

Does Vaginal Cuff Creation and Avoidance of a Uterine Manipulator Improve the Prognosis of Total Laparoscopic Radical Hysterectomy for Early Cervical Cancer? A Retrospective Multicenter Study

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical and Pathologic Data
2.2. Treatment Protocol and Response Assessment
2.3. Variable Definitions
2.4. Statistical Analysis
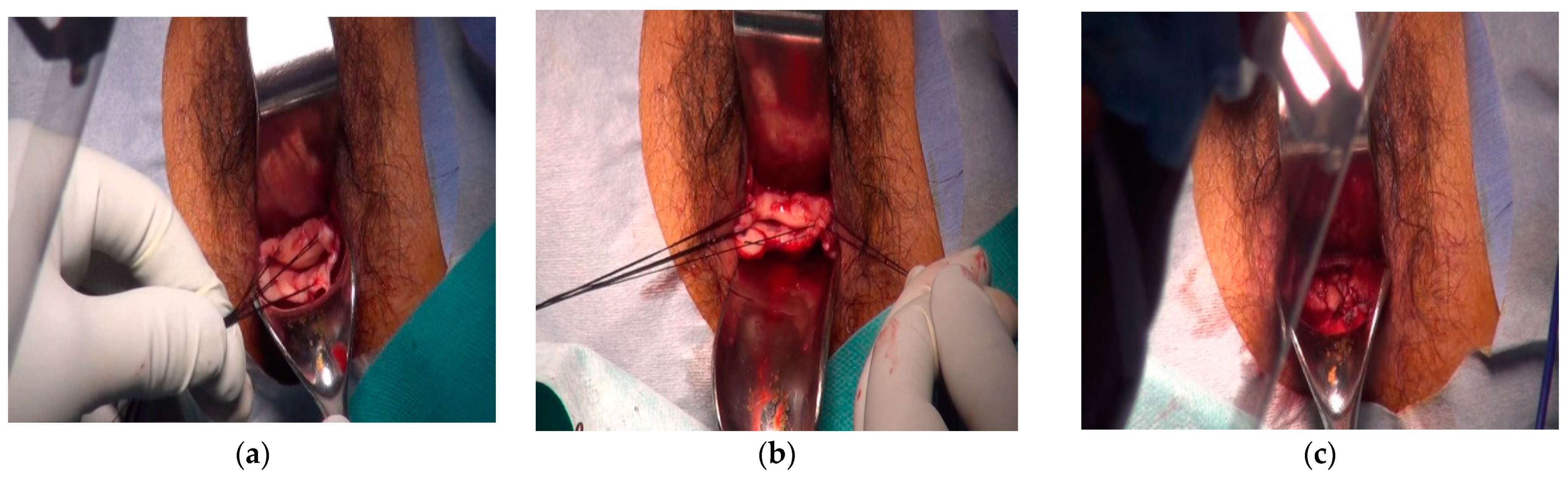
2.5. Procedure
2.6. Port Site Setting
3. Results
3.1. Patient Characteristics
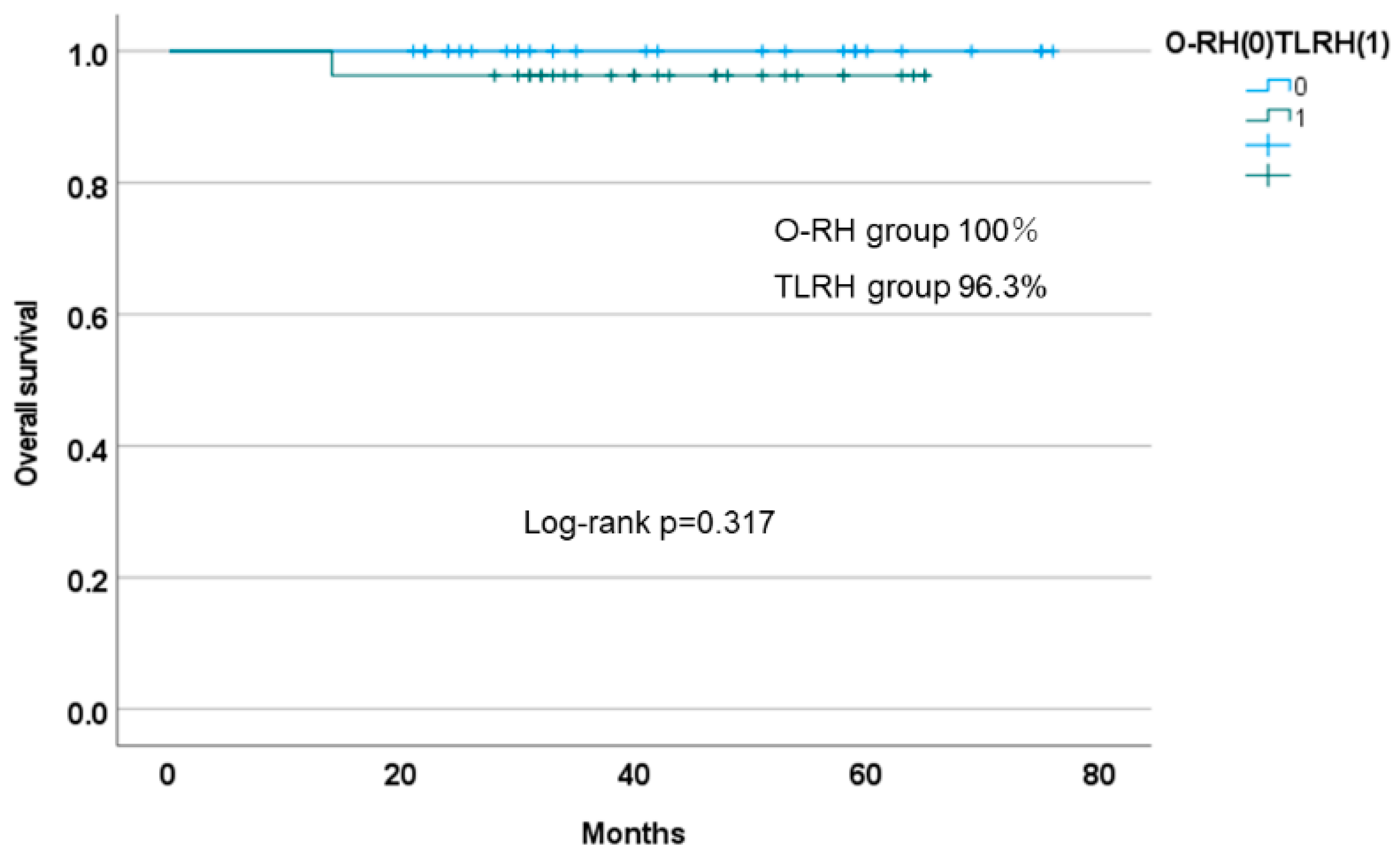
3.2. Survival Outcomes
3.3. Adjuvant Therapy
3.4. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Zanetti, R.; Ferlay, J. Cancer Incidence in Five Continents. IARC Scientific Publication No. 166. Volume XI. Available online: https://ci5.iarc.fr (accessed on 10 June 2022).
- Nezhat, C.R.; Burrell, M.O.; Nezhat, F.R.; Benigno, B.B.; Welander, C.E. Laparoscopic radical hysterectomy with paraaortic and pelvic node dissection. Am. J. Obstet. Gynecol. 1992, 166, 864–865. [Google Scholar] [CrossRef]
- Wright, J.D.; Herzog, T.J.; Neugut, A.I.; Burke, W.M.; Lu, Y.S.; Lewin, S.N.; Hershman, D.L. Comparative effectiveness of minimally invasive and abdominal radical hysterectomy for cervical cancer. Gynecol. Oncol. 2012, 127, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Shah, C.A.; Beck, T.; Liao, J.B.; Giannakopoulos, N.V.; Veljovich, D.; Paley, P. Surgical and oncologic outcomes after robotic radical hysterectomy as compared to open radical hysterectomy in the treatment of early cervical cancer. J. Gynecol. Oncol. 2017, 28, e82. [Google Scholar] [CrossRef] [PubMed]
- Corrado, G.; Vizza, E.; Legge, F.; Anchora, L.P.; Sperduti, I.; Fagotti, A.; Mancini, E.; Gallotta, V.; Zampa, A.; Chiofalo, B.; et al. Comparison of different surgical approaches for stage ib1 cervical cancer patients: A multi-institution study and a review of the literature. Int. J. Gynecol. Cancer 2018, 28, 1020–1028. [Google Scholar] [CrossRef]
- Gil-Moreno, A.; Carbonell-Socias, M.; Salicrú, S.; Centeno-Mediavilla, C.; Franco-Camps, S.; Colas, E.; Oaknin, A.; Pérez-Benavente, A.; Díaz-Feijoo, B. Radical hysterectomy: Efficacy and safety in the dawn of minimally invasive techniques. J. Minim. Invasive Gynecol. 2019, 26, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally invasive versus abdominal radical hysterectomy for cervical cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Melamed, A.; Margul, D.J.; Chen, L.; Keating, N.L.; Del Carmen, M.G.; Yang, J.; Seagle, B.L.; Alexander, A.; Barber, E.L.; Rice, L.W.; et al. Survival after minimally invasive radical hysterectomy for early-Stage cervical cancer. N. Engl. J. Med. 2018, 379, 1905–1914. [Google Scholar] [CrossRef]
- Lewicki, P.J.; Basourakos, S.P.; Qiu, Y.; Hu, J.C.; Sheyn, D.; Hijaz, A.; Shoag, J.E. Effect of a randomized, controlled trial on surgery for cervical cancer. N. Engl. J. Med. 2021, 384, 1669–1671. [Google Scholar] [CrossRef]
- Van den Haak, L.; Alleblas, C.; Nieboer, T.E.; Rhemrev, J.P.; Jansen, F.W. Efficacy and safety of uterine manipulators in laparoscopic surgery: A review. Arch. Gynecol. Obstet. 2015, 292, 1003–1011. [Google Scholar] [CrossRef]
- Padilla-Iserte, P.; Lago, V.; Tauste, C.; Díaz-Feijoo, B.; Gil-Moreno, A.; Oliver, R.; Coronado, P.; Martín-Salamanca, M.B.; Pantoja-Garrido, M.; Marcos-Sanmartin, J.; et al. Spanish Society of Gynecology and Obstetrics Spanish Investigational Network Gynecologic Oncology Group. Impact of uterine manipulator on oncological outcome in endometrial cancer surgery. Am. J. Obstet. Gynecol. 2021, 224, 65.e1–65.e11. [Google Scholar] [CrossRef]
- Nitecki, R.; Ramirez, P.T.; Frumovitz, M.; Krause, K.J.; Tergas, A.I.; Wright, J.D.; Rauh-Hain, J.A.; Melamed, A. Survival After Minimally Invasive vs Open Radical Hysterectomy for Early-Stage Cervical Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2020, 6, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- Ronsini, C.; Köhler, C.; De Franciscis, P.; La Verde, M.; Mosca, L.; Solazzo, M.C.; Colacurci, N. Laparo-assisted vaginal radical hysterectomy as a safe option for Minimal Invasive Surgery in early stage cervical cancer: A systematic review and meta-analysis. Gynecol. Oncol. 2022, 166, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Leitao, M.M., Jr.; Zhou, Q.C.; Brandt, B.; Iasonos, A.; Sioulas, V.; Mager, K.L.; Shahin, M.; Bruce, S.; Black, D.R.; Kay, C.G.; et al. The MEMORY Study: MulticentEr study of Minimally invasive surgery versus Open Radical hYsterectomy in the management of early-stage cervical cancer: Survival outcomes. Gynecol. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Alfonzo, E.; Wallin, E.; Ekdahl, L.; Staf, C.; Rådestad, A.F.; Reynisson, P.; Stålberg, K.; Falconer, H.; Persson, J.; Dahm-Kähler, P. No survival difference between robotic and open radical hysterectomy for women with early-stage cervical cancer: Results from a nationwide population-based cohort study. Eur. J. Cancer 2019, 116, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Manzour, N.; Núñez-Cordoba, J.M.; Chiva, L.; Chacón, E.; Boria, F.; Vara-García, J.; Rodriguez-Velandia, Y.P.; Minguez, J.A.; Alcazar, J.L. Pattern of relapse in patients with stage IB1 cervical cancer after radical hysterectomy as primary treatment. Minimally invasive surgery vs. open approach. Systematic review and meta-analysis. Gynecol. Oncol. 2022, 164, 455–460. [Google Scholar] [CrossRef]
- Lago, V.; Tiermes, M.; Padilla-Iserte, P.; Matute, L.; Gurrea, M.; Domingo, S. Protective maneuver to avoid tumor spillage during laparoscopic radical hysterectomy: Vaginal cuff closure. J. Minim. Invasive Gynecol. 2021, 28, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Kohler, C.; Hertel, H.; Herrmann, J.; Marnitz, S.; Mallmann, P.; Favero, G.; Plaikner, A.; Martus, P.; Gajda, M.; Schneider, A. Laparoscopic radical hysterectomy with transvaginal closure of vaginal cuff-A multicenter analysis. Int. J. Gynecol. Cancer 2019, 29, 845–850. [Google Scholar] [CrossRef]
- Kanno, K.; Andou, M.; Yanai, S.; Toeda, M.; Nimura, R.; Ichikawa, F.; Teishikata, Y.; Shirane, T.; Sakate, S.; Kihira, T.; et al. Long-term oncological outcomes of minimally invasive radical hysterectomy for early-stage cervical cancer: A retrospective, single-institutional study in the wake of the LACC trial. J. Obstet. Gynaecol. Res. 2019, 45, 2425–2434. [Google Scholar] [CrossRef]
- Ding, B.; Guan, X.; Duan, K.; Shen, Y. Laparoscopic radical hysterectomy with enclosed colpotomy without the use of uterine manipulator for early-stage cervical cancer. J. Minim. Access Surg. 2021, 17, 570–572. [Google Scholar] [CrossRef]
- Clavien, P.A.; Strasberg, S.M. Severity grading of surgical complications. Ann. Surg. 2009, 250, 197–198. [Google Scholar] [CrossRef]
- Nagase, S.; Ohta, T.; Takahashi, F.; Yaegashi, N.; Board members of the 2020 Committee on Gynecologic Oncology of the Japan Society of Obstetrics and Gynecology. Annual report of the Committee on Gynecologic Oncology, the Japan Society of Obstetrics and Gynecology: Annual patient report for 2017 and annual treatment report for 2012. J. Obstet. Gynaecol. Res. 2021, 47, 1631–1642. [Google Scholar] [CrossRef] [PubMed]
- Margul, D.J.; Yang, J.; Seagle, B.L.; Kocherginsky, M.; Shahabi, S. Outcomes and costs of open, robotic, and laparoscopic radical hysterectomy for stage IB1 cervical cancer. J. Clin. Oncol. 2018, 36, 5502. [Google Scholar] [CrossRef]
- Sert, B.M.; Kristensen, G.B.; Kleppe, A.; Dørum, A. Long-term oncological outcomes and recurrence patterns in early-stage cervical cancer treated with minimally invasive versus abdominal radical hysterectomy: The Norwegian Radium Hospital experience. Gynecol. Oncol. 2021, 162, 284–291. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 94) | TLRH (n = 36) | O-RH (n = 58) | ||
|---|---|---|---|---|
| Age, years | 0.200 | |||
| Median (range) | 45.5 (28–77) | 44.5 (28–77) | 48 (29–76) | |
| BMI, kg/m2 | 1 | |||
| Median, range | 20.9 (15.1–35.4) | 20.6 (17.9–27.8) | 21.1 (17–35.4) | |
| Para | 0.181 | |||
| 0 | 17 | 9 | 8 | |
| >1 | 77 | 27 | 50 | |
| Histology | 1 | |||
| SCC | 70 | 27 | 43 | |
| Adenocarcinoma/adenosquamous | 24 | 9 | 15 * | |
| Conization | ||||
| Done | 10 (27.7%) | |||
| No conization | 26 (62.3%) | |||
| Tumor size (preoperative, MRI) | 0.001 | |||
| <2 cm | 41 | 23 | 17 | |
| 2–4 cm | 54 | 13 | 41 | |
| Operative time (min) | 382 | 382 (270–460) | 382 (200–689) | 0.768 |
| Amount of bleeding | 417 | 198 (5–1772) | 517.5 (123–2360) | <0.001 |
| Post-operative stage (FIGO 2018) | <0.01 | |||
| 1B1 | 34 | 20 | 14 | |
| 1B2 | 30 | 11 | 19 | |
| 2A1 | 3 | 1 | 2 | |
| 2B | 2 | 2 | ||
| 3C1p | 25 | 4 | 21 | |
| LVSI | 0.03 | |||
| + | 16 | 39 | ||
| − | 20 | 19 | ||
| Number of harvested lymph nodes | 26 (12–63) | 29 (18–57) | 25 (12–63) | 0.471 |
| Lymph node metastasis | <0.01 | |||
| + | 25 | 4 | 21 | |
| − | 67 | 32 | 37 | |
| Adjuvant therapy | 0.08 | |||
| Chemo | 18 | 9 | 9 | |
| Rad | 5 | 2 | 3 | |
| CCRT | 32 | 6 | 26 | |
| None | 39 | 19 | 20 | |
| Complication | ||||
| Blood transfusion | 1 | 3 | 0.305 | |
| Ileus | 0 | 0 | - | |
| Lymph edema (Grade < 1) | 4 | 1 | 0.381 | |
| Lymphangitis (Grade < 2) | 2 | 2 | 1.000 | |
| DVT (Grade < 2) | 2 | 2 | 1.000 | |
| Cuff dehiscene (Grade < 1) | 1 | 0 | - | |
| Port site hernia (Grade < 1) | 1 | 0 | - | |
| Bladder injury (Grade < 1) | 0 | 2 | 0.179 | |
| Obturator nerve injury (Grade < 1) | 1 | 0 | 0.389 |
| All (n = 54) | TLRH (n = 27) | O-RH (n = 27) | p | |
|---|---|---|---|---|
| Age, years | ||||
| Median (range) | 46 (29–77) | 46 (30–77) | 46 (29–75) | 0.670 |
| BMI, kg/m2 | ||||
| Median, range | 21.2 (15.1–35.4) | 21.2 (17.9–27.8) | 21.7 (17–35.4) | 0.074 |
| Para | 0.022 | |||
| 0 | 8 | 7 | 1 | |
| >1 | 46 | 20 | 26 | |
| Histology | 1 | |||
| SCC | 41 | 21 | 20 | |
| Adenocarcinoma/adenosquamous | 13 | 6 | 7 | |
| Tumor size (MRI) | 1 | |||
| <2 cm | 24 | 12 | 12 | |
| ≥2 cm | 30 | 15 | 15 | |
| Operative time (min) | 382 | 384 (270–460) | 377 (253–663) | 0.768 |
| Amount of bleeding | 417 | 196 (5–1772) | 550 (123–2360) | <0.001 |
| Post-operative stage (FIGO2018) | 0.224 | |||
| 1B1 | 39 | 15 | 12 | |
| 1B2 | 15 | 8 | 7 | |
| 2A1 | 1 | 1 | ||
| 2B | 1 | |||
| 3C1p | 11 | 3 | 8 | |
| LVSI | 1 | |||
| + | 27 | 13 | 14 | |
| − | 27 | 14 | 13 | |
| Number of harvested lymph node | 26.5 (13–57) | 30 (18–57) | 23 (13–55) | 0.109 |
| Lymph node metastasis | 0.175 | |||
| + | 11 | 3 | 8 | |
| − | 43 | 24 | 19 | |
| Adjuvant therapy | 1.00 | |||
| Chemo | 10 | 7 | 3 | |
| Rad | 3 | 1 | 2 | |
| CCRT | 12 | 5 | 7 | |
| None | 29 | 14 | 15 |
| Case | Age | Histology | Tumor Size (MRI) | Tumor Size (Histology) | LVSI | Recurrence | Rupture Site | Prognosis |
|---|---|---|---|---|---|---|---|---|
| 1 | 47 | SCC | 35 | 45 | - | - | Anterior | NED |
| 2 | 44 | SCC | 27 | 25 | + | + | Anterior | DOD |
| 3 | 50 | SCC | 20 | 18 | + | - | Rt, lateral | NED |
| 4 | 40 | AC | 0 | 10 | - | - | Lt, lateral | NED |
| 5 | 74 | SCC | 16 | 9 | - | - | Rt, lateral | NED |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kondo, E.; Yoshida, K.; Kubo-Kaneda, M.; Nii, M.; Okamoto, K.; Magawa, S.; Nimua, R.; Okumura, A.; Okugawa, T.; Yamawaki, T.; et al. Does Vaginal Cuff Creation and Avoidance of a Uterine Manipulator Improve the Prognosis of Total Laparoscopic Radical Hysterectomy for Early Cervical Cancer? A Retrospective Multicenter Study. Cancers 2022, 14, 4389. https://doi.org/10.3390/cancers14184389
Kondo E, Yoshida K, Kubo-Kaneda M, Nii M, Okamoto K, Magawa S, Nimua R, Okumura A, Okugawa T, Yamawaki T, et al. Does Vaginal Cuff Creation and Avoidance of a Uterine Manipulator Improve the Prognosis of Total Laparoscopic Radical Hysterectomy for Early Cervical Cancer? A Retrospective Multicenter Study. Cancers. 2022; 14(18):4389. https://doi.org/10.3390/cancers14184389
Chicago/Turabian StyleKondo, Eiji, Kenta Yoshida, Michiko Kubo-Kaneda, Masafumi Nii, Kota Okamoto, Shoichi Magawa, Ryo Nimua, Asumi Okumura, Toshiharu Okugawa, Takaharu Yamawaki, and et al. 2022. "Does Vaginal Cuff Creation and Avoidance of a Uterine Manipulator Improve the Prognosis of Total Laparoscopic Radical Hysterectomy for Early Cervical Cancer? A Retrospective Multicenter Study" Cancers 14, no. 18: 4389. https://doi.org/10.3390/cancers14184389
APA StyleKondo, E., Yoshida, K., Kubo-Kaneda, M., Nii, M., Okamoto, K., Magawa, S., Nimua, R., Okumura, A., Okugawa, T., Yamawaki, T., Nagao, K., Yoshimura, K., Watashige, N., Yanoh, K., & Ikeda, T. (2022). Does Vaginal Cuff Creation and Avoidance of a Uterine Manipulator Improve the Prognosis of Total Laparoscopic Radical Hysterectomy for Early Cervical Cancer? A Retrospective Multicenter Study. Cancers, 14(18), 4389. https://doi.org/10.3390/cancers14184389