
A Systematic Review on the Impact of Hypofractionated and Stereotactic Radiotherapy on Immune Cell Subpopulations in Cancer Patients


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
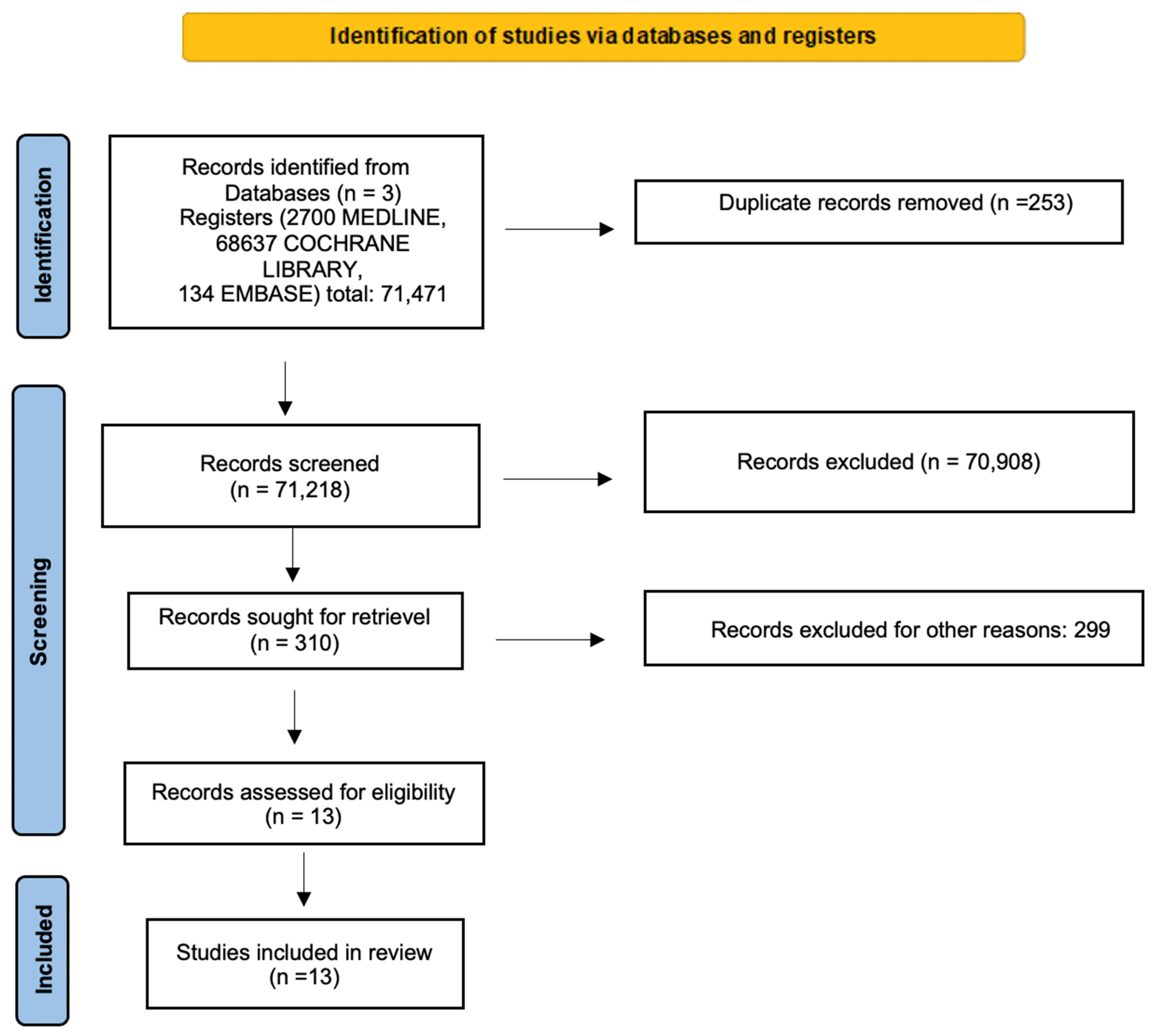
2.1. Search Strategy
2.2. Study Selection and Data Extraction
2.3. Inclusion and Exclusion Criteria
3. Results
3.1. Current Published Evidences of Changes in Lymphocyte Subsets after HFRT
3.2. Current Published Evidence of Changes in Lymphocyte Subsets after SBRT
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Martin, A.; Gaya, A. Stereotactic body radiotherapy: A review. Clin. Oncol. 2010, 22, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Systemic effects of local radiotherapy. Lancet Oncol. 2009, 10, 718–726. [Google Scholar] [CrossRef]
- Menetrier-Caux, C.; Ray-Coquard, I.; Blay, J.Y.; Caux, C. Lymphopenia in Cancer Patients and its Effects on Response to Immunotherapy: An opportunity for combination with Cytokines? J. Immunother. Cancer 2019, 7, 85. [Google Scholar] [CrossRef] [PubMed]
- Manuel, M.; Tredan, O.; Bachelot, T.; Clapisson, G.; Courtier, A.; Parmentier, G.; Rabeony, T.; Grives, A.; Perez, S.; Mouret, J.F.; et al. Lymphopenia combined with low TCR diversity (divpenia) predicts poor overall survival in metastatic breast cancer patients. Oncoimmunology 2012, 1, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Liao, Z.; Gomez, D.; Levy, L.; Zhuang, Y.; Gebremichael, R.A.; Hong, D.S.; Komaki, R.; Welsh, J.W. Lymphopenia association with gross tumor volume and lung V5 and its effects on non-small cell lung cancer patient outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Wild, A.T.; Herman, J.M.; Dholakia, A.S.; Moningi, S.; Lu, Y.; Rosati, L.M.; Hacker-Prietz, A.; Assadi, R.K.; Saeed, A.M.; Pawlik, T.M.; et al. Lymphocyte-Sparing Effect of Stereotactic Body Radiation Therapy in Patients With Unresectable Pancreatic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Patel, R.R.; Verma, V.; Ramapriyan, R.; Barsoumian, H.B.; Cortez, M.A.; Welsh, J.W. Interaction between lymphopenia, radiotherapy technique, dosimetry, and survival outcomes in lung cancer patients receiving combined immunotherapy and radiotherapy. Radiother. Oncol. 2020, 150, 114–120. [Google Scholar] [CrossRef]
- Mellman, I.; Coukos, G.; Dranoff, G. Cancer immunotherapy comes of age. Nature 2011, 480, 480–489. [Google Scholar] [CrossRef]
- Mirjolet, C.; Charon-Barra, C.; Ladoire, S.; Arbez-Gindre, F.; Bertaut, A.; Ghiringhelli, F.; Leroux, A.; Peiffert, D.; Borg, C.; Bosset, J.F.; et al. Tumor lymphocyte immune response to preoperative radiotherapy in locally advanced rectal cancer: The LYMPHOREC study. Oncoimmunology 2018, 7, e1396402. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Wang, Q. Comparative analysis of the effect of different radiotherapy regimes on lymphocyte and its subpopulations in breast cancer patients. Clin. Transl. Oncol. 2018, 20, 1219–1225. [Google Scholar] [CrossRef]
- Linares-Galiana, I.; Berenguer-Frances, M.A.; Canas-Cortes, R.; Pujol-Canadell, M.; Comas-Anton, S.; Martinez, E.; Laplana, M.; Perez-Montero, H.; Pla-Farnos, M.J.; Navarro-Martin, A.; et al. Changes in peripheral immune cells after intraoperative radiation therapy in low-risk breast cancer. J. Radiat. Res. 2021, 62, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Maehata, Y.; Onishi, H.; Kuriyama, K.; Aoki, S.; Araya, M.; Saito, R.; Tominaga, L.; Oguri, M.; Araki, T. Immune responses following stereotactic body radiotherapy for stage I primary lung cancer. Biomed. Res. Int. 2013, 2013, 731346. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Yu, H.; Ni, C.; Zhang, T.; Liu, L.; Lv, Q.; Zhang, Z.; Wang, Z.; Wu, D.; Wu, P.; et al. Hypofractionated stereotactic radiation therapy activates the peripheral immune response in operable stage I non-small-cell lung cancer. Sci. Rep. 2017, 7, 4866. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, J.; Slebioda, T.; Kmiec, Z.; Zaucha, R. Changes in systemic immune response after stereotactic ablative radiotherapy. Preliminary results of a prospective study in patients with early lung cancer. Pol. Arch. Intern. Med. 2017, 127, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Martin, A.; Galiana, I.L.; Berenguer Frances, M.A.; Cacicedo, J.; Canas Cortes, R.; Comas Anton, S.; Padrones Sanchez, S.; Bolivar Cuevas, S.; Parry, R.; Guedea Edo, F. Preliminary Study of the Effect of Stereotactic Body Radiotherapy (SBRT) on the Immune System in Lung Cancer Patients Unfit for Surgery: Immunophenotyping Analysis. Int. J. Mol. Sci. 2018, 19, 3963. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, M.P.; Bornschlegl, S.; Park, S.S.; Gastineau, D.A.; Roberts, L.R.; Dietz, A.B.; Hallemeier, C.L. Comprehensive assessment of circulating immune cell populations in response to stereotactic body radiation therapy in patients with liver cancer. Adv. Radiat. Oncol. 2017, 2, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Yuan, B.Y.; Chen, G.W.; Zhao, X.M.; Hu, Y.; Zhu, W.C.; Zeng, Z.C.; Chen, Y.X. Association Between Circulating Lymphocyte Populations and Outcome After Stereotactic Body Radiation Therapy in Patients with Hepatocellular Carcinoma. Front. Oncol. 2019, 9, 896. [Google Scholar] [CrossRef]
- Kane, N.; Romero, T.; Diaz-Perez, S.; Rettig, M.B.; Steinberg, M.L.; Kishan, A.U.; Schaue, D.; Reiter, R.E.; Knudsen, B.S.; Nickols, N.G. Significant changes in macrophage and CD8 T cell densities in primary prostate tumors 2 weeks after SBRT. Prostate Cancer Prostatic Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- McGee, H.M.; Daly, M.E.; Azghadi, S.; Stewart, S.L.; Oesterich, L.; Schlom, J.; Donahue, R.; Schoenfeld, J.D.; Chen, Q.; Rao, S.; et al. Stereotactic Ablative Radiation Therapy Induces Systemic Differences in Peripheral Blood Immunophenotype Dependent on Irradiated Site. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 1259–1270. [Google Scholar] [CrossRef]
- Crocenzi, T.; Cottam, B.; Newell, P.; Wolf, R.F.; Hansen, P.D.; Hammill, C.; Solhjem, M.C.; To, Y.Y.; Greathouse, A.; Tormoen, G.; et al. A hypofractionated radiation regimen avoids the lymphopenia associated with neoadjuvant chemoradiation therapy of borderline resectable and locally advanced pancreatic adenocarcinoma. J. Immunother. Cancer 2016, 4, 45. [Google Scholar] [CrossRef]
- Formenti, S.C.; Rudqvist, N.P.; Golden, E.; Cooper, B.; Wennerberg, E.; Lhuillier, C.; Vanpouille-Box, C.; Friedman, K.; Ferrari de Andrade, L.; Wucherpfennig, K.W.; et al. Radiotherapy induces responses of lung cancer to CTLA-4 blockade. Nat. Med. 2018, 24, 1845–1851. [Google Scholar] [CrossRef] [PubMed]
- Venkatesulu, B.P.; Mallick, S.; Lin, S.H.; Krishnan, S. A systematic review of the influence of radiation-induced lymphopenia on survival outcomes in solid tumors. Crit. Rev. Oncol. Hematol. 2018, 123, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Cropet, C.; Van Glabbeke, M.; Sebban, C.; Le Cesne, A.; Judson, I.; Tredan, O.; Verweij, J.; Biron, P.; Labidi, I.; et al. Lymphopenia as a prognostic factor for overall survival in advanced carcinomas, sarcomas, and lymphomas. Cancer Res. 2009, 69, 5383–5391. [Google Scholar] [CrossRef] [PubMed]
- Weichselbaum, R.R.; Liang, H.; Deng, L.; Fu, Y.X. Radiotherapy and immunotherapy: A beneficial liaison? Nat. Rev. Clin. Oncol. 2017, 14, 365–379. [Google Scholar] [CrossRef] [PubMed]
- Chandra, R.A.; Wilhite, T.J.; Balboni, T.A.; Alexander, B.M.; Spektor, A.; Ott, P.A.; Ng, A.K.; Hodi, F.S.; Schoenfeld, J.D. A systematic evaluation of abscopal responses following radiotherapy in patients with metastatic melanoma treated with ipilimumab. Oncoimmunology 2015, 4, e1046028. [Google Scholar] [CrossRef] [PubMed]
- Mole, R.H. Whole body irradiation; radiobiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef]
- Gupta, A.; Probst, H.C.; Vuong, V.; Landshammer, A.; Muth, S.; Yagita, H.; Schwendener, R.; Pruschy, M.; Knuth, A.; van den Broek, M. Radiotherapy promotes tumor-specific effector CD8+ T cells via dendritic cell activation. J. Immunol. 2012, 189, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Formenti, S.C. Role of T lymphocytes in tumor response to radiotherapy. Front. Oncol. 2012, 2, 95. [Google Scholar] [CrossRef]
- de la Cruz-Merino, L.; Illescas-Vacas, A.; Grueso-Lopez, A.; Barco-Sanchez, A.; Miguez-Sanchez, C.; Cancer Immunotherapies Spanish, G. Radiation for Awakening the Dormant Immune System, a Promising Challenge to be Explored. Front. Immunol. 2014, 5, 102. [Google Scholar] [CrossRef]
- Lan, J.; Li, R.; Yin, L.M.; Deng, L.; Gui, J.; Chen, B.Q.; Zhou, L.; Meng, M.B.; Huang, Q.R.; Mo, X.M.; et al. Targeting Myeloid-derived Suppressor Cells and Programmed Death Ligand 1 Confers Therapeutic Advantage of Ablative Hypofractionated Radiation Therapy Compared With Conventional Fractionated Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 74–87. [Google Scholar] [CrossRef]
- Song, C.W.; Kim, H.; Cho, H.; Kim, M.S.; Paek, S.H.; Park, H.J.; Griffin, R.J.; Terezakis, S.; Cho, L.C. HIF-1alpha Inhibition Improves Anti-Tumor Immunity and Promotes the Efficacy of Stereotactic Ablative Radiotherapy (SABR). Cancers 2022, 14, 3273. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.M. Radiation Damage to Tumor Vasculature Initiates a Program That Promotes Tumor Recurrences. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Louagie, H.; Van Eijkeren, M.; Philippe, J.; Thierens, H.; de Ridder, L. Changes in peripheral blood lymphocyte subsets in patients undergoing radiotherapy. Int. J. Radiat. Biol. 1999, 75, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, F.; Lindemalm, C.; Choudhury, A.; Granstam-Bjorneklett, H.; Helander, I.; Lekander, M.; Mikaelsson, E.; Nilsson, B.; Ojutkangas, M.L.; Osterborg, A.; et al. NK-cell and T-cell functions in patients with breast cancer: Effects of surgery and adjuvant chemo- and radiotherapy. Br. J. Cancer 2007, 97, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Vivier, E.; Ugolini, S.; Blaise, D.; Chabannon, C.; Brossay, L. Targeting natural killer cells and natural killer T cells in cancer. Nat. Rev. Immunol. 2012, 12, 239–252. [Google Scholar] [CrossRef]
- Childs, R.; Chernoff, A.; Contentin, N.; Bahceci, E.; Schrump, D.; Leitman, S.; Read, E.J.; Tisdale, J.; Dunbar, C.; Linehan, W.M.; et al. Regression of metastatic renal-cell carcinoma after nonmyeloablative allogeneic peripheral-blood stem-cell transplantation. N. Engl. J. Med. 2000, 343, 750–758. [Google Scholar] [CrossRef]
- Pilones, K.A.; Kawashima, N.; Yang, A.M.; Babb, J.S.; Formenti, S.C.; Demaria, S. Invariant natural killer T cells regulate breast cancer response to radiation and CTLA-4 blockade. Clin. Cancer Res. 2009, 15, 597–606. [Google Scholar] [CrossRef]
- Meylan, M.; Petitprez, F.; Becht, E.; Bougouin, A.; Pupier, G.; Calvez, A.; Giglioli, I.; Verkarre, V.; Lacroix, G.; Verneau, J.; et al. Tertiary lymphoid structures generate and propagate anti-tumor antibody-producing plasma cells in renal cell cancer. Immunity 2022, 55, 527–541.e525. [Google Scholar] [CrossRef]
- Affara, N.I.; Ruffell, B.; Medler, T.R.; Gunderson, A.J.; Johansson, M.; Bornstein, S.; Bergsland, E.; Steinhoff, M.; Li, Y.; Gong, Q.; et al. B cells regulate macrophage phenotype and response to chemotherapy in squamous carcinomas. Cancer Cell 2014, 25, 809–821. [Google Scholar] [CrossRef]
- Schaue, D.; Xie, M.W.; Ratikan, J.A.; McBride, W.H. Regulatory T cells in radiotherapeutic responses. Front. Oncol. 2012, 2, 90. [Google Scholar] [CrossRef]
- Sakaguchi, S.; Mikami, N.; Wing, J.B.; Tanaka, A.; Ichiyama, K.; Ohkura, N. Regulatory T Cells and Human Disease. Annu. Rev. Immunol. 2020, 38, 541–566. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| HFRT | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Pathology | n of pts | Study Design | RT | Systemic Therapy | Lymphocyte Parameters | Outcome | Sample |
| Mirjolet [9] | 2018 | Rectal Cancer | 237 | retrospective | NEO-ADJ RT long-course (<2 Gy/fx) vs. short course(>2 Gy/fx) | concomitant CHT + adj | TILs: CD8C and FoxP3 T cells | impact of TILS on PFS and OS: high FoxP3 TIL better PFS; decrease CD8C/FoxP3 TILs ratio better PFS & OS; lower CD8C/FoxP3 ratio with short-course RT | tumor tissue (biopsy and surgical sample) |
| Yuan [10] | 2018 | Breast Cancer | 60 | observational | ADJ RT (50 Gy/25 fx vs. 40.3 Gy/13 fx) | ADJ CHT | TLC, lymph subpopulation (T, B, NK cells) | lymph dropped after RT, recovered at 6 m, higher value in hypo; subpopulations change with different fx schedule | peripheral blood |
| Linares-Galiana [11] | 2021 | Breast Cancer | 13 | observational | IORT (20 Gy/1 fx) | hormone therapy | NK, Treg, MDSC | NK CD56+ high CD16+ increased 3 w after IORT | peripheral blood |
| SBRT | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Pathology | n of pts | Study Design | RT | Systemic Therapy | Lymphocyte Parameters and Cytokines | Outcome | Sample |
| Maehata [12] | 2013 | NSCLC | 62 | retrospective | SBRT (40–70 Gy/4–10 fx) | none | TLC and lymph subsets: CD3+, CD4+, CD8+, CD19+, CD56+, and NKA | Lymph subset, NKA post-RT lower than pre-SBRT | peripheral blood |
| Zhang [13] | 2017 | NSCLC | 6 | observational | SBRT (48 Gy/4–8 fx) | none | T, B cells, cytokines | CD8+ T cells transformed into activated T cells; increase in IL-2, T NF-α, IFN-γ; reduce production of TGF-β in CD4+ T cells; naïve B cells and double-neg B cells lower | peripheral blood |
| Rutkowski [14] | 2017 | NSCLC | 89 | prospective | SBRT (54–60 Gy/3–8 fx) | none | CD4+, CD8+ T cells, T-bet, GATA-3, ROR-γt, FoxP3, CRP, ANC, WBC | CD8+, CD4+, CD4(+) T cells expressing GATA-3+, T-bet+, ROR-γt+ increased; CD4+FoxP3+ cells decreased | peripheral blood |
| Navarro [15] | 2018 | NSCLC, LUNG M+ | 7 | prospective | SBRT (50–60 Gy/4–8 fx)) | none | total lymph, CD56+high CD16+NK, CD4+CD25+ Foxp3+ CDA5RA Treg, G-MDSCs, Mo-MDSCs | Increase CD56+highCD16+NK 6 m; decrease CD4+CD25+ Foxp3+CDA5RA Treg, G-MDSCs and Mo-MDSCs at 6 m; T CD3+CD8+, T CD3+CD4+ and TCD4/CD8 ratio increase | peripheral blood |
| Gustafson [16] | 2017 | Liver cancer (CCA, HCC, liver M+) | 10 | observational | SBRT (50–60 Gy/3–5 fx) | none | CD8+ T cells; CD4+CD25+ CD127lo Treg cells; CD56+CD16+ NK cells; PD-1 | no difference in CD8+ T cells, CD4+CD25+ CD127lo Treg cells, NK cells and PD-1 expression; decrease in CD56brCD16- NK | peripheral blood |
| Zhuang [17] | 2019 | HCC | 78 | Retrospective | SBRT (48–60 Gy/5–8 fx) | none | TPLCs, CLPs | TPLC, B cells, NK, T cells subpop reduced 10 days after SBRT (B cells lower value) | peripheral blood |
| Kane [18] | 2022 | PCa | 6 | prospective | neoadj SBRT (24 Gy/3fx) (prior to RP) | none | T CD3+CD8+, T CD3+CD4+, Treg cell (CD4 + FOXp3), CD68 + and CD163+ macrophage | T CD3+CD8+ decreased; T CD3+CD4+ and Treg cell (CD4 + FOXp3) stable; CD68 and CD163+ macrophage increased | tumor tissue (biopsy and surgical sample) |
| McGee [19] | 2019 | various: lung, liver, adrenal, brain, bone, and others | 68 | prospective | SBRT (20–54 Gy/1–5 fx) | none | CD8 T cells, CD4 T cells, NK cells, TIM3+ expression | Total and cytotoxic NK decreased, TIM3+ increased, CD4+ T cells, activated and CD25+ CD4+ memory T cells, and activated CD25+ CD8+ memory T cells increased, TNF-a, RANTES decreased after RT in parenchymal sites, no brain | peripheral blood |
| Crocenzi [20] | 2016 | Pancreatic Cancer | 20 | prospective | SBRT (30 Gy/3 fx) vs. CFRT (50.4 Gy/28 fx) | NEO-ADJ CHT | T cells subsets: CD3+, CD4+, CD8+, Treg; cytokines; | CD4+, CD8+, Treg reduced in CFRT. IL-15 reduced in CFRT and SBRT | peripheral blood |
| Formenti [21] | 2019 | NSCLC M+ | 39 | prospective | SBRT (30 Gy/5 fx; 28.5 Gy/3 fx) | IT | T cells subsets (peripheral bl): CD3+, CD4+, CD8+, Treg; | increase in CD8+, CD4+ T cells | peripheral blood |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takanen, S.; Bottero, M.; Nisticò, P.; Sanguineti, G. A Systematic Review on the Impact of Hypofractionated and Stereotactic Radiotherapy on Immune Cell Subpopulations in Cancer Patients. Cancers 2022, 14, 5190. https://doi.org/10.3390/cancers14215190
Takanen S, Bottero M, Nisticò P, Sanguineti G. A Systematic Review on the Impact of Hypofractionated and Stereotactic Radiotherapy on Immune Cell Subpopulations in Cancer Patients. Cancers. 2022; 14(21):5190. https://doi.org/10.3390/cancers14215190
Chicago/Turabian StyleTakanen, Silvia, Marta Bottero, Paola Nisticò, and Giuseppe Sanguineti. 2022. "A Systematic Review on the Impact of Hypofractionated and Stereotactic Radiotherapy on Immune Cell Subpopulations in Cancer Patients" Cancers 14, no. 21: 5190. https://doi.org/10.3390/cancers14215190
APA StyleTakanen, S., Bottero, M., Nisticò, P., & Sanguineti, G. (2022). A Systematic Review on the Impact of Hypofractionated and Stereotactic Radiotherapy on Immune Cell Subpopulations in Cancer Patients. Cancers, 14(21), 5190. https://doi.org/10.3390/cancers14215190