Cell-Free DNA Analysis within the Challenges of Thyroid Cancer Management

 , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
3. cfDNA Analysis in Thyroid Cancers
3.1. Detection of Circulating Cell-Free BRAFV600E in PTC
3.2. Detection of Circulating Cell-Free M918T RET in MTC
3.3. Tissue-Based Multigene cfDNA Studies
3.4. Assessment of cfDNA Quantity and Quality
4. Diagnostics
4.1. Clinical Challenges
4.2. Role of cfDNA Analysis
5. Prognostics
5.1. Clinical Challenges
5.2. Role of cfDNA
6. Follow-Up Phase
6.1. Clinical Challenges
6.2. Role of cfDNA
7. Management of Advanced Disease
7.1. Clinical Challenges
7.2. Role of cfDNA
8. Conclusions

Author Contributions
Funding
Conflicts of Interest
References
- Davies, L.; Welch, H.G. Current Thyroid Cancer Trends in the United States. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974–2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef]
- Schlumberger, M.J. Papillary and follicular thyroid carcinoma. N. Engl. J. Med. 1998, 338, 297–306. [Google Scholar] [CrossRef] [PubMed]
- McLeod, D.S.; Sawka, A.M.; Cooper, D.S. Controversies in primary treatment of low-risk papillary thyroid cancer. Lancet 2013, 381, 1046–1057. [Google Scholar] [CrossRef]
- Passler, C.; Scheuba, C.; Prager, G.; Kaczirek, K.; Kaserer, K.; Zettinig, G.; Niederle, B. Prognostic factors of papillary and follicular thyroid cancer: Differences in an iodine-replete endemic goiter region. Endocr. Relat. Cancer 2004, 11, 131–139. [Google Scholar] [CrossRef]
- Chiofalo, M.G.; D’Anna, R.; Di Gennaro, F.; Setola, S.V.; Marotta, V. Great veins invasion in follicular thyroid cancer: Single-centre study assessing prevalence and clinical outcome. Endocrine 2018, 62, 71–75. [Google Scholar] [CrossRef]
- Grebe, S.K.; Hay, I.D. Follicular thyroid cancer. Endocrinol. Metab. Clin. N. Am. 1995, 24, 761–801. [Google Scholar] [CrossRef]
- Wada, N.; Duh, Q.Y.; Miura, D.; Brunaud, L.; Wong, M.G.; Clark, O.H. Chromosomal aberrations by comparative genomic hybridization in hurthle cell thyroid carcinomas are associated with tumor recurrence. J. Clin. Endocrinol. Metab. 2002, 87, 4595–4601. [Google Scholar] [CrossRef]
- Sabra, M.M.; Ghossein, R.; Tuttle, R.M. Time Course and Predictors of Structural Disease Progression in Pulmonary Metastases Arising from Follicular Cell-Derived Thyroid Cancer. Thyroid 2016, 26, 518–524. [Google Scholar] [CrossRef]
- Sanders, E.M., Jr.; LiVolsi, V.A.; Brierley, J.; Shin, J.; Randolph, G.W. An evidence-based review of poorly differentiated thyroid cancer. World J. Surg. 2007, 31, 934–945. [Google Scholar] [CrossRef]
- Lee, D.Y.; Won, J.K.; Lee, S.H.; Park, D.J.; Jung, K.C.; Sung, M.W.; Wu, H.G.; Kim, K.H.; Park, Y.J.; Hah, J.H. Changes of Clinicopathologic Characteristics and Survival Outcomes of Anaplastic and Poorly Differentiated Thyroid Carcinoma. Thyroid 2016, 26, 404–413. [Google Scholar] [CrossRef]
- Molinaro, E.; Romei, C.; Biagini, A.; Sabini, E.; Agate, L.; Mazzeo, S.; Materazzi, G.; Sellari-Franceschini, S.; Ribechini, A.; Torregrossa, L.; et al. Anaplastic thyroid carcinoma: From clinicopathology to genetics and advanced therapies. Nat. Rev. Endocrinol. 2017, 13, 644–660. [Google Scholar] [CrossRef]
- Kuo, E.J.; Sho, S.; Li, N.; Zanocco, K.A.; Yeh, M.W.; Livhits, M.J. Risk Factors Associated with Reoperation and Disease-Specific Mortality in Patients with Medullary Thyroid Carcinoma. JAMA Surg. 2018, 153, 52–59. [Google Scholar] [CrossRef]
- Marotta, V.; Sciammarella, C.; Colao, A.A.; Faggiano, A. Application of molecular biology of differentiated thyroid cancer for clinical prognostication. Endocr. Relat. Cancer 2016, 23, R499–R515. [Google Scholar] [CrossRef]
- Sun, K.; Jiang, P.; Chan, K.C.; Wong, J.; Cheng, Y.K.; Liang, R.H.; Chan, W.K.; Ma, E.S.; Chan, S.L.; Cheng, S.H.; et al. Plasma DNA tissue mapping by genome-wide methylation sequencing for noninvasive prenatal, cancer, and transplantation assessments. Proc. Natl. Acad. Sci. USA 2015, 112, E5503–E5512. [Google Scholar] [CrossRef] [PubMed]
- Phallen, J.; Sausen, M.; Adleff, V.; Leal, A.; Hruban, C.; White, J.; Anagnostou, V.; Fiksel, J.; Cristiano, S.; Papp, E.; et al. Direct detection of early-stage cancers using circulating tumor DNA. Sci. Transl. Med. 2017, 9, eaan2415. [Google Scholar] [CrossRef]
- Thierry, A.R.; El Messaoudi, S.; Gahan, P.B.; Anker, P.; Stroun, M. Origins, structures, and functions of circulating DNA in oncology. Cancer Metastasis Rev. 2016, 35, 347–376. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Hsieh, J.S.; Chang, M.Y.; Huang, T.J.; Chen, F.M.; Cheng, T.L.; Alexandersen, K.; Huang, Y.S.; Tzou, W.S.; Lin, S.R. Molecular detection of APC, K-ras, and p53 mutations in the serum of colorectal cancer patients as circulating biomarkers. World J. Surg. 2004, 28, 721–726. [Google Scholar] [CrossRef]
- Fujiwara, K.; Fujimoto, N.; Tabata, M.; Nishii, K.; Matsuo, K.; Hotta, K.; Kozuki, T.; Aoe, M.; Kiura, K.; Ueoka, H.; et al. Identification of epigenetic aberrant promoter methylation in serum DNA is useful for early detection of lung cancer. Clin Cancer Res 2005, 11, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- La Thangue, N.B.; Kerr, D.J. Predictive biomarkers: A paradigm shift towards personalized cancer medicine. Nat. Rev. Clin. Oncol. 2011, 8, 587–596. [Google Scholar] [CrossRef]
- Thierry, A.R.; Mouliere, F.; El Messaoudi, S.; Mollevi, C.; Lopez-Crapez, E.; Rolet, F.; Gillet, B.; Gongora, C.; Dechelotte, P.; Robert, B.; et al. Clinical validation of the detection of KRAS and BRAF mutations from circulating tumor DNA. Nat. Med. 2014, 20, 430–435. [Google Scholar] [CrossRef]
- Basik, M.; Aguilar-Mahecha, A.; Rousseau, C.; Diaz, Z.; Tejpar, S.; Spatz, A.; Greenwood, C.M.; Batist, G. Biopsies: Next-generation biospecimens for tailoring therapy. Nat. Rev. Clin. Oncol. 2013, 10, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Gerlinger, M.; Rowan, A.J.; Horswell, S.; Math, M.; Larkin, J.; Endesfelder, D.; Gronroos, E.; Martinez, P.; Matthews, N.; Stewart, A.; et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N. Engl. J. Med. 2012, 366, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Clark, T.A.; Chung, J.H.; Kennedy, M.; Hughes, J.D.; Chennagiri, N.; Lieber, D.S.; Fendler, B.; Young, L.; Zhao, M.; Coyne, M.; et al. Analytical Validation of a Hybrid Capture-Based Next-Generation Sequencing Clinical Assay for Genomic Profiling of Cell-Free Circulating Tumor DNA. J. Mol. Diagn. JMD 2018, 20, 686–702. [Google Scholar] [CrossRef]
- Chae, Y.K.; Davis, A.A.; Jain, S.; Santa-Maria, C.; Flaum, L.; Beaubier, N.; Platanias, L.C.; Gradishar, W.; Giles, F.J.; Cristofanilli, M. Concordance of Genomic Alterations by Next-Generation Sequencing in Tumor Tissue versus Circulating Tumor DNA in Breast Cancer. Mol. Cancer Ther. 2017, 16, 1412–1420. [Google Scholar] [CrossRef]
- Chan, K.C.; Jiang, P.; Chan, C.W.; Sun, K.; Wong, J.; Hui, E.P.; Chan, S.L.; Chan, W.C.; Hui, D.S.; Ng, S.S.; et al. Noninvasive detection of cancer-associated genome-wide hypomethylation and copy number aberrations by plasma DNA bisulfite sequencing. Proc. Natl. Acad. Sci. USA 2013, 110, 18761–18768. [Google Scholar] [CrossRef]
- Leighl, N.B.; Page, R.D.; Raymond, V.M.; Daniel, D.B.; Divers, S.G.; Reckamp, K.L.; Villalona-Calero, M.A.; Dix, D.; Odegaard, J.I.; Lanman, R.B.; et al. Clinical Utility of Comprehensive Cell-free DNA Analysis to Identify Genomic Biomarkers in Patients with Newly Diagnosed Metastatic Non-small Cell Lung Cancer. Clin. Cancer Res. 2019, 25, 4691–4700. [Google Scholar] [CrossRef]
- Schou, J.V.; Larsen, F.O.; Sorensen, B.S.; Abrantes, R.; Boysen, A.K.; Johansen, J.S.; Jensen, B.V.; Nielsen, D.L.; Spindler, K.L. Circulating cell-free DNA as predictor of treatment failure after neoadjuvant chemo-radiotherapy before surgery in patients with locally advanced rectal cancer. Ann. Oncol. 2018, 29, 610–615. [Google Scholar] [CrossRef]
- Agostini, M.; Pucciarelli, S.; Enzo, M.V.; Del Bianco, P.; Briarava, M.; Bedin, C.; Maretto, I.; Friso, M.L.; Lonardi, S.; Mescoli, C.; et al. Circulating cell-free DNA: A promising marker of pathologic tumor response in rectal cancer patients receiving preoperative chemoradiotherapy. Ann. Surg. Oncol. 2011, 18, 2461–2468. [Google Scholar] [CrossRef]
- Ottaviano, M.; Giuliano, M.; Tortora, M.; La Civita, E.; Liotti, A.; Longo, M.; Bruzzese, D.; Cennamo, M.; Riccio, V.; De Placido, P.; et al. A New Horizon of Liquid Biopsy in Thymic Epithelial Tumors: The Potential Utility of Circulating Cell-Free DNA. Front. Oncol. 2020, 10, 602153. [Google Scholar] [CrossRef]
- Carow, K.; Read, C.; Hafner, N.; Runnebaum, I.B.; Corner, A.; Durst, M. A comparative study of digital PCR and real-time qPCR for the detection and quantification of HPV mRNA in sentinel lymph nodes of cervical cancer patients. BMC Res. Notes 2017, 10, 532. [Google Scholar] [CrossRef]
- Elazezy, M.; Joosse, S.A. Techniques of using circulating tumor DNA as a liquid biopsy component in cancer management. Comput. Struct. Biotechnol. J. 2018, 16, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Uchida, J.; Kato, K.; Kukita, Y.; Kumagai, T.; Nishino, K.; Daga, H.; Nagatomo, I.; Inoue, T.; Kimura, M.; Oba, S.; et al. Diagnostic Accuracy of Noninvasive Genotyping of EGFR in Lung Cancer Patients by Deep Sequencing of Plasma Cell-Free DNA. Clin. Chem. 2015, 61, 1191–1196. [Google Scholar] [CrossRef]
- Zane, M.; Agostini, M.; Enzo, M.V.; Casal Ide, E.; Del Bianco, P.; Torresan, F.; Merante Boschin, I.; Pennelli, G.; Saccani, A.; Rubello, D.; et al. Circulating cell-free DNA, SLC5A8 and SLC26A4 hypermethylation, BRAF(V600E): A non-invasive tool panel for early detection of thyroid cancer. Biomed. Pharmacother. 2013, 67, 723–730. [Google Scholar] [CrossRef]
- Salvianti, F.; Giuliani, C.; Petrone, L.; Mancini, I.; Vezzosi, V.; Pupilli, C.; Pinzani, P. Integrity and Quantity of Total Cell-Free DNA in the Diagnosis of Thyroid Cancer: Correlation with Cytological Classification. Int. J. Mol. Sci. 2017, 18, 1350. [Google Scholar] [CrossRef]
- Pupilli, C.; Pinzani, P.; Salvianti, F.; Fibbi, B.; Rossi, M.; Petrone, L.; Perigli, G.; De Feo, M.L.; Vezzosi, V.; Pazzagli, M.; et al. Circulating BRAFV600E in the diagnosis and follow-up of differentiated papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2013, 98, 3359–3365. [Google Scholar] [CrossRef]
- Patel, K.B.; Cormier, N.; Fowler, J.; Partridge, A.; Theurer, J.; Black, M.; Pinto, N.; Yoo, J.; Fung, K.; MacNeil, D.; et al. Detection of Circulating Tumor DNA in Patients with Thyroid Nodules. Int. J. Endocrinol. 2021, 2021, 8909224. [Google Scholar] [CrossRef]
- Hu, S.; Ewertz, M.; Tufano, R.P.; Brait, M.; Carvalho, A.L.; Liu, D.; Tufaro, A.P.; Basaria, S.; Cooper, D.S.; Sidransky, D.; et al. Detection of serum deoxyribonucleic acid methylation markers: A novel diagnostic tool for thyroid cancer. J. Clin. Endocrinol. Metab. 2006, 91, 98–104. [Google Scholar] [CrossRef]
- Kim, B.H.; Kim, I.J.; Lee, B.J.; Lee, J.C.; Kim, I.S.; Kim, S.J.; Kim, W.J.; Jeon, Y.K.; Kim, S.S.; Kim, Y.K. Detection of plasma BRAF(V600E) mutation is associated with lung metastasis in papillary thyroid carcinomas. Yonsei Med. J. 2015, 56, 634–640. [Google Scholar] [CrossRef]
- Cradic, K.W.; Milosevic, D.; Rosenberg, A.M.; Erickson, L.A.; McIver, B.; Grebe, S.K. Mutant BRAF(T1799A) can be detected in the blood of papillary thyroid carcinoma patients and correlates with disease status. J. Clin. Endocrinol. Metab. 2009, 94, 5001–5009. [Google Scholar] [CrossRef]
- Kwak, J.Y.; Jeong, J.J.; Kang, S.W.; Park, S.; Choi, J.R.; Park, S.J.; Kim, E.K.; Chung, W.Y. Study of peripheral BRAF(V600E) mutation as a possible novel marker for papillary thyroid carcinomas. Head Neck 2013, 35, 1630–1633. [Google Scholar] [CrossRef] [PubMed]
- Condello, V.; Macerola, E.; Ugolini, C.; De Napoli, L.; Romei, C.; Materazzi, G.; Elisei, R.; Basolo, F. Analysis of circulating tumor DNA does not improve the clinical management of patients with locally advanced and metastatic papillary thyroid carcinoma. Head Neck 2018, 40, 1752–1758. [Google Scholar] [CrossRef] [PubMed]
- Klimaite, R.; Kazokaite, M.; Kondrotiene, A.; Dauksiene, D.; Verkauskiene, R.; Zilaitiene, B.; Dauksa, A. Diagnostic Value of Circulating Cell-free DNA in Patients with Papillary Thyroid Cancer. Anticancer Res. 2022, 42, 2289–2299. [Google Scholar] [CrossRef] [PubMed]
- Higazi, A.M.; El Hini, S.H.; El-Sharkawy, E.A.; Gayyed, M.F.; Aziz, N.A.; Matta, R.A. Diagnostic Role of Cell-free DNA Integrity in Thyroid Cancer Particularly for Bethesda IV Cytology. Endocr. Pract. 2021, 27, 673–681. [Google Scholar] [CrossRef]
- Lan, X.; Bao, H.; Ge, X.; Cao, J.; Fan, X.; Zhang, Q.; Liu, K.; Zhang, X.; Tan, Z.; Zheng, C.; et al. Genomic landscape of metastatic papillary thyroid carcinoma and novel biomarkers for predicting distant metastasis. Cancer Sci. 2020, 111, 2163–2173. [Google Scholar] [CrossRef] [PubMed]
- Sandulache, V.C.; Williams, M.D.; Lai, S.Y.; Lu, C.; William, W.N.; Busaidy, N.L.; Cote, G.J.; Singh, R.R.; Luthra, R.; Cabanillas, M.E. Real-Time Genomic Characterization Utilizing Circulating Cell-Free DNA in Patients with Anaplastic Thyroid Carcinoma. Thyroid Off. J. Am. Thyroid Assoc. 2017, 27, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Ciampi, R.; Romei, C.; Ramone, T.; Matrone, A.; Prete, A.; Gambale, C.; Materazzi, G.; De Napoli, L.; Torregrossa, L.; Basolo, F.; et al. Pre- and Post-Operative Circulating Tumoral DNA in Patients with Medullary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2022, 107, e3420–e3427. [Google Scholar] [CrossRef]
- Qin, Y.; Wang, J.R.; Wang, Y.; Iyer, P.; Cote, G.J.; Busaidy, N.L.; Dadu, R.; Zafereo, M.; Williams, M.D.; Ferrarotto, R.; et al. Clinical Utility of Circulating Cell-Free DNA Mutations in Anaplastic Thyroid Carcinoma. Thyroid 2021, 31, 1235–1243. [Google Scholar] [CrossRef]
- Jensen, K.; Thakur, S.; Patel, A.; Mendonca-Torres, M.C.; Costello, J.; Gomes-Lima, C.J.; Walter, M.; Wartofsky, L.; Burman, K.D.; Bikas, A.; et al. Detection of BRAFV600E in Liquid Biopsy from Patients with Papillary Thyroid Cancer Is Associated with Tumor Aggressiveness and Response to Therapy. J. Clin. Med. 2020, 9, 2481. [Google Scholar] [CrossRef]
- Sato, A.; Tanabe, M.; Tsuboi, Y.; Niwa, T.; Shinozaki-Ushiku, A.; Seto, Y.; Murakami, Y. Circulating Tumor DNA Harboring the BRAF(V600E) Mutation May Predict Poor Outcomes of Primary Papillary Thyroid Cancer Patients. Thyroid 2021, 31, 1822–1828. [Google Scholar] [CrossRef]
- Cote, G.J.; Evers, C.; Hu, M.I.; Grubbs, E.G.; Williams, M.D.; Hai, T.; Duose, D.Y.; Houston, M.R.; Bui, J.H.; Mehrotra, M.; et al. Prognostic Significance of Circulating RET M918T Mutated Tumor DNA in Patients with Advanced Medullary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2017, 102, 3591–3599. [Google Scholar] [CrossRef] [PubMed]
- Allin, D.M.; Shaikh, R.; Carter, P.; Thway, K.; Sharabiani, M.T.A.; Gonzales-de-Castro, D.; O’Leary, B.; Garcia-Murillas, I.; Bhide, S.; Hubank, M.; et al. Circulating tumour DNA is a potential biomarker for disease progression and response to targeted therapy in advanced thyroid cancer. Eur. J. Cancer 2018, 103, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Gouda, M.A.; Ong, E.; Huang, H.J.; McPhaul, L.W.; Yoon, S.; Janku, F.; Gianoukakis, A.G. Ultrasensitive detection of BRAF V600E mutations in circulating tumor DNA of patients with metastatic thyroid cancer. Endocrine 2022, 76, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Xing, M. Molecular pathogenesis and mechanisms of thyroid cancer. Nat. Rev. Cancer 2013, 13, 184–199. [Google Scholar] [CrossRef] [PubMed]
- Guerra, A.; Sapio, M.R.; Marotta, V.; Campanile, E.; Rossi, S.; Forno, I.; Fugazzola, L.; Budillon, A.; Moccia, T.; Fenzi, G.; et al. The primary occurrence of BRAF(V600E) is a rare clonal event in papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2012, 97, 517–524. [Google Scholar] [CrossRef]
- Gandolfi, G.; Sancisi, V.; Torricelli, F.; Ragazzi, M.; Frasoldati, A.; Piana, S.; Ciarrocchi, A. Allele percentage of the BRAF V600E mutation in papillary thyroid carcinomas and corresponding lymph node metastases: No evidence for a role in tumor progression. J. Clin. Endocrinol. Metab. 2013, 98, E934–E942. [Google Scholar] [CrossRef]
- Fugazzola, L.; Muzza, M.; Pogliaghi, G.; Vitale, M. Intratumoral Genetic Heterogeneity in Papillary Thyroid Cancer: Occurrence and Clinical Significance. Cancers 2020, 12, 383. [Google Scholar] [CrossRef]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF gene in human cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef]
- Elisei, R.; Cosci, B.; Romei, C.; Bottici, V.; Renzini, G.; Molinaro, E.; Agate, L.; Vivaldi, A.; Faviana, P.; Basolo, F.; et al. Prognostic significance of somatic RET oncogene mutations in sporadic medullary thyroid cancer: A 10-year follow-up study. J. Clin. Endocrinol. Metab. 2008, 93, 682–687. [Google Scholar] [CrossRef]
- Jahr, S.; Hentze, H.; Englisch, S.; Hardt, D.; Fackelmayer, F.O.; Hesch, R.D.; Knippers, R. DNA fragments in the blood plasma of cancer patients: Quantitations and evidence for their origin from apoptotic and necrotic cells. Cancer Res. 2001, 61, 1659–1665. [Google Scholar]
- Huang, Z.; Bassil, C.F.; Murphy, S.K. Methylation-specific PCR. Methods Mol. Biol. 2013, 1049, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Papini, E.; Guglielmi, R.; Bianchini, A.; Crescenzi, A.; Taccogna, S.; Nardi, F.; Panunzi, C.; Rinaldi, R.; Toscano, V.; Pacella, C.M. Risk of malignancy in nonpalpable thyroid nodules: Predictive value of ultrasound and color-Doppler features. J. Clin. Endocrinol. Metab. 2002, 87, 1941–1946. [Google Scholar] [CrossRef]
- Remonti, L.R.; Kramer, C.K.; Leitao, C.B.; Pinto, L.C.; Gross, J.L. Thyroid ultrasound features and risk of carcinoma: A systematic review and meta-analysis of observational studies. Thyroid 2015, 25, 538–550. [Google Scholar] [CrossRef]
- Kovatcheva, R.D.; Shinkov, A.D.; Dimitrova, I.D.; Ivanova, R.B.; Vidinov, K.N.; Ivanova, R.S. Evaluation of the Diagnostic Performance of EU-TIRADS in Discriminating Benign from Malignant Thyroid Nodules: A Prospective Study in One Referral Center. Eur. Thyroid J. 2021, 9, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Scappaticcio, L.; Maiorino, M.I.; Iorio, S.; Docimo, G.; Longo, M.; Grandone, A.; Luongo, C.; Cozzolino, I.; Piccardo, A.; Trimboli, P.; et al. Exploring the Performance of Ultrasound Risk Stratification Systems in Thyroid Nodules of Pediatric Patients. Cancers 2021, 13, 5304. [Google Scholar] [CrossRef] [PubMed]
- Cap, J.; Ryska, A.; Rehorkova, P.; Hovorkova, E.; Kerekes, Z.; Pohnetalova, D. Sensitivity and specificity of the fine needle aspiration biopsy of the thyroid: Clinical point of view. Clin. Endocrinol. 1999, 51, 509–515. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedus, L.; Paschke, R.; Valcavi, R.; Vitti, P. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules—2016 Update. Endocr. Pract. 2016, 22, 622–639. [Google Scholar] [CrossRef]
- Dutta, S.; Tarafdar, S.; Mukhopadhyay, P.; Bhattacharyya, N.P.; Ghosh, S. Plasma Cell-Free DNA to Differentiate Malignant from Benign Thyroid Nodules. J. Clin. Endocrinol. Metab. 2021, 106, e2262–e2270. [Google Scholar] [CrossRef]
- Marotta, V.; Bifulco, M.; Vitale, M. Significance of RAS Mutations in Thyroid Benign Nodules and Non-Medullary Thyroid Cancer. Cancers 2021, 13, 3785. [Google Scholar] [CrossRef]
- Marotta, V.; Sapio, M.R.; Guerra, A.; Vitale, M. BRAF mutation in cytology samples as a diagnostic tool for papillary thyroid carcinoma. Expert Opin. Med. Diagn. 2011, 5, 277–290. [Google Scholar] [CrossRef]
- Pitoia, F.; Bueno, F.; Urciuoli, C.; Abelleira, E.; Cross, G.; Tuttle, R.M. Outcomes of patients with differentiated thyroid cancer risk-stratified according to the American thyroid association and Latin American thyroid society risk of recurrence classification systems. Thyroid 2013, 23, 1401–1407. [Google Scholar] [CrossRef] [PubMed]
- Eustatia-Rutten, C.F.; Corssmit, E.P.; Biermasz, N.R.; Pereira, A.M.; Romijn, J.A.; Smit, J.W. Survival and death causes in differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2006, 91, 313–319. [Google Scholar] [CrossRef]
- Momesso, D.P.; Tuttle, R.M. Update on differentiated thyroid cancer staging. Endocrinol. Metab. Clin. N. Am. 2014, 43, 401–421. [Google Scholar] [CrossRef]
- Castagna, M.G.; Maino, F.; Cipri, C.; Belardini, V.; Theodoropoulou, A.; Cevenini, G.; Pacini, F. Delayed risk stratification, to include the response to initial treatment (surgery and radioiodine ablation), has better outcome predictivity in differentiated thyroid cancer patients. Eur. J. Endocrinol. 2011, 165, 441–446. [Google Scholar] [CrossRef]
- Lamartina, L.; Grani, G.; Arvat, E.; Nervo, A.; Zatelli, M.C.; Rossi, R.; Puxeddu, E.; Morelli, S.; Torlontano, M.; Massa, M.; et al. 8th edition of the AJCC/TNM staging system of thyroid cancer: What to expect (ITCO#2). Endocr. Relat. Cancer 2018, 25, L7–L11. [Google Scholar] [CrossRef]
- Park, S.Y.; Cho, Y.Y.; Kim, H.I.; Choe, J.H.; Kim, J.H.; Kim, J.S.; Oh, Y.L.; Hahn, S.Y.; Shin, J.H.; Kim, K.; et al. Clinical Validation of the Prognostic Stage Groups of the Eighth-Edition TNM Staging for Medullary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2018, 103, 4609–4616. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2015, 26, 1–133. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Tala, H.; Shah, J.; Leboeuf, R.; Ghossein, R.; Gonen, M.; Brokhin, M.; Omry, G.; Fagin, J.A.; Shaha, A. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: Using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid 2010, 20, 1341–1349. [Google Scholar] [CrossRef]
- Enewold, L.; Zhu, K.; Ron, E.; Marrogi, A.J.; Stojadinovic, A.; Peoples, G.E.; Devesa, S.S. Rising thyroid cancer incidence in the United States by demographic and tumor characteristics, 1980–2005. Cancer Epidemiol. Biomark. Prev. 2009, 18, 784–791. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Cham, Switzerland; American Joint Commission on Cancer: Chicago, IL, USA, 2017. [Google Scholar]
- Guerra, A.; Fugazzola, L.; Marotta, V.; Cirillo, M.; Rossi, S.; Cirello, V.; Forno, I.; Moccia, T.; Budillon, A.; Vitale, M. A high percentage of BRAFV600E alleles in papillary thyroid carcinoma predicts a poorer outcome. J. Clin. Endocrinol. Metab. 2012, 97, 2333–2340. [Google Scholar] [CrossRef] [PubMed]
- Barbet, J.; Campion, L.; Kraeber-Bodere, F.; Chatal, J.F. Prognostic impact of serum calcitonin and carcinoembryonic antigen doubling-times in patients with medullary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2005, 90, 6077–6084. [Google Scholar] [CrossRef] [PubMed]
- Laure Giraudet, A.; Al Ghulzan, A.; Auperin, A.; Leboulleux, S.; Chehboun, A.; Troalen, F.; Dromain, C.; Lumbroso, J.; Baudin, E.; Schlumberger, M. Progression of medullary thyroid carcinoma: Assessment with calcitonin and carcinoembryonic antigen doubling times. Eur. J. Endocrinol. 2008, 158, 239–246. [Google Scholar] [CrossRef]
- Marotta, V.; Botti, G.; Ionna, F.; Pezzullo, L. TSH modulation in advanced differentiated thyroid cancer: A continuous walk on the tightrope between prognostic stratification, adverse events, and levothyroxine bioavailability. Minerva Endocrinol. 2022, 47, 99–102. [Google Scholar] [CrossRef]
- Eustatia-Rutten, C.F.; Smit, J.W.; Romijn, J.A.; van der Kleij-Corssmit, E.P.; Pereira, A.M.; Stokkel, M.P.; Kievit, J. Diagnostic value of serum thyroglobulin measurements in the follow-up of differentiated thyroid carcinoma, a structured meta-analysis. Clin. Endocrinol. 2004, 61, 61–74. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Trimboli, P.; Verburg, F.A.; Giovanella, L. Significance of “de novo” appearance of thyroglobulin antibodies in patients with differentiated thyroid cancer. Int. J. Biol. Mark. 2020, 35, 41–49. [Google Scholar] [CrossRef]
- Hiltzik, D.; Carlson, D.L.; Tuttle, R.M.; Chuai, S.; Ishill, N.; Shaha, A.; Shah, J.P.; Singh, B.; Ghossein, R.A. Poorly differentiated thyroid carcinomas defined on the basis of mitosis and necrosis: A clinicopathologic study of 58 patients. Cancer 2006, 106, 1286–1295. [Google Scholar] [CrossRef]
- Mazzaferri, E.L.; Robbins, R.J.; Spencer, C.A.; Braverman, L.E.; Pacini, F.; Wartofsky, L.; Haugen, B.R.; Sherman, S.I.; Cooper, D.S.; Braunstein, G.D.; et al. A consensus report of the role of serum thyroglobulin as a monitoring method for low-risk patients with papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2003, 88, 1433–1441. [Google Scholar] [CrossRef]
- Baudin, E.; Do Cao, C.; Cailleux, A.F.; Leboulleux, S.; Travagli, J.P.; Schlumberger, M. Positive predictive value of serum thyroglobulin levels, measured during the first year of follow-up after thyroid hormone withdrawal, in thyroid cancer patients. J. Clin. Endocrinol. Metab. 2003, 88, 1107–1111. [Google Scholar] [CrossRef]
- Durante, C.; Montesano, T.; Attard, M.; Torlontano, M.; Monzani, F.; Costante, G.; Meringolo, D.; Ferdeghini, M.; Tumino, S.; Lamartina, L.; et al. Long-term surveillance of papillary thyroid cancer patients who do not undergo postoperative radioiodine remnant ablation: Is there a role for serum thyroglobulin measurement? J. Clin. Endocrinol. Metab. 2012, 97, 2748–2753. [Google Scholar] [CrossRef]
- Pazaitou-Panayiotou, K.; Chrisoulidou, A.; Mandanas, S.; Tziomalos, K.; Doumala, E.; Patakiouta, F. Predictive factors that influence the course of medullary thyroid carcinoma. Int. J. Clin. Oncol. 2014, 19, 445–451. [Google Scholar] [CrossRef]
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; De Vathaire, F.; et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocrinol. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef]
- Modigliani, E.; Cohen, R.; Campos, J.M.; Conte-Devolx, B.; Maes, B.; Boneu, A.; Schlumberger, M.; Bigorgne, J.C.; Dumontier, P.; Leclerc, L.; et al. Prognostic factors for survival and for biochemical cure in medullary thyroid carcinoma: Results in 899 patients. The GETC Study Group. Groupe d’etude des tumeurs a calcitonine. Clin. Endocrinol. 1998, 48, 265–273. [Google Scholar] [CrossRef]
- Marotta, V.; Sciammarella, C.; Vitale, M.; Colao, A.; Faggiano, A. The evolving field of kinase inhibitors in thyroid cancer. Crit. Rev. Oncol. Hematol. 2015, 93, 60–73. [Google Scholar] [CrossRef]
- Marotta, V.; Chiofalo, M.G.; Di Gennaro, F.; Daponte, A.; Sandomenico, F.; Vallone, P.; Costigliola, L.; Botti, G.; Ionna, F.; Pezzullo, L. Kinase-inhibitors for iodine-refractory differentiated thyroid cancer: Still far from a structured therapeutic algorithm. Crit. Rev. Oncol. Hematol. 2021, 162, 103353. [Google Scholar] [CrossRef]
- Liu, H.; Yang, D.; Li, L.; Tu, Y.; Chen, C.; Sun, S. Appraisal of radioiodine refractory thyroid cancer: Advances and challenges. Am. J. Cancer Res. 2020, 10, 1923–1936. [Google Scholar]
- Bachelot, A.; Cailleux, A.F.; Klain, M.; Baudin, E.; Ricard, M.; Bellon, N.; Caillou, B.; Travagli, J.P.; Schlumberger, M. Relationship between tumor burden and serum thyroglobulin level in patients with papillary and follicular thyroid carcinoma. Thyroid 2002, 12, 707–711. [Google Scholar] [CrossRef]
- Brose, M.S.; Schlumbeger, M.; Jeffers, M.; Kappeler, C.; Meinhardt, G.; Pena, C.E.A. Analysis of Biomarkers and Association with Clinical Outcomes in Patients with Differentiated Thyroid Cancer: Subanalysis of the Sorafenib Phase III DECISION Trial. Clin. Cancer Res. 2019, 25, 7370–7380. [Google Scholar] [CrossRef]
- Tahara, M.; Schlumberger, M.; Elisei, R.; Habra, M.A.; Kiyota, N.; Paschke, R.; Dutcus, C.E.; Hihara, T.; McGrath, S.; Matijevic, M.; et al. Exploratory analysis of biomarkers associated with clinical outcomes from the study of lenvatinib in differentiated cancer of the thyroid. Eur. J. Cancer 2017, 75, 213–221. [Google Scholar] [CrossRef]
- Wells, S.A., Jr.; Robinson, B.G.; Gagel, R.F.; Dralle, H.; Fagin, J.A.; Santoro, M.; Baudin, E.; Elisei, R.; Jarzab, B.; Vasselli, J.R.; et al. Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: A randomized, double-blind phase III trial. J. Clin. Oncol. 2012, 30, 134–141. [Google Scholar] [CrossRef]
- Elisei, R.; Schlumberger, M.J.; Muller, S.P.; Schoffski, P.; Brose, M.S.; Shah, M.H.; Licitra, L.; Jarzab, B.; Medvedev, V.; Kreissl, M.C.; et al. Cabozantinib in progressive medullary thyroid cancer. J. Clin. Oncol. 2013, 31, 3639–3646. [Google Scholar] [CrossRef] [PubMed]
- Smallridge, R.C.; Marlow, L.A.; Copland, J.A. Anaplastic thyroid cancer: Molecular pathogenesis and emerging therapies. Endocr. Relat. Cancer 2009, 16, 17–44. [Google Scholar] [CrossRef]
- Ferrari, S.M.; Elia, G.; Ragusa, F.; Ruffilli, I.; La Motta, C.; Paparo, S.R.; Patrizio, A.; Vita, R.; Benvenga, S.; Materazzi, G.; et al. Novel treatments for anaplastic thyroid carcinoma. Gland Surg. 2020, 9, S28–S42. [Google Scholar] [CrossRef] [PubMed]
- Bible, K.C.; Kebebew, E.; Brierley, J.; Brito, J.P.; Cabanillas, M.E.; Clark, T.J., Jr.; Di Cristofano, A.; Foote, R.; Giordano, T.; Kasperbauer, J.; et al. 2021 American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2021, 31, 337–386. [Google Scholar] [CrossRef] [PubMed]
- Geeurickx, E.; Hendrix, A. Targets, pitfalls and reference materials for liquid biopsy tests in cancer diagnostics. Mol. Asp. Med. 2020, 72, 100828. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study (Year) | Design | Method/Matrix | N. of PTC | Prevalence of cfBRAFV600E in BRAF Positive PTC (%) | Prevalence of cfBRAFV600E in BRAF Negative PTC (%) |
|---|---|---|---|---|---|
| Kwak et al. (2013) [41] | prospective | qPCR/serum | 94 | 0 | 0 |
| Pupilli et al. (2013) [36] | prospective | allele-specific qPCR/plasma | 22 | 91.7 | 30 |
| Kim et al. (2015) [39] | retrospective | peptide nucleic acid clamp qPCR/plasma | 72 | 6.1 | not available |
| Condello et al. (2018) [42] | prospective | allele-specific qPCR + dPCR/plasma | 46 | 0 * | 0 * |
| Jensen et al. (2020) [49] | prospective | microfluidic dPCR preceded by COLD-PCR/plasma | 57 ** | 42.1 | not applicable |
| Patel et al. (2021) [37] | prospective | qPCR/plasma | 20 | 33.3 | 40 |
| Sato et al. (2021) [50] | prospective | droplet dPCR/plasma | 22 | 31 | 0 |
| Study (Year) | Design | Study Population(N) | cfDNA Analysis * | Main Findings | Diagnostic Performance |
|---|---|---|---|---|---|
| Pupilli et al. (2013) [36] | prospective | 38 PTC, 31 NG, 49 HC. | cfBRAFV600E | Higher percentage of mutated alleles in PTC, as compared with NG. | In the Thy3 cytology, 80% NPV and 33% PPV for PTC vs. NG. |
| Patel et al. (2021) [37] | prospective | 68 PTC, 3 FTC, 38 NG. | cfBRAFV600E | All cfBRAFV600E positive patients were affected with PTC classical variant. | (a) Specificity/PPV 100% for PTC vs. NG; (b) Sensitivity/NPV 22.1/41.8 for PTC vs. NG. |
| Zane et al. (2013) [34] | retrospective | 86 PTC, 58 MTC, 9 ATC, 5 synchronous MTC-FTC, 23 FA, 19 HC. | cfDNA fragments of different length (low:ALU83, long:ALU244): absolute concentration. | Concentrations of both the high and the low-length amplicon were higher in thyroid cancer, as compared with HC. | (a) Low length amplicon: 0.91 AUC, 73.5% sensitivity, and 94.7% specificity for thyroid cancer vs. HC; (b) High length amplicon: 0.84 AUC, 67% sensitivity, and 100% specificity for thyroid cancer vs. HC. |
| Higazi et al. (2021) [44] | retrospective | 18 PTC, 21 FTC, 21 MTC, 25 NG, 25 HC. | cfDNA fragments of different length (low:ALU83, long:ALU244): absolute concentration and integrity index **. | Concentrations of both the high and the low length amplicon and the integrity index were higher in thyroid cancer, as compared with NG and HC | (a) Integrity index: AUC 0.93, sensitivity 86%, and specificity 100% for thyroid cancer vs. HC; AUC 0.97, sensitivity 88%, and specificity 100% for thyroid cancer vs. NG; (b) ALU83 concentration: AUC 0.97, sensitivity 88%, and specificity 92% for thyroid cancer vs. HC; AUC 0.89, sensitivity 72%, and specificity 92% for thyroid cancer vs. NG; (c) ALU244 concentration: AUC 0.98, sensitivity 100%, and specificity 92% for thyroid cancer vs. HC; AUC 0.97, sensitivity 100%, and specificity 84% for thyroid cancer vs. NG; (d) in the Bethesda IV category specificity was 100% for the integrity index and 91% for ALU- 83 and -244 |
| Klimaite et al. (2022) [43] | prospective | 68 PTC and 31 NG, 86 HC. | cfDNA fragments of different length (low:β-actin99, long:β-actin394): absolute concentration and integrity index. | (a) Concentrations of both the high and the low length amplicon were higher in PTC, as compared with HC; (b) The integrity index was higher in PTC, as compared with both HC and NG. | (a) Integrity index: AUC 0.901, sensitivity 98.5%, and specificity 64% for PTC vs. HC; AUC 0.629, sensitivity 69.1%, and specificity 66.7% for PTC vs. NG; (b) β-actin99 concentration: AUC 0.593, sensitivity 75%, and specificity 73.3% for PTC vs. HC; (c) β-actin394 concentration: AUC 0.827, sensitivity 98.5%, and specificity 64% for PTC vs. HC. |
| Dutta et al. (2021) [69] | prospective | 20 PTC, 4 FTC, 13 NG (all with indeterminate cytology [Bethesda III/IV]) | Total cfDNA concentration | cfDNA concentration was higher in thyroid cancer, as compared with NG. | Sensitivity 100%, and specificity 92.3% for thyroid cancer vs. NG. |
| Hu et al. (2006) [38] | prospective | 31 PTC, 7 FTC, 15 NG. | Methylation level of CALCA, CDH1, TIMP3, DAPK, and RARβ2 cfDNA | (a) Methylation of circulating TIMP3 and RARβ2 occurred solely in thyroid cancer; (b) Analysis of each of the included genes was able to predict malignancy with high specificity | (a) Sensitivity for thyroid cancer vs. NG: 29, 24, 21, 32, 32% for CALCA, CDH1, TIMP3, DAPK, RARβ2, respectively; Specificity for thyroid cancer vs. NG: 100, 100, 100, 95, 100% for CALCA, CDH1, TIMP3, DAPK, RARβ2, respectively: (b) The positivity of at least 1 gene showed 68% sensitivity and 95% specificity for thyroid cancer vs. NG |
| Study (Year) | Design | Histology (N) | cfDNA Analysis | Clinico-Pathological Factors * | Outcome * |
|---|---|---|---|---|---|
| Kim et al. (2015) [39] | retrospective | BRAFV600E positive PTC (49) | cfBRAFV600E | Lung metastases p < 0.001. | - |
| Jensen et al. (2020) [49] | prospective | BRAFV600E positive PTC (57) | cfBRAFV600E | High tumor size p = 0.03; Gross extra-thyroidal extension p = 0.02; Pulmonary micro-metastases p = 0.04 High-risk ATA category p = 0.002 | non-excellent treatment response p = 0.001 |
| Sato et al. (2021) [50] | prospective | BRAFV600E positive PTC (57) | cfBRAFV600E ** | Extra-thyroidal extension p = 0.01 High somatic BRAFV600E fractional abundance p < 0.01 | - |
| Patel et al. (2021) [37] | prospective | PTC (45) | cfBRAFV600E | High T-stage p < 0.05 Extra-thyroidal extension p < 0.05. | - |
| Cote et al. (2017) [51] | prospective | Sporadic RET M918T positive MTC (50) with persistent post-surgical disease | cfRET M918T ***. | Distant metastasis p = 0.03 Stage Ivc p = 0.01 | Survival p < 0.0001. |
| Qin et al. (2021) [48] | retrospective | ATC (87) | Mutated cfPIK3CA **** | - | Survival p < 0.05 |
| Ciampi et al. (2022) [47] | prospective | Sporadic MTC harboring somatic mutations (29) | cfDNA detection of the mutations identified on tumor tissue ***** | High values of Ct and CEA p = 0.0307 and 0.0013, respectively ****** High somatic variation allele frequency p = 0.0468 ***** | Persistent biochemical/structural disease p = 0.0005 ******* |
| Zane et al. (2013) [34] | retrospective | PTC (86), MTC (58), ATC (9), synchronous MTC-FTC (5), FA(23) | cfDNA ALU83 and ALU244 concentrations and integrity index ******** | Significant increase from FA/PTC to ATC (ALU83 concentration p < 0.0001; ALU244 concentration p < 0.0001; Integrity index p < 0.0001); Somatic BRAFV600E mutation (Integrity index p = 0.02) | - |
| Klimaite et al. (2022) [43] | prospective | PTC (68) | cfDNA GADPH and β-actin99 concentrations; cfDNA β-actin394/99 integrity index | Tumor size > 2 cm (β-actin99 concentration p < 0.05; Integrity index β-actin394/99 p < 0.05) | - |
| Lan et al. (2020) [45] | retrospective | PTC (36) | cfDNA detection and cfDNA detection of somatic mutations **** | Distant metastasis (cfDNA detection p = 0.04; cfDNA detection of somatic mutations p = 0.015) Tumor size (cfDNA detection p = 0.001; cfDNA detection of somatic mutations p = 0.008) Invasiveness (cfDNA detection p = 0.01) | - |
| Dutta et al. (2021) [69] | prospective | PTC (33), FTC (4) | Total cfDNA concentration ********* | Lymph node metastasis p = 0.005 Lymphovascular invasion p < 0.001 Capsular invasion p < 0.001 Extra-thyroidal extension p < 0.001 pTNM staging p = 0.005 | - |
| Management Settings | N. of Studies (N. of Patients) | Main Evidence |
|---|---|---|
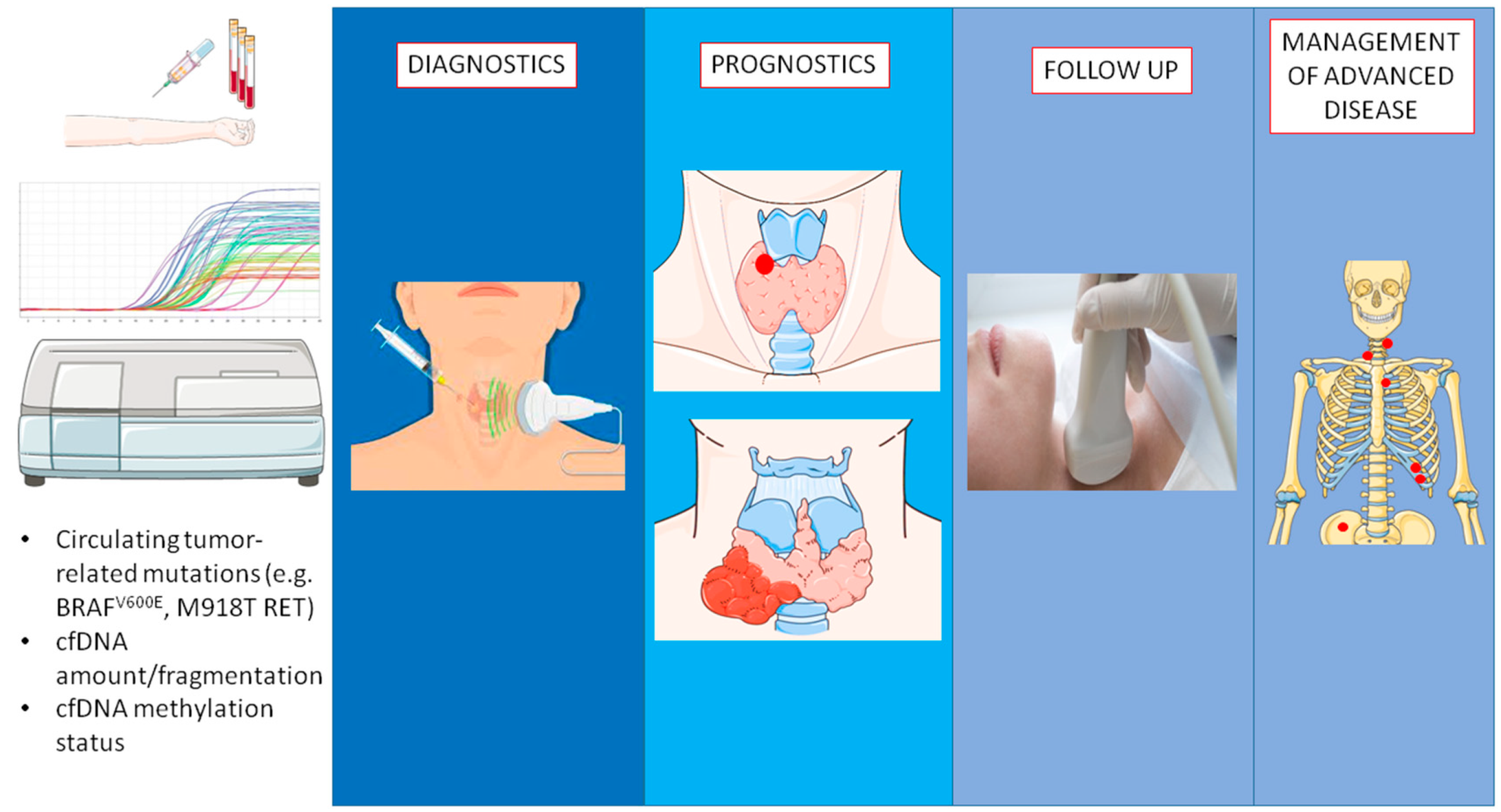
| Diagnostics | 7 (812) | cfBRAFV600E, cfDNA concentration/fragmentation, cfDNA methylation status are useful tools for the presurgical identification of malignant nodules. |
| Prognostics | 11 (632) | Circulating free tumor-related mutations are related to worst outcome/poor clinic-pathological features. |
| Follow-up | 2 (212) | cfBRAFV600E and cfDNA methylation status are useful tools for the detection of disease status during follow-up. |
| Management advanced disease | 1 (51) | cfDNA concentration is a suitable marker of spontaneous and treatment-related morphological slope |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marotta, V.; Cennamo, M.; La Civita, E.; Vitale, M.; Terracciano, D. Cell-Free DNA Analysis within the Challenges of Thyroid Cancer Management. Cancers 2022, 14, 5370. https://doi.org/10.3390/cancers14215370
Marotta V, Cennamo M, La Civita E, Vitale M, Terracciano D. Cell-Free DNA Analysis within the Challenges of Thyroid Cancer Management. Cancers. 2022; 14(21):5370. https://doi.org/10.3390/cancers14215370
Chicago/Turabian StyleMarotta, Vincenzo, Michele Cennamo, Evelina La Civita, Mario Vitale, and Daniela Terracciano. 2022. "Cell-Free DNA Analysis within the Challenges of Thyroid Cancer Management" Cancers 14, no. 21: 5370. https://doi.org/10.3390/cancers14215370
APA StyleMarotta, V., Cennamo, M., La Civita, E., Vitale, M., & Terracciano, D. (2022). Cell-Free DNA Analysis within the Challenges of Thyroid Cancer Management. Cancers, 14(21), 5370. https://doi.org/10.3390/cancers14215370