
Quality-of-Life Evaluation of Patients with Unresectable Locally Advanced or Locally Recurrent Head and Neck Carcinoma Treated with Head and Neck Photoimmunotherapy


Abstract
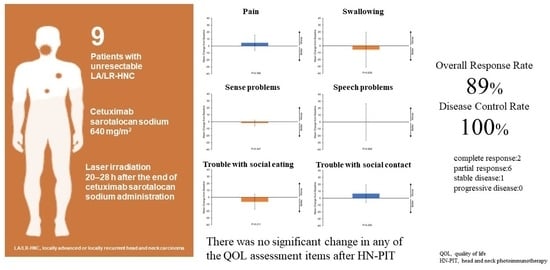
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Outcomes and Assessments
2.4. Drug Administration of Cetuximab Sarotalocan Sodium
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
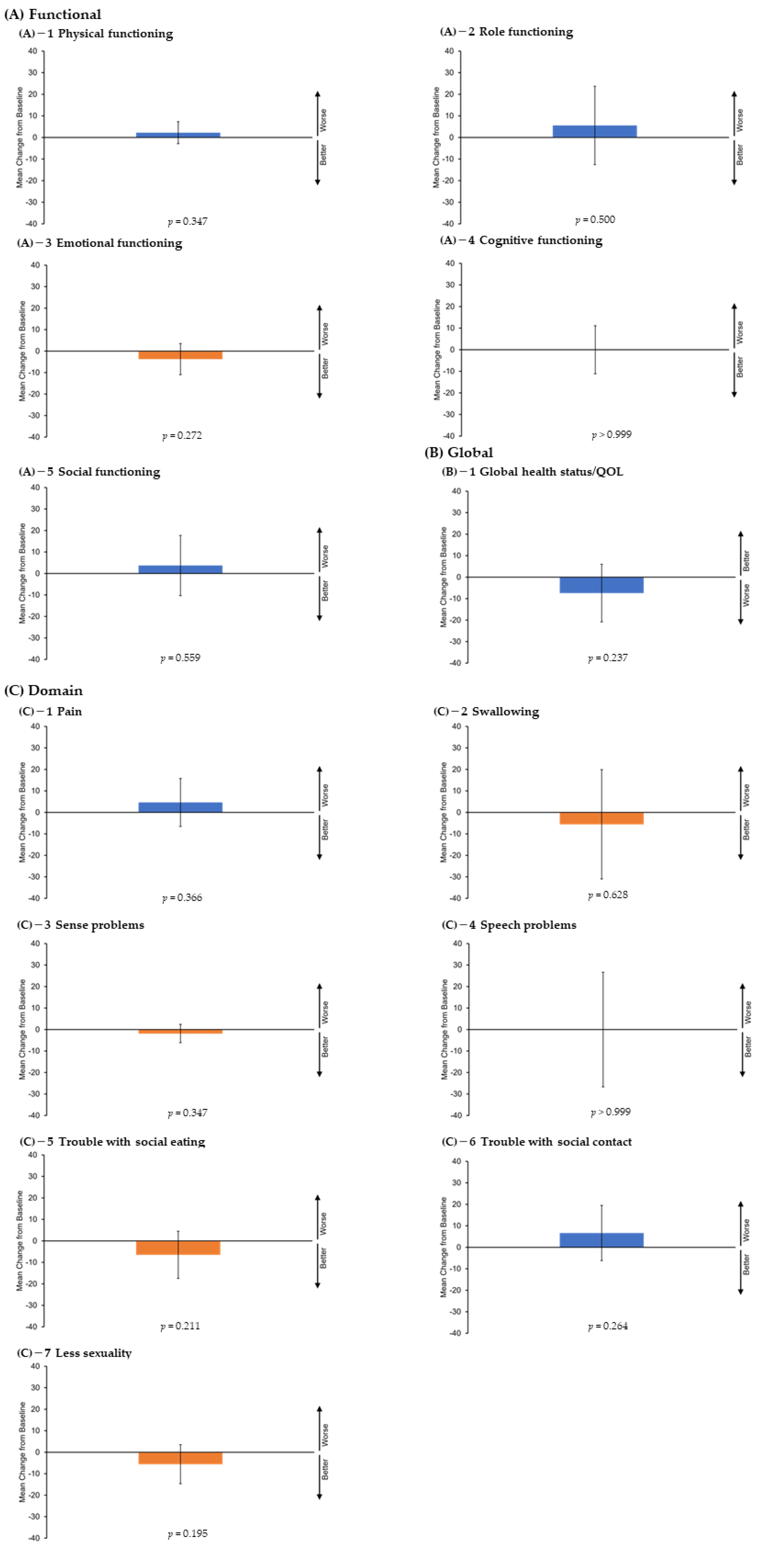
3.2. QOL Assessment
3.3. Efficacy
3.4. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Head and Neck Cancers Version 2.2022. 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 4 July 2022).
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (keynote-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Okamoto, I.; Tsukahara, K.; Sato, H. Single-center prospective study on the efficacy of nivolumab against platinum-sensitive recurrent or metastatic head and neck squamous cell carcinoma. Sci. Rep. 2022, 12, 2025. [Google Scholar] [CrossRef] [PubMed]
- Mitsunaga, M.; Ogawa, M.; Kosaka, N.; Rosenblum, L.T.; Choyke, P.L.; Kobayashi, H. Cancer cell-selective in vivo near infrared photoimmunotherapy targeting specific membrane molecules. Nat. Med. 2011, 17, 1685–1691. [Google Scholar] [CrossRef]
- Ogawa, M.; Tomita, Y.; Nakamura, Y.; Lee, M.J.; Lee, S.; Tomita, S.; Nagaya, T.; Sato, K.; Yamauchi, T.; Iwai, H.; et al. Immunogenic cancer cell death selectively induced by near infrared photoimmunotherapy initiates host tumor immunity. Oncotarget 2017, 8, 10425–10436. [Google Scholar] [CrossRef] [PubMed]
- Cognetti, D.M.; Johnson, J.M.; Curry, J.M.; Kochuparambil, S.T.; McDonald, D.; Mott, F.; Fidler, M.J.; Stenson, K.; Vasan, N.R.; Razaq, M.A.; et al. Phase 1/2a, open-label, multicenter study of rm-1929 photoimmunotherapy in patients with locoregional, recurrent head and neck squamous cell carcinoma. Head Neck 2021, 43, 3875–3887. [Google Scholar] [CrossRef]
- Okamoto, I.; Okada, T.; Tokashiki, K.; Tsukahara, K. A case treated with photoimmunotherapy under a navigation system for recurrent lesions of the lateral pterygoid muscle. In Vivo 2022, 36, 1035–1040. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Nat. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Bjordal, K.; Ahlner-Elmqvist, M.; Tollesson, E.; Jensen, A.B.; Razavi, D.; Maher, E.J.; Kaasa, S. Development of a European Organization for Research and Treatment of Cancer (EORTC) questionnaire module to be used in quality of life assessments in head and neck cancer patients. EORTC Quality of Life Study Group. Acta Oncol. 1994, 33, 879–885. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C.H. TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell: Oxford, UK, 2011. [Google Scholar]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). Version 4.03. 2010. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf (accessed on 4 July 2022).
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Tahara, M.; Okano, S.; Enokida, T.; Ueda, Y.; Fujisawa, T.; Shinozaki, T.; Tomioka, T.; Okano, W.; Biel, M.A.; Ishida, K.; et al. A phase I, single-center, open-label study of RM-1929 photoimmunotherapy in Japanese patients with recurrent head and neck squamous cell carcinoma. Int. J. Clin. Oncol. 2021, 26, 1812–1821. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of Checkmate 141 with analyses by tumor PD-L1 expression. Oral Oncol. 2018, 81, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, D.; Suzuki, H.; Koide, Y.; Beppu, S.; Kadowaki, S.; Sone, M.; Hanai, N. Prognostic markers in head and neck cancer patients treated with nivolumab. Cancers 2018, 10, 466. [Google Scholar] [CrossRef]
- Okamoto, I.; Sato, H.; Kondo, T.; Koyama, N.; Fushimi, C.; Okada, T.; Miura, K.; Matsuki, T.; Yamashita, T.; Omura, G.; et al. Efficacy and safety of nivolumab in 100 patients with recurrent or metastatic head and neck cancer—A retrospective multicentre study. Acta Otolaryngol. 2019, 139, 918–925. [Google Scholar] [CrossRef]
- Matsuki, T.; Okamoto, I.; Fushimi, C.; Sawabe, M.; Kawakita, D.; Sato, H.; Tsukahara, K.; Kondo, T.; Okada, T.; Tada, Y.; et al. Hematological predictive markers for recurrent or metastatic squamous cell carcinomas of the head and neck treated with nivolumab: A multicenter study of 88 patients. Cancer Med. 2020, 9, 5015–5024. [Google Scholar] [CrossRef]
- Matsuki, T.; Okamoto, I.; Fushimi, C.; Takahashi, H.; Okada, T.; Kondo, T.; Sato, H.; Ito, T.; Tokashiki, K.; Tsukahara, K.; et al. Real-world, long-term outcomes of nivolumab therapy for recurrent or metastatic squamous cell carcinoma of the head and neck and impact of the magnitude of best overall response: A retrospective multicenter study of 88 patients. Cancers 2020, 12, 3427. [Google Scholar] [CrossRef]
- Matsuo, M.; Yasumatsu, R.; Masuda, M.; Toh, S.; Wakasaki, T.; Hashimoto, K.; Taura, M.; Uchi, R.; Nakagawa, T. Relationship between immune-related adverse events and the long-term outcomes in recurrent/metastatic head and neck squamous cell carcinoma treated with nivolumab. Oral Oncol. 2020, 101, 104525. [Google Scholar] [CrossRef]
- Sato, Y.; Fukuda, N.; Wang, X.; Urasaki, T.; Ohmoto, A.; Nakano, K.; Yunokawa, M.; Ono, M.; Sato, Y.; Mitani, H.; et al. Efficacy of nivolumab for head and neck cancer patients with primary sites and histological subtypes excluded from the Checkmate-141 trial. Cancer Manag. Res. 2020, 12, 4161–4168. [Google Scholar] [CrossRef]
- Wakasaki, T.; Yasumatsu, R.; Masuda, M.; Takeuchi, T.; Manako, T.; Matsuo, M.; Jiromaru, R.; Uchi, R.; Komune, N.; Noda, T.; et al. Prognostic biomarkers of salvage chemotherapy following nivolumab treatment for recurrent and/or metastatic head and neck squamous cell carcinoma. Cancers 2020, 12, 2299. [Google Scholar] [CrossRef]
- Ueki, Y.; Takahashi, T.; Ota, H.; Shodo, R.; Yamazaki, K.; Horii, A. Predicting the treatment outcome of nivolumab in recurrent or metastatic head and neck squamous cell carcinoma: Prognostic value of combined performance status and modified Glasgow prognostic score. Eur. Arch. Otorhinolaryngol. 2020, 277, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Chikuie, N.; Hamamoto, T.; Ueda, T.; Taruya, T.; Kono, T.; Furuie, H.; Ishino, T.; Takeno, S. Baseline neutrophil-to-lymphocyte ratio and Glasgow prognostic score are associated with clinical outcome in patients with recurrent or metastatic head and neck squamous cell carcinoma treated with nivolumab. Acta Med. Okayama 2021, 75, 335–343. [Google Scholar] [PubMed]
- Minohara, K.; Matoba, T.; Kawakita, D.; Takano, G.; Oguri, K.; Murashima, A.; Nakai, K.; Iwaki, S.; Hojo, W.; Matsumura, A.; et al. Novel prognostic score for recurrent or metastatic head and neck cancer patients treated with nivolumab. Sci. Rep. 2021, 11, 16992. [Google Scholar] [CrossRef] [PubMed]
- Tanoue, K.; Tamura, S.; Kusaba, H.; Shinohara, Y.; Ito, M.; Tsuchihashi, K.; Shirakawa, T.; Otsuka, T.; Ohmura, H.; Isobe, T.; et al. Predictive impact of c-reactive protein to albumin ratio for recurrent or metastatic head and neck squamous cell carcinoma receiving nivolumab. Sci. Rep. 2021, 11, 2741. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, I.; Okada, T.; Tokashiki, K.; Tsukahara, K. Photoimmunotherapy for managing recurrent laryngeal cancer cervical lesions: A case report. Case Rep. Oncol. 2022, 15, 34–39. [Google Scholar] [CrossRef]
- Nagaya, T.; Friedman, J.; Maruoka, Y.; Ogata, F.; Okuyama, S.; Clavijo, P.E.; Choyke, P.L.; Allen, C.; Kobayashi, H. Host immunity following near-infrared photoimmunotherapy is enhanced with PD-1 checkpoint blockade to eradicate established antigenic tumors. Cancer Immunol. Res. 2019, 7, 401–413. [Google Scholar] [CrossRef]
- Law, A.W.; Mole, R.H. Direct and abscopal effects of x-radiation on the thymus of the weanling rat. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1961, 3, 233–248. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | All Patients (n = 9) | |
|---|---|---|
| No. | % | |
| Age, years | ||
| Mean | 73 | |
| Median | 73 | |
| Range | 67–77 | |
| Sex | ||
| Male | 8 | 89 |
| Female | 1 | 11 |
| ECOG performance status | ||
| PS 0 | 9 | 100 |
| PS 1 | 0 | 0 |
| Primary tumor site | ||
| Oropharynx | 2 | 22 |
| p16-positive | 0 | - |
| p16-negative | 2 | - |
| Oral cavity | 3 | 33 |
| Hypopharynx | 2 | 22 |
| Larynx | 2 | 22 |
| T category | ||
| T0 | 1 | 11 |
| T1 | 1 | 11 |
| T2 | 3 | 33 |
| T3 | 2 | 22 |
| T4 | 2 | 22 |
| N category | ||
| N0 | 8 | 89 |
| N1/N2/N3 | 1 | 11 |
| M category | ||
| M0 | 9 | 100 |
| M1 | 0 | 0 |
| Previous surgery | ||
| Yes | 9 | 100 |
| No | 0 | 0 |
| Previous radiation therapy | ||
| Yes | 9 | 100 |
| No | 0 | 0 |
| Previous chemotherapy | ||
| Yes | 2 | 22 |
| No | 7 | 78 |
| Reason for unresectability | ||
| Difficulty in reconstructive surgery | 7 | 78 |
| Iatrogenic multiple recurrent lesions after radiotherapy or multiple surgeries | 2 | 22 |
| Case | Primary Tumor Site | Location of Target Lesion |
|---|---|---|
| 1 | Larynx | Cervical lymph node |
| 2 | Oral cavity | Buccal mucosa |
| 3 | Hypopharynx | Oropharynx (anterior wall/lateral wall/superior wall) |
| 4 | Oropharynx | Oropharynx (anterior wall) |
| 5 | Oral cavity | Tongue/upper gingiva/lower gingiva |
| 6 | Oral cavity | Maxillary sinus |
| 7 | Larynx | Reconstructed skin valve site/oropharynx (anterior wall/posterior wall) |
| 8 | Oropharynx | Reconstructed skin valve site/oropharynx (anterior wall/lateral wall) |
| 9 | Hypopharynx | Oropharynx (anterior wall/lateral wall/posterior wall) |
| QOL Score LS Mean (95% CI) | Change from Baseline LS Mean (95% CI) | p-Value vs. Baseline | |
|---|---|---|---|
| Functional scales | |||
| Physical functioning | |||
| Pre-HN-PIT | 88.1 (80.7–95.6) | - | - |
| 4 weeks | 90.4 (83.0–97.8) | 2.2 (−2.9–7.3) | 0.347 |
| Role functioning | |||
| Pre-HN-PIT | 85.2 (70.9–99.4) | - | - |
| 4 weeks | 90.7 (76.5–105.0) | 5.6 (−12.6–23.7) | 0.500 |
| Emotional functioning | |||
| Pre-HN-PIT | 89.8 (80.4–99.2) | - | - |
| 4 weeks | 86.1 (76.7–95.5) | −3.7 (−10.9–3.5) | 0.272 |
| Cognitive functioning | |||
| Pre-HN-PIT | 87.0 (73.7–100.4) | - | - |
| 4 weeks | 87.0 (73.7–100.4) | 0.0 (−11.1–11.1) | >0.999 |
| Social functioning | |||
| Pre-HN-PIT | 88.9 (77.7–100.1) | - | - |
| 4 weeks | 92.6 (81.4–103.8) | 3.7 (−10.3–17.7) | 0.559 |
| Global health status | |||
| Global health status/QoL | |||
| Pre-HN-PIT | 68.5 (51.7–85.3) | - | - |
| 4 weeks | 61.1 (44.3–77.9) | −7.4 (−20.8–6.0) | 0.237 |
| Domain scales | |||
| Pain | |||
| Pre-HN-PIT | 21.3 (5.1–37.5) | - | - |
| 4 weeks | 25.9 (9.8–42.1) | 4.6 (−6.5–15.8) | 0.366 |
| Swallowing | |||
| Pre-HN-PIT | 30.6 (10.7–50.5) | - | - |
| 4 weeks | 25.0 (5.1–44.9) | −5.6 (−31.0–19.9) | 0.628 |
| Sense problems | |||
| Pre-HN-PIT | 9.3 (−7.7–26.2) | - | - |
| 4 weeks | 7.4 (−9.6–24.4) | −1.9 (−6.1–2.4) | 0.347 |
| Speech problems | |||
| Pre-HN-PIT | 34.6 (18.8–50.3) | - | - |
| 4 weeks | 34.6 (18.8–50.3) | 0.0 (−26.7–26.7) | >0.999 |
| Trouble with social eating | |||
| Pre-HN-PIT | 33.3 (14.2–52.4) | - | - |
| 4 weeks | 26.9 (7.8–46.0) | −6.5 (−17.5–4.5) | 0.211 |
| Trouble with social contact | |||
| Pre-HN-PIT | 9.6 (−4.0–23.3) | - | - |
| 4 weeks | 16.3 (2.6–29.9) | 6.7 (−6.1–19.5) | 0.264 |
| Less sexuality | |||
| Pre-HN-PIT | 18.5 (−6.5–43.6) | - | - |
| 4 weeks | 13.0 (−12.1–38.0) | −5.6 (−14.6–3.5) | 0.195 |
| Patients, n (%) | Grade | Grade | Grade | Grade | Grade | Grades |
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | all | |
| Pain | 1 (11) | 7 (78) | 1 (11) | 0 (0) | 0 (0) | 9 (100) |
| Mucositis | 1 (11) | 6 (68) | 1 (11) | 0 (0) | 0 (0) | 8 (89) |
| Laryngeal edema | 0 (0) | 2 (22) | 0 (0) | 1 (11) | 0 (0) | 3 (33) |
| Dysphagia | 0 (0) | 1 (11) | 2 (22) | 0 (0) | 0 (0) | 3 (33) |
| Tongue and pharyngeal edema | 0 (0) | 2 (22) | 1 (11) | 0 (0) | 0 (0) | 3 (33) |
| Nausea | 3 (33) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 3 (33) |
| Hyponatremia | 0 (0) | 0 (0) | 2 (22) | 0 (0) | 0 (0) | 2 (22) |
| Hemorrhage | 2 (22) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (22) |
| Diarrhea | 2 (22) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 2 (22) |
| Acute kidney injury | 0 (0) | 0 (0) | 0 (0) | 1 (11) | 0 (0) | 1 (11) |
| Anemia | 0 (0) | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 1 (11) |
| Hypokalemia | 0 (0) | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 1 (11) |
| Liver dysfunction | 0 (0) | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 1 (11) |
| Weight loss | 0 (0) | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 1 (11) |
| Acneiform rash | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Fever | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Aspiration | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Hyperkalemia | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Trismus | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Constipation | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Dehydration | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Intratumoral broken needle fragments | 0 (0) | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Oral dysesthesia | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
| Edema of face | 1 (11) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (11) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okamoto, I.; Okada, T.; Tokashiki, K.; Tsukahara, K. Quality-of-Life Evaluation of Patients with Unresectable Locally Advanced or Locally Recurrent Head and Neck Carcinoma Treated with Head and Neck Photoimmunotherapy. Cancers 2022, 14, 4413. https://doi.org/10.3390/cancers14184413
Okamoto I, Okada T, Tokashiki K, Tsukahara K. Quality-of-Life Evaluation of Patients with Unresectable Locally Advanced or Locally Recurrent Head and Neck Carcinoma Treated with Head and Neck Photoimmunotherapy. Cancers. 2022; 14(18):4413. https://doi.org/10.3390/cancers14184413
Chicago/Turabian StyleOkamoto, Isaku, Takuro Okada, Kunihiko Tokashiki, and Kiyoaki Tsukahara. 2022. "Quality-of-Life Evaluation of Patients with Unresectable Locally Advanced or Locally Recurrent Head and Neck Carcinoma Treated with Head and Neck Photoimmunotherapy" Cancers 14, no. 18: 4413. https://doi.org/10.3390/cancers14184413
APA StyleOkamoto, I., Okada, T., Tokashiki, K., & Tsukahara, K. (2022). Quality-of-Life Evaluation of Patients with Unresectable Locally Advanced or Locally Recurrent Head and Neck Carcinoma Treated with Head and Neck Photoimmunotherapy. Cancers, 14(18), 4413. https://doi.org/10.3390/cancers14184413