis, E.; Laval-Jeantet, M. MR imaging of intravoxel incoherent motions: Application to diffusion and perfusion in neurologic disorders. Radiology 1986, 161, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Yue, Y.; Jin, Y.; Guo, J.; Zuo, L.; Peng, H.; Chan, Q. Intravoxel incoherent motion and ADC measurements for differentiating benign from malignant thyroid nodules: Utilizing the most repeatable region of interest delineation at 3.0 T. Cancer Imaging 2020, 20, 9. [Google Scholar] [CrossRef] [PubMed]
- ter Voert, E.E.G.W.; Delso, G.; Porto, M.; Huellner, M.; Veit-Haibach, P. Intravoxel incoherent motion protocol evaluation and data quality in normal and malignant liver tissue and comparison to the literature. Invest. Radiol. 2016, 51, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Cho, G.Y.; Moy, L.; Kim, S.G.; Baete, S.H.; Moccaldi, M.; Babb, J.S.; Sodickson, D.K.; Sigmund, E.E. Evaluation of breast cancer using intravoxel incoherent motion (IVIM) histogram analysis: Comparison with malignant status, histological subtype, and molecular prognostic factors. Eur. Radiol. 2016, 26, 2547–2558. [Google Scholar] [CrossRef] [PubMed]
- Pu, J.; Liang, Y.; He, Q.; Shao, J.-W.; Zhou, M.-J.; Xiang, S.-T.; Li, Y.-W.; Li, J.-B.; Ji, S.-J. Correlation Between IVIM-DWI Parameters and Pathological Classification of Idiopathic Orbital Inflammatory Pseudotumors: A Preliminary Study. Front. Oncol. 2022, 12, 809430. [Google Scholar] [CrossRef] [PubMed]
- Fornasa, F. Diffusion-weighted Magnetic Resonance Imaging: What Makes Water Run Fast or Slow? J. Clin. Imaging Sci. 2011, 1, 27. [Google Scholar] [CrossRef]
- Meyer, H.-J.; Höhn, A.K.; Surov, A. Relationships between apparent diffusion coefficient (ADC) histogram analysis parameters and PD-L 1-expression in head and neck squamous cell carcinomas: A preliminary study. Radiol. Oncol. 2021, 55, 150–157. [Google Scholar] [CrossRef]
- Yin, Y.; Sedlaczek, O.; Muller, B.; Warth, A.; Gonzalez-Vallinas, M.; Lahrmann, B.; Grabe, N.; Kauczor, H.-U.; Breuhahn, K.; Vignon-Clementel, I.E.; et al. Tumor Cell Load and Heterogeneity Estimation From Diffusion-Weighted MRI Calibrated With Histological Data: An Example From Lung Cancer. IEEE Trans. Med. Imaging 2018, 37, 35–46. [Google Scholar] [CrossRef]
- Liang, J.; Li, J.; Li, Z.; Meng, T.; Chen, J.; Ma, W.; Chen, S.; Li, X.; Wu, Y.; He, N. Differentiating the lung lesions using Intravoxel incoherent motion diffusion-weighted imaging: A meta-analysis. BMC Cancer 2020, 20, 799. [Google Scholar] [CrossRef]
- Iima, M. Perfusion-driven Intravoxel Incoherent Motion (IVIM) MRI in Oncology: Applications, Challenges, and Future Trends. Magn. Reson. Med. Sci. 2021, 20, 125–138. [Google Scholar] [CrossRef]
- Lopez de Rodas, M.; Nagineni, V.; Ravi, A.; Datar, I.J.; Mino-Kenudson, M.; Corredor, G.; Barrera, C.; Behlman, L.; Rimm, D.L.; Herbst, R.S.; et al. Role of tumor infiltrating lymphocytes and spatial immune heterogeneity in sensitivity to PD-1 axis blockers in non-small cell lung cancer. J. Immunother. Cancer 2022, 10, e004440. [Google Scholar] [CrossRef] [PubMed]
- Zeng, S.; Liang, L.; Zhang, Q.; Xu, Y.; Tang, H.; Zhang, Z.; Zhang, X.; Jiang, T.; Hu, X. Using functional magnetic resonance imaging to evaluate an acute allograft rejection model in rats. Magn. Reson. Imaging 2019, 58, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, T.; Hébert, M.; Bilodeau, L.; Sebastiani, G.; Cerny, M.; Olivié, D.; Gao, Z.-H.; Sylvestre, M.-P.; Cloutier, G.; Nguyen, B.N.; et al. Intravoxel incoherent motion diffusion-weighted MRI for the characterization of inflammation in chronic liver disease. Eur. Radiol. 2021, 31, 1347–1358. [Google Scholar] [CrossRef]
- Lizotte, P.H.; Ivanova, E.V.; Awad, M.M.; Jones, R.E.; Keogh, L.; Liu, H.; Dries, R.; Almonte, C.; Herter-Sprie, G.S.; Santos, A.; et al. Multiparametric profiling of non-small-cell lung cancers reveals distinct immunophenotypes. JCI Insight 2016, 1, e89014. [Google Scholar] [CrossRef]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab Versus Docetaxel in Previously Treated Patients With Advanced Non-Small-Cell Lung Cancer: Two-Year Outcomes From Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; et al. Five-Year Survival Outcomes From the PACIFIC Trial: Durvalumab After Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Horiuchi, S.; Morooka, H.; Ibi, T.; Takahashi, N.; Ikeya, T.; Shimizu, Y.; Hoshi, E. Inter-tumor heterogeneity of PD-L1 expression in non-small cell lung cancer. J. Thorac. Dis. 2019, 11, 4982–4991. [Google Scholar] [CrossRef]
- Stella, G.M.; Bortolotto, C.; Filippi, A.R. Intrathoracic core needle biopsy and repeat biopsy for PD-L1 evaluation in non-small cell lung cancer. J. Thorac. Dis. 2018, 10, S4031–S4033. [Google Scholar] [CrossRef]
- Casale, S.; Bortolotto, C.; Stella, G.M.; Filippi, A.R.; Gitto, S.; Bottinelli, O.M.; Carnevale, S.; Morbini, P.; Preda, L. Recent advancement on PD-L1 expression quantification: The radiologist perspective on CT-guided FNAC. Diagn. Interv. Radiol. 2021, 27, 214–218. [Google Scholar] [CrossRef]
- Heymann, J.J.; Bulman, W.A.; Swinarski, D.; Pagan, C.A.; Crapanzano, J.P.; Haghighi, M.; Fazlollahi, L.; Stoopler, M.B.; Sonett, J.R.; Sacher, A.G.; et al. PD-L1 expression in non-small cell lung carcinoma: Comparison among cytology, small biopsy, and surgical resection specimens. Cancer Cytopathol. 2017, 125, 896–907. [Google Scholar] [CrossRef]
- Boyero, L.; Sánchez-Gastaldo, A.; Alonso, M.; Noguera-Uclés, J.F.; Molina-Pinelo, S.; Bernabé-Caro, R. Primary and acquired resistance to immunotherapy in lung cancer: Unveiling the mechanisms underlying of immune checkpoint blockade therapy. Cancers 2020, 12, 3729. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Jiang, W.; Wang, H.; He, J.; Su, C.; Yu, Q. Impact of Smoking History on Response to Immunotherapy in Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 703143. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, R.P.; Sharma, S.; Watabe, K. The confounders of cancer immunotherapy: Roles of lifestyle, metabolic disorders and sociological factors. Cancers 2020, 12, 2983. [Google Scholar] [CrossRef] [PubMed]
- Carbone, D.P.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.M.; Ciuleanu, T.E.; Badin, F.; et al. CheckMate 026 Investigators First-Line Nivolumab in Stage IV or Recurrent Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Method | Summary |
|---|---|
| Algorithm 0 | Linear fitting of D and pf, linear fitting of D* |
| Algorithm 1 | Linear fitting of D and pf, non-linear fitting of D* |
| Algorithm 2 | Linear fitting of D and pf, linear fitting of D*, ignoring D contribution for low b-values |
| Algorithm 3 | Full non-linear fitting of D, pf and D* |
| Results for Fixed-Size ROIs | |||||||
|---|---|---|---|---|---|---|---|
| Units | Mean | St. Dev. | p-Value WMW | Correlation with PD-L1 Protein | |||
| G0 | G1 | G0 | G1 | ||||
| ADC | µm2/s × 106 | 1445.8 | 1519.8 | 359.6 | 310.7 | 0.842 | −0.073 |
| D | µm2/s × 106 | 1173.3 | 1327.0 | 289.5 | 373.0 | 0.356 | 0.035 |
| D* | µm2/s × 104 | 189.2 | 122.0 | 65.7 | 31.3 | 0.008 | −0.374 |
| pf | µm2/s × 103 | 274.3 | 209.7 | 184.9 | 82.1 | 0.549 | −0.148 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bortolotto, C.; Stella, G.M.; Messana, G.; Lo Tito, A.; Podrecca, C.; Nicora, G.; Bellazzi, R.; Gerbasi, A.; Agustoni, F.; Grimm, R.; et al. Correlation between PD-L1 Expression of Non-Small Cell Lung Cancer and Data from IVIM-DWI Acquired during Magnetic Resonance of the Thorax: Preliminary Results. Cancers 2022, 14, 5634. https://doi.org/10.3390/cancers14225634
Bortolotto C, Stella GM, Messana G, Lo Tito A, Podrecca C, Nicora G, Bellazzi R, Gerbasi A, Agustoni F, Grimm R, et al. Correlation between PD-L1 Expression of Non-Small Cell Lung Cancer and Data from IVIM-DWI Acquired during Magnetic Resonance of the Thorax: Preliminary Results. Cancers. 2022; 14(22):5634. https://doi.org/10.3390/cancers14225634
Chicago/Turabian StyleBortolotto, Chandra, Giulia Maria Stella, Gaia Messana, Antonio Lo Tito, Chiara Podrecca, Giovanna Nicora, Riccardo Bellazzi, Alessia Gerbasi, Francesco Agustoni, Robert Grimm, and et al. 2022. "Correlation between PD-L1 Expression of Non-Small Cell Lung Cancer and Data from IVIM-DWI Acquired during Magnetic Resonance of the Thorax: Preliminary Results" Cancers 14, no. 22: 5634. https://doi.org/10.3390/cancers14225634
APA StyleBortolotto, C., Stella, G. M., Messana, G., Lo Tito, A., Podrecca, C., Nicora, G., Bellazzi, R., Gerbasi, A., Agustoni, F., Grimm, R., Zacà, D., Filippi, A. R., Bottinelli, O. M., & Preda, L. (2022). Correlation between PD-L1 Expression of Non-Small Cell Lung Cancer and Data from IVIM-DWI Acquired during Magnetic Resonance of the Thorax: Preliminary Results. Cancers, 14(22), 5634. https://doi.org/10.3390/cancers14225634