Simple Summary
Our study estimated the risk of laryngeal and lung cancers according to the industrial classification. Certain industries have been found to be vulnerable to respiratory cancer. In particular, workers employed in the land transportation industries have a high risk of laryngeal cancer. Moreover, workers employed in fishing, mining, transportation, construction, animal production, and healthcare industries have a high risk of lung cancer. As an increased risk of respiratory tract cancers has been identified in certain industries in this study, appropriate policy intervention is needed to prevent occupational cancers.
Abstract
The number of cases and incidence rates of laryngeal and lung cancers have been increasing globally. Therefore, identifying the occupational causes of such cancers is an important concern for policymakers to prevent cancers and deaths. We used national health insurance service claims data in Korea. We included 10,786,000 workers aged between 25 and 64 years. In total, 74,366,928 total person-years of follow-up were included in this study with a mean follow-up of 6.89 years for each person. The standardized incidence ratio (SIR) and 95% confidence intervals (CIs) referenced with the total workers were estimated. For laryngeal cancer, increased SIRs were observed in the land transportation industry among male workers (SIR [95% CI]: 1.65 [1.02–2.53]). For lung cancer, elevated SIRs were observed in the industries including animal production (1.72 [1.03–2.68]), fishing (1.70 [1.05–2.60]), mining (1.69 [1.22–2.27]), travel (1.41 [1.00–1.93]), and transportation (1.22 [1.15–1.30]) among male workers. For female works, healthcare (2.08 [1.04–3.72]) and wholesale (1.88 [1.18–2.85]) industries were associated with a high risk of lung cancer. As an increased risk of respiratory tract cancers has been identified in employees associated with certain industries, appropriate policy intervention is needed to prevent occupational cancers.
1. Introduction
Analyzing risks and preventing respiratory tract cancers have become an important issue worldwide in recent decades. The number of cases and incidence rates of laryngeal and lung cancers has been increasing globally [1]. Globally, approximately 185,000 and 2.2 million patients were newly diagnosed with laryngeal and lung cancers, respectively, and approximately 100,000 and 1.8 million died from them in 2020 [2]. In South Korea, 1222 and 29,960 patients were newly diagnosed with laryngeal and lung cancers in 2019, accounting for 0.5% and 11.8% of the total cancer cases [3]. In particular, lung cancer, which is a leading cause of cancer deaths, imposes a major burden on both individuals and society [4]. Therefore, identifying the causes of respiratory tract cancers is an important concern for clinical physicians, epidemiologists, and policymakers to prevent cancers and deaths.
So far, certain environmental and occupational factors have been reported to contribute to the development of laryngeal and lung cancers. One British study reported that occupational factors accounted for approximately 2.9% and 21.1% of laryngeal and lung cancers in men, respectively, and 1.6% and 5.3% in women, suggesting that occupational exposure has significant importance in the incidence of respiratory tract cancers [5]. According to the International Agency for Research on Cancer (IARC), several occupational and environmental exposures, including asbestos, heavy metals, outdoor air pollution and particulate matter (PM), silica dust, and welding fumes were identified as lung carcinogens. For laryngeal cancer, asbestos and strong inorganic acid mist were identified as carcinogens with sufficient evidence in humans [6]. Meanwhile, not only hazardous substances, but also some industries themselves were associated with respiratory tract cancers. For example, in studies conducted in USA and northern European countries, the rubber production industry was related to an increased risk of laryngeal and lung cancers among workers [7,8].
Despite the importance of exploring possible carcinogens, uncovering the association between occupational exposure and laryngeal and lung cancers has been limited due to the rarity of such cancers. Our study aimed to estimate the risks of laryngeal and lung cancers for each industrial classification using national public health insurance claim data with more than 70 million person-years of follow-up in Korea [9]. The early diagnosis of laryngeal and lung cancers could promote disease intervention and reduce psychological problems and socioeconomic costs. Therefore, assessing the incidence of respiratory tract cancers in workers exposed to occupational risk factors is an important social issue. Therefore, this study aimed to analyze the differences in the incidence of respiratory tract cancers in certain social domains of industrial groups using big data covering workers in Korea. Our results may contribute to developing appropriate polices for cancer prevention by identifying industries and workers at risk of respiratory tract cancers.
2. Materials and Methods
2.1. Study Sample
We used the National Health Insurance Service (NHIS) database for analyzing data from 2009 to 2015. The Korean NHIS claims database contains information on all medical use, procedures, and prescriptions of outpatients and inpatients of nearly the entire population of the nation. The NHIS is a mandatory public health insurance service and covers approximately 98% of the nation’s population comprising more than 50 million residents [10]. The NHIS dataset includes individual demographic variables such as age, sex, type of insurance, and industrial category.
In our closed cohort design, we included 10,786,000 workers aged between 25 and 64 years who were observed in 2009, which was the starting point of this study (Table 1). From 2009 to 2015, 74,366,928 total person-years were included in this study with a mean follow-up of 6.89 years for each person.

Table 1.
Baseline distribution of age group and included number of workers.
2.2. Cancers
Diseases were defined and coded based on the Korean Standard Classification of Diseases, which corresponds to the 10th revision of International Classification of Diseases (ICD-10). Our target diseases were laryngeal cancer (ICD code: C32) and lung cancer (ICD code: C33, C34). The target cancers were classified for inpatients with claims information with larynx cancer (C32) and lung cancer (C33, C34) as their primary diagnosis.
2.3. Industrial Classification
The Korean Standard Industrial Classification (KSIC), which is based on the 4th revision of the International Standard Industrial Classification was used to classify workers’ industrial categories [11]. We first estimated the risk of cancer incidences by industry using the code ‘section’ that classifies the industries into 21 sections (alphabet code), and then using the code ‘group’ that classifies the industries into 232 groups (3-digit code).
2.4. Statistical Analysis
For each cancer, the number of cases and follow-up period (person-year) by sex and age groups were calculated. The age-standardized incidence ratio (SIR) and its 95% confidence intervals (CIs) referenced with the total workers were estimated. Age standardization was performed by 5-year unit of age from 25 to 64 years. To calculate SIRs, the number of observed cases was divided by the expected number of cases for each industrial classification, and the CIs were estimated using the Poisson distribution. SIR was calculated for industrial sections or groups with more than 5 cancer cases. Significance was set at p < 0.05. All statistical analyses and visualization were performed using the SAS, version 9.4 (SAS Institute, Cary, NC, USA) and R software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria).
2.5. Ethics Statement
The NHIS dataset was anonymized before the release of the NHIS dataset to the authors. The Institutional Review Board of the Yonsei Health System reviewed and approved the study (IRB number: Y-2017-0100).
3. Results
Out of the total 10,786,000 included workers, 1150 and 15,013 workers were newly diagnosed with laryngeal and lung cancers, respectively. Laryngeal cancer was recorded in 1123 male workers and 27 female workers. Meanwhile, lung cancer was recorded in 12,270 male workers and 2743 female workers. In both laryngeal and lung cancers, the incidence rate increased as the age of workers increased (Table 2).
Table 2.
Follow-up period and number of incidence cancer cases according to sex and age group.
Figure 1 presents the SIRs of laryngeal cancer compared to the whole workers in each industrial section. Industrial section ‘E. Water supply; sewage, waste management, materials recovery’ and ‘U. Activities of extraterritorial organizations and bodies’ were omitted due to the lack of incidence in these sections. Sex stratification was performed only for male workers because of the low incidence of laryngeal cancer among female workers. Only ‘H. Transportation and storage’ section (SIR [95% CI]: 1.19 [1.00–1.42]) was marginally associated with laryngeal cancer.
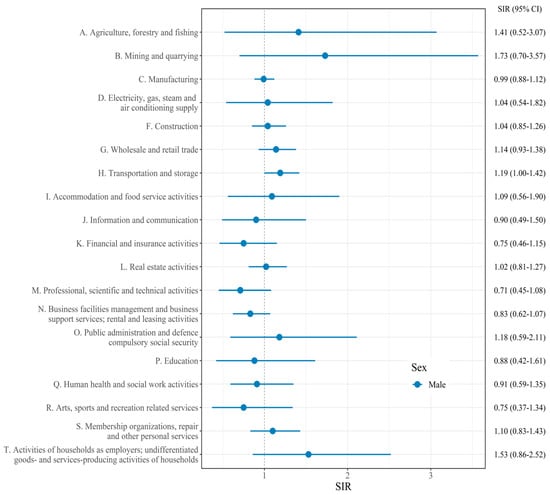
Figure 1.
Standardized incidence ratio (SIR) and confidence intervals (CIs) of laryngeal cancer for each industry section.
Figure 2 depicts the SIRs of lung cancer compared to all workers in each industrial section. Among male workers, significantly increased SIRs were observed in the ‘A. Agriculture, forestry, and fishing’ (SIR [95% CI]: 1.50 [1.17–1.90]), ‘B. Mining and quarrying’ (SIR [95% CI]: 1.44 [1.11–1.85]), ‘F. Construction’ (SIR [95% CI]: 1.07 [1.01–1.13]), ‘H. Transportation and storage’ (SIR [95% CI]: 1.17 [1.11–1.24]), ‘N. Business facilities management and business support services; rental and leasing activities’ (SIR [95% CI]: 1.09 [1.02–1.17]), and ‘O. Public administration and defense; compulsory social security’ sections (SIR [95% CI]: 1.21 [1.00–1.45]). Among female workers, the ‘G. Wholesale and retail trade’ (SIR [95% CI]: 1.13 [1.00–1.26]) section was associated with a high risk of lung cancer.
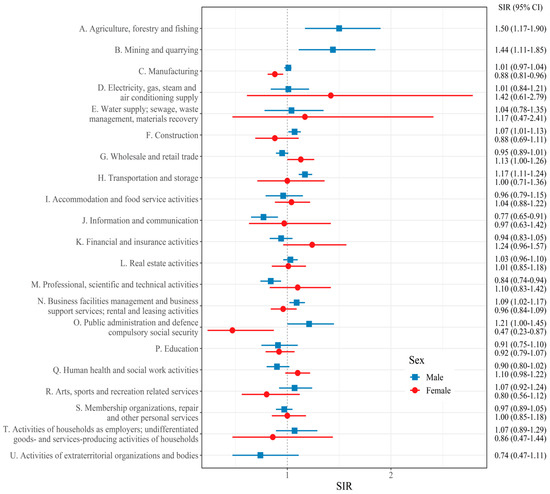
Figure 2.
Standardized incidence ratio (SIR) and confidence intervals (CIs) of lung cancer for each industry section.
Table 3 presents the industrial group with a significantly higher risk of laryngeal cancer among male workers. Significantly increased SIR was observed in the ‘passenger land transport, except transport via railways’ (SIR [95% CI]: 1.65 [1.02–2.53]) group. SIRs of laryngeal cancer for other industries are shown in Table S1.
Table 3.
Industry groups with a significantly higher risk of laryngeal cancer.
Table 4 presents the industrial groups with a significantly higher risk of lung cancer. Among male workers, significantly increased SIRs were observed in the ‘animal production’ (SIR [95% CI]: 1.72 [1.03–2.68]), ‘fishing’ (SIR [95% CI]: 1.70 [1.05–2.60]), ‘mining of coal and lignite’ (SIR [95% CI]: 1.69 [1.22–2.27]), ‘activities of travel agencies and tour operators and tourist assistance activities’ (SIR [95% CI]: 1.41 [1.00–1.93]), ‘cleaning and pest control services of building and industrial facilities’ (SIR [95% CI]: 1.23 [1.04–1.46]), ‘support activities for transportation’ (SIR [95% CI]: 1.22 [1.15–1.30]), ‘Heavy and civil engineering construction’ (SIR [95% CI]: 1.17 [1.05–1.31]), and ‘real estate activities on a fee or contract basis’ (SIR [95% CI]: 1.11 [1.01–1.23]).
Table 4.
Industry groups with a significantly higher risk of lung cancer.
Among female workers, significantly increased SIRs were observed in the ‘other human health activities’ (SIR [95% CI]: 2.08 [1.04–3.72]), ‘wholesale of machinery, equipment, and supplies’ (SIR [95% CI]: 1.88 [1.18–2.85]), and ‘hospital activities’ (SIR [95% CI]: 1.29 [1.01–1.63]). SIRs of lung cancer for other industries are shown in Table S2.
4. Discussion
This study aimed to investigate the risks of laryngeal and lung cancers for each industrial classification. The results revealed a diverse cancer incidence across industries. When referenced with total workers, employees in the land transportation industry were associated with a risk of laryngeal cancer. In the case of lung cancer, workers in animal production, fishing, mining, travel activities, transportation, construction, real estate activities, wholesale, and healthcare industries were associated with lung cancer.
Overall, both laryngeal and lung cancer incidence rates increased with age. This result is in line with previous epidemiological studies [3,12]. The high incidence of cancer in the elderly can be attributable to the effect of chronic conditions or accumulated years of risky health behaviors such as smoking and alcohol drinking [13]. In addition, workers were more likely to be exposed to occupational carcinogens such as asbestos in past working conditions [14].
4.1. Laryngeal Cancer
Previous research has revealed an increased risk of laryngeal cancer among workers in several industrial sectors, including the automobile, railroad, lumber, food, and rubber industries [7,15,16]. Additionally, blue-collar workers (production workers, transport equipment operators, and laborers) were reportedly at a higher risk of laryngeal cancer, while white-collar workers were reportedly at a lower risk of laryngeal cancer according to a previous meta-analysis [17]. Overall, our results are consistent with previous findings that workers in the transportation industries have an increased risk of laryngeal cancer [18].
For workers in the transportation industry, occupational exposure to engine exhaust and ambient air pollution might contribute to an increased risk of laryngeal cancer. Previous studies investigated whether occupational exposure to diesel and gasoline exhaust can induce laryngeal cancer. For instance, a Canadian study has identified an elevated relative risk (RR) of laryngeal cancer (RR [95% CI]: 1.59 [1.08–2.33]) [19]. According to a Turkish case–control study, increased odds ratios (ORs) of laryngeal cancer was observed for occupational exposure to both diesel exhaust (OR [95% CI]: 1.5 [1.3–1.9]) and gasoline exhaust (OR [95% CI]: 1.6 [1.3–2.0] [20]. A previous study that estimated meta-RR revealed that the presence of engine exhaust is significantly associated with laryngeal cancer [21]. Additionally, few studies have suggested an association between air pollutants and PM and laryngeal cancer. Air pollutants such as PM10, PM2.5, and NO2 are related to increased risks of laryngeal cancer [22,23,24]. In line with prior findings, we revealed that workers in the land transport industry (e.g., bus drivers and taxi drivers) are at risk of laryngeal cancer.
4.2. Lung Cancer
Previous research has revealed that workers in various industries including the rubber manufacturing, petroleum, iron/steel foundry, and nuclear industries were at risk of lung cancer [8,25,26]. In our study, an increased risk of lung cancer was also associated with employees working in a wider variety of industries compared with laryngeal cancer.
Industries that may be exposed to occupational dust such as crystalline silica and asbestos include the mining and construction industries. Thus, our findings support the results of previous studies that reported an association between these industries and lung cancer [27,28]. In addition to occupational dust, these workers are highly likely to be exposed to carcinogens such as radon gas, polycyclic aromatic hydrocarbons (PAHs), and welding fumes.
In the case of the transportation industry, significantly increased SIR was observed for lung cancer. Our results are consistent with the results of recent previous studies that revealed a significant relationship between transportation and lung cancer risk [29,30]. Respiratory carcinogens, such as diesel/gasoline engine exhaust, air pollution, and PM, have been reported as factors that may expose workers in the transportation industry. The increased risk of lung cancer among travel assistance activities could be also attributable to characteristics similar to those in the transportation industry. Workers in the travel agency industry often participate in providing transportation services for tourists [31], and because of this similarity, this industry was included in the transportation industry before the recent KSIC revision.
Several recent studies have reported the relationship between the fishing industry and lung cancer. For instance, a Norwegian epidemiological study observed a high risk of lung cancer among seafarers and fishermen [32], and a Japanese study reported a high risk of lung cancer among workers in the fishing industry [33]. Carcinogens such as diesel engine exhaust, PAHs, and benzene that can be present in ships have also been considered the cause of the high lung cancer incidence among workers in the fishing industry [34].
In our study, the high lung cancer risk was observed among male workers employed in the animal production industry group, which contradicts previous reports that state that farm animal exposure reduces the risk of lung cancer [35]. Moreover, it should be considered that confounding variables such as smoking were not adjusted in this study. Nevertheless, a study has reported that occupational exposure to animal contact or organic dust of animal origin increases the risk of lung cancer [36]. Moreover, our findings were in line with previous studies that showed that workers in the agriculture industry were related to a high risk of lung cancer [37,38]. Occupational exposure to pesticides has been pointed out as the main causes of high lung cancer incidences among agriculture workers [37,39].
A previous case–control study revealed that professional cleaning activities were associated with high risk of lung cancer among female workers [40]. Workers in the ‘cleaning and pest control services’ industry could be exposed to pesticides and cleaning agents, which were carcinogen to lung cancer [41,42]. Workers in the real estate activities industry were reported to have a high risk of lung cancer mortality in preceding studies [30,43]. On the other hand, another study reported a protective effect of this industry on lung cancer [44]. It is unclear whether workers in the real estate activities industry are exposed to occupational carcinogens, so caution is needed in interpretation of these results.
In the case of lung cancer among female workers, our findings support previous studies that revealed a high risk of lung cancer among workers in the healthcare industry [43,45]. Occupational exposure to ionizing radiation or night shifts might be possible explanations [46,47]. Moreover, our findings support that of a previous study that revealed an increased risk in lung cancer mortality among female workers in the wholesale sector, possibly due to the exposure of dust containing silica from the machines or diesel exhausts in the storage warehouse [43].
An insignificantly increased risk was observed in workers in the petroleum, steel manufacturing, and metal foundry industries, which had been reported to be related to lung cancer in previous studies. These results should be considered along with the relatively short follow-up period of this study and the changes in the working environment over the decades.
4.3. Limitations
Although our study was based on a large sample size from the NHIS dataset, the findings should be interpreted with caution due to the following limitations. First, we did not adjust for important confounding factors such as smoking and drinking due to lack of information. Nevertheless, a recent study by Jung et al. that analyzed the smoking status of Korean workers provides a glimpse into the confounding effect of smoking on the association between respiratory tract cancer and industrial groups [48]. According to the study, in male workers, the prevalence of smoking was higher among the workers in the fishing, mining, and construction industries than that of overall male workers. On the other hand, the smoking prevalence of the workers in the industries of animal production, travel agencies, cleaning and pest control services, and real estate activities did not differ notably from that of overall workers. Moreover, in the case of women, a lower prevalence of smoking was observed in healthcare workers compared to overall female workers. Furthermore, alcohol beverages are classified as a carcinogenic agent with sufficient evidence in humans (IARC group 1) for laryngeal cancer [49]. Therefore, drinking habit can act as a strong confounding factor, especially for laryngeal cancer. In addition, environmental factors including residential areas, outdoor particulate matter exposures, and second-hand tobacco smoking, and individual respiratory disease history can have a confounding effect on the relationship between respiratory tract cancer incidences and industrial groups. Nevertheless, the purpose of the current study was to identify vulnerable industries that may need intervention and to provide information that can help policymakers implement occupational safety and health policies. Further in-depth studies are needed to confirm whether the risk of laryngeal and lung cancers is independent of the confounding factors. Second, we could not consider which industry the workers were engaged in before 2009. Additionally, the trend of the risk according to the period of employment in the industry could not be estimated. Third, our study only presented risks according to the industrial classification, and specific occupational carcinogens could not be specified. Further studies with exposure data are needed, and an alternative job exposure matrix using industrial classification should be used to clarify the association between cancer incidence and industrial classification. Fourth, it should also be considered that, even in the same industry, the risk of cancer incidence changes with the times due to changes in working environments [8].
5. Conclusions
Our study estimated the risk of laryngeal and lung cancers according to the industrial classification and suggested the at-risk industries. Certain industries have been revealed as vulnerable social domains for respiratory tract cancers. In particular, workers employed in the transportation have a high risk of both laryngeal and lung cancers. Despite the recent developments of occupational environments, an increased risk of respiratory tract cancers has been identified in certain industries in this study. Therefore, appropriate policy intervention is needed to prevent occupational cancers.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers14215219/s1, Table S1: Standardized incidence ratio (SIR) and confidence intervals (CIs) of laryngeal cancer for each industry group; Table S2: Standardized incidence ratio (SIR) and confidence intervals (CIs) of lung cancer for each industry group.
Author Contributions
Conceptualization, S.-U.B., W.L. and J.-H.Y.; methodology, W.-R.L., K.-B.Y.; formal analysis, W.-R.L., K.-B.Y.; investigation, S.-U.B.; data curation, J.-H.C., K.-E.L., W.L. and J.-H.Y.; writing—original draft preparation, S.-U.B.; writing—review and editing, S.-U.B., W.L. and J.-H.Y.; visualization, S.-U.B.; supervision, W.L. and J.-H.Y.; project administration, J.-H.C., K.-E.L., W.L. and J.-H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Occupational Safety and Health Research Institute through the “Establishment and Utilization of Standards Control Groups of Worker—Development of Health Risk Screening Program”. The funder had no role in either the direction or methodology of the study.
Institutional Review Board Statement
The data used in this study were anonymized before their release from the NHIS. The Institutional Review Board (IRB) of Yonsei University Health System approved the study design (IRB number: Y-2017-0100).
Informed Consent Statement
Patient consent was waived by the IRB.
Data Availability Statement
The data are not publicly available.
Acknowledgments
We acknowledge the government authorities of the Department of Big Data Steering, National Health Insurance Service. We thank all the scientists working in the National Health Insurance Service who collected and handled the information from medical claims data of the National Health Insurance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- GBD 2019 Respiratory Tract Cancers Collaborators. Global, regional, and national burden of respiratory tract cancers and associated risk factors from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Respir. Med. 2021, 9, 1030–1049. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Won, Y.J.; Lee, J.J.; Jung, K.W.; Kim, H.J.; Kong, H.J.; Im, J.S.; Seo, H.G.; The Community of Population-Based Regional Cancer Registries. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2019. Cancer Res. Treat. 2022, 54, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Cancer Collaboration. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef] [PubMed]
- Rushton, L.; Bagga, S.; Bevan, R.; Brown, T.P.; Cherrie, J.W.; Holmes, P.; Fortunato, L.; Slack, R.; Van Tongeren, M.; Young, C.; et al. Occupation and cancer in Britain. Br. J. Cancer 2010, 102, 1428–1437. [Google Scholar] [CrossRef]
- Loomis, D.; Guha, N.; Hall, A.L.; Straif, K. Identifying occupational carcinogens: An update from the IARC Monographs. Occup. Environ. Med. 2018, 75, 593–603. [Google Scholar] [CrossRef]
- Kogevinas, M.; Sala, M.; Boffetta, P.; Kazerouni, N.; Kromhout, H.; Hoar-Zahm, S. Cancer risk in the rubber industry: A review of the recent epidemiological evidence. Occup. Environ. Med. 1998, 55, 1–12. [Google Scholar] [CrossRef]
- Boniol, M.; Koechlin, A.; Boyle, P. Meta-analysis of occupational exposures in the rubber manufacturing industry and risk of cancer. Int. J. Epidemiol. 2017, 46, 1940–1947. [Google Scholar] [CrossRef]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef]
- Shin, D.W.; Cho, B.; Guallar, E. Korean national health insurance database. JAMA Intern. Med. 2016, 176, 138. [Google Scholar] [CrossRef]
- Statistics Korea. Korean Standard Industrial Classfication. Available online: https://kssc.kostat.go.kr:8443/ksscNew_web/ekssc/main/main.do# (accessed on 30 August 2022).
- de la Cour, C.D.; Munk, C.; Aalborg, G.L.; Kjaer, S.K. Base of tongue/tonsillar and laryngeal cancer in Denmark 1994-2018: Temporal trends in incidence according to education and age. Oral. Oncol. 2022, 128, 105832. [Google Scholar] [CrossRef]
- White, M.C.; Holman, D.M.; Boehm, J.E.; Peipins, L.A.; Grossman, M.; Henley, S.J. Age and cancer risk: A potentially modifiable relationship. Am. J. Prev. Med. 2014, 46, S7–S15. [Google Scholar] [CrossRef]
- Kim, H.R. Overview of asbestos issues in Korea. J. Korean Med. Sci. 2009, 24, 363–367. [Google Scholar] [CrossRef]
- Flanders, W.D.; Rothman, K.J. Occupational risk for laryngeal cancer. Am. J. Public Health 1982, 72, 369–372. [Google Scholar] [CrossRef]
- Laakkonen, A.; Kauppinen, T.; Pukkala, E. Cancer risk among Finnish food industry workers. Int. J. Cancer 2006, 118, 2567–2571. [Google Scholar] [CrossRef]
- Bayer, O.; Camara, R.; Zeissig, S.R.; Ressing, M.; Dietz, A.; Locati, L.D.; Ramroth, H.; Singer, S. Occupation and cancer of the larynx: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2016, 273, 9–20. [Google Scholar] [CrossRef]
- Elci, O.C.; Dosemeci, M.; Blair, A. Occupation and the risk of laryngeal cancer in Turkey. Scand. J. Work Environ. Health 2001, 27, 233–239. [Google Scholar] [CrossRef]
- Aronson, K.J.; Howe, G.R.; Carpenter, M.; Fair, M.E. Surveillance of potential associations between occupations and causes of death in Canada, 1965–1991. Occup. Environ. Med. 1999, 56, 265–269. [Google Scholar] [CrossRef]
- Elci, O.C.; Akpinar-Elci, M.; Blair, A.; Dosemeci, M. Risk of laryngeal cancer by occupational chemical exposure in Turkey. J. Occup. Environ. Med. 2003, 45, 1100–1106. [Google Scholar] [CrossRef]
- Paget-Bailly, S.; Cyr, D.; Luce, D. Occupational exposures and cancer of the larynx-systematic review and meta-analysis. J. Occup. Environ. Med. 2012, 54, 71–84. [Google Scholar] [CrossRef]
- Kim, H.B.; Shim, J.Y.; Park, B.; Lee, Y.J. Long-Term Exposure to Air Pollutants and Cancer Mortality: A Meta-Analysis of Cohort Studies. Int. J. Environ. Res. Public Health 2018, 15, 2608. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Xu, R.; Li, S.; Coelho, M.; Saldiva, P.H.N.; Sim, M.R.; Abramson, M.J.; Guo, Y. Associations between long-term exposure to PM2.5 and site-specific cancer mortality: A nationwide study in Brazil between 2010 and 2018. Environ. Pollut. 2022, 302, 119070. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Deng, W.; Liu, Y.; Zhao, W.; Liu, J.; Cao, Y.; Deng, J. Association between ambient air pollution and laryngeal neoplasms incidence in twelve major Chinese cities, 2006–2013. Environ. Sci. Pollut. Res. Int. 2020, 27, 39274–39282. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Kamal, R.; Ahamed, I.; Wagh, M.; Bihari, V.; Sathian, B.; Kesavachandran, C.N. PAH exposure-associated lung cancer: An updated meta-analysis. Occup. Med. 2018, 68, 255–261. [Google Scholar] [CrossRef]
- Cardis, E.; Vrijheid, M.; Blettner, M.; Gilbert, E.; Hakama, M.; Hill, C.; Howe, G.; Kaldor, J.; Muirhead, C.R.; Schubauer-Berigan, M.; et al. The 15-Country Collaborative Study of Cancer Risk among Radiation Workers in the Nuclear Industry: Estimates of radiation-related cancer risks. Radiat. Res. 2007, 167, 396–416. [Google Scholar] [CrossRef]
- Hancock, D.G.; Langley, M.E.; Chia, K.L.; Woodman, R.J.; Shanahan, E.M. Wood dust exposure and lung cancer risk: A meta-analysis. Occup. Environ. Med. 2015, 72, 889–898. [Google Scholar] [CrossRef]
- Li, L.; Jiang, M.; Li, X.; Zhou, B. Association between Coalmine Dust and Mortality Risk of Lung Cancer: A Meta-Analysis. Biomed. Res. Int. 2021, 2021, 6624799. [Google Scholar] [CrossRef]
- Lee, W.; Kang, M.Y.; Kim, J.; Lim, S.S.; Yoon, J.H. Cancer risk in road transportation workers: A national representative cohort study with 600,000 person-years of follow-up. Sci. Rep. 2020, 10, 11331. [Google Scholar] [CrossRef]
- Jung, J.K.H.; Feinstein, S.G.; Palma Lazgare, L.; Macleod, J.S.; Arrandale, V.H.; McLeod, C.B.; Peter, A.; Demers, P.A. Examining lung cancer risks across different industries and occupations in Ontario, Canada: The establishment of the Occupational Disease Surveillance System. Occup. Environ. Med. 2018, 75, 545–552. [Google Scholar] [CrossRef]
- Prideaux, B. The role of the transport system in destination development. Tour. Manag. 2000, 21, 53–63. [Google Scholar] [CrossRef]
- Ugelvig Petersen, K.; Pukkala, E.; Martinsen, J.I.; Lynge, E.; Tryggvadottir, L.; Weiderpass, E.; Kjaerheim, K.; Heikkinen, S.; Hansen, J. Cancer incidence among seafarers and fishermen in the Nordic countries. Scand. J. Work Environ. Health 2020, 46, 461–468. [Google Scholar] [CrossRef]
- Eguchi, H.; Wada, K.; Prieto-Merino, D.; Smith, D.R. Lung, gastric and colorectal cancer mortality by occupation and industry among working-aged men in Japan. Sci. Rep. 2017, 7, 43204. [Google Scholar] [CrossRef]
- Oldenburg, M.; Baur, X.; Schlaich, C. Occupational risks and challenges of seafaring. J. Occup. Health 2010, 52, 249–256. [Google Scholar] [CrossRef]
- Tual, S.; Lemarchand, C.; Boulanger, M.; Dalphin, J.C.; Rachet, B.; Marcotullio, E.; Velten, M.; Guizard, A.V.; Clin, B.; Baldi, I.; et al. Exposure to Farm Animals and Risk of Lung Cancer in the AGRICAN Cohort. Am. J. Epidemiol. 2017, 186, 463–472. [Google Scholar] [CrossRef]
- Peters, S.; Kromhout, H.; Olsson, A.C.; Wichmann, H.E.; Bruske, I.; Consonni, D.; Landi, M.T.; Caporaso, N.; Siemiatycki, J.; Richiardi, L.; et al. Occupational exposure to organic dust increases lung cancer risk in the general population. Thorax 2012, 67, 111–116. [Google Scholar] [CrossRef]
- Boulanger, M.; Tual, S.; Lemarchand, C.; Guizard, A.V.; Delafosse, P.; Marcotullio, E.; Pons, R.; Piel, C.; Pouchieu, C.; Baldi, I.; et al. Lung cancer risk and occupational exposures in crop farming: Results from the AGRIculture and CANcer (AGRICAN) cohort. Occup. Environ. Med. 2018, 75, 776–785. [Google Scholar] [CrossRef]
- Suraya, A.; Nowak, D.; Sulistomo, A.W.; Icksan, A.G.; Berger, U.; Syahruddin, E.; Bose-O’Reilly, S. Excess Risk of Lung Cancer Among Agriculture and Construction Workers in Indonesia. Ann. Glob. Health 2021, 87, 8. [Google Scholar] [CrossRef]
- Kim, B.; Park, E.Y.; Kim, J.; Park, E.; Oh, J.K.; Lim, M.K. Occupational Exposure to Pesticides and Lung Cancer Risk: A Propensity Score Analyses. Cancer Res. Treat. 2022, 54, 130–139. [Google Scholar] [CrossRef]
- Atramont, A.; Guida, F.; Mattei, F.; Matrat, M.; Cenee, S.; Sanchez, M.; Carton, M.; Menvielle, G.; Marrer, E.; Neri, M.; et al. Professional Cleaning Activities and Lung Cancer Risk Among Women: Results From the ICARE Study. J. Occup. Environ. Med. 2016, 58, 610–616. [Google Scholar] [CrossRef]
- Van den Borre, L.; Deboosere, P. Health risks in the cleaning industry: A Belgian census-linked mortality study (1991–2011). Int. Arch. Occup. Environ. Health 2018, 91, 13–21. [Google Scholar] [CrossRef]
- Bonner, M.R.; Freeman, L.E.; Hoppin, J.A.; Koutros, S.; Sandler, D.P.; Lynch, C.F.; Hines, C.J.; Thomas, K.; Blair, A.; Alavanja, M.C. Occupational Exposure to Pesticides and the Incidence of Lung Cancer in the Agricultural Health Study. Environ. Health Perspect. 2017, 125, 544–551. [Google Scholar] [CrossRef]
- Robinson, C.F.; Sullivan, P.A.; Li, J.; Walker, J.T. Occupational lung cancer in US women, 1984-1998. Am. J. Ind. Med. 2011, 54, 102–117. [Google Scholar] [CrossRef]
- Tse, L.A.; Yu, I.T.; Qiu, H.; Au, J.S.; Wang, X.R. Occupational risks and lung cancer burden for Chinese men: A population-based case-referent study. Cancer Causes Control. 2012, 23, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Corbin, M.; McLean, D.; Mannetje, A.; Dryson, E.; Walls, C.; McKenzie, F.; Maule, M.; Cheng, S.; Cunningham, C.; Kromhout, H.; et al. Lung cancer and occupation: A New Zealand cancer registry-based case-control study. Am. J. Ind. Med. 2011, 54, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Lie, J.A.; Kjaerheim, K.; Tynes, T. Ionizing radiation exposure and cancer risk among Norwegian nurses. Eur. J. Cancer Prev. 2008, 17, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Schernhammer, E.S.; Feskanich, D.; Liang, G.; Han, J. Rotating night-shift work and lung cancer risk among female nurses in the United States. Am. J. Epidemiol. 2013, 178, 1434–1441. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Koh, D.H.; Choi, S.; Park, J.H.; Kim, H.C.; Lee, S.G.; Park, D. Estimates of the Prevalence, Intensity and the Number of Workers Exposed to Cigarette Smoking across Occupations and Industries in Korea. J. Korean Med. Sci. 2019, 34, e213. [Google Scholar] [CrossRef]
- Roswall, N.; Weiderpass, E. Alcohol as a risk factor for cancer: Existing evidence in a global perspective. J. Prev. Med. Public Health 2015, 48, 1–9. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).