

Feasibility, Method and Early Outcome of Image-Guided Volumetric Modulated Arc Radiosurgery Followed by Resection for AJCC Stage IIA–IIIB High-Risk Large Intraocular Melanoma

 , , , , ,
, , , , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Eligibility
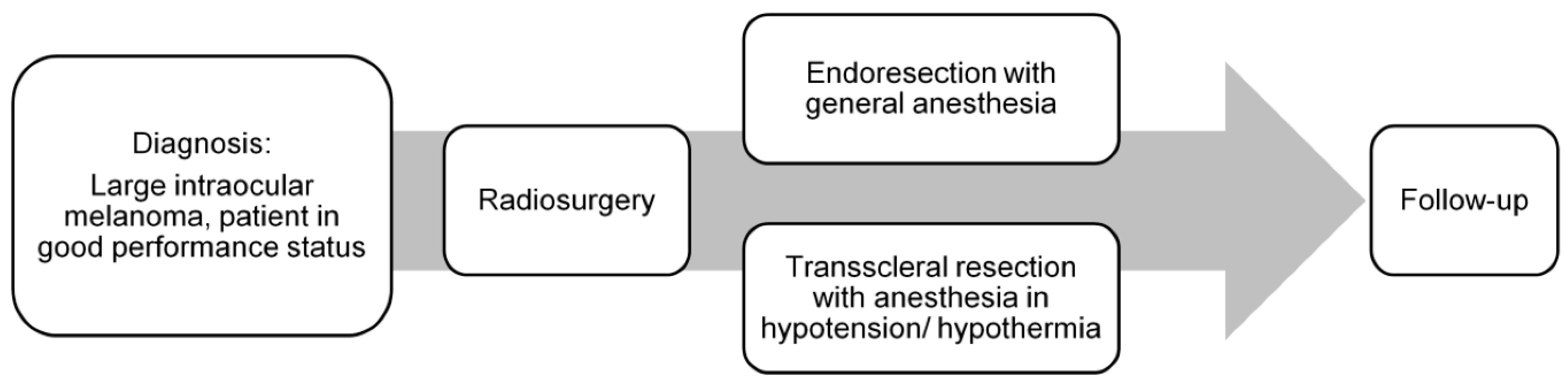
2.2. Treatment Schedule
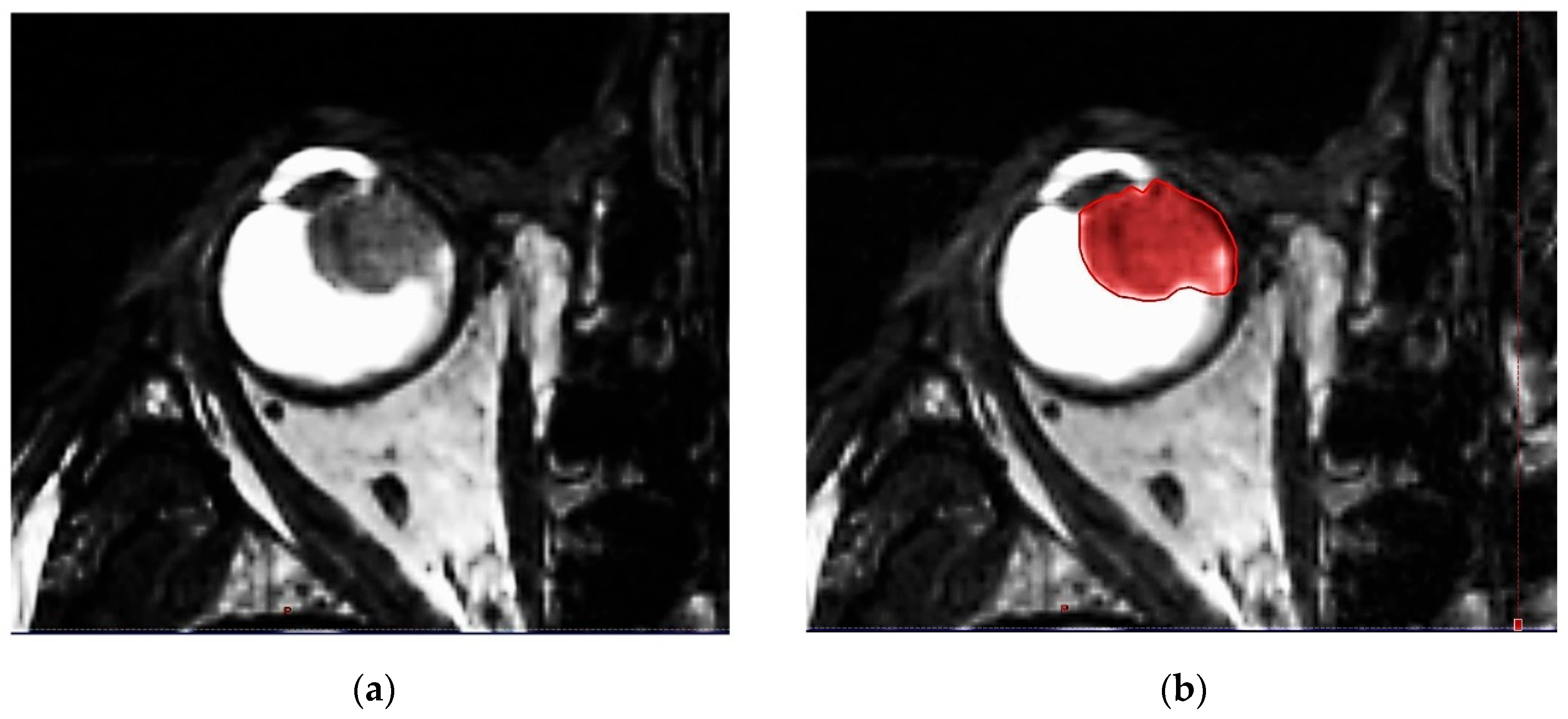
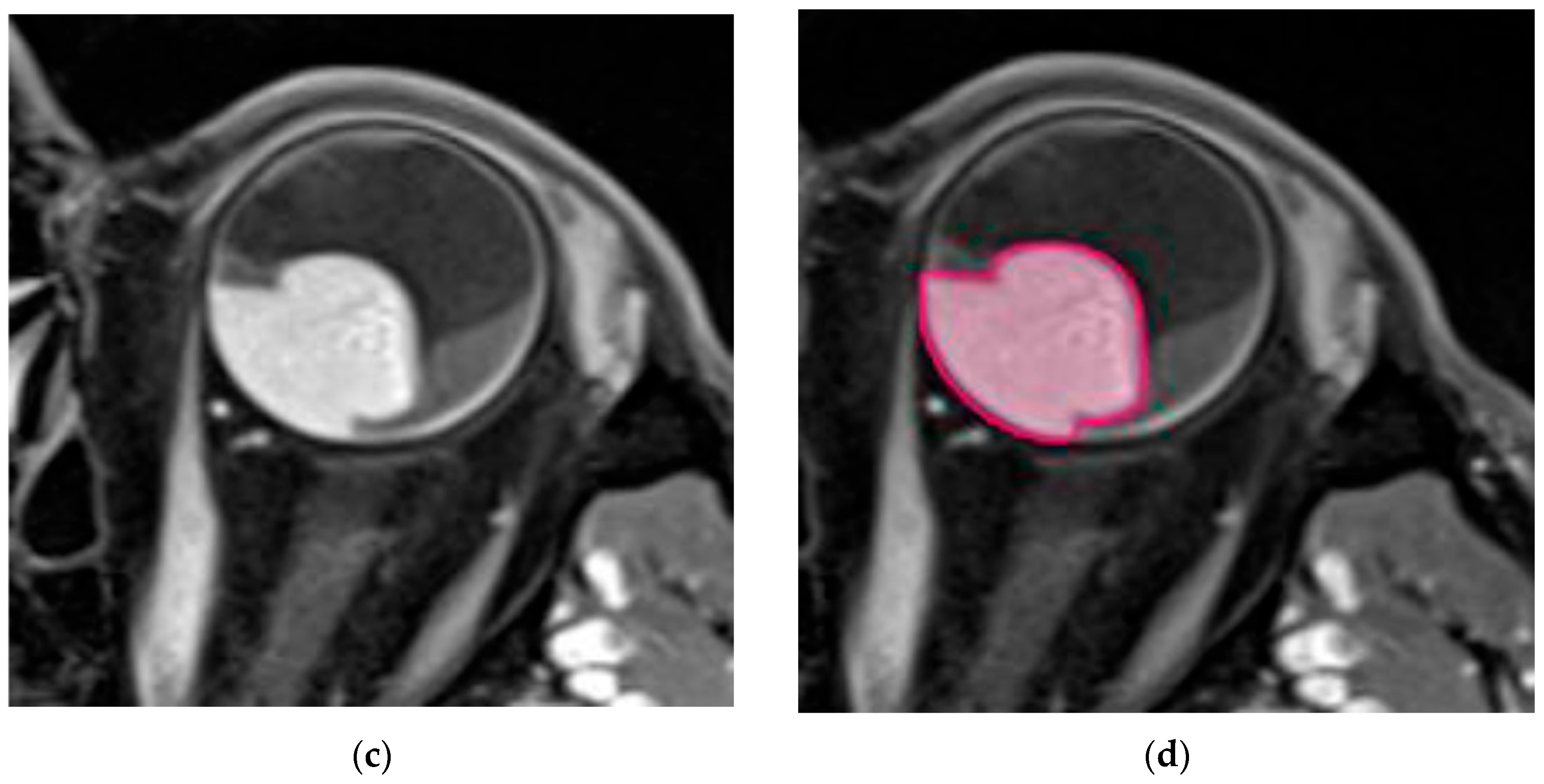
2.3. Treatment Planning, Part 1: Imaging, Target Definition and Treatment Set-Up
2.4. Treatment Planning, Part 2: External Beam Planning, Dose Metrics and Quality Control
2.5. Pre-Treatment Preparation, Immobilization Devices and Technique
2.6. Treatment, Image Guidance
2.7. Histopathology and Tumor Characterization
2.8. Follow-Up
3. Results
4. Discussion
5. Conclusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Force, T.; Simpson, E.R.; Gallie, B.; Laperrierre, N.; Beiki-Ardakani, A.; Kivelä, T.; Raivio, V.; Heikkonen, J.; Desjardins, L.; Dendale, R.; et al. The american brachytherapy society consensus guidelines for plaque brachytherapy of uveal melanoma and retinoblastoma. Brachytherapy 2014, 13, 1–14. [Google Scholar]
- Papakostas, T.D.; Lane, A.M.; Morrison, M.; Gragoudas, E.S.; Kim, I.K. Long-term outcomes after proton beam irradiation in patients with large choroidal melanomas. JAMA Ophthalmol. 2017, 135, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, L.; Kivelä, T.; Damato, B.E.; Jager, M.J. (Eds.) Current concepts in uveal melanoma. In Developments in Ophthalmology; Karger: Basel, Switzerland, 2012; Volume 49, pp. 182–186. [Google Scholar]
- Bechrakis, N.E.; Petousis, V.; Willerding, G.; Krause, L.; Wachtlin, J.; Stroux, A.; Foerster, M.H. Ten-year results of transscleral resection of large uveal melanomas: Local tumour control and metastatic rate. Br. J. Ophthalmol. 2010, 94, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Damato, B.E.; Paul, J.; Foulds, W.S. Risk factors for residual and recurrent uveal melanoma after trans-scleral local resection. Br. J. Ophthalmol. 1996, 80, 102–108. [Google Scholar] [CrossRef]
- Bechrakis, N.E.; Höcht, S.; Martus, P.; Kreusel, K.M.; Heese, J.; Foerster, M.H. Endoresektion von großen uvealen melanomen nach protonenbestrahlung. Der Ophthalmol. 2004, 101, 370–376. [Google Scholar] [CrossRef]
- Bechrakis, N.E.; Blatsios, G.; Schmid, E.; Petousis, V.; Willerding, G.; Foerster, M.H. Die behandlung von großen aderhautmelanomen durch chirurgische exzisionsverfahren. Spektrum Der Augenheilkd. 2010, 24, 17–22. [Google Scholar] [CrossRef]
- Kocher, M.; Wittig, A.; Piroth, M.D.; Treuer, H.; Seegenschmiedt, H.; Ruge, M.; Grosu, A.L.; Guckenberger, M. Stereotactic radiosurgery for treatment of brain metastases. A report of the degro working group on stereotactic radiotherapy. Strahlenther. Onkol. 2014, 190, 521–532. [Google Scholar] [CrossRef]
- Kosydar, S.; Robertson, J.C.; Woodfin, M.; Mayr, N.A.; Sahgal, A.; Timmerman, R.D.; Lo, S.S. Systematic review and meta-analysis on the use of photon-based stereotactic radiosurgery versus fractionated stereotactic radiotherapy for the treatment of uveal melanoma. Am. J. Clin. Oncol. 2021, 44, 32–42. [Google Scholar] [CrossRef]
- Hazelaar, C.; Dahele, M.; Mostafavi, H.; van der Weide, L.; Slotman, B.J.; Verbakel, W.F. Subsecond and submillimeter resolution positional verification for stereotactic irradiation of spinal lesions. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 1154–1162. [Google Scholar] [CrossRef]
- Ruschin, M.; Sahgal, A.; Soliman, H.; Myrehaug, S.; Tseng, C.-L.; Bola, R.; Yeboah, C.; Sarfehnia, A.; Chugh, B.; Eriksson, M.; et al. Clinical image coregistration variability on a dedicated radiosurgery unit. Neurosurgery 2019, 85, E101–E108. [Google Scholar] [CrossRef]
- Ciernik, I.F.; Wösle, M.; Krause, L.; Krayenbuehl, J. Optimizing radiosurgery with photons for ocular melanoma. Phys. Imaging Radiat. Oncol. 2018, 6, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Parker, T.; Rigney, G.; Kallos, J.; Stefko, S.T.; Kano, H.; Niranjan, A.; Green, A.L.; Aziz, T.; Rath, P.; Lunsford, L.D. Gamma knife radiosurgery for uveal melanomas and metastases: A systematic review and meta-analysis. Lancet Oncol. 2020, 21, 1526–1536. [Google Scholar] [CrossRef]
- Smyth, G.; Evans, P.M.; Bamber, J.C.; Bedford, J.L. Recent developments in non-coplanar radiotherapy. Br. J. Radiol. 2019, 92, 20180908. [Google Scholar] [CrossRef]
- Biewald, E.; Lautner, H.; Gök, M.; Horstmann, G.A.; Sauerwein, W.; Flühs, D.; Bornfeld, N. Endoresection of large uveal melanomas: Clinical results in a consecutive series of 200 cases. Br. J. Ophthalmol. 2017, 101, 204–208. [Google Scholar] [CrossRef]
- Furdova, A.; Strmen, P.; Waczulikova, I.; Chorvath, M.; Sramka, M.; Slezak, P. One-day session linac-based stereotactic radiosurgery of posterior uveal melanoma. Eur. J. Ophthalmol. 2012, 22, 226–235. [Google Scholar] [CrossRef]
- Skinner, C.C.; Augsburger, J.J.; Augsburger, B.D.; Correa, Z.M. Comparison of alternative tumor size classifications for posterior uveal melanomas. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3335–3342. [Google Scholar] [CrossRef] [PubMed]
- Honavar, S.G. Is collaborative ocular melanoma study (coms) still relevant? Indian J. Ophthalmol. 2018, 66, 1385–1387. [Google Scholar] [CrossRef]
- ACR–AAPM Technical Standard for Medical Physics Performance Monitoring of Stereotactic Body Radiation Therapy (SBRT). Available online: https://www.acr.org/Clinical-Resources/Practice-Parameters-and-Technical-Standards (accessed on 6 February 2022).
- Chao, S.T.; Dad, L.K.; Dawson, L.A.; Desai, N.B.; Pacella, M.; Rengan, R.; Xiao, Y.; Yenice, K.M.; Rosenthal, S.A.; Hartford, A. Acr-astro practice parameter for the performance of stereotactic body radiation therapy. Am. J. Clin. Oncol. 2020, 43, 545–552. [Google Scholar] [CrossRef]
- Brainlab AG, O.-P.-S., 81829. Munich, Germany. Frameless Radiosurgery Mask System by Brainlab®. Available online: https://www.brainlab.com/radiosurgery-products/exactrac-x-ray/ (accessed on 23 August 2022).
- Multi-Institutional Target Delineation in Oncology Group. Human-computer interaction in radiotherapy target volume delineation: A prospective, multi-institutional comparison of user input devices. J. Digit. Imaging 2011, 24, 794–803. [Google Scholar] [CrossRef]
- McShan, D.L.; Matrone, G.; Fraass, B.A.; Lichter, A.S. A large screen digitizer system for radiation therapy treatment planning. Int. J. Radiat. Oncol. Biol. Phys. 1993, 26, 681–684. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (sabr-comet): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Brainlab AG, O.-P.-S., 81829 Munich, Germany. Available online: https://userguides.brainlab.com/de/guides/cranial-srs/ (accessed on 23 August 2022).
- Kalantzis, G.; Qian, J.; Han, B.; Luxton, G. Fidelity of dose delivery at high dose rate of volumetric modulated arc therapy in a truebeam linac with flattening filter free beams. J. Med. Phys. 2012, 37, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Brainlab AG, O.-P.-S., 81829, Munich. Available online: https://www.brainlab.com/radiosurgery-products/elements/ (accessed on 23 August 2022).
- Reynolds, T.A.; Jensen, A.R.; Bellairs, E.E.; Ozer, M. Dose gradient index for stereotactic radiosurgery/radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 604–611. [Google Scholar] [CrossRef]
- Jeraj, R.; Keall, P.J.; Siebers, J.V. The effect of dose calculation accuracy on inverse treatment planning. Phys. Med. Biol. 2002, 47, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (ctcae) v5.0, 27 November 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 15 August 2022).
- Weber, D.C.; Bogner, J.; Verwey, J.; Georg, D.; Dieckmann, K.; Escudé, L.; Caro, M.; Pötter, R.; Goitein, G.; Lomax, A.J.; et al. Proton beam radiotherapy versus fractionated stereotactic radiotherapy for uveal melanomas: A comparative study. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 373–384. [Google Scholar] [CrossRef]
- Cranial srs, rt Elements Cranial srs, Version 3.0. Brainlab Software User Manual, 10th ed.; Date of Issue: 6 November 2020 (iso 8601); BRAINLAB [BrainLAB AG]: Munich, Germany.
- Kim, J.W.; Damato, B.E.; Hiscott, P. Noncontiguous tumor recurrence of posterior uveal melanoma after transscleral local resection. Arch. Ophthalmol. 2002, 120, 1659–1664. [Google Scholar] [CrossRef]
- Local recurrence significantly increases the risk of metastatic uveal melanoma. Ophthalmology 2016, 123, 86–91. [CrossRef]
- Eibl-Lindner, K.; Furweger, C.; Nentwich, M.; Foerster, P.; Wowra, B.; Schaller, U.; Muacevic, A. Robotic radiosurgery for the treatment of medium and large uveal melanoma. Melanoma Res. 2016, 26, 51–57. [Google Scholar] [CrossRef]
- Mor, J.M.; Semrau, R.; Baus, W.; Koch, K.R.; Schaub, F.; Cursiefen, C.; Marnitz, S.; Heindl, L.M. Cyberknife®: Eine neue therapieoption bei uvealem melanom. Der Ophthalmol. 2018, 115, 302–308. [Google Scholar] [CrossRef]
- Biltekin, F.; Yazici, G. Dosimetric comparison and secondary malignancy risk estimation for linac-based and robotic stereotactic radiotherapy in uveal melanoma. Med. Dosim. 2021, 46, 364–369. [Google Scholar] [CrossRef]
- Slopsema, R.L.; Mamalui, M.; Zhao, T.; Yeung, D.; Malyapa, R.; Li, Z. Dosimetric properties of a proton beamline dedicated to the treatment of ocular disease. Med. Phys. 2014, 41, 011707. [Google Scholar] [CrossRef] [PubMed]
- Egger, E.; Schalenbourg, A.; Zografos, L.; Bercher, L.; Boehringer, T.; Chamot, L.; Goitein, G. Maximizing local tumor control and survival after proton beam radiotherapy of uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 138–147. [Google Scholar] [CrossRef]
- Seibel, I.; Riechardt, A.I.; Erb-Eigner, K.; Böker, A.; Cordini, D.; Heufelder, J.; Joussen, A.M. Proton beam irradiation: A safe procedure in postequatorial extraocular extension from uveal melanoma. Am. J. Ophthalmol. 2018, 191, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Slopsema, R.L.; Mamalui, M.; Bolling, J.; Flampouri, S.; Yeung, D.; Li, Z.; Rutenberg, M.S.; Dagan, R. Can ct imaging improve targeting accuracy in clip-based proton therapy of ocular melanoma? Phys. Med. Biol. 2019, 64, 035010. [Google Scholar] [CrossRef]
- Gragoudas, E.S.; Lane, A.M.; Regan, S.; Li, W.; Judge, H.E.; Munzenrider, J.E.; Seddon, J.M.; Egan, K.M. A randomized controlled trial of varying radiation doses in the treatment of choroidal melanoma. Arch. Ophthalmol. 2000, 118, 773–778. [Google Scholar] [CrossRef]
- Wösle, M.; Krause, L.; Sreenivasa, S.; Vordermark, D.; Ciernik, I.F. Stereotactic radiotherapy for choroidal melanomas by means of hybridarc™: Physics and technique of linac-based photon beam therapy. Strahlenther. Onkol. 2018, 194, 929–943. [Google Scholar] [CrossRef]
- Georg, D.; Dieckmann, K.; Bogner, J.; Zehetmayer, M.; Pötter, R. Impact of a micromultileaf collimator on stereotactic radiotherapy of uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 881–891. [Google Scholar] [CrossRef]
- Suesskind, D.; Scheiderbauer, J.; Buchgeister, M.; Partsch, M.; Budach, W.; Bartz-Schmidt, K.U.; Ritz, R.; Grisanti, S.; Paulsen, F. Retrospective evaluation of patients with uveal melanoma treated by stereotactic radiosurgery with and without tumor resection. JAMA Ophthalmol. 2013, 131, 630–637. [Google Scholar] [CrossRef]
- Damato, B.; Wong, D.; Green, F.D.; Mackenzie, J.M. Intrascleral recurrence of uveal melanoma after transretinal “endoresection”. Br. J. Ophthalmol. 2001, 85, 114–115. [Google Scholar] [CrossRef]
- Bornfeld, N.; Talies, S.; Anastassiou, G.; Schilling, H.; Schuler, A.; Horstmann, G.A. endoscopic resection of malignant melanomas of the uvea after preoperative stereotactic single dose convergence irradiation with the leksell gamma knife. Ophthalmologe 2002, 99, 338–344. [Google Scholar] [CrossRef]
- Schilling, H.; Bornfeld, N.; Talies, S.; Anastassiou, G.; Schueler, A.; Horstmann, G.; Jurklies, B. Endoresektion großer melanome der uvea nach stereotaktischer single-dose-vorbestrahlung mit dem leksell gamma-knife—Erste erfahrungen an 46 fällen. Klin. Mon. Fur Augenheilkd. 2006, 223, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Bornfeld, N.; Bechrakis, N.E. Perspectives in ocular oncology. Klin. Monbl. Augenheilkd 2010, 227, 529. [Google Scholar] [CrossRef] [PubMed]
- Sinyavskiy, O.A.; Troyanovsky, R.L.; Ivanov, P.I.; Golovin, A.S.; Tibilov, A.V.; Solonina, S.N.; Astapenko, A.M.; Zubatkina, I.S. Microinvasive tumor endoresection in combination with ocular stereotactic radiosurgery. J. Neurosurg. 2016, 125, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Bechrakis, N.E.; Foerster, M.H. Neoadjuvant proton beam radiotherapy combined with subsequent endoresection of choroidal melanomas. Int. Ophthalmol. Clin. 2006, 46, 95–107. [Google Scholar] [CrossRef]
- Romano, M.R.; Catania, F.; Confalonieri, F.; Zollet, P.; Allegrini, D.; Sergenti, J.; Lanza, F.B.; Ferrara, M.; Angi, M. Vitreoretinal surgery in the prevention and treatment of toxic tumour syndrome in uveal melanoma: A systematic review. Int. J. Mol. Sci. 2021, 22, 10066. [Google Scholar] [CrossRef]
- Egger, E.; Zografos, L.; Schalenbourg, A.; Beati, D.; Böhringer, T.; Chamot, L.; Goitein, G. Eye retention after proton beam radiotherapy for uveal melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 867–880. [Google Scholar] [CrossRef]
- Henderson, M.A.; Shirazi, H.; Lo, S.S.; Mendonca, M.S.; Fakiris, A.J.; Witt, T.C.; Worth, R.M.; Timmerman, R.D. Stereotactic radiosurgery and fractionated stereotactic radiotherapy in the treatment of uveal melanoma. Technol. Cancer Res. Treat. 2006, 5, 411–419. [Google Scholar] [CrossRef]
- Tran, B.K.; Schalenbourg, A.; Bovey, E.; Zografos, L.; Wolfensberger, T.J. Role of vitreoretinal surgery in maximizing treatment outcome following complications after proton therapy for uveal melanoma. Retina 2013, 33, 1777–1783. [Google Scholar] [CrossRef]
- Mayo, C.; Martel, M.K.; Marks, L.B.; Flickinger, J.; Nam, J.; Kirkpatrick, J. Radiation dose-volume effects of optic nerves and chiasm. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S28–S35. [Google Scholar] [CrossRef]
- Milano, M.T.; Grimm, J.; Soltys, S.G.; Yorke, E.; Moiseenko, V.; Tomé, W.A.; Sahgal, A.; Xue, J.; Ma, L.; Solberg, T.D.; et al. Single- and multi-fraction stereotactic radiosurgery dose tolerances of the optic pathways. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 87–99. [Google Scholar] [CrossRef]
- Joye, R.P.; Williams, L.B.; Chan, M.D.; Witkin, A.J.; Schirmer, C.M.; Mignano, J.E.; Wazer, D.E.; Yao, K.C.; Wu, J.K.; Duker, J.S. Local control and results of leksell gamma knife therapy for the treatment of uveal melanoma. Ophthalmic Surg. Lasers Imaging Retin. 2014, 45, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Özcan, G.; Gündüz, A.K.; Mirzayev, İ.; Oysul, K.; Uysal, H. Early results of stereotactic radiosurgery in uveal melanoma and risk factors for radiation retinopathy. Turk. J. Ophthalmol. 2020, 50, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Arnett, A.L.H.; Reynolds, M.M.; Pulido, J.S.; Parney, I.F.; Laack, N.N. Gamma knife stereotactic radiosurgery for the treatment of primary and metastatic ocular malignancies. Stereotact. Funct. Neurosurg. 2017, 95, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Muacevic, A.; Nentwich, M.; Wowra, B.; Staerk, S.; Kampik, A.; Schaller, U. Development of a streamlined, non-invasive robotic radiosurgery method for treatment of uveal melanoma. Technol. Cancer Res. Treat. 2008, 7, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Béliveau-Nadeau, D.; Callejo, S.; Roberge, D. Technique for robotic stereotactic irradiation of choroidal melanoma. Cureus 2016, 8, e582. [Google Scholar] [CrossRef]
- Damato, B.; Kacperek, A.; Errington, D.; Heimann, H. Proton beam radiotherapy of uveal melanoma. Saudi J. Ophthalmol. 2013, 27, 151–157. [Google Scholar] [CrossRef]
- Ferreira, T.A.; Saraiva, P.; Genders, S.W.; Buchem, M.V.; Luyten, G.P.M.; Beenakker, J.W. Ct and mr imaging of orbital inflammation. Neuroradiology 2018, 60, 1253–1266. [Google Scholar] [CrossRef]




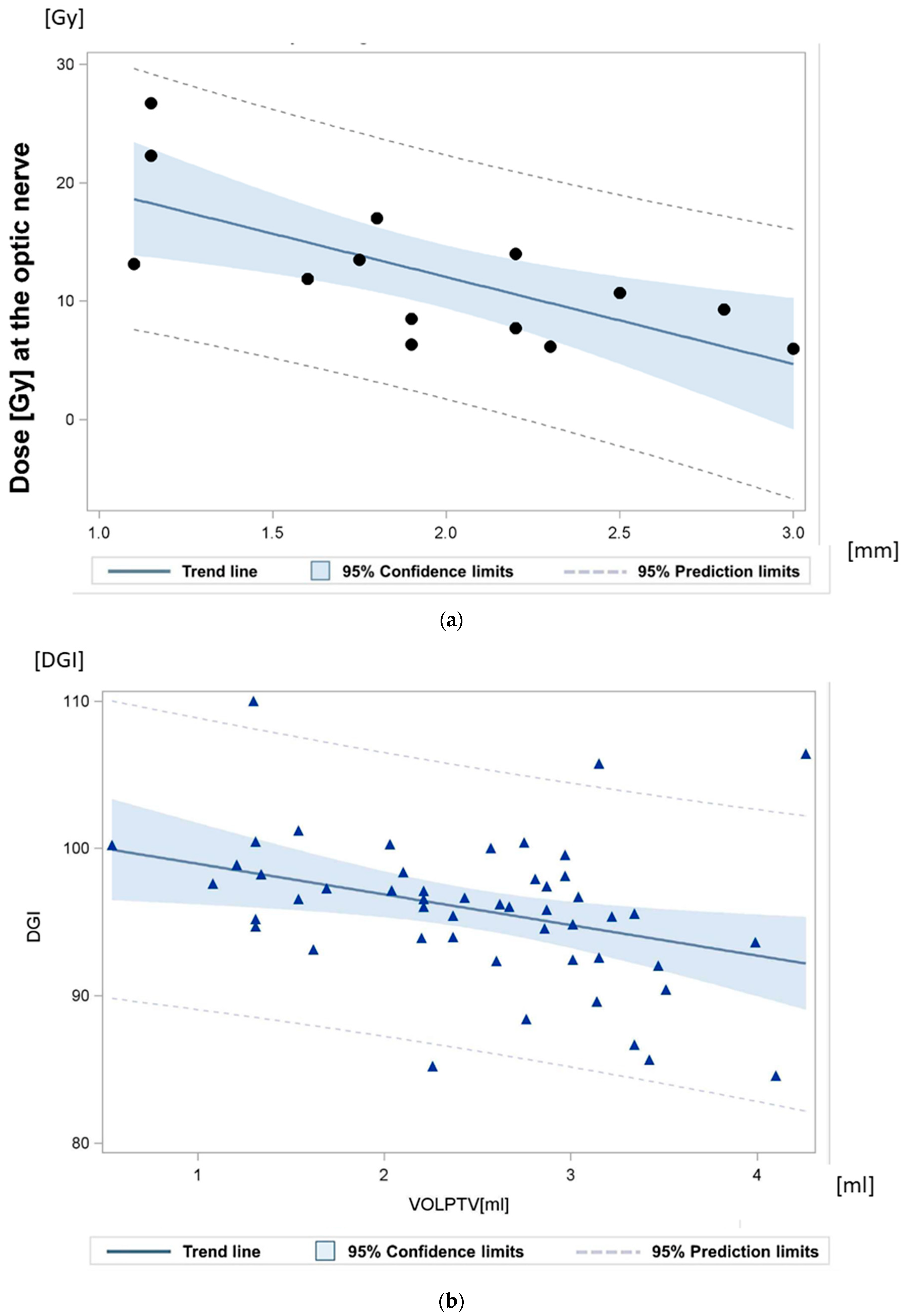
 ” Each sign representing one radiation plan.
” Each sign representing one radiation plan.
” Each sign representing one radiation plan.
” Each sign representing one radiation plan.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Obligatory Inclusion and Exclusion Criteria for Combined Radiosurgery and Resection | |
| Inclusion criteria | |
| Standard brachytherapy with Ruthenium-106 (106Ru) plaque | not applicable |
| Tumor thickness | ≥8.00 mm |
| Performance status (ECOG) | 0–1 |
| Magnetic resonance imaging | obligatory |
| For endoresection, compatibility with general anesthesia | obligatory |
| For transscleral resection, compatibility with general anesthesia in hypotension | obligatory |
| Exclusion criteria | |
| Complete loss of visual acuity | No light perception (Lux defect) |
| Localization | Ring melanoma |
| Tumor involvement of the ciliary body | Broad involvement of the ciliary body, ≥25% of the ciliary body |
| Extraocular tumor extension | Present |
| Anticoagulation or antiplatelet therapy | If this cannot be discontinued perioperatively |
| Patient and tumor characteristics | |
| Patient and tumor characteristics | Number of Patients |
| Histology | |
| Spindle cell (>90% spindle cells) | 26 |
| Mixed (>10% epithelioid cells and <90% spindle cells) | 15 |
| Epithelioid (>90% epithelioid cells) | 7 |
| Pleomorph cells | 2 |
| Ki67% | |
| No expression | 13 |
| Low expression | 27 |
| Intermediate high expression | 10 |
| High expression | 0 |
| BAP1 Immunohistochemistry (IHC)—nuclear staining | |
| BAP1 negative | 15 |
| BAP1 IHC nuclear positivity: low | 9 |
| BAP1 IHC nuclear positivity: high | 26 |
| HMB45 | |
| Positive | 19 |
| Not determined or negative | 31 |
| Monosomy for chromosome 3 | |
| Yes | 12 |
| No | 13 |
| Denial of the determination, or not determined | 25 |
| cT-category | |
| cT2a | 4 |
| cT2b | 1 |
| cT3a | 23 |
| cT3b | 5 |
| cT4a | 10 |
| cT4b | 7 |
| cN/M-category | |
| cN0/cM0 | 50 |
| AJCC stage—8th edition | |
| IIA | 4 |
| IIB | 24 |
| IIIA | 15 |
| IIIB | 7 |
| Resection modality | |
| Transscleral Resection | 11 |
| Endoresection | 39 |
| Age | Median and Range |
| Median | 55 years |
| Range | 26–84 years |
| Adverse Events within 12 Days after Radiosurgery, and before Resection according to CTCAE Version 5.0 | |||||
| CTC Score immediate after SRS | CTC 0 | CTC I | CTC II | CTC III | CTC IV |
| 1. Visual acuity | 50 | 0 | 0 | 0 | 0 |
| 2. Eye pain | 46 | 4 | 0 | 0 | 0 |
| 3. Inflammation | 48 | 2 | 0 | 0 | 0 |
| 4. Optic nerve disorder, including papilledema | 50 | 0 | 0 | 0 | 0 |
| 5. Other ocular side-effects: hemorrhage; extraocular muscle paresis; eyelid function disorder; glaucoma; periorbital edema | 49 | 1 | 0 | 0 | 0 |
| Adverse Events within 30 days after resection according to CTCAE Version 5.0 | |||||
| CTC Score:After resection | Not yet assessable, but light perception verifiable | ||||
| 1. Visual acuity | 50 | ||||
| CTC Score:After resection | CTC 0–I | CTC II | CTC III | CTC IV | |
| 2. Eye pain | 43 | 7 | 0 | 0 | |
| 3. Inflammation | 44 | 6 | 0 | 0 | |
| 4. Other ocular side-effects: hemorrhage; extraocular muscle paresis; eyelid function disorder; glaucoma; periorbital edema | 40 | 7 | 1 | 1 | |
| Adverse Events more than 30 days after radiosurgery and resection, up to the last follow-up (mean 18 months) according to CTCAE, Version 5.0 | |||||
| CTC Score: Last follow-up | Visual acuity improvement | idem | I | II and N(Y)Q* | |
| 1. Visual acuity | 8 | 10 | 14 | 17* | 1*/** |
| CTC Score: Last follow-up | CTC 0 | CTC I | CTC II | CTC III–IV | N(Y)Q |
| 2. Eye pain | 48 | 1 | 0 | 0 | 1** |
| 3. Inflammation | 46 | 3 | 0 | 0 | 1** |
| 4. Optic nerve disorder, including papilledema | 45 | 0 | 3 | 1 | 1** |
| 5. Macular edema | 24 | 7 | 7 | 0 | 11*/1** |
| 6. Other ocular side-effects: hemorrhage; extraocular muscle paresis; eyelid function disorder; glaucoma; periorbital edema | 39 | 5 | 4 | 1** | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guberina, M.; Sokolenko, E.; Guberina, N.; Dalbah, S.; Pöttgen, C.; Lübcke, W.; Indenkämpen, F.; Lachmuth, M.; Flühs, D.; Chen, Y.; et al. Feasibility, Method and Early Outcome of Image-Guided Volumetric Modulated Arc Radiosurgery Followed by Resection for AJCC Stage IIA–IIIB High-Risk Large Intraocular Melanoma. Cancers 2022, 14, 4729. https://doi.org/10.3390/cancers14194729
Guberina M, Sokolenko E, Guberina N, Dalbah S, Pöttgen C, Lübcke W, Indenkämpen F, Lachmuth M, Flühs D, Chen Y, et al. Feasibility, Method and Early Outcome of Image-Guided Volumetric Modulated Arc Radiosurgery Followed by Resection for AJCC Stage IIA–IIIB High-Risk Large Intraocular Melanoma. Cancers. 2022; 14(19):4729. https://doi.org/10.3390/cancers14194729
Chicago/Turabian StyleGuberina, Maja, Ekaterina Sokolenko, Nika Guberina, Sami Dalbah, Christoph Pöttgen, Wolfgang Lübcke, Frank Indenkämpen, Manfred Lachmuth, Dirk Flühs, Ying Chen, and et al. 2022. "Feasibility, Method and Early Outcome of Image-Guided Volumetric Modulated Arc Radiosurgery Followed by Resection for AJCC Stage IIA–IIIB High-Risk Large Intraocular Melanoma" Cancers 14, no. 19: 4729. https://doi.org/10.3390/cancers14194729
APA StyleGuberina, M., Sokolenko, E., Guberina, N., Dalbah, S., Pöttgen, C., Lübcke, W., Indenkämpen, F., Lachmuth, M., Flühs, D., Chen, Y., Hoffmann, C., Deuschl, C., Jabbarli, L., Fiorentzis, M., Foerster, A., Rating, P., Ebenau, M., Grunewald, T., Bechrakis, N., & Stuschke, M. (2022). Feasibility, Method and Early Outcome of Image-Guided Volumetric Modulated Arc Radiosurgery Followed by Resection for AJCC Stage IIA–IIIB High-Risk Large Intraocular Melanoma. Cancers, 14(19), 4729. https://doi.org/10.3390/cancers14194729