

Dose-Escalated Salvage Radiotherapy for Macroscopic Local Recurrence of Prostate Cancer in the Prostate-Specific Membrane Antigen Positron Emission Tomography Era
 , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sargos, P.; Chabaud, S.; Latorzeff, I.; Magne, N.; Benyoucef, A.; Supiot, S.; Pasquier, D.; Abdiche, M.S.; Gilliot, O.; Graff-Cailleaud, P.; et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localised prostate cancer after radical prostatectomy (GETUG-AFU 17): A randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1341–1352. [Google Scholar] [CrossRef]
- Kneebone, A.; Fraser-Browne, C.; Duchesne, G.M.; Fisher, R.; Frydenberg, M.; Herschtal, A.; Williams, S.G.; Brown, C.; Delprado, W.; Haworth, A.; et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020, 21, 1331–1340. [Google Scholar] [CrossRef]
- Bluemel, C.; Krebs, M.; Polat, B.; Linke, F.; Eiber, M.; Samnick, S.; Lapa, C.; Lassmann, M.; Riedmiller, H.; Czernin, J.; et al. 68Ga-PSMA-PET/CT in Patients with Biochemical Prostate Cancer Recurrence and Negative 18F-Choline-PET/CT. Clin. Nucl. Med. 2016, 41, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Eiber, M.; Maurer, T.; Souvatzoglou, M.; Beer, A.J.; Ruffani, A.; Haller, B.; Graner, F.P.; Kubler, H.; Haberkorn, U.; Eisenhut, M.; et al. Evaluation of Hybrid (6)(8)Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence After Radical Prostatectomy. J. Nucl. Med. 2015, 56, 668–674. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Perera, M.; Papa, N.; Roberts, M.; Williams, M.; Udovicich, C.; Vela, I.; Christidis, D.; Bolton, D.; Hofman, M.S.; Lawrentschuk, N.; et al. Gallium-68 Prostate-specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer-Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-Specific Membrane Antigen-Avid Lesions: A Systematic Review and Meta-Analysis. Eur. Urol. 2020, 77, 403–417. [Google Scholar]
- Calais, J.; Czernin, J.; Cao, M.; Kishan, A.U.; Hegde, J.V.; Shaverdian, N.; Sandler, K.; Chu, F.I.; King, C.R.; Steinberg, M.L.; et al. (68)Ga-PSMA-11 PET/CT Mapping of Prostate Cancer Biochemical Recurrence After Radical Prostatectomy in 270 Patients with a PSA Level of Less Than 1.0 ng/mL: Impact on Salvage Radiotherapy Planning. J. Nucl. Med. 2018, 59, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Pozdnyakov, A.; Kulanthaivelu, R.; Bauman, G.; Ortega, C.; Veit-Haibach, P.; Metser, U. The impact of PSMA PET on the treatment and outcomes of men with biochemical recurrence of prostate cancer: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2022. [Google Scholar] [CrossRef]
- Ghadjar, P.; Hayoz, S.; Bernhard, J.; Zwahlen, D.R.; Holscher, T.; Gut, P.; Polat, B.; Hildebrandt, G.; Muller, A.C.; Plasswilm, L.; et al. Dose-Intensified Versus Conventional-Dose Salvage Radiotherapy for Biochemically Recurrent Prostate Cancer After Prostatectomy: The SAKK 09/10 Randomized Phase 3 Trial. Eur. Urol. 2021, 80, 306–315. [Google Scholar] [CrossRef]
- Shelan, M.; Odermatt, S.; Bojaxhiu, B.; Nguyen, D.P.; Thalmann, G.N.; Aebersold, D.M.; Dal Pra, A. Disease Control With Delayed Salvage Radiotherapy for Macroscopic Local Recurrence Following Radical Prostatectomy. Front. Oncol. 2019, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Dal Pra, A.; Panje, C.; Zilli, T.; Arnold, W.; Brouwer, K.; Garcia, H.; Glatzer, M.; Gomez, S.; Herrera, F.; Kaouthar, K.; et al. Salvage radiotherapy for macroscopic local recurrences after radical prostatectomy: A national survey on patterns of practice. Strahlenther. Onkol. 2018, 194, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Bruni, A.; Ingrosso, G.; Trippa, F.; Di Staso, M.; Lanfranchi, B.; Rubino, L.; Parente, S.; Frassinelli, L.; Maranzano, E.; Santoni, R.; et al. Macroscopic locoregional relapse from prostate cancer: Which role for salvage radiotherapy? Clin. Transl. Oncol. 2019, 21, 1532–1537. [Google Scholar] [CrossRef] [PubMed]
- Zaine, H.; Vandendorpe, B.; Bataille, B.; Lacornerie, T.; Wallet, J.; Mirabel, X.; Lartigau, E.; Pasquier, D. Salvage Radiotherapy for Macroscopic Local Recurrence Following Radical Prostatectomy. Front. Oncol. 2021, 11, 669261. [Google Scholar] [CrossRef] [PubMed]
- Zilli, T.; Jorcano, S.; Peguret, N.; Caparrotti, F.; Hidalgo, A.; Khan, H.G.; Vees, H.; Miralbell, R. Results of Dose-Adapted Salvage Radiotherapy After Radical Prostatectomy Based on an Endorectal MRI Target Definition Model. Am. J. Clin. Oncol. 2017, 40, 194–199. [Google Scholar] [CrossRef]
- Lee, S.U.; Cho, K.H.; Kim, J.H.; Kim, Y.S.; Nam, T.K.; Kim, J.S.; Cho, J.; Choi, S.H.; Shim, S.J.; Kim, J.H.; et al. Clinical Outcome of Salvage Radiotherapy for Locoregional Clinical Recurrence After Radical Prostatectomy. Technol. Cancer Res. Treat. 2021, 20, 15330338211041212. [Google Scholar] [CrossRef]
- Francolini, G.; Jereczek-Fossa, B.A.; Di Cataldo, V.; Simontacchi, G.; Marvaso, G.; Zerella, M.A.; Gentile, P.; Bianciardi, F.; Allegretta, S.; Detti, B.; et al. Stereotactic radiotherapy for prostate bed recurrence after prostatectomy, a multicentric series. BJU Int. 2020, 125, 417–425. [Google Scholar] [CrossRef]
- Francolini, G.; Jereczek-Fossa, B.A.; Di Cataldo, V.; Simontacchi, G.; Marvaso, G.; Gandini, S.; Corso, F.; Ciccone, L.P.; Zerella, M.A.; Gentile, P.; et al. Stereotactic or conventional radiotherapy for macroscopic prostate bed recurrence: A propensity score analysis. Radiol. Med. 2022, 127, 449–457. [Google Scholar] [CrossRef]
- Schmidt-Hegemann, N.S.; Stief, C.; Kim, T.H.; Eze, C.; Kirste, S.; Strouthos, I.; Li, M.; Schultze-Seemann, W.; Ilhan, H.; Fendler, W.P.; et al. Outcome after PSMA PET/CT based salvage radiotherapy in patients with biochemical recurrence after radical prostatectomy: A bi-institutional retrospective analysis. J. Nucl. Med. 2019, 60, 227–233. [Google Scholar] [CrossRef]
- Vogel, M.M.E.; Dewes, S.; Sage, E.K.; Devecka, M.; Eitz, K.A.; Gschwend, J.E.; Eiber, M.; Combs, S.E.; Schiller, K. Feasibility and Outcome of PSMA-PET-Based Dose-Escalated Salvage Radiotherapy versus Conventional Salvage Radiotherapy for Patients With Recurrent Prostate Cancer. Front. Oncol. 2021, 11, 715020. [Google Scholar] [CrossRef]
- Tamihardja, J.; Zehner, L.; Hartrampf, P.; Lisowski, D.; Kneitz, S.; Cirsi, S.; Razinskas, G.; Flentje, M.; Polat, B. Salvage Nodal Radiotherapy as Metastasis-Directed Therapy for Oligorecurrent Prostate Cancer Detected by Positron Emission Tomography Shows Favorable Outcome in Long-Term Follow-Up. Cancers 2022, 14, 3766. [Google Scholar] [CrossRef]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Ghadjar, P.; Aebersold, D.M.; Albrecht, C.; Bohmer, D.; Flentje, M.; Ganswindt, U.; Hocht, S.; Holscher, T.; Sedlmayer, F.; Wenz, F.; et al. Use of androgen deprivation and salvage radiation therapy for patients with prostate cancer and biochemical recurrence after prostatectomy. Strahlenther. Onkol. 2018, 194, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading, C. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Carrie, C.; Magne, N.; Burban-Provost, P.; Sargos, P.; Latorzeff, I.; Lagrange, J.L.; Supiot, S.; Belkacemi, Y.; Peiffert, D.; Allouache, N.; et al. Short-term androgen deprivation therapy combined with radiotherapy as salvage treatment after radical prostatectomy for prostate cancer (GETUG-AFU 16): A 112-month follow-up of a phase 3, randomised trial. Lancet Oncol. 2019, 20, 1740–1749. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf (accessed on 4 May 2022).
- Meijer, D.; Eppinga, W.S.C.; Mohede, R.M.; Vanneste, B.G.L.; Meijnen, P.; Meijer, O.W.M.; Daniels, L.A.; van den Bergh, R.C.N.; Lont, A.P.; Ettema, R.H.; et al. Prostate-Specific Membrane Antigen Positron Emission Tomography/Computed Tomography Is Associated with Improved Oncological Outcome in Men Treated with Salvage Radiation Therapy for Biochemically Recurrent Prostate Cancer. Eur. Urol. Oncol. 2022, 5, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Emmett, L.; van Leeuwen, P.J.; Nandurkar, R.; Scheltema, M.J.; Cusick, T.; Hruby, G.; Kneebone, A.; Eade, T.; Fogarty, G.; Jagavkar, R.; et al. Treatment Outcomes from (68)Ga-PSMA PET/CT-Informed Salvage Radiation Treatment in Men with Rising PSA After Radical Prostatectomy: Prognostic Value of a Negative PSMA PET. J. Nucl. Med. 2017, 58, 1972–1976. [Google Scholar] [CrossRef]
- Tendulkar, R.D.; Agrawal, S.; Gao, T.; Efstathiou, J.A.; Pisansky, T.M.; Michalski, J.M.; Koontz, B.F.; Hamstra, D.A.; Feng, F.Y.; Liauw, S.L.; et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy after Radical Prostatectomy. J. Clin. Oncol. 2016, 34, 3648–3654. [Google Scholar] [CrossRef]
- Schwenck, J.; Olthof, S.C.; Pfannenberg, C.; Reischl, G.; Wegener, D.; Marzec, J.; Bedke, J.; Stenzl, A.; Nikolaou, K.; la Fougere, C.; et al. Intention-to-Treat Analysis of (68)Ga-PSMA and (11)C-Choline PET/CT Versus CT for Prostate Cancer Recurrence after Surgery. J. Nucl. Med. 2019, 60, 1359–1365. [Google Scholar] [CrossRef]
- Shipley, W.U.; Seiferheld, W.; Lukka, H.R.; Major, P.P.; Heney, N.M.; Grignon, D.J.; Sartor, O.; Patel, M.P.; Bahary, J.P.; Zietman, A.L.; et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N. Engl. J. Med. 2017, 376, 417–428. [Google Scholar] [CrossRef]
- Kerkmeijer, L.G.W.; Groen, V.H.; Pos, F.J.; Haustermans, K.; Monninkhof, E.M.; Smeenk, R.J.; Kunze-Busch, M.; de Boer, J.C.J.; van der Voort van Zijp, J.; van Vulpen, M.; et al. Focal Boost to the Intraprostatic Tumor in External Beam Radiotherapy for Patients with Localized Prostate Cancer: Results From the FLAME Randomized Phase III Trial. J. Clin. Oncol. 2021, 39, 787–796. [Google Scholar] [CrossRef]
- Cozzarini, C.; Fiorino, C.; Deantoni, C.; Briganti, A.; Fodor, A.; La Macchia, M.; Noris Chiorda, B.; Rancoita, P.M.; Suardi, N.; Zerbetto, F.; et al. Higher-than-expected severe (Grade 3–4) late urinary toxicity after postprostatectomy hypofractionated radiotherapy: A single-institution analysis of 1176 patients. Eur. Urol. 2014, 66, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Zilli, T.; Jorcano, S.; Peguret, N.; Caparrotti, F.; Hidalgo, A.; Khan, H.G.; Vees, H.; Weber, D.C.; Miralbell, R. Dose-adapted salvage radiotherapy after radical prostatectomy based on an erMRI target definition model: Toxicity analysis. Acta Oncol. 2014, 53, 96–102. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Overall |
|---|---|
| Patients, n (%) | 59 (100.0) |
| Follow-up (months) | 38.2 (29.0, 48.3) |
| KPS (%) | 90 (90, 100) |
| Age at SRT Start (years) | 71.1 (66.2, 76.3) |
| PSA at Primary Diagnosis (ng/mL) | 6.9 (5.4, 11.6) |
| PSA at Primary Diagnosis, n (%) | |
| <10 ng/mL | 33 (55.9) |
| 10–20 ng/mL | 12 (20.3) |
| >20 ng/mL | 7 (11.9) |
| N/A | 7 (11.9) |
| PSA at SRT Start (ng/mL) | 0.8 (0.4, 1.7) |
| Gleason Score | |
| ISUP Group 1 (≤6) | 15 (25.4) |
| ISUP Group 2 + 3 (7) | 27 (45.8) |
| ISUP Group 4 + 5 (≥8) | 16 (27.1) |
| N/A | 1 (1.7) |
| Postoperative Tumor Classification n (%) | |
| pT2b | 1 (1.7) |
| pT2c | 29 (49.2) |
| pT3a | 14 (23.7) |
| pT3b | 13 (22.0) |
| N/A | 2 (3.4) |
| Postoperative Nodal Status, n (%) | |
| Negative (pN0) | 52 (88.1) |
| Positive (pN1) | 5 (8.5) |
| N/A | 2 (3.4) |
| Postoperative Surgical Margin, n (%) | |
| Negative (R0) | 36 (61.0) |
| Positive (R1) | 16 (27.1) |
| N/A | 7 (11.9) |
| Initial D’Amico Risk Class, n (%) | |
| High | 57 (96.6) |
| N/A | 2 (3.4) |
| Imaging Method, n (%) | |
| PSMA PET/CT | 59 (100.0) |
| MRI | 37 (62.7) |
| Disease Pattern Before SRT, n (%) | |
| Prostatic fossa recurrence | 48 (81.4) |
| Prostatic fossa recurrence + locoregional LN metastasis | 11 (18.6) |
| Number of LN Metastases, n (%) | |
| 0 | 48 (81.4) |
| 1 | 4 (6.8) |
| 2 | 3 (5.1) |
| 3 | 2 (3.4) |
| ≥4 | 2 (3.4) |
| Time from Surgery to PSMA PET/CT (months) | 67.0 (37.4, 117.9) |
| Time from Surgery to SRT (months) | 68.1 (38.8, 119.3) |
| Treatment Characteristics | Overall |
|---|---|
| Concomitant ADT, n (%) | |
| ADT | 19 (32.2) |
| No ADT | 40 (67.8) |
| ADT duration (months) | 24.2 (15.4, 31.0) |
| SIB concept, n (%) | |
| Two dose levels | 31 (52.5) |
| Three dose levels | 28 (47.5) |
| Number of fractions | 33 (33, 33) |
| Prostate bed PTV dose (Gy) | 56.1 (56.1, 56.1) |
| Prostate bed PTVBoost1 dose (Gy) | 69.3 (69.3, 69.3) |
| Prostate bed PTVBoost2 dose (Gy) | 72.6 (72.6, 75.5) |
| Lymph node PTVBoostLN (Gy) | 66.9 (61.4, 69.3) |
| Biochemical Progression-Free Survival | Univariable | Multivariable | ||
| Variables | HR (95% CI) | p Value * | HR (95% CI) | p Value * |
| PSA at SRT Start (ng/mL) | 1.05 (0.80, 1.38) | 0.743 | ||
| Total Dose (Gy) | 1.08 (0.79, 1.48) | 0.644 | ||
| Time from RP to SRT (months) | 1.00 (0.99, 1.02) | 0.551 | 1.02 (1.00, 1.04) | 0.101 |
| Gleason Score ≥ 8 | ||||
| No | Ref | Ref | ||
| Yes | 2.95 (0.59, 14.65) | 0.186 | 11.44 (0.65, 202.39) | 0.096 |
| Concomitant ADT | ||||
| No | Ref | Ref | ||
| Yes | 2.33 (0.47, 11.57) | 0.300 | ||
| Postoperative Nodal Status | ||||
| Negative (pN0) | Ref | Ref | ||
| Positive (pN1) | 8.65 (1.50, 50.09) | 0.016 | 9.11 (1.24, 67.21) | 0.030 |
| Postoperative Surgical Margin | ||||
| Negative (R0) | Ref | Ref | ||
| Positive (R1) | 0.55 (0.06, 4.95) | 0.596 | ||
| Metastasis-free survival | Univariable | Multivariable | ||
| Variables | HR (95% CI) | p Value * | HR (95% CI) | p Value * |
| PSA at SRT Start (ng/mL) | 1.06 (0.73, 1.56) | 0.752 | ||
| Total Dose (Gy) | 1.13 (0.76, 1.67) | 0.533 | ||
| Time from RP to SRT (months) | 1.00 (0.99, 1.02) | 0.541 | 1.03 (1.01, 1.05) | 0.019 |
| Gleason Score ≥ 8 | ||||
| No | Ref | Ref | ||
| Yes | 5.31 (0.85, 33.08) | 0.074 | 19.25 (1.68, 221.11) | 0.018 |
| Concomitant ADT | ||||
| No | Ref | Ref | ||
| Yes | 1.37 (0.23, 8.22) | 0.730 | ||
| Postoperative Nodal Status | ||||
| Negative (pN0) | Ref | Ref | ||
| Positive (pN1) | 3.09 (0.34, 28.53) | 0.319 | ||
| Postoperative Surgical Margin | ||||
| Negative (R0) | Ref | Ref | ||
| Positive (R1) | 0.03 (0.00, 487.93) | 0.481 | ||
| Number of pts | RT Dose (Gy) | Median Follow-Up | bPFS | mPFS | OS | |
|---|---|---|---|---|---|---|
| Shelan [10] | 69 | 72–74 Gy | 38 mo | 5 y: 44% | 5 y: 76% | NA |
| Bruni [12] | 105 | >70 Gy: 58 pts 66–70 Gy: 43 pts < 66 Gy: 4 pts | 52 mo | 5 y: 69.7% | 5 y: 86.1% | 5 y: 85.5% |
| Zili [14] | 131 * | 64–74 Gy | 36 mo | 5 y: 45.6% | 5 y: 85.2% | 5 y: 92.5% |
| Zaine [13] | 89 | Median 70 Gy | 54 mo | 5 y: 50.8% | 5 y: 76.6% | 5 y: 90.2% |
| Lee [15] | 60 | Median 70.2 Gy | 83 mo | 7 y: 67.0% | 7 y: 83.6% | 7 y: 91.2% |
| Schmidt-Hegemann [18] | 30 ** | Median 70 Gy | 23 mo | 2 y: 78.0% | - | - |
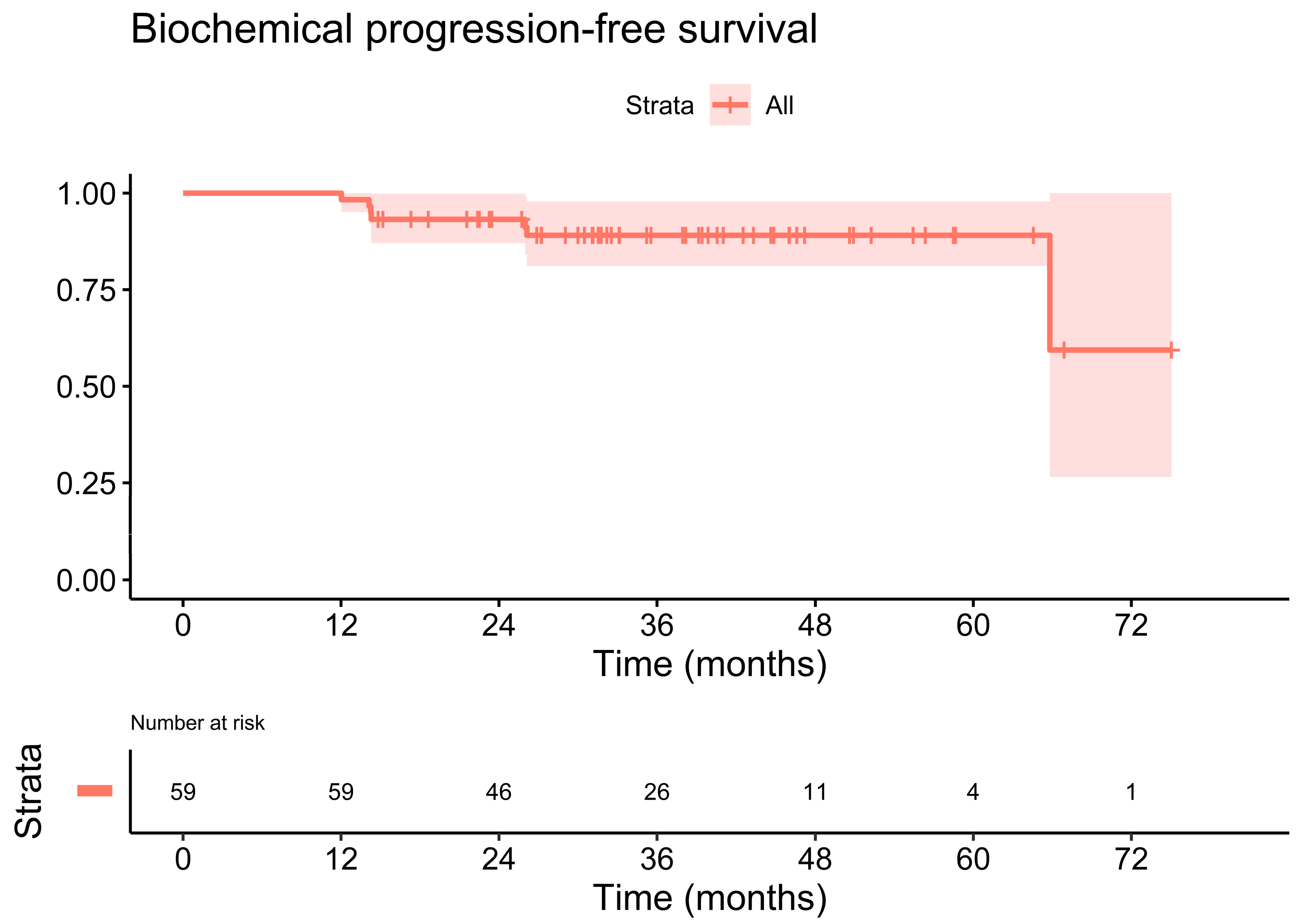
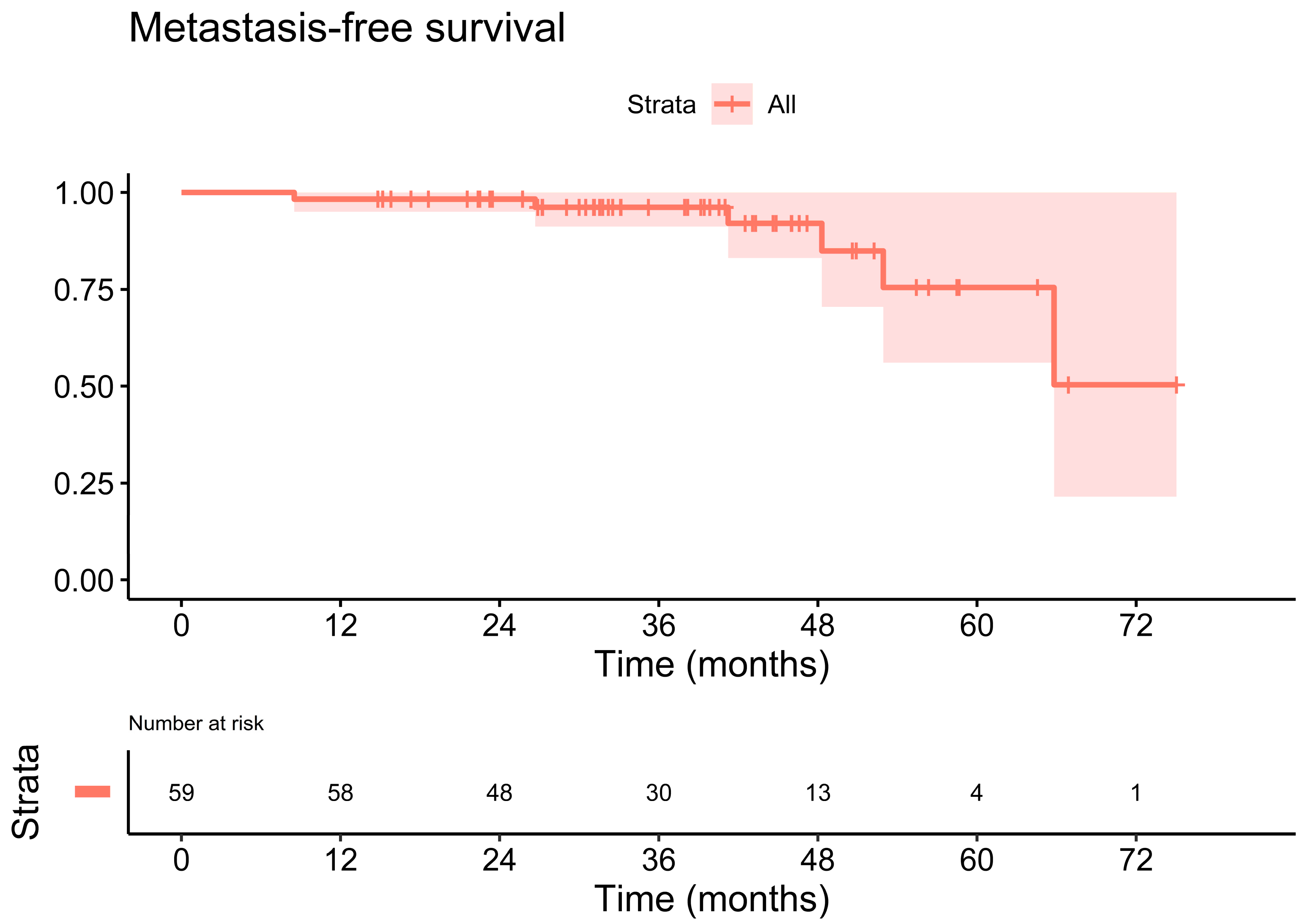
| Our series | 59 | Median 69.3 Gy | 38 mo | 3 y: 89.1% | 3 y: 96.2% | 3 y: 100.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamihardja, J.; Zehner, L.; Hartrampf, P.E.; Cirsi, S.; Wegener, S.; Buck, A.K.; Flentje, M.; Polat, B. Dose-Escalated Salvage Radiotherapy for Macroscopic Local Recurrence of Prostate Cancer in the Prostate-Specific Membrane Antigen Positron Emission Tomography Era. Cancers 2022, 14, 4956. https://doi.org/10.3390/cancers14194956
Tamihardja J, Zehner L, Hartrampf PE, Cirsi S, Wegener S, Buck AK, Flentje M, Polat B. Dose-Escalated Salvage Radiotherapy for Macroscopic Local Recurrence of Prostate Cancer in the Prostate-Specific Membrane Antigen Positron Emission Tomography Era. Cancers. 2022; 14(19):4956. https://doi.org/10.3390/cancers14194956
Chicago/Turabian StyleTamihardja, Jörg, Leonie Zehner, Philipp E. Hartrampf, Sinan Cirsi, Sonja Wegener, Andreas K. Buck, Michael Flentje, and Bülent Polat. 2022. "Dose-Escalated Salvage Radiotherapy for Macroscopic Local Recurrence of Prostate Cancer in the Prostate-Specific Membrane Antigen Positron Emission Tomography Era" Cancers 14, no. 19: 4956. https://doi.org/10.3390/cancers14194956
APA StyleTamihardja, J., Zehner, L., Hartrampf, P. E., Cirsi, S., Wegener, S., Buck, A. K., Flentje, M., & Polat, B. (2022). Dose-Escalated Salvage Radiotherapy for Macroscopic Local Recurrence of Prostate Cancer in the Prostate-Specific Membrane Antigen Positron Emission Tomography Era. Cancers, 14(19), 4956. https://doi.org/10.3390/cancers14194956