

Risk of Cardiovascular Disease Death in Older Malignant Melanoma Patients: A Population-Based Study

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Population and Data Collection
2.3. Study Design and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Malignant Melanoma Patients’ CVD Risk Compared to the General Population
3.3. Causes of Death in Malignant Melanoma Patients
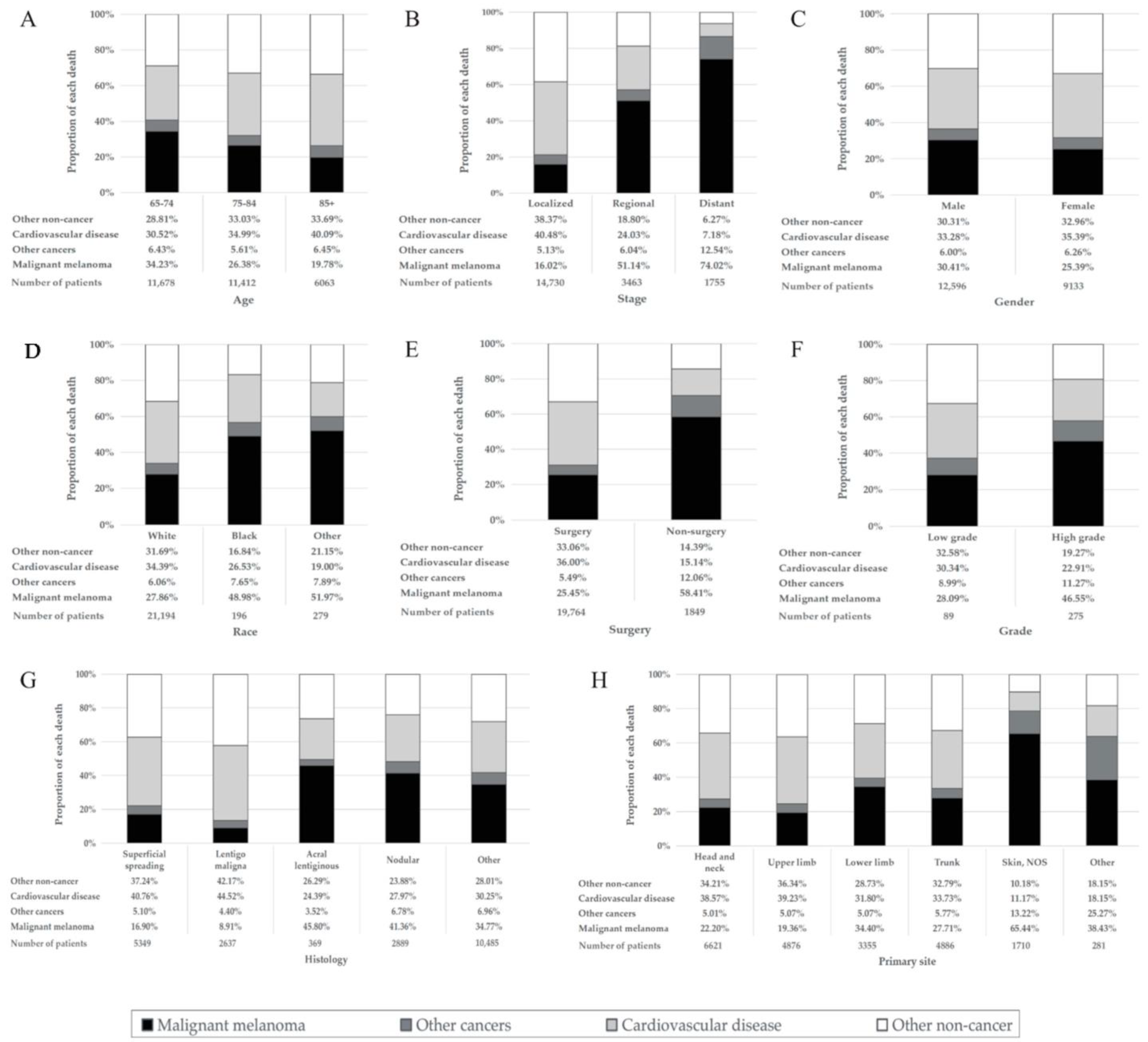
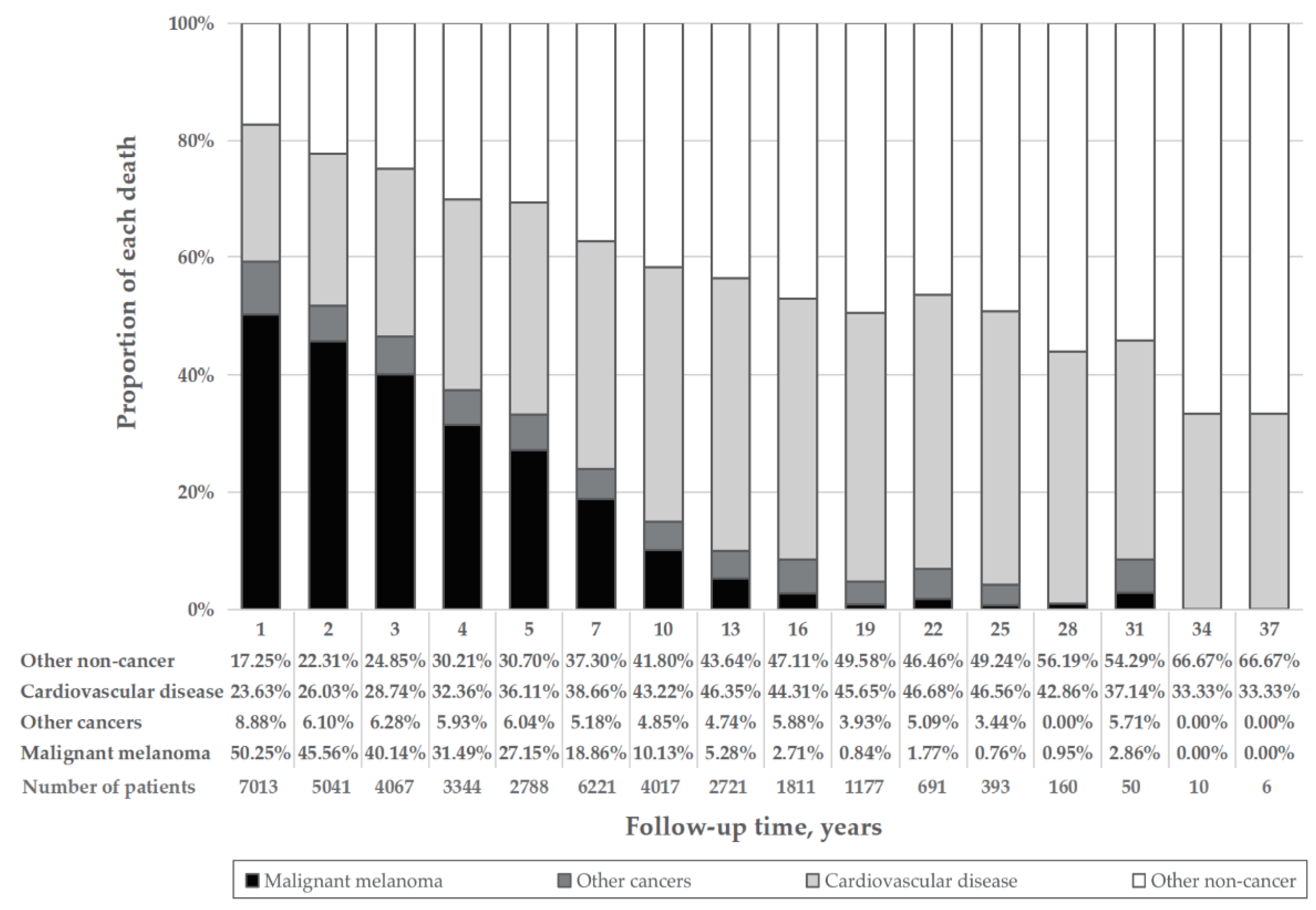
3.4. Subgroup Analysis of Proportion of Deaths
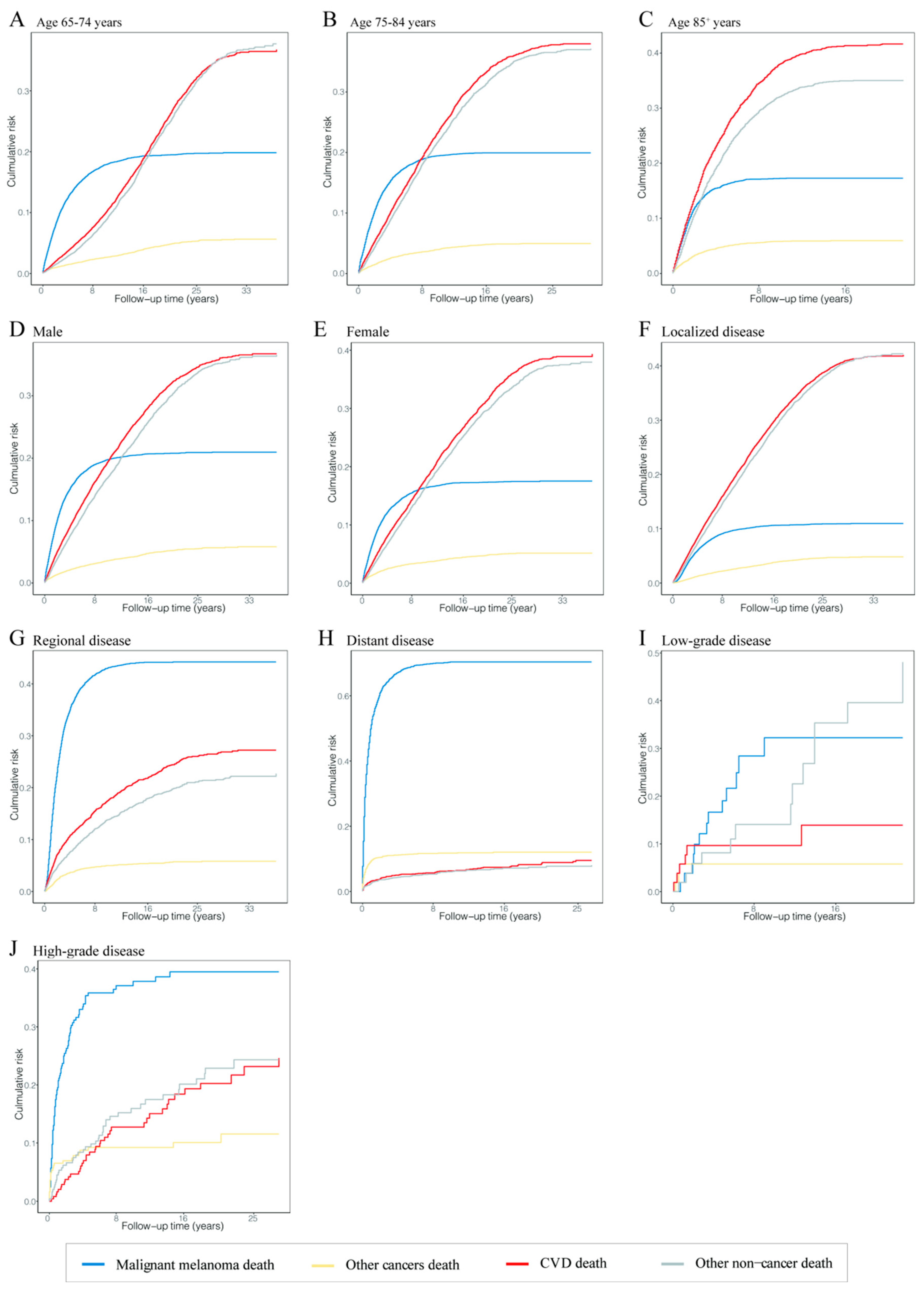
3.5. Cumulative Mortality in Malignant Melanoma Patients
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Welch, H.G.; Mazer, B.L.; Adamson, A.S. The Rapid Rise in Cutaneous Melanoma Diagnoses. N. Engl. J. Med. 2021, 384, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Strongman, H.; Gadd, S.; Matthews, A.; Mansfield, K.E.; Stanway, S.; Lyon, A.R.; Dos-Santos-Silva, I.; Smeeth, L.; Bhaskaran, K. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: A population-based cohort study using multiple linked UK electronic health records databases. Lancet 2019, 394, 1041–1054. [Google Scholar] [CrossRef]
- Horn, S.; Stoltzfus, K.; Mackley, H.; Lehrer, E.; Zhou, S.; Dandekar, S.; Fox, E.; Rizk, E.; Trifiletti, D.; Rao, P.; et al. Long-term causes of death among pediatric patients with cancer. Cancer 2020, 126, 3102–3113. [Google Scholar] [CrossRef]
- Zaorsky, N.; Churilla, T.; Egleston, B.; Fisher, S.; Ridge, J.; Horwitz, E.; Meyer, J. Causes of death among cancer patients. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 400–407. [Google Scholar] [CrossRef]
- Papadopoulos, F. Suicide and cardiovascular death after a cancer diagnosis. N. Engl. J. Med. 2012, 367, 276–277. [Google Scholar] [CrossRef]
- Schadendorf, D.; Fisher, D.E.; Garbe, C.; Gershenwald, J.E.; Grob, J.J.; Halpern, A.; Herlyn, M.; Marchetti, M.A.; McArthur, G.; Ribas, A.; et al. Melanoma. Nat. Rev. Dis. Primers 2015, 1, 15003. [Google Scholar] [CrossRef]
- Ijaz, N.; Buta, B.; Xue, Q.L.; Mohess, D.T.; Bushan, A.; Tran, H.; Batchelor, W.; deFilippi, C.R.; Walston, J.D.; Bandeen-Roche, K.; et al. Interventions for Frailty Among Older Adults With Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 482–503. [Google Scholar] [CrossRef]
- Bronte, E.; Bronte, G.; Novo, G.; Rinaldi, G.; Bronte, F.; Passiglia, F.; Russo, A. Cardiotoxicity mechanisms of the combination of BRAF-inhibitors and MEK-inhibitors. Pharmacol. Ther. 2018, 192, 65–73. [Google Scholar] [CrossRef]
- Salem, J.E.; Manouchehri, A.; Moey, M.; Lebrun-Vignes, B.; Bastarache, L.; Pariente, A.; Gobert, A.; Spano, J.P.; Balko, J.M.; Bonaca, M.P.; et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: An observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018, 19, 1579–1589. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef] [PubMed]
- Inno, A.; Maurea, N.; Metro, G.; Carbone, A.; Russo, A.; Gori, S. Immune checkpoint inhibitors-associated pericardial disease: A systematic review of case reports. Cancer Immunol. Immunother. 2021, 70, 3041–3053. [Google Scholar] [CrossRef] [PubMed]
- Elshanbary, A.; Zaazouee, M.; Abdelmonem, M.; Mohammed, Y.; Abdel-Aziz, W. Risk factors for cardiovascular mortality and melanoma-specific mortality among patients with melanoma: A SEER based study. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. (ECP) 2021, 31, 293–300. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. SEER Data & Software. Available online: https://seer.cancer.gov/data-software/ (accessed on 23 June 2022).
- Centers for Disease Control and Prevention. About Multiple Cause of Death, 1999–2020. Available online: https://wonder.cdc.gov/mcd-icd10.html (accessed on 23 June 2022).
- Weberpals, J.; Jansen, L.; Muller, O.J.; Brenner, H. Long-term heart-specific mortality among 347 476 breast cancer patients treated with radiotherapy or chemotherapy: A registry-based cohort study. Eur. Heart J. 2018, 39, 3896–3903. [Google Scholar] [CrossRef]
- Nam, H.S.; Kim, H.C.; Kim, Y.D.; Lee, H.S.; Kim, J.; Lee, D.H.; Heo, J.H. Long-term mortality in patients with stroke of undetermined etiology. Stroke 2012, 43, 2948–2956. [Google Scholar] [CrossRef]
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. SEER Research Plus Data Description Cases Diagnosed in 1975–2018. Available online: https://seer.cancer.gov/data-software/documentation/seerstat/nov2020/TextData.FileDescription.pdf (accessed on 23 June 2022).
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. Dictionary of SEER*Stat Variables. Available online: https://seer.cancer.gov/data-software/documentation/seerstat/nov2020/seerstat-variable-dictionary-nov2020.pdf (accessed on 23 June 2022).
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. SEER Cause of Death Recode 1969+ (03/01/2018) SEER Data Reporting Tools. Available online: https://seer.cancer.gov/codrecode/1969_d03012018/index.html (accessed on 23 June 2022).
- Abdel-Qadir, H.; Austin, P.C.; Lee, D.S.; Amir, E.; Tu, J.V.; Thavendiranathan, P.; Fung, K.; Anderson, G.M. A Population-Based Study of Cardiovascular Mortality Following Early-Stage Breast Cancer. JAMA Cardiol. 2017, 2, 88–93. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. How to obtain the P value from a confidence interval. BMJ 2011, 343, d2304. [Google Scholar] [CrossRef]
- Breslow, N.E.; Day, N.E.; Heseltine, E. Statistical Methods in Cancer Research. Volume II—The Design and Analysis of Cohort Studies; IARC Scientific Publications: Geneva, Switzerland, 1987; pp. 1–406. [Google Scholar]
- Estève, J.; Benhamou, E.; Raymond, L. Statistical Methods in Cancer Research. Volume IV. Descriptive Epidemiology; IARC Scientific Publications: Geneva, Switzerland, 1994; pp. 1–302. [Google Scholar]
- Sturgeon, K.M.; Deng, L.; Bluethmann, S.M.; Zhou, S.; Trifiletti, D.M.; Jiang, C.; Kelly, S.P.; Zaorsky, N.G. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur. Heart J. 2019, 40, 3889–3897. [Google Scholar] [CrossRef]
- Rees, M.; Liao, H.; Spillane, J.; Speakman, D.; McCormack, C.; Donahoe, S.; Pohl, M.; Webb, A.; Gyorki, D.; Henderson, M. Melanoma in the very elderly, management in patients 85years of age and over. J. Geriatr. Oncol. 2018, 9, 488–493. [Google Scholar] [CrossRef]
- Abdel-Rahman, O. Risk of cardiac death among cancer survivors in the United States: A SEER database analysis. Expert Rev. Anticancer Ther. 2017, 17, 873–878. [Google Scholar] [CrossRef]
- Weilandt, J.; Diehl, K.; Schaarschmidt, M.L.; Kiecker, F.; Sasama, B.; Pronk, M.; Ohletz, J.; Konnecke, A.; Muller, V.; Utikal, J.; et al. Patient preferences for treatment of advanced melanoma: Impact of comorbidities. J. Dtsch. Dermatol. Ges. 2021, 19, 58–70. [Google Scholar] [CrossRef]
- Lau, B.; Cole, S.; Gange, S. Competing risk regression models for epidemiologic data. Am. J. Epidemiol. 2009, 170, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Stoltzfus, K.C.; Zhang, Y.; Sturgeon, K.; Sinoway, L.I.; Trifiletti, D.M.; Chinchilli, V.M.; Zaorsky, N.G. Fatal heart disease among cancer patients. Nat. Commun. 2020, 11, 2011. [Google Scholar] [CrossRef]
- Crocetti, E.; Fancelli, L.; Manneschi, G.; Caldarella, A.; Pimpinelli, N.; Chiarugi, A.; Nardini, P.; Buzzoni, C. Melanoma survival: Sex does matter, but we do not know how. Eur. J. Cancer Prev. 2016, 25, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Kindem, S.; Garcias-Ladaria, J.; Requena, C.; Guillen, C.; Oliver, V.; Nagore, E. Survival advantage of women in localized melanoma mainly relies on clinical-pathological differences by sex. A retrospective study of 1607 patients in Valencia, Spain. Eur. J. Dermatol. 2015, 25, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Joosse, A.; De Vries, E.; van Eijck, C.H.; Eggermont, A.M.; Nijsten, T.; Coebergh, J.W. Reactive oxygen species and melanoma: An explanation for gender differences in survival? Pigment Cell Melanoma Res. 2010, 23, 352–364. [Google Scholar] [CrossRef]
- Davis, L.E.; Shalin, S.C.; Tackett, A.J. Current state of melanoma diagnosis and treatment. Cancer Biol. Ther. 2019, 20, 1366–1379. [Google Scholar] [CrossRef]
- Michel, L.; Helfrich, I.; Hendgen-Cotta, U.B.; Mincu, R.I.; Korste, S.; Mrotzek, S.M.; Spomer, A.; Odersky, A.; Rischpler, C.; Herrmann, K.; et al. Targeting early stages of cardiotoxicity from anti-PD1 immune checkpoint inhibitor therapy. Eur. Heart J. 2022, 43, 316–329. [Google Scholar] [CrossRef]
- Quagliariello, V.; Passariello, M.; Coppola, C.; Rea, D.; Barbieri, A.; Scherillo, M.; Monti, M.G.; Iaffaioli, R.V.; De Laurentiis, M.; Ascierto, P.A.; et al. Cardiotoxicity and pro-inflammatory effects of the immune checkpoint inhibitor Pembrolizumab associated to Trastuzumab. Int. J. Cardiol. 2019, 292, 171–179. [Google Scholar] [CrossRef]
- Quagliariello, V.; Passariello, M.; Rea, D.; Barbieri, A.; Iovine, M.; Bonelli, A.; Caronna, A.; Botti, G.; De Lorenzo, C.; Maurea, N. Evidences of CTLA-4 and PD-1 Blocking Agents-Induced Cardiotoxicity in Cellular and Preclinical Models. J. Pers. Med. 2020, 10, 179. [Google Scholar] [CrossRef]
- Mukunda, N.; Vallabhaneni, S.; Lefebvre, B.; Fradley, M.G. Cardiotoxicity of Systemic Melanoma Treatments. Curr. Treat. Opt. Oncol. 2022, 23, 240–253. [Google Scholar] [CrossRef] [PubMed]
- Arangalage, D.; Degrauwe, N.; Michielin, O.; Monney, P.; Ozdemir, B.C. Pathophysiology, diagnosis and management of cardiac toxicity induced by immune checkpoint inhibitors and BRAF and MEK inhibitors. Cancer Treat. Rev. 2021, 100, 102282. [Google Scholar] [CrossRef] [PubMed]
- Heinzerling, L.; Ott, P.A.; Hodi, F.S.; Husain, A.N.; Tajmir-Riahi, A.; Tawbi, H.; Pauschinger, M.; Gajewski, T.F.; Lipson, E.J.; Luke, J.J. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J. Immunother. Cancer 2016, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Bentebibel, S.E.; Diab, A. Cytokines in the Treatment of Melanoma. Curr. Oncol. Rep. 2021, 23, 83. [Google Scholar] [CrossRef]
- Fang, S.; Xu, T.; Xiong, M.; Zhou, X.; Wang, Y.; Haydu, L.E.; Ross, M.I.; Gershenwald, J.E.; Prieto, V.G.; Cormier, J.N.; et al. Role of Immune Response, Inflammation, and Tumor Immune Response-Related Cytokines/Chemokines in Melanoma Progression. J. Investig. Dermatol. 2019, 139, 2352–2358. [Google Scholar] [CrossRef]
- Tobin, R.P.; Jordan, K.R.; Kapoor, P.; Spongberg, E.; Davis, D.; Vorwald, V.M.; Couts, K.L.; Gao, D.; Smith, D.E.; Borgers, J.S.W.; et al. IL-6 and IL-8 Are Linked with Myeloid-Derived Suppressor Cell Accumulation and Correlate with Poor Clinical Outcomes in Melanoma Patients. Front. Oncol. 2019, 9, 1223. [Google Scholar] [CrossRef]
- Lavi, G.; Voronov, E.; Dinarello, C.A.; Apte, R.N.; Cohen, S. Sustained delivery of IL-1 Ra from biodegradable microspheres reduces the number of murine B16 melanoma lung metastases. J. Control. Release 2007, 123, 123–130. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. of MM Patient (% in the Overall Cohort) | No. of Deaths (% in the Overall Deaths) | No. Alive (% in the Overall Alive) |
|---|---|---|---|
| All patients | 39,510 | 21,729 | 17,781 |
| Cause of death | |||
| Malignant Melanoma | NA | 6149 (28.3) | NA |
| Other cancers | NA | 1328 (6.1) | NA |
| CVD | NA | 7424 (34.2) | NA |
| Other noncancer a | NA | 6828 (31.4) | NA |
| Diagnostic age (y) | |||
| 65–74 | 20,674 (52.3) | 8947 (41.2) | 11,727 (66.0) |
| 75–84 | 13,229 (33.5) | 8454 (38.9) | 4775 (26.8) |
| 85+ | 5607 (14.2) | 4328 (19.9) | 1279 (7.2) |
| Gender | |||
| Male | 23,030 (58.3) | 12,596 (58.0) | 10,434 (58.7) |
| Female | 16480 (41.7) | 9133 (42.0) | 7347 (41.3) |
| Race | |||
| White | 37,993 (96.2) | 21,194 (97.5) | 16,799 (94.5) |
| Black | 246 (0.6) | 196 (0.9) | 50 (0.3) |
| Other b | 449 (1.2) | 279 (1.3) | 170 (1.0) |
| Unknown | 822 (2.0) | 60 (0.3) | 762 (4.2) |
| Stage | |||
| Localized | 25,182 (63.7) | 14,730 (67.8) | 10,452 (58.8) |
| Regional | 4143 (10.5) | 3463 (15.9) | 680 (3.8) |
| Distant | 1861 (4.7) | 1755 (7.1) | 106 (0.6) |
| Unknown | 8324 (21.1) | 1781 (8.2) | 6543 (36.8) |
| Grade | |||
| Low (Grade I+II) | 35,667 (90.3) | 18,563 (85.4) | 17,104 (96.2) |
| High (Grade III+IV) | 3843 (9.7) | 3166 (14.6) | 677 (3.8) |
| Surgery | |||
| Yes | 36,632 (92.7) | 19,764 (91.0) | 16,868 (94.9) |
| No | 2622 (6.6) | 1849 (8.5) | 773 (4.3) |
| Unknown | 256 (0.7) | 116 (0.5) | 140 (0.8) |
| Characteristic | No. of General Population (% in the General Population) | No. of Deaths (% in the Overall Deaths) | No. Alive (% in the Overall Alive) |
|---|---|---|---|
| All populations | 40,267,984 | 631,573 | 39,636,411 |
| Age (y) | |||
| 65–74 | 21,713,429 (53.9) | 114,483 (18.1) | 21,598,946 (54.5) |
| 75–84 | 13,061,122 (32.4) | 205,180 (32.5) | 12,855,942 (32.4) |
| 85+ | 5,493,433 (13.6) | 311,910 (49.4) | 5,181,523 (13.1) |
| Gender | |||
| Male | 17,362,960 (43.1) | 282,694 (44.8) | 17,080,266 (43.1) |
| Female | 22,905,024 (56.9) | 348,879 (55.2) | 22,556,145 (56.9) |
| Race | |||
| White | 34,971,197 (86.8) | 556,057 (88.0) | 34,415,140 (86.8) |
| Black | 3,541,901 (8.8) | 60,048 (9.5) | 3,481,853 (8.8) |
| Other a | 1,754,886 (4.4) | 15,468 (2.5) | 1,739,418 (4.4) |
| Characteristic | Overall Cohort | Surgery Cohort | Nonsurgery Cohort | |||
|---|---|---|---|---|---|---|
| SMR (95% CI) | p Value a | SMR (95% CI) | p Value a | SMR (95% CI) | p Value a | |
| Overall | 1.98 (1.93–2.03) | ˂0.001 | 1.98 (1.93–2.03) | ˂0.001 | 2.47 (2.19–2.78) | ˂ 0.001 |
| Diagnostic age (y) | ||||||
| 65–74 | 3.09 (2.98–3.21) | ˂0.001 | 3.09 (2.98–3.21) | ˂0.001 | 4.61 (3.69–5.70) | ˂0.001 |
| 75–84 | 1.30 (1.25–1.34) | ˂0.001 | 1.29 (1.24–1.34) | ˂0.001 | 2.36 (1.92–2.87) | ˂0.001 |
| 85+ | 1.27 (1.21–1.33) | ˂0.001 | 1.25 (1.19–1.32) | ˂0.001 | 1.72 (1.39–2.11) | ˂0.001 |
| Gender | ||||||
| Male | 2.00 (1.94–2.06) | ˂0.001 | 1.99 (1.93–2.05) | ˂0.001 | 2.31 (1.96–2.70) | ˂0.001 |
| Female | 1.95 (1.88–2.02) | ˂0.001 | 1.93 (1.87–2.00) | ˂0.001 | 2.66 (2.21–3.17) | ˂0.001 |
| Race | ||||||
| White | 1.99 (1.94–2.03) | ˂0.001 | 1.97 (1.92–2.02) | ˂0.001 | 2.54 (2.25–2.86) | ˂0.001 |
| Black | 2.77 (2.07–3.63) | ˂0.001 | 2.87 (2.13–3.78) | ˂0.001 | 2.23 (0.25–8.06) | 0.370 |
| Other b | 3.13 (2.35–4.10) | ˂0.001 | 3.11 (2.31–4.10) | ˂0.001 | 3.75 (0.75–10.97) | 0.052 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miao, J.; Wang, Y.; Gu, X.; Lin, W.; Ouyang, Z.; Wang, M.; Chen, M.; Zhao, S.; Wang, X.; Su, J. Risk of Cardiovascular Disease Death in Older Malignant Melanoma Patients: A Population-Based Study. Cancers 2022, 14, 4783. https://doi.org/10.3390/cancers14194783
Miao J, Wang Y, Gu X, Lin W, Ouyang Z, Wang M, Chen M, Zhao S, Wang X, Su J. Risk of Cardiovascular Disease Death in Older Malignant Melanoma Patients: A Population-Based Study. Cancers. 2022; 14(19):4783. https://doi.org/10.3390/cancers14194783
Chicago/Turabian StyleMiao, Jiapeng, Yujie Wang, Xiaoyu Gu, Wenrui Lin, Zhen Ouyang, Mi Wang, Mingliang Chen, Shuang Zhao, Xianggui Wang, and Juan Su. 2022. "Risk of Cardiovascular Disease Death in Older Malignant Melanoma Patients: A Population-Based Study" Cancers 14, no. 19: 4783. https://doi.org/10.3390/cancers14194783
APA StyleMiao, J., Wang, Y., Gu, X., Lin, W., Ouyang, Z., Wang, M., Chen, M., Zhao, S., Wang, X., & Su, J. (2022). Risk of Cardiovascular Disease Death in Older Malignant Melanoma Patients: A Population-Based Study. Cancers, 14(19), 4783. https://doi.org/10.3390/cancers14194783