
Genomic Instability in Cerebrospinal Fluid Cell-Free DNA Predicts Poor Prognosis in Solid Tumor Patients with Meningeal Metastasis

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Information
2.2. Plasma Cell-Free DNA Extraction
2.3. cfDNA Extraction from CSF
2.4. Library Preparation and Next-Generation Sequencing
2.5. Low-Throughput Whole-Genome Sequencing
2.6. Calculation of the GI Score
2.7. Statistical Analysis
3. Results
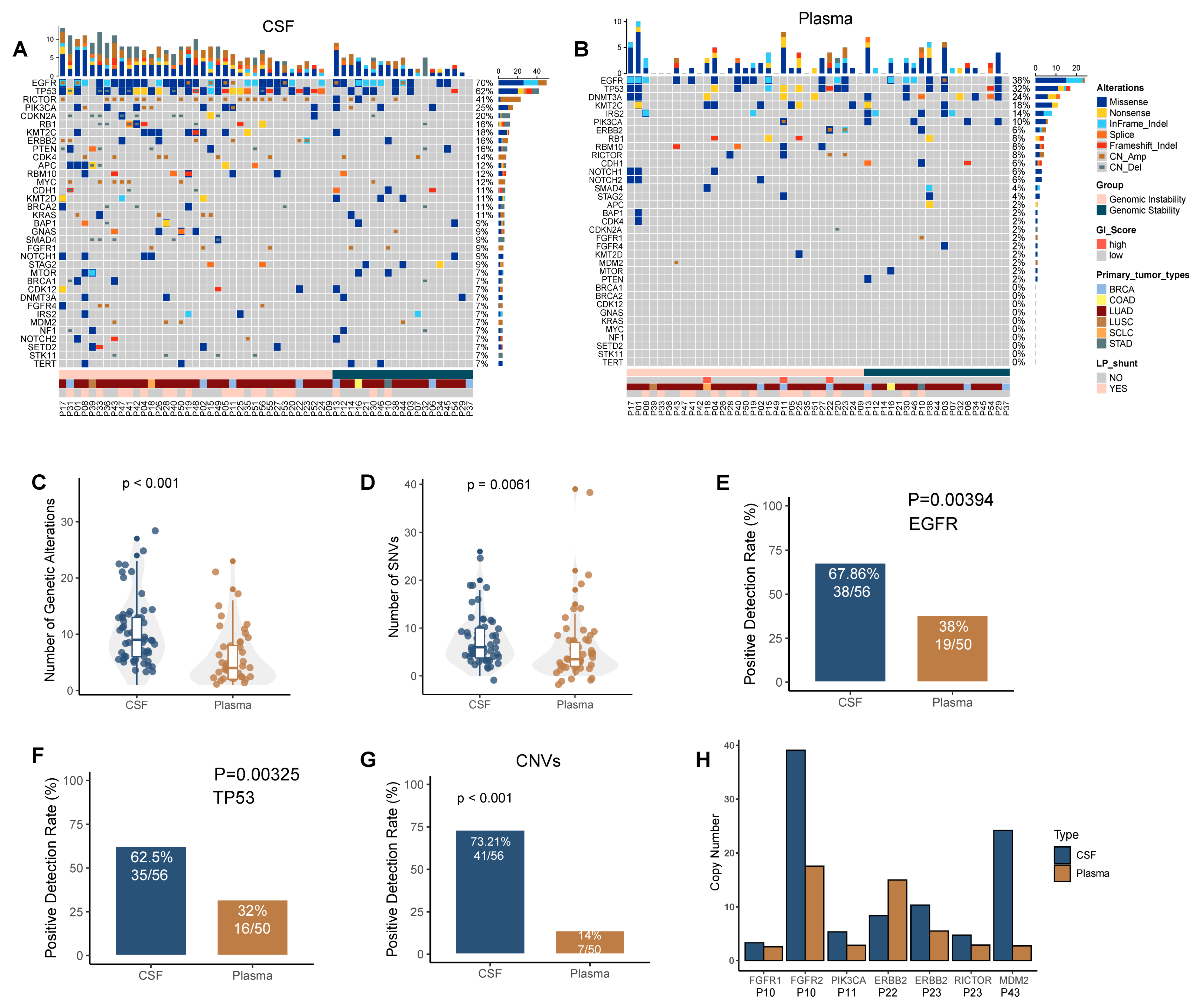
3.1. Cerebrospinal Fluid ctDNA Show More Genetic Variation Events Than Plasma ctDNA
3.2. A Panel-Developed GI Score Was Established to Describe the GI Status in CSF ctDNA and Verified Using Whole-Genome Sequencing-Based Copy Number Analysis
3.3. Increased GI Was Detected in Mm Lesions-Derived CSF ctDNA Compared with Plasma ctDNA
3.4. GI Is Associated with Poor Prognosis, High Intracranial Pressure, and Low Karnofsky Performance Status Scores in MM Patients
3.5. Co-Mutations of Tp53 and Hotspot Driver Genes Were Associated with a High GI Score and Poor Prognosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chamberlain, M.; Soffietti, R.; Raizer, J.; Rudà, R.; Brandsma, D.; Boogerd, W.; Taillibert, S.; Groves, M.D.; le Rhun, E.; Junck, L.; et al. Leptomeningeal metastasis: A Response Assessment in Neuro-Oncology critical review of endpoints and response criteria of published randomized clinical trials. Neuro-Oncology 2014, 16, 1176–1185. [Google Scholar] [CrossRef] [PubMed]
- le Rhun, E.; Taillibert, S.; Chamberlain, M.C. Carcinomatous meningitis: Leptomeningeal metastases in solid tumors. Surg. Neurol. Int. 2013, 4, S265–S288. [Google Scholar] [PubMed]
- Corbin, Z.A.; Nagpal, S. Leptomeningeal Metastases. JAMA Oncol. 2016, 2, 839. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, H.; Wakuda, K.; Fukuda, M.; Kenmotsu, H.; Mukae, H.; Ito, K.; Chibana, K.; Inoue, K.; Miura, S.; Tanaka, K.; et al. A Phase II Study of Osimertinib for Radiotherapy-Naive Central Nervous System Metastasis From NSCLC: Results for the T790M Cohort of the OCEAN Study (LOGIK1603/WJOG9116L). J. Thorac. Oncol. 2021, 16, 2121–2132. [Google Scholar] [CrossRef]
- Lee, E.; Keam, B.; Kim, D.W.; Kim, T.M.; Lee, S.H.; Chung, D.H.; Heo, D.S. Erlotinib versus gefitinib for control of leptomeningeal carcinomatosis in non-small-cell lung cancer. J. Thorac. Oncol. 2013, 8, 1069–1074. [Google Scholar] [CrossRef]
- Tijhuis, A.E.; Johnson, S.C.; McClelland, S.E. The emerging links between chromosomal instability (CIN), metastasis, inflammation and tumour immunity. Mol. Cytogenet. 2019, 12, 17. [Google Scholar] [CrossRef]
- Bakhoum, S.F.; Cantley, L.C. The Multifaceted Role of Chromosomal Instability in Cancer and Its Microenvironment. Cell 2018, 174, 1347–1360. [Google Scholar] [CrossRef]
- Bakhoum, S.F.; Ngo, B.; Laughney, A.M.; Cavallo, J.A.; Murphy, C.J.; Ly, P.; Shah, P.; Sriram, R.K.; Watkins, T.B.K.; Taunk, N.K.; et al. Chromosomal instability drives metastasis through a cytosolic DNA response. Nature 2018, 553, 467–472. [Google Scholar] [CrossRef]
- Steeg, P.S. Targeting metastasis. Nat. Rev. Cancer 2016, 16, 201–218. [Google Scholar] [CrossRef]
- Nguyen, B.; Fong, C.; Luthra, A.; Smith, S.A.; DiNatale, R.G.; Nandakumar, S.; Walch, H.; Chatila, W.K.; Madupuri, R.; Kundra, R.; et al. Genomic characterization of metastatic patterns from prospective clinical sequencing of 25,000 patients. Cell 2022, 185, 563–575.e511. [Google Scholar] [CrossRef]
- Duijf, P.H.G.; Nanayakkara, D.; Nones, K.; Srihari, S.; Kalimutho, M.; Khanna, K.K. Mechanisms of Genomic Instability in Breast Cancer. Trends Mol. Med. 2019, 25, 595–611. [Google Scholar] [CrossRef] [PubMed]
- Slade, D. PARP and PARG inhibitors in cancer treatment. Genes Dev. 2020, 34, 360–394. [Google Scholar] [CrossRef]
- Mateo, J.; Lord, C.J.; Serra, V.; Tutt, A.; Balmaña, J.; Castroviejo-Bermejo, M.; Cruz, C.; Oaknin, A.; Kaye, S.B.; de Bono, J.S. A decade of clinical development of PARP inhibitors in perspective. Ann. Oncol. 2019, 30, 1437–1447. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, H.; Chen, P.; Sun, Z.; Zhang, Z.; Yin, Q.; Sun, H.; Yu, J. The Presence of Genomic Instability in Cerebrospinal Fluid in Patients with Meningeal Metastasis. Cancer Manag. Res. 2021, 13, 4853–4863. [Google Scholar] [CrossRef] [PubMed]
- Woodhouse, R.; Li, M.; Hughes, J.; Delfosse, D.; Skoletsky, J.; Ma, P.; Meng, W.; Dewal, N.; Milbury, C.; Clark, T.; et al. Clinical and analytical validation of FoundationOne Liquid CDx, a novel 324-Gene cfDNA-based comprehensive genomic profiling assay for cancers of solid tumor origin. PLoS ONE 2020, 15, e0237802. [Google Scholar] [CrossRef] [PubMed]
- Crowley, E.; di Nicolantonio, F.; Loupakis, F.; Bardelli, A. Liquid biopsy: Monitoring cancer-genetics in the blood. Nat. Rev. Clin. Oncol. 2013, 10, 472–484. [Google Scholar] [CrossRef] [PubMed]
- Dawson, S.J.; Tsui, D.W.; Murtaza, M.; Biggs, H.; Rueda, O.M.; Chin, S.F.; Dunning, M.J.; Gale, D.; Forshew, T.; Mahler-Araujo, B.; et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N. Engl. J. Med. 2013, 368, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.S.; Jiang, B.Y.; Yang, J.J.; Zhang, X.C.; Zhang, Z.; Ye, J.Y.; Zhong, W.Z.; Tu, H.Y.; Chen, H.J.; Wang, Z.; et al. Unique genetic profiles from cerebrospinal fluid cell-free DNA in leptomeningeal metastases of EGFR-mutant non-small-cell lung cancer: A new medium of liquid biopsy. Ann. Oncol. 2018, 29, 945–952. [Google Scholar] [CrossRef]
- Pentsova, E.I.; Shah, R.H.; Tang, J.; Boire, A.; You, D.; Briggs, S.; Omuro, A.; Lin, X.; Fleisher, M.; Grommes, C.; et al. Evaluating Cancer of the Central Nervous System Through Next-Generation Sequencing of Cerebrospinal Fluid. J. Clin. Oncol. 2016, 34, 2404–2415. [Google Scholar] [CrossRef]
- Ying, S.; Ke, H.; Ding, Y.; Liu, Y.; Tang, X.; Yang, D.; Li, M.; Liu, J.; Yu, B.; Xiang, J.; et al. Unique genomic profiles obtained from cerebrospinal fluid cell-free DNA of non-small cell lung cancer patients with leptomeningeal metastases. Cancer Biol. Ther. 2019, 20, 562–570. [Google Scholar] [CrossRef]
- Lennon, N.J.; Adalsteinsson, V.A.; Gabriel, S.B. Technological considerations for genome-guided diagnosis and management of cancer. Genome Med. 2016, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Wan, J.C.M.; Massie, C.; Garcia-Corbacho, J.; Mouliere, F.; Brenton, J.D.; Caldas, C.; Pacey, S.; Baird, R.; Rosenfeld, N. Liquid biopsies come of age: Towards implementation of circulating tumour DNA. Nat. Rev. Cancer 2017, 17, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Adalsteinsson, V.A.; Ha, G.; Freeman, S.S.; Choudhury, A.D.; Stover, D.G.; Parsons, H.A.; Gydush, G.; Reed, S.C.; Rotem, D.; Rhoades, J.; et al. Scalable whole-exome sequencing of cell-free DNA reveals high concordance with metastatic tumors. Nat. Commun. 2017, 8, 1324. [Google Scholar] [CrossRef] [PubMed]
- Murtaza, M.; Dawson, S.J.; Tsui, D.W.; Gale, D.; Forshew, T.; Piskorz, A.M.; Parkinson, C.; Chin, S.F.; Kingsbury, Z.; Wong, A.S.; et al. Non-invasive analysis of acquired resistance to cancer therapy by sequencing of plasma DNA. Nature 2013, 497, 108–112. [Google Scholar] [CrossRef] [PubMed]
- McEwen, A.E.; Leary, S.E.S.; Lockwood, C.M. Beyond the Blood: CSF-Derived cfDNA for Diagnosis and Characterization of CNS Tumors. Front. Cell Dev. Biol. 2020, 8, 45. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.M.; Li, Y.S.; Jiang, B.Y.; Tu, H.Y.; Tang, W.F.; Yang, J.J.; Zhang, X.C.; Ye, J.Y.; Yan, H.H.; Su, J.; et al. Clinical Utility of Cerebrospinal Fluid Cell-Free DNA as Liquid Biopsy for Leptomeningeal Metastases in ALK-Rearranged NSCLC. J. Thorac. Oncol. 2019, 14, 924–932. [Google Scholar] [CrossRef]
- Seoane, J.; de Mattos-Arruda, L.; le Rhun, E.; Bardelli, A.; Weller, M. Cerebrospinal fluid cell-free tumour DNA as a liquid biopsy for primary brain tumours and central nervous system metastases. Ann. Oncol. 2019, 30, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Godek, K.M.; Venere, M.; Wu, Q.; Mills, K.D.; Hickey, W.F.; Rich, J.N.; Compton, D.A. Chromosomal Instability Affects the Tumorigenicity of Glioblastoma Tumor-Initiating Cells. Cancer Discov. 2016, 6, 532–545. [Google Scholar] [CrossRef] [PubMed]
- Drews, R.M.; Hernando, B.; Tarabichi, M.; Haase, K.; Lesluyes, T.; Smith, P.S.; Gavarró, L.M.; Couturier, D.L.; Liu, L.; Schneider, M.; et al. A pan-cancer compendium of chromosomal instability. Nature 2022, 606, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhou, X.A.; Zhang, N.; Wang, J. Evolving insights: How DNA repair pathways impact cancer evolution. Cancer Biol. Med. 2020, 17, 805–827. [Google Scholar] [CrossRef]
- Lin, N.; Dunn, I.F.; Glantz, M.; Allison, D.L.; Jensen, R.; Johnson, M.D.; Friedlander, R.M.; Kesari, S. Benefit of ventriculoperitoneal cerebrospinal fluid shunting and intrathecal chemotherapy in neoplastic meningitis: A retrospective, case-controlled study. J. Neurosurg. 2011, 115, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Wang, V.Y.; Barbaro, N.M.; Lawton, M.T.; Pitts, L.; Kunwar, S.; Parsa, A.T.; Gupta, N.; McDermott, M.W. Complications of lumboperitoneal shunts. Neurosurgery 2007, 60, 1045–1048; discussion 1049. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.H.; Wang, X.G.; Piao, Y.Z.; Wang, P.; Li, P.; Li, W.L. Lumboperitoneal shunt for the treatment of leptomeningeal metastasis. Med. Hypotheses 2015, 84, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Yates, J.W.; Chalmer, B.; McKegney, F.P. Evaluation of patients with advanced cancer using the Karnofsky performance status. Cancer 1980, 45, 2220–2224. [Google Scholar] [CrossRef]
- Mor, V.; Laliberte, L.; Morris, J.N.; Wiemann, M. The Karnofsky Performance Status Scale. An examination of its reliability and validity in a research setting. Cancer 1984, 53, 2002–2007. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Ledermann, J.A.; Selle, F.; Gebski, V.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Poveda, A.; Pignata, S.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet. Oncol. 2017, 18, 1274–1284. [Google Scholar] [CrossRef]
- Mateo, J.; Porta, N.; Bianchini, D.; McGovern, U.; Elliott, T.; Jones, R.; Syndikus, I.; Ralph, C.; Jain, S.; Varughese, M.; et al. Olaparib in patients with metastatic castration-resistant prostate cancer with DNA repair gene aberrations (TOPARP-B): A multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 162–174. [Google Scholar] [CrossRef]
- Huang, X.; Motea, E.A.; Moore, Z.R.; Yao, J.; Dong, Y.; Chakrabarti, G.; Kilgore, J.A.; Silvers, M.A.; Patidar, P.L.; Cholka, A.; et al. Leveraging an NQO1 Bioactivatable Drug for Tumor-Selective Use of Poly(ADP-ribose) Polymerase Inhibitors. Cancer Cell 2016, 30, 940–952. [Google Scholar] [CrossRef] [PubMed]
- Birkbak, N.J.; Eklund, A.C.; Li, Q.; McClelland, S.E.; Endesfelder, D.; Tan, P.; Tan, I.B.; Richardson, A.L.; Szallasi, Z.; Swanton, C. Paradoxical relationship between chromosomal instability and survival outcome in cancer. Cancer Res. 2011, 71, 3447–3452. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 56 1 |
|---|---|
| Gender | |
| Female | 29 (52%) |
| Male | 27 (48%) |
| Age | |
| ≤55 | 27 (48%) |
| >55 | 29 (52%) |
| Primary tumor type | |
| BRCA | 7 (12%) |
| COAD | 1 (1.8%) |
| LUAD | 45 (80%) |
| LUSC | 1 (1.8%) |
| SCLC | 1 (1.8%) |
| STAD | 1 (1.8%) |
| KPS | 70 (60, 80) |
| Intracranial pressure (Kpa) | 1.5 (1.1, 3.1) |
| LP shunt | 20 (36%) |
| Genomic status | |
| GI | 37 (66.1%) |
| GS | 19 (33.9%) |
| Characteristic | GI, N = 37 1 | GS, N = 19 1 | p-Value 2 |
|---|---|---|---|
| Gender | 0.074 | ||
| Female | 16 (43%) | 13 (68%) | |
| Male | 21 (57%) | 6 (32%) | |
| Age | 0.6 | ||
| ≤55 | 17 (46%) | 10 (53%) | |
| >55 | 20 (54%) | 9 (47%) | |
| Primary tumor type | 0.4 | ||
| BRCA | 4 (11%) | 3 (16%) | |
| COAD | 0 (0%) | 1 (5.3%) | |
| LUAD | 31 (84%) | 14 (74%) | |
| LUSC | 1 (2.7%) | 0 (0%) | |
| SCLC | 1 (2.7%) | 0 (0%) | |
| STAD | 0 (0%) | 1 (5.3%) | |
| Intracranial pressure (Kpa) | 1.7 (1.2, 3.2) | 1.3 (1, 1.8) | 0.094 |
| LP shunt | 0.026 | ||
| No | 20 (54%) | 16 (84%) | |
| Yes | 17 (46%) | 3 (16%) | |
| GI score | 0.28 (0.19, 0.42) | 0.03 (0.02, 0.04) | <0.001 |
| Characteristics | Total (N) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | ||
| Sex | 45 | ||||
| Female | 20 | Reference | |||
| Male | 25 | 1.339 (0.688–2.606) | 0.390 | ||
| Age | 45 | ||||
| ≤55 | 21 | Reference | |||
| >55 | 24 | 0.992 (0.514–1.915) | 0.981 | ||
| LP Shunt | 45 | ||||
| No | 29 | Reference | |||
| Yes | 16 | 1.669 (0.855–3.260) | 0.133 | ||
| KPS | 45 | 0.991 (0.967–1.016) | 0.489 | ||
| Genomic Status | 45 | ||||
| GS | 14 | Reference | |||
| GI | 31 | 2.338 (1.109–4.929) | 0.026 | 2.338 (1.109–4.929) | 0.026 |
| Characteristics | Total (N) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | ||
| Gender | 45 | ||||
| Female | 20 | Reference | |||
| Male | 25 | 1.764 (0.915–3.400) | 0.090 | ||
| Age | 45 | ||||
| ≤55 | 21 | Reference | |||
| >55 | 24 | 0.872 (0.459–1.658) | 0.677 | ||
| LP Shunt | 45 | ||||
| No | 29 | Reference | |||
| Yes | 16 | 1.473 (0.764–2.840) | 0.248 | ||
| KPS | 45 | 0.978 (0.953–1.003) | 0.082 | ||
| Genomic Status | 45 | ||||
| GS | 14 | Reference | |||
| GI | 31 | 2.109 (1.030–4.317) | 0.041 | 2.109 (1.030–4.317) | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, P.; Zhang, Q.; Han, L.; Cheng, Y.; Sun, Z.; Yin, Q.; Zhang, Z.; Yu, J. Genomic Instability in Cerebrospinal Fluid Cell-Free DNA Predicts Poor Prognosis in Solid Tumor Patients with Meningeal Metastasis. Cancers 2022, 14, 5028. https://doi.org/10.3390/cancers14205028
Wang P, Zhang Q, Han L, Cheng Y, Sun Z, Yin Q, Zhang Z, Yu J. Genomic Instability in Cerebrospinal Fluid Cell-Free DNA Predicts Poor Prognosis in Solid Tumor Patients with Meningeal Metastasis. Cancers. 2022; 14(20):5028. https://doi.org/10.3390/cancers14205028
Chicago/Turabian StyleWang, Peng, Qiaoling Zhang, Lei Han, Yanan Cheng, Zengfeng Sun, Qiang Yin, Zhen Zhang, and Jinpu Yu. 2022. "Genomic Instability in Cerebrospinal Fluid Cell-Free DNA Predicts Poor Prognosis in Solid Tumor Patients with Meningeal Metastasis" Cancers 14, no. 20: 5028. https://doi.org/10.3390/cancers14205028
APA StyleWang, P., Zhang, Q., Han, L., Cheng, Y., Sun, Z., Yin, Q., Zhang, Z., & Yu, J. (2022). Genomic Instability in Cerebrospinal Fluid Cell-Free DNA Predicts Poor Prognosis in Solid Tumor Patients with Meningeal Metastasis. Cancers, 14(20), 5028. https://doi.org/10.3390/cancers14205028